
Abstract
Chronic pain is currently under-diagnosed and under-treated, partly because doctors’ training in pain management is often inadequate. This situation looks certain to become worse with the rapidly increasing elderly population unless there is a wider adoption of best pain management practice. This paper reviews current knowledge of the development of chronic pain and the multidisciplinary team approach to pain therapy. The individual topics covered include nociceptive and neuropathic pain, peripheral sensitization, central sensitization, the definition and diagnosis of chronic pain, the biopsychosocial model of pain and the multidisciplinary approach to pain management. This last section includes an example of the implementation of a multidisciplinary approach in Belgium and describes the various benefits it offers; for example, the early multidimensional diagnosis of chronic pain and rapid initiation of evidence-based therapy based on an individual treatment plan. The patient also receives continuity of care, while pain relief is accompanied by improvements in physical functioning, quality of life and emotional stress. Other benefits include decreases in catastrophizing, self-reported patient disability, and depression. Improved training in pain management is clearly needed, starting with the undergraduate medical curriculum, and this review is intended to encourage further study by those who manage patients with chronic pain.
Introduction
Chronic pain affects approximately 20% of the adult population in developed countriesCitation1–3 and has a profound effect upon individuals, economies and society in general, yet remains under-diagnosed and under-treatedCitation4,Citation5. Relevant factors are that doctors’ training in pain management is often insufficient or almost non-existentCitation6,Citation7, many have misconceptions about the prescription of opioidsCitation8, and improving clinical knowledge could lead to better outcomesCitation9. The prevalence of chronic pain increases with age, and by the age of 70 pain affects 79% of women and 53% of menCitation10. The burgeoning elderly population – the European Commission predicts that almost a quarter of the population of its 27 member states will be more than 65 years of age by 2035Citation11 – suggests that, without an increased knowledge of pain physiology and the wider adoption of best pain management practice, the shortfall in care for these patients is likely to become rapidly worse.
The international CHANGE PAIN Advisory Board of leading pain specialists meets regularly to discuss specific topics to try and achieve consensus on measures that could enhance the care of pain patients. Aware of the urgent and growing need to improve the management of chronic cancer and non-cancer pain, at its meeting on 17th and 18th June 2011 the Advisory Board reviewed current knowledge of the development of chronic pain and the advantages of a multidisciplinary team approach to the provision of pain therapy, in order to support its wider dissemination. A number of consensus points were agreed as being of particular importance. Following relevant presentations to the Board, potential points were discussed and groups of Board members then answered pre-prepared questions on the topics via a local area network. Analysis of the answers was followed by more discussion, and draft versions of the consensus points were further refined by the authors.
The development of chronic pain
Nociceptive and neuropathic pain
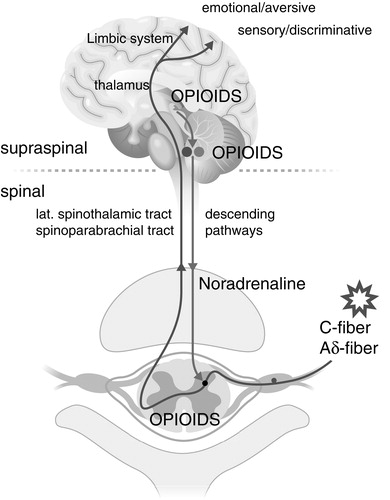
Nociceptive pain is usually transient and may be either somatic or visceral. As a result of tissue damage and inflammation – caused by conditions such as traumaCitation12, arthritisCitation13, or cancerCitation14 – peripheral nociceptors are activated by molecules such as prostaglandins, substance P, histamine and bradykinin. These cause depolarization of the nociceptors that is transmitted to the spinal cord via slow, non-myelinated C fibers and fast, myelinated Aδ fibers. In the spinal cord, the incoming signals are then modulated, transmitted to second order neurons by neurotransmitters, and passed to the brain stem via ascending pathways (). For example, glutamate has an excitatory effect and enhances pain, whereas gamma-aminobutyric acid (GABA) has an inhibitory effect and reduces painCitation15,Citation16. The brain stem essentially acts as a mediator of transmission to higher centers, where the pain signals are interpretedCitation17,Citation18. Pain perception is simultaneously modified by descending pain pathways. Information about noxious stimuli is transmitted from the limbic system and midbrain structures down through the periaqueductal grey to the brainstem, especially the rostroventral medullaCitation19. Here the signals are filtered before passing to the dorsal horn of the spinal cord at the level of the incoming pain signal. Key neurotransmitters in the descending pathways are noradrenaline, which reduces pain, and serotonin (or 5-hydroxytryptamine), which may have both facilitatory and inhibitory functionsCitation20,Citation21.
