
Abstract
Objective:
Larch arabinogalactan (ResistAid) may prevent cold infections due to its immune-stimulatory properties. In a placebo-controlled, double-blind, randomized clinical trial, the effect of a proprietary larch arabinogalactan preparation on the incidences of common colds and its effect on cold symptoms, as a well established model for immune function, was compared to placebo.
Research design and methods:
A total of 199 healthy participants who had a self reported cold infection rate of three in 6 months were randomly assigned to receive a total of either 4.5 g of an arabinogalactan preparation (n = 101) or placebo (n = 98) over a period of 12 weeks.
Main outcome measures:
The participants documented each common cold episode in a diary, and rated 10 predefined infection symptoms on a 4 point rating scale during an infection period, resulting in an infection score. The common cold episodes were confirmed by medical doctors.
Clinical trial registration:
ISRCTN41183655.
Results:
In the full analysis set (FAS), arabinogalactan tended to decrease the incidence of common cold (p = 0.055). The number of participants affected by a cold was significantly reduced by arabinogalactan supplementation (p = 0.038). Concerning the per protocol (PP) collective, the incidences of common cold (p = 0.040) and the number of participants affected by the infection (p = 0.033) were significantly fewer after arabinogalactan compared to placebo consumption. The severity of symptoms at episode start as experienced by the participants was significantly higher after arabinogalactan supplementation (p = 0.028). The treatment was well tolerated with no significant differences between the study groups.
Conclusion:
The present study demonstrated that larch arabinogalactan increased the body’s potential to defend against common cold infection. While the immunomodulatory effect of arabinogalactan can be assumed, its mechanism of action remains to be elucidated.
Introduction
Growing evidence obtained from in vitro, animal and human studies strongly suggest the immunomodulatory effect of arabinogalactanCitation1. Arabinogalactan is a long, densely branched, polysaccharide with molecular weight ranging from 10,000 to 120,000 Daltons. It is mostly present in glycoprotein form, bound to a protein spine of threonine, proline or serine (arabinogalactan protein)Citation2. In nature, arabinogalactans are found in microbial systems and plants. Among the many plants containing arabinogalactan are several immune-enhancing species such as Echinacea purpurea and Curucuma longaCitation3,Citation4. The major commercial source of arabinogalactan, however, is the larch tree. Arabinogalactans extracted from Larix spp. bark are water soluble, highly branched molecules composed of galactose and arabinose units in a 6:1 ratio, with trace amounts of glucuronic acid. Larch arabinogalactan has a galactan backbone that features β(1,3) linkages and galactose β(1,6) and arabinose β(1,6 and 1,3) sugar side chainsCitation1.
Although generally harmless in symptomology, common cold infections count among the most frequent diseases in humans and, in fact, each person of the general population will catch a cold occasionallyCitation5. The common cold is, in most cases, a viral infectious disease of the upper respiratory systemCitation5. A well functioning immune system, including the innate and adaptive immune responses, is crucial for the defense against viral infections such as common colds.
According to the European Food Safety Authority (EFSA)Citation6, defense against pathogens at specific sites of the body, for example the upper respiratory tract, is a particular aspect of immune function. In this respect, an appropriate outcome measure is the number of episodes including severity or duration of the infection. This corresponds to the current scientific view on appropriate markers of the immune systemCitation7,Citation8.
The innate immune system comprises cells like neutrophils, monocytes, macrophages, complement factors and natural killer (NK) cells which rapidly recognize and respond to pathogens. This immune response depends largely on the recognition of pathogen associated molecular patterns (PAMP) by so-called pattern recognition receptors (PRR). The adaptive immune response, composed of highly specialized, systemic cells and processes, follows a few days later.
Arabinogalactan from larch was demonstrated to stimulate the innate immunity by increasing the NK cell cytotoxicity and the phagocytic capacity of macrophages and monocytes mediated by pro-inflammatory cytokinesCitation9–12. Udani et al.Citation13 suggested that arabinogalactan acts in a more specific manner on the adaptive immunity, as shown in the increase in antibody response to the pneumonia vaccine.
The aim of the present interventional study was to reveal the potential superiority of a proprietary arabinogalactan extract from the larch tree (ResistAid) as compared to placebo on naturally acquired common cold episodes and the severity of the symptoms in otherwise healthy participants. The primary endpoint was the reduction of number of cold episodes over a period of 12 weeks in a comparison between arabinogalactan and placebo study arms.
The susceptibility to common colds is often related to a weak immune status or a lack of strong immune defenseCitation14,Citation15. Thus, the common cold was used as a model system to determine the effect of an arabinogalactan preparation on the human system against invading pathogens.
Patients and methods
Trial design
The study was conducted as a prospective multi-center, randomized, double-blind, placebo-controlled study in healthy outpatient participants, with recurring upper respiratory tract infections (URTI). The study was approved by the local Ethics Advisory committee, Ethikkommission Charité-Universitätsmedizin, and carried out in accordance with the Declaration of Helsinki (Hong Kong 1989, Somerset 1996) as well as the ICH-GCP guidelines and EU recommendations (CPMP/ICH/135/95; Topic E6 [R1]). The study was registered in the International Standard Randomized Controlled Trial Number Register (http://www.isrctn.org/) as ISRCTN41183655.
Participants
Between October 2010 and February 2011, a total of 204 otherwise healthy participants who had a self reported cold infection rate of three in 6 months were enrolled at six study sites in Germany. Inclusion criteria were: age 18–70 years, written consent to participate, and at least three infections of upper airways within the last 6 months. The exclusion criteria were as follows: acute or chronic upper airways disease, suspected influenza or swine flu, vaccination against influenza or swine flu within 21 days before the study start, BMI > 30, clinically significant abnormal laboratory parameters, known sensibility to one of the ingredients of the study product, immune deficiency diseases, severe organ or systemic disorders, body temperature ≥38°C, pregnancy or nursing, intake of preparations that can influence the study outcome, incidence of alcohol, medication or drug abuse, use of pre- and probiotics, participation in a clinical study within the previous 30 days. Participants were instructed not to change their eating habits. Participants gave written informed consent prior to the study.
Interventions
During the study period of 12 weeks, participants received a total of either 4.5 g of a proprietary water-based extract from larch tree (ResistAid†) or placebo. The active ingredients are the soluble fiber arabinogalactan and bioactive flavonoids. ResistAidFootnote† is a fine brown powder with a neutral taste and a fine pine-like aroma that dissolves quickly in water or juice. The placebo product was maltodextrin (Maltrin M100). Verum and placebo were provided in sachets manufactured by Proderma, Switzerland. Participants were instructed to dissolve the content of a sachet in approximately 100–150 mL of liquid and take the prepared drink daily at breakfast. During the 12 week study period, a total of three basic visits were performed: at baseline, after 6 weeks and at the end after 12 weeks. Additionally, an episode visit was performed at the start and on the fifth day of each common cold episode. During an episode, the participants were instructed to record and assess their cold symptoms for a period of 14 days. For each occurring infection, the same procedure was performed. Thus, the total number of visits per participant varies depending on the number of infection episodes. Eating habits were recorded in a diet diary at start and end of the study. Compliance was checked by counting returned capsules. The accepted compliance rate was defined as 75–125% of capsules consumed. Biochemical parameters were assessed at baseline and at the end of the intervention.
Outcomes
The primary objective of the present study, the frequency of common cold episodes, was defined as the number of common cold infections during the study period. All the common cold episodes had to be documented in the subject diary and confirmed by an investigator during the 12 week intervention period. As secondary outcome parameters, the duration of cold episodes (based on subject diary), the episode intensity (as change of the total sum score after 5 days compared to start of episode at first episode visit, based on case report file [CRF] and subject diary), and the episode intensity at start of episode (sum score on day 1 based on subject diary) were assessed. For assessment of episode intensity, the participants had to rate ten predefined cold symptoms during the infection episode, on a rating scale (0 = complaint free, 1 = weak symptoms, 2 = moderate symptoms, 3 = strong symptoms) and had to document them in a diary. Symptoms were as follows: headache, joint pain, sore throat, difficulty swallowing, hoarseness, coughing, a watery nasal discharge, nasal congestion, cold related sleeping difficulties, body temperature >38°C. By summation of the scores of the individual symptoms, a sum of scores (=total score) was calculated at episode start and after 5 days. The duration of an episode was defined as the number of days since episode start until the first symptom-free day. Eating habits based on a 3 day record were assessed.
As a concurrent variable, the efficacy of the investigational product was evaluated by the participants and the investigator at the end of each common cold episode as ‘very good’, ‘good’, ‘moderate’, or ‘poor’. The safety and tolerability of the product was evaluated by the documentation of adverse events, the assessment of laboratory parameters and by the global evaluation of the tolerability by the investigator and the subject at the end of the study. At each visit, the investigator asked the subject if any adverse events (AE) had occurred and recorded the respective AE. For any AE that occurred, the investigator recorded the seriousness, intensity, time of occurrence and duration of the observed AE. Further, the investigator recorded his/her judgment as to whether the observed AE has a causal relation to the intake of the investigational product as well as any actions taken due to an AE. The number of AEs was the basis for comparison between the study arms.