Figure 1. Ascending and descending pathways.
In 2009, the definition of neuropathic pain was revised by an expert committee of the Neuropathic Pain Special Interest Group of the International Association for the Study of Pain (NeuPSIG); it is now “pain arising as direct consequence of a lesion or disease affecting the somatosensory system”Citation22. The cause may be, for example, trauma, surgery, diabetes, herpes zoster virus, alcohol or cancer. As a result, there is a switch in the phenotype of the sensory neurons and their pain signaling mechanisms. Alterations in the function of sodium channels (which generate pain signals)Citation23, potassium channels (which inhibit pain signals)Citation24 and calcium channels (which facilitate transmitter release) have been reportedCitation25. The pain produced is typically burning, tingling or ‘electric’ in character, and may be accompanied by allodynia – in which normally non-painful stimuli evoke pain – and hyperalgesiaCitation18. Neuropathic pain tends to be more severe than nociceptive pain and also more difficult to treatCitation26.
It should be noted that both nociceptive and neuropathic pain can coexist, in conditions such as back pain and cancer pain, and both may become chronic. It is important that neuropathic pain is not confused with sensitization; the distinction between central or peripheral sensitization and neuropathic pain is often not made, although the underlying pathology is different. Understanding the differences between nociceptive and neuropathic pain, and how they develop, is essential if the patient is to receive the most effective pain therapy.
Consensus point
Understanding current theories of the development of chronic pain is crucial for everyone involved in pain treatment.
Peripheral sensitization
Nociceptive pain is normally experienced as the result of noxious stimuli acting on high threshold nociceptors. In peripheral sensitization, the threshold for activation is reduced and membrane excitability increasesCitation27. The presence of injury or disease causes the local release of inflammatory mediators – protons, adenosine triphosphate, prostaglandins, substance P and histamine – that also attract immune cellsCitation28. These cells, in turn, release cytokines such as interleukin-1β and tumor necrosis factor (TNF), which elicit action potentials by increasing sodium and calcium currents at the nociceptor terminalCitation27. This inflammatory response may be accompanied by ectopic action potentials (i.e. where there is no peripheral stimulus), particularly when there has been damage to neurons.
Central sensitization
If the transmission of pain signals from the periphery to the spinal cord persists, changes may occur in the CNS and produce central sensitization. This can be defined as pain hypersensitivity that may arise from a reduced threshold for activation and an abnormal amplification of sensory signaling within the CNSCitation29. Although nociceptive stimulation from the periphery may be both increased and prolonged initially, the pain experience is disconnected from the peripheral pathology. The process of central sensitization may initially be reversibleCitation30, but it can also become permanent. Its effect at central sites can lead to the establishment of co-morbidities such as depression and anxietyCitation31, as well as to hypersensitivity to other stimuli or the development of more diffuse pain states.
A number of different mechanisms are involved. The development of central sensitization may begin with a nociceptive input from the periphery to a synapse in the dorsal horn of the spinal cord, causing the pre-synaptic neuron to release substance P and glutamate into the synaptic cleft, lowering the threshold of neuronal excitabilityCitation29. By combining with post-synaptic ion channel receptors, the most important of which are N-methyl D-aspartate (NMDA) receptors and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors, these compounds enable the pain signal to be transmitted upwards to the thalamus. Simultaneous activation of Toll-like receptor 4 (TLR4) on microglia cells leads to the release of inflammatory modulators. In addition, pre-synaptic NMDA receptors play a part; blocking these receptors with ketamine reduces the release of substance P and excitatory amino acids. If the nociceptive input from the periphery persists, the prolonged activation of NMDA receptors is accompanied by an increase in NMDA receptor density and the experience of pain is enhancedCitation32,Citation33.
Allodynia, hyperalgesia and spontaneous pain may be produced by central sensitization, but there are additional signs and symptoms. Secondary hyperalgesia (i.e. increased sensitivity to pain in the undamaged tissue around the original injury) indicates central sensitization. Another characteristic is facilitated temporal summation or ‘wind-up’, in which repeated identical stimuli become increasingly painful in spite of unchanged stimulus intensityCitation29,Citation34. NMDA receptors are involved in this process because ‘wind-up’ can be countered with ketamineCitation35. Other clinical features of central sensitization are the expansion of areas of referred pain (a spinal phenomenon resulting from the involvement of neurons other than those receiving a persistent nociceptive input), impaired descending inhibition and enhanced descending facilitation.
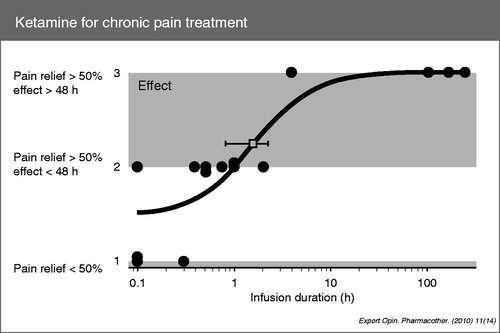
In the case of ‘wind-up’, pre-synaptic NMDA receptors respond to short-term ketamine exposure and produce analgesia. However, it is important to note that this response to ketamine is not synonymous with central sensitization, which is a phenomenon of post-synaptic NMDA receptors. Central sensitization is relatively resistant to ketamine and requires long-term exposure to be effective (). A 1 hour infusion produces over 50% pain relief, but the effect is short-lived and lasts less than 48 hoursCitation36. Some evidence suggests that longer infusions (±100 hours) are required to produce desensitization, but can produce long-term relief from chronic pain which lasts several months; for example, in patients with complex regional pain syndromeCitation37. Thus a persistent effect after ketamine withdrawal may be regarded as a sign of NMDA activity and sensitization.
Figure 2. Duration of pain relief produced by ketamine. (From Noppers I, Niesters M, Aarts L, et al. Ketamine for the treatment of chronic non-cancer pain. Expert Opin Pharmacother 2010;11:2417-29).
There is also evidence that defective descending inhibitory control (DIC) is present in various chronic pain syndromesCitation19,Citation38–40, and may itself be a cause of central sensitization. The presence of defective DIC may be identified by techniques such as offset analgesia, a temporal contrast mechanism for studying endogenous pain reliefCitation41, and diffuse noxious inhibitory control (DNIC), a spatial contrast mechanism which utilizes two stimuli.
Chronic pain: diagnosis and mechanism-based treatment
Chronic pain has traditionally been defined solely on the basis of its duration; for example, as “pain which persists past the normal time of healing. With non-malignant pain, three months is the most convenient point of division between acute and chronic pain, but for research purposes six months will often be preferred”Citation42. Consequently, diagnosis is often similarly based on duration, but this takes no account of the specific causative mechanisms or clinical significance. Knowledge of the causative mechanisms is important, in order to institute the most appropriate treatment strategy, and unless the correct underlying mechanisms are addressed analgesic therapy is likely to prove ineffectiveCitation43. Identification of the multiple mechanisms responsible for the production of pain syndromes and their molecular components has been a major advance in our understanding of painCitation18. However, identification of the pathophysiological mechanisms responsible for distinct pain syndromes is incomplete at present, and multiple mechanisms may coexist in many pain conditions, so combination therapy is often indicatedCitation18. There remains a need for valid and reliable assessment tools which can accurately link specific clinical signs and symptoms to a particular mechanismCitation44.
In recent years, a definition based on a prognostic risk score has been shown to have better predictive validity for pain outcomes than pain duration aloneCitation45. By emphasizing factors other than pain (e.g. activity limitation and depression) this definition may suggest possible avenues for improving outcomes in addition to simply controlling pain (for example, increasing exercise levels and improving mood)Citation45.