Sample size estimation
The sample size calculation, based on two sample t-tests, was determined by the effect size (group comparison), as well as the previously determined requirements of the significance level (5.0%, two-sided) and power (80%). The assumption of the effect size was based on the results of an unpublished superiority clinical study with a comparable design with an effect size of 0.49 for FAS and 0.42 for the PP population. No interim analysis was planned.
Randomization and blinding
The random allocation sequence was computer generated with a block size of four. The ratio of randomization between the verum and the placebo group was 1:1. Based upon the random list which was generated by an independent statistician, each container with sachets received a randomization number during packaging by a contract packaging company. Randomization was concealed from the study sites. The randomization sequence was stored under lock and key by Lonza Ltd. Investigators at the study sites enrolled participants and assigned them to random numbers in a sequential order. Verum and placebo were identical in appearance and taste. Both study participants and investigators assessing outcomes were blinded to treatment assignment. Unblinding occurred only after closure of the database. No blinding envelope was opened.
Statistical analysis
All the variables contained in the data collection were presented descriptively using their statistical key data or their frequency distribution and statistically analyzed in view of the group specific differences (pχ2-value). The Mann–Whitney U-test was employed to test for between-groups comparison (pU). All statistical analyses were carried out on the FAS, including all randomized participants that received at least one intervention treatment and had data apart from baseline data, and on the PP set, including all randomized participants without major protocol deviations. Statistical analyses were performed with SPSS (SPSS for Windows, Release 19, LEAD Technologies Inc.). Values of p < 0.05 were considered significant. Means are given with standard deviation (SD) and confidence intervals (CI) of 95%.
Results
Subject recruitment
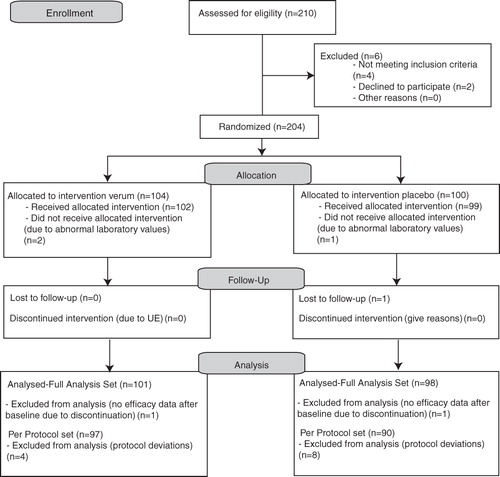
Out of 210 men and women assessed for eligibility, 204 were randomized (). As three participants showed abnormal baseline laboratory values, 201 participants received treatment. Two participants were lost to follow up. The remaining 199 participants represent the FAS, thereof 101 in the verum and 98 in the placebo arm. Of these participants, twelve were excluded from the PP analysis due to major protocol deviations resulting in 187 participants (97 in the verum and 90 in the placebo arm). Participants were recruited between October 2010 and February 2011. The last subject completed the study in May 2011.
Figure 1. Subject flow.
Baseline data
Of the 199 participants, 65 (33%) were men and 134 (67%) were women. All participants reported that they had experienced at least three cold episodes in the 6 months prior to beginning the study. The baseline characteristics () and the eating habits at baseline and at the end of the study period did not differ between interventional groups.
Table 1. Baseline characteristics of the arabinogalactan and the placebo groups (FAS).
Incidence of common cold infection
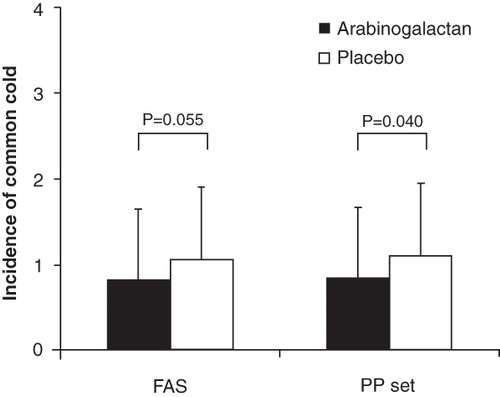
Arabinogalactan treatment as compared to placebo tended to decrease the mean number of common cold episodes in the FAS population – verum group (VG): 0.83 (SD 0.82; CI 0.67–0.99) vs. placebo group (PG): 1.06 (SD 0.85; CI 0.89–1.23; pU = 0.055) (). The number of participants affected by a cold episode significantly differed between the study arms (nactive = 59 [58%]; nplacebo = 71 [72%]; pχ2 = 0.038). In the PP population, the mean number of episodes was 0.85 (SD 0.82; CI 0.68–1.10) in the verum and 1.1 (SD 0.85; CI 0.92–1.28) in the placebo group (pU = 0.040) (). Significantly fewer participants suffered from a cold episode in the active group (n = 58; 60%) as opposed to the placebo group (n = 67; 74%) (pχ2 = 0.033).
Figure 2. Incidence of common cold infections following 12 week arabinogalactan or placebo supplementation according to the FAS and the PP population. Values are mean ± SD.
Intensitiy and duration of common cold episodes
The intensity of symptoms did not differ between the active group (8.4; SD 6.8; CI 6.6–10.3) and the placebo group (8.5; SD 6.6; CI 6.8–10.2) regarding the change in the sum of scores from day 1 to day 5 of a cold episode (pU = 0.10). This applies also for the change in the total sum of score documented in the subject diary with a mean of 5.85 (SD 8.35; CI 3.9–7.8) in the verum group and 4.73 (SD 8.08; CI 3.0–6.4) in the placebo group (pU = 0.59).
Regarding the sum of the cold symptom scores assessed at the first episode visit, there was a non-significant difference between the verum (13.3; SD 6.6; CI 11.8–14.7) and placebo group (11.6; SD 6.3; CI 10.4–12.9; pU = 0.06), while the sum of score documented in the subject diary at episode start differed between study arms – VG: 13.7 (SD 6.9; CI 12.2–15.2) vs. PG: 11.5 (SD 6.5; CI 10.2–12.8; pU = 0.028).
The duration of the common cold episodes did not differ between the study arms – VG: 8.5 (SD 2.8; CI 7.8–9.2) vs. PG: 8.3 (SD 2.9; CI 7.6–9.0; pU = 0.61).
Increase in symptom-free days
Analysis of symptom-free days was performed for a study duration of 10 weeks, which was chosen for comparison reasons as it had been achieved by the whole PP population. The percentage of days that participants from the PP collective did not suffer from cold symptoms was significantly higher in the arabinogalactan group (91.2%) compared to the placebo group (88.5%) (pchi < 0.001).
Global evaluation of the efficacy (FAS)
At the end of the study, the global assessment of efficacy for arabinogalactan treatment was rated as ‘very good’ or as ‘good’ by 83.7% of participants and by the physicians for 87.8% of the participants. For placebo, the efficacy was rated as ‘very good’ or ‘good’ by the investigators for 75.2% of the participants and by 73.7% participants in self-assessment. Both physicians and participants rated the efficacy of the arabinogalactan preparation better than the placebo (pχ2 = 0.023 and pχ2 = 0.090, respectively).
Safety evaluation
All measured clinical parameters, body weight, temperature, heart rate and blood pressure remained nearly constant during the study, with no significant differences between the two study populations.
A total of 16 adverse events occurred during the study period. Eight of them occurred in the active group (gastro-intestinal infection [n = 2], cramp-like chest pain, purulent bronchitis, cervical syndrome, urinary infection, pneumonia right lower lobe, abnormal laboratory values at final visit). Another eight events occurred in the placebo group (gastroenteritis [n = 2], hypoglycemia with cold sweat, urinary infection, abnormal laboratory values at final visit, soft stool 30 minutes after intake of the investigational product, hay fever, lumbago). One adverse event (pneumonia right lower lobe) in the active group was classified as serious; this was, however, not related to the intervention. This serious adverse event led to study termination by the subject. One adverse event in the placebo group was judged as possibly related to the intake of the investigational product. The two study groups did not differ in the proportion of participants with adverse events (pχ2 = 0.94).
Discussion
The present study provided, in a placebo-controlled, randomized double blind intervention, clinical evidence for a link between consuming a proprietary larch arabinogalactan preparation and a reduction in the number of seasonal common cold episodes. The primary endpoint was reached with a statistical significance in the PP population. In the FAS collective, significance was just missed; however, a strong positive trend was shown.
The average number of episodes observed in the present study was smaller than expected, which possibly had an effect on the obtained results. Given a higher total number of episodes, the primary endpoint would most likely have been reached in the FAS population as well.