The diagnosis of chronic pain requires a multiple step approach, with different tests and investigations being applied at each step. To complement a medical history and physical examination, the physician may use a questionnaire to aid diagnosis. Examples include painDETECT, which can identify the presence of a neuropathic pain component in patients suffering from low back pain with high sensitivity and specificityCitation46, and the Douleur Neuropathique 4 (DN4)Citation47. Other assessment tools include the Standardized Evaluation of Pain (StEP), which uses a structured interview and standardized examination to differentiate pain phenotypes independent of aetiologyCitation48. More technical and sophisticated techniques are under evaluation: for example, Quantitative Sensory TestingCitation49 analyzes perception in response to external stimuli of controlled intensity, and is especially suitable for quantifying hyperalgesia and allodynia in painful neuropathic syndromes.
Clinical investigations might include X-rays, magnetic resonance imaging or computed tomography. Blood tests may indicate the presence of inflammation or infection. In special cases, nerve conduction studies might be used to determine any changes in amplitude or conduction velocity, and somatosensory evoked potential studies to indicate dysfunction of the somatosensory pathways. The function of small fiber (Aδ and C) sensory pathways can be specifically evaluated using laser evoked potentialsCitation50 or the contact heat evoked potential stimulator (CHEPS)Citation51. Suspected small fiber neuropathy is rarely an indication for nerve biopsy, and should instead be investigated with skin biopsy, allowing visualization and quantification of intra-epidermal nerve fibresCitation52. Finally, there is a role for pharmacological intervention in diagnosis; for example, the local application of lidocaine at the peripheral origin of pain, different formulations of opioids, or drugs like amitriptyline and tapentadol which may help to restore descending inhibitory control.
Consensus point
Different types of investigation can help determine the causative mechanisms involved in chronic pain.
The multidisciplinary approach to treatment
The biopsychosocial model
This model of pain, first proposed by EngelCitation53, is now widely accepted as the most heuristic approach to understanding the true nature of chronic pain. It is based on the concept that pain is essentially an interactive psychophysiological behavior pattern that cannot be divided into distinct psychosocial and physical components, and that psychological and social factors must therefore be taken into account when considering treatmentCitation54. Supporting evidence that an appreciation of the biopsychosocial model is essential for understanding the patient with chronic pain comes from a number of studies. For example, catastrophizing and unemployment have been shown to be amongst the strongest predictors of disability one year later in patients with either acute or chronic low back painCitation55,Citation56. Other psychological and social factors that are important prognostic indicators of future pain include anxiety and high levels of distressCitation57,Citation58, and self-rated healthCitation59. Furthermore, numerous studies have demonstrated a beneficial effect of behavioral and psychological interventions in the management of chronic low back painCitation60–63. These results strongly indicate that psychological treatment needs to be integrated with other therapeutic components, such as physical therapy and medication management, or the effectiveness of treatment will be compromised.
Consensus point
A biopsychosocial approach is essential to understanding the patient with chronic pain.
The multidisciplinary team
The complexity of the pain experience means that the diverse aspects of chronic pain are best treated by a multidisciplinary team, enabling patients to benefit from the co-ordination and integration of various medical disciplines and treatment modalities. They are more likely to benefit from an early and accurate diagnosis, and to receive various therapies specifically tailored to their individual needs. Each team member should have a basic knowledge of the physiology and clinical practices associated with chronic pain, and of the expertise of fellow team members. Regular communication between all team members is essential, to help ensure a consistency of approach and good continuity of care, whilst simultaneously avoiding inadequate pain control, unnecessary specialist visits, redundant testing and increased costs. More information about many important aspects of multidisciplinary pain treatment can be found in the booklet ‘Towards a multidisciplinary team approach in chronic pain management’, which was developed by members of the CHANGE PAIN Advisory Board and is now available online at www.change-pain.com.
Consensus point
Multidisciplinary management of chronic pain requires a core multidisciplinary team of healthcare professionals.
The structure of multidisciplinary teams varies considerably, but the core team generally consists of three physicians (e.g. primary care physician, anesthesiologist/pain specialist and psychiatrist), plus non-physicians (e.g. psychologist, physiotherapist and nurses)Citation64. The primary care physician has a key role, acting as gatekeeper of the treatment strategy, as well as being responsible for the long-term care of the patient and referral where necessary. Other specialists that often play a role in the core team include neurologists, rheumatologists, orthopedists, neurosurgeons and rehabilitation therapistsCitation64. As chronic pain affects all aspects of daily living, there is a wider team of medical and non-medical specialists which is more flexible in structure and often provides support for the patient on an ad hoc basis. Members might include pharmacists, dieticians, complementary therapists, educational therapists, occupational therapists and medical social workers.
Multidisciplinary teams are generally managed by the anesthesiologist/pain specialist, who also co-ordinates patients’ individual treatment plansCitation65. Many teams operate syndrome-orientated clinics, such as headache clinics and low back pain centers. Consultations usually involve two or more specialists, and this collaborative approach is also demonstrated by regular joint consultations and pain conferences, which review the pain management and progress of individual patients. These scheduled meetings facilitate optimization of patient care, and provide an opportunity for the referral of patients to a different member of the multidisciplinary team where it is deemed appropriate.
This philosophy has been put into practice in Belgium, where nine multidisciplinary centers for treating chronic pain were established in 2005Citation66. Each had to include at least three medical and three paramedical specialties, and the Director had to have both extra training and at least three years’ full time experience in pain management. The subsequent success of these centers led to the creation of 36 new multidisciplinary teams to treat patients with early stage pain, using a biopsychosocial approach agreed with the Belgian Pain Society. Each includes a pain specialist and a psychiatrist, and all hospital services are available to the team. These measures are complemented by a third mechanism – established at 73 different locations – to tackle pain as early as possible, by using a specially trained nurse to identify patients at risk of developing chronic pain and referring them to a pain specialist for a full diagnosisCitation66.
What are the benefits?
Many of the advantages of the multidisciplinary approach come from the streamlining and rationalization of pain management. It offers an early, multidimensional diagnosis of chronic pain and a rapid initiation of evidence-based therapy according to an individualized treatment plan. A wide array of pharmacological and non-pharmacological treatment options is made available, which the patient can discuss with the various specialists involved. Duplication of investigations is avoided and treatment failure can be picked up early.
For the patient, there is continuity of care, delivered in a programmed and co-ordinated manner. Studies have consistently reported reductions in pain intensity following multidisciplinary pain treatment in patients with chronic low back painCitation61,Citation67, fibromyalgiaCitation68 and temporomandibular disordersCitation69. Recent evidence-based treatment guidelines recommend a multidisciplinary approach for treating several chronic pain conditions, including low back painCitation70 and osteoarthritisCitation71. Furthermore, treatment leads not only to pain relief but also to improvements in physical functioning, quality of life, emotional stress and behavioral outcomes. These, in turn, confer psychological advantages such as greater self-esteem.
In clinical trials, multidisciplinary pain treatment has been shown to facilitate the regaining of physical functioning and the ability to return to workCitation72,Citation73. It is also associated with increases in perceived control over pain and decreases in catastrophizing, self-reported patient disability, pain intensity and depressionCitation74. A meta-analysis of 65 studies, which evaluated the efficacy of multidisciplinary treatment for chronic back pain, concluded that this approach is superior to either conventional unimodal treatment or no treatment, with regard both to patients’ subjective ratings of pain and to behavioral variablesCitation67. Moreover, there is evidence that these benefits are maintained for more than 10 yearsCitation75. In one geographical region of Denmark, the annual rate of lumbar disc operations decreased by almost half following the establishment of two nonsurgical, multidisciplinary spine clinics, and the rate of elective, first-time disc surgeries decreased by approximately two thirdsCitation62.
However, there is still evidence of a lack of consistency in the treatment of patients with chronic pain. Two recent longitudinal studies in the UK investigated the use of National Health Service resources by patients with chronic low back pain and osteoarthritis pain, from the perspective of primary care and secondary care pain clinicsCitation76,Citation77. The primary care study found that most patients received a wide variety of pain medications with no overall prescribing pattern or treatment pathwayCitation76. Many received non-drug treatment, most frequently physiotherapy. The investigators concluded that chronic pain is managed through individualized patient pathways and that evidence-based guidelines for primary care treatment and referral are neededCitation76. The secondary care study revealed wide variations between pain clinics in the source of referral, non-drug treatments, investigations requested and the duration of patients’ registration, as a result of differences in local policies and structuresCitation77. Many patients received no non-drug treatment from the clinic. This study highlighted the lack of a clearly defined model of practice for specialist pain clinicsCitation77.