Regarding intensity and duration of cold symptoms, no significant differences between study arms could be observed, except for the endpoint intensity of symptoms at episode start, based on records in the subject diary. On the first day of the episode, there was a statistically significant slightly higher total symptom score in the arabinogalactan study arm. However, no significant differences were observed for the same secondary endpoint based on records from the first episode visit in the CRF. Further, since the two study arms do not significantly differ with respect to the change in symptom intensity after 5 days, the effect observed on day 1 does not prevail.
The large spread in the data might be the reason that no significant differences in the duration of cold episodes could be obtained. At the respective time point of starting the documentation in the subject diary, great differences in symptom strength were present, i.e. the participants presumably started documenting at different stages of the cold episodes. The reason could be the highly variable individual subjective perception of the disease process by the participants.
The ability of a person to defend against the common cold is influenced by their individual immunocompetencies and susceptibility to a cold infection depends in part on environmental factors including psychological stress, lack of vitamins or exposure to wet conditions and low temperatures. Therefore, every subject is at risk for getting a cold, at least occasionallyCitation14,Citation15. As such, the participants included in the present clinical trial were of both sexes and aged 18 to 70 years and, hence, represent the general population.
The supplementation with an arabinogalactan preparation reduced the number of common cold episodes by 23%, which suggests an immunomodulatory effect of arabinogalactan. Indeed, our data are in line with in vitro and animal studies that showed various immunomodulating effects of arabinogalactan on markers of the innate as well as adaptive immunity. Hence, in response to arabinogalactan, human peripheral blood mononuclear cells (PBMC) and their subpopulations have been shown to release pro-inflammatory cytokines which stimulated NK cytotoxicityCitation11. Moreover, larch arabinogalactan activated lymphocytes and macrophages in vitro which provokes a variety of cellular response including enhanced phagocytosis, oxidative burst and the modulation of cytokine productionCitation9. A study in dogs demonstrated increases in neutrophils and eosinophils in blood without effects on serum immunoglobulin (Ig) G, IgM or IgA following oral administration of arabinogalactan from larchCitation10. The same proprietary larch arabinogalactan has recently been demonstrated a selective immune-stimulatory effect on the adaptive immune system, as shown by the increase of the antibody response of healthy volunteers to the pneumonia vaccineCitation13. Markers of the innate immune system, like total white blood cells, cytokines or complement, however, were not changed.
Although the receptor specificity of arabinogalactans is not well characterized, there is strong evidence that arabinogalactans have access to immune cells and are thereby involved in the elimination of invading pathogens. Thus, arabinogalactan may enhance the on-going immune response in order to react as quickly as possible to an infection by pathogens. Moreover, the symptoms of the common cold are primarily related to the immune response, which might explain why participants in the active group experienced the cold symptoms more severely. This in turn might suggest the effectiveness of arabinogalactan in activating the immune response.
As a unique dietary fiber, arabinogalactan impacts the digestive physiology. Grieshop et al.Citation10 revealed that larch arabinogalactan significantly enhanced gut microflora, especially increasing the beneficial fecal bacteria populations bifidobacteria and lactobacilli. The positive effect of these potentially protective bacteria on inhibition of invading pathogens has been demonstrated in vitro and in vivoCitation16,Citation17. This might support the proposed immunomodulating effects of arabinogalactan and is worthy of further investigation in human clinical studies. Indeed, further studies about the underlying mechanism and receptor specificity of arabinogalactan remain to be conducted.
The present study demonstrated the safety and tolerability of a larch arabinogalactan preparation. This is consistent with results of controlled animal studies demonstrating an absence of adverse effects, mortality and signs of toxicity after oral application of larch arabinogalactanCitation18.
Conclusion
Our study in healthy participants, representing the general population, confirms the hypothesis of a prophylactic effect of larch arabinogalactan supplementation on the incidence of common cold. The data showed for the first time the effectiveness of an arabinogalactan preparation in protecting against infections caused by pathogens and suggest a general increase in days free of cold symptoms, which might be of economic benefit.
Transparency
Declaration of funding
Lonza Ltd providing financial support for all aspects of this clinical study. The funders were involved in study design, manuscript writing, and made the decision to submit the paper for publication. Lonza Ltd had no role in data collection, analysis, and interpretation.
J.G. designed research; B.G. conducted research; L.R. and J.G. analyzed data; L.R. wrote the paper. L.R. had primary responsibility for final content. All authors read and approved the final manuscript.
Declaration of financial/other relationships
L.R., B.G. and J.G. are employed by a contract research organization that received funding from Lonza Ltd.
CMRO peer reviewers on this manuscript have received honoraria for their review work, but have no other relevant financial relationships to disclose.
Acknowledgments
We thank Norman Bitterlich PhD for his support in statistical analysis of the data. We thank the investigators R. Busch, C. Lauster, S. Beutner, H.-J. Kramm, J. Förstermann, and P. Sandow for their excellent work.
Previous presentation: Boehme L, Grube B, Gruenwald J, Freitas U. Role of ResistAidTM in reducing the occurrence of the common cold. Poster presented at World Immune regulation Meeting-VI, Davos, Switzerland, 18–21 March 2012. Boehme L, Grube B, Gruenwald J, Freitas U. Role of ResistAidTM in reducing the occurrence of the common cold. Talk and poster presentation at Vitafoods Europe, Geneva, Switzerland, 22–24 May 2012.
Notes
*ResistAid is a registered trade name of Lonza Ltd, Basel, Switzerland.
*ResistAid is a registered trade name of Lonza Ltd, Basel, Switzerland.
*Maltrin M100 is a registered trade name of the Grain Processing Corporation, Muscatine, Iowa, USA.
†ResistAid is a registered trade name of Lonza Ltd, Basel, Switzerland.
References
- Kelly GS. Larch arabinogalactan: clinical relevance of a novel immune-enhancing polysaccharide. Altern Med Rev 1999;4:96-103
- D’Adamo P. Larch arabinogalactan is a novel immune modulator. J Naturopath Med 1996;4:32-9
- Gonda R, Tomoda M, Ohara N, et al. Arabinogalactan core structure and immunological activities of ukonan C, an acidic polysaccharide from the rhizome of Curcuma longa. Biol Pharm Bull 1993;16:235-8
- Bossy A, Blaschek W, Classen B. Characterization and immunolocalization of arabinogalactan-proteins in roots of Echinacea purpurea. Planta Med 2009;75:1526-33
- Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis 2005;5:718-25
- EFSA guidance on antioxdants + oxidative stress + CVD. Guidance on the scientific requirements for health claims related to antioxidants and oxidative stress and cardiovascular health. EFSA Journal 2011;9:2474
- Cummings JH, Antoine JM, Azpiroz F, et al. PASSCLAIM – gut health and immunity. Eur J Nutr 2004;43(Suppl 2):II118-73
- Albers R, Antoine JM, Bourdet-Sicard R, et al. Markers to measure immunomodulation in human nutrition intervention studies. Br J Nutr 2005;94:452-81
- Choi EM, Kim AJ, Kim YO, et al. Immunomodulating activity of arabinogalactan and fucoidan in vitro. J Med Food 2005;8:446-53
- Grieshop CM, Flickinger EA, Fahey GC Jr. Oral administration of arabinogalactan affects immune status and fecal microbial populations in dogs. J Nutr 2002;132:478-82
- Hauer J, Anderer FA. Mechanism of stimulation of human natural killer cytotoxicity by arabinogalactan from Larix occidentalis. Cancer Immunol Immunother 1993;36:237-44
- Currier NL, Lejtenyi D, Miller SC. Effect over time of in-vivo administration of the polysaccharide arabinogalactan on immune and hemopoietic cell lineages in murine spleen and bone marrow. Phytomedicine 2003;10:145-53
- Udani JK, Singh BB, Barrett ML, et al. Proprietary arabinogalactan extract increases antibody response to the pneumonia vaccine: a randomized, double-blind, placebo-controlled, pilot study in healthy volunteers. Nutr J 2010;9:32
- Cohen S, Tyrrell DA, Smith AP. Psychological stress and susceptibility to the common cold. N Engl J Med 1991;325:606-12
- Cohen S, Tyrrell DA, Smith AP. Negative life events, perceived stress, negative affect, and susceptibility to the common cold. J Pers Soc Psychol 1993;64:131-40
- de Vrese M, Schrezenmeir J. Probiotics, prebiotics, and synbiotics. Adv Biochem Eng Biotechnol 2008;111:1-66
- de Vrese M, Winkler P, Rautenberg P, et al. Effect of Lactobacillus gasseri PA 16/8, Bifidobacterium longum SP 07/3, B. bifidum MF 20/5 on common cold episodes: a double blind, randomized, controlled trial. Clin Nutr 2005;24:481-91
- Groman EV, Enriquez PM, Jung C, et al. Arabinogalactan for hepatic drug delivery. Bioconjug Chem 1994;5:547-56