The development of a standard set of quality indicators could reduce the variation between multidisciplinary pain management teams and lead to a higher overall standard of care. This might include assessment of:
patient outcomes, in terms of reduced intensity and/or frequency of pain, improved physical and psychological functioning, quality of life and patient satisfaction
compliance with guidelines and evidence-based practices developed for specific patient populations, types of pain, and conditions or procedures
use of standardized assessment instruments, such as the Short Form 36 and the McGill Pain Questionnaire
philosophy and organizational strategy orientated towards continuous improvement
quality and frequency of communication within the team
monitoring of team performance and the ready availability of appropriate education and training.
Conclusions
It is important that everyone involved in the management of chronic pain understands the development of chronic pain and the pathophysiological processes involved. This is patently not the case at present and the consequences include poor diagnosis, inappropriate drug therapy, and neglect of concomitant symptoms such as anxiety and catastrophizing. The number of patients with chronic pain looks set to increase dramatically and improved training in pain management is clearly needed, starting with the undergraduate medical course. Even in developed countries the amount of time currently allocated to pain management is generally inadequate; in the UK, for example, the median time spent on pain management by a medical student is 13 hours, and sometimes as little as 6 hoursCitation78. When the undergraduate training of all healthcare professionals is analyzed, education about the identification, assessment and treatment of pain represents less than 1% of university-based teaching – yet pain is the most common reason for patients to consult their general practitionerCitation78. Continuing medical education must also play a part, and this review of the development of chronic pain and best clinical practice is intended to encourage further study by those who manage patients with chronic pain.
Transparency
Declaration of funding
This article was based on a meeting held in Brussels, Belgium, on 17th and 18th June 2011, which was supported by Grünenthal GmbH, Aachen, Germany, who also sponsored the preparation of this manuscript.
Declaration of financial/other relationships
The following authors received honoraria for attending the meeting in Brussels: J.P., K.A., D.A., E.A., F.C., A.D., F.H., M.K.-K., A.C.M., P.M., B.M., G.M.-S., A.N., C.P.H., P.S., M.S., G.V. G.V. and G.M.-S. have been chairmen of Grünenthal’s International CHANGE PAIN Advisory Board since June 2009, and receive honoraria in this context.
CMRO peer reviewers may have received honoraria for their review work. The peer reviewers on this manuscript have disclosed that they have no relevant financial relationships.
Acknowledgments
The authors thank Derrick Garwood Ltd, Cambridge, UK, for editorial support, which was sponsored by Grünenthal GmbH, Aachen, Germany.
References
- Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain 2006;10: 287-333
- Sjøgren P, Ekholm O, Peuckmann V, et al. Epidemiology of chronic pain in Denmark: an update. Eur J Pain 2009;13:287-92
- Langley PC. The prevalence, correlates and treatment of pain in the European Union. Curr Med Res Opin 2011;27:463-80
- McCarberg BH, Nicholson BD, Todd KH, et al. The impact of pain on quality of life and the unmet needs of pain management: results from pain sufferers and physicians participating in an Internet survey. Am J Ther 2008;15:312-20
- Akashi M, Yano E, Aruga E. Under-diagnosis of pain by primary physicians and late referral to a palliative care team. BMC Palliative Care 2012;11:7
- Peker L, Celebi N, Canbay O, et al. Doctors’ opinions, knowledge and attitudes towards cancer pain management in a university hospital. Agri 2008;20:20-30
- Kim MH, Park H, Park EC, et al. Attitude and knowledge of physicians about cancer pain management: young doctors of South Korea in their early career. Jpn J Clin Oncol 2011;41:783-91
- Wolfert MZ, Gilson AM, Dahl JL, et al. Opioid analgesics for pain control: Wisconsin physicians’ knowledge, beliefs, attitudes, and prescribing practices. Pain Medicine 2010;11:425-34
- Chen L, Houghton M, Seefeld L, et al. Opioid therapy for chronic pain: physicians’ attitude and current practice patterns. J Opioid Manag 2011;7:267-76
- Bergh I, Steen G, Waern M, et al. Pain and its relation to cognitive function and depressive symptoms: a Swedish population study of 70-year-old men and women. J Pain Symp Manag 2003;26:903-12
- European Commission. Population projections 2008–2060. Available at: http://europa.eu/rapid/press-release_STAT-08-119_en.htm [Last accessed 15 February 2013]
- Kehlet H, Jensen TS, Woolf CJ. Persistent surgical pain: risk factors and prevention. Lancet 2006;367:1618-25
- Schaible HG, Richter F, Ebersberger A, et al. Joint pain. Exp Brain Res 2009;196:153-62
- Mantyh PW. Cancer pain and its impact on diagnosis, survival, and quality of life. Nat Rev Neurosci 2006;7:797-809
- Fundytus ME. Glutamate receptors and nociception: implications for the drug treatment of pain. CNS Drugs 2001;15:29-58
- Jasmin L, Wu MV, Ohara PT. GABA puts a stop to pain. Curr Drug Targets CNS Neurol Disord 2004;3:487-505
- Millan MJ. Descending control of pain. Prog Neurobiol 2002;66:355-474
- Woolf CJ. Pain: moving from symptom control toward mechanism-specific pharmacologic management. Ann Intern Med 2004;140:441-51
- Ossipov MH, Dussor GH, Porreca F. Central modulation of pain. J Clin Invest 2010;120:3779-87
- D’Mello R, Dickenson AH. Spinal cord mechanisms of pain. Br J Anaesth 2008;101:8-16
- Marks DM, Shah MJ, Patkar AA, et al. Serotonin–norepinephrine reuptake inhibitors for pain control: premise and promise. Curr Neuropharmacol 2009;7:331-6
- Geber C, Baumgärtner U, Schwab R, et al. Revised definition of neuropathic pain and its grading system: an open case series illustrating its use in clinical practice. Am J Med 2009;122(10 Suppl):S3-12
- Hargus NJ, Patel MK. Voltage-gated Na+ channels in neuropathic pain. Expert Opin Investig Drugs 2007;16:635-46
- Munro G, Dalby-Brown W. Kv7 (KCNQ) channel modulators and neuropathic pain. J Med Chem 2007;50:2576-82
- Todorovic SM, Jevtovic-Todorovic V. The role of T-type calcium channels in peripheral and central pain processing. CNS Neurol Disord Drug Targets 2006;5:639-53
- Schmidt CO, Schweikert B, Wenig CM, et al. Modelling the prevalence and cost of back pain with neuropathic components in the general population. Eur J Pain 2009;13:1030-5
- Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu Rev Neurosci 2009;32:1-32
- Zhang N, Oppenheim JJ. Crosstalk between chemokines and neuronal receptors bridges immune and nervous systems. J Leukoc Biol 2005;78:1210-14
- Sandkühler J. Models and mechanisms of hyperalgesia and allodynia. Physiol Rev 2009;89:707-58
- Arendt-Nielsen L. Pathophysiology of referred muscle pain. In: Fernández-de-las-Peñas C, Arendt Nielsen L, Gerwin R (eds.) Tension-Type and Cervicogenic Headache: Pathophysiology, Diagnosis, and Management. Sudbury, Massachusetts, USA: Jones & Bartlett, 2010:51-9
- Smart KM, Blake C, Staines A, et al. Self-reported pain severity, quality of life, disability, anxiety and depression in patients classified with ‘nociceptive’, ‘peripheral neuropathic’ and ‘central sensitization’ pain. The discriminant validity of mechanisms-based classifications of low back (±leg) pain. Man Ther 2012;17:119-25
- Mannion RJ, Woolf CJ. Pain mechanisms and management: a central perspective. Clin J Pain. 2000;16(Suppl):S144-56
- Larssen M. Ionotropic glutamate receptors in spinal nociceptive processing. Mol Neurobiol 2009;40:260-88
- Pedersen JL, Andersen OK, Arendt-Nielsen L, et al. Hyperalgesia and temporal summation of pain after heat injury in man. Pain 1998;74:189-97
- Guirimand F, Dupont X, Brasseur L, et al. The effects of ketamine on the temporal summation (wind-up) of the RIII nociceptive flexion reflex and pain in humans. Anesth Analg 2000;90:408-14
- Noppers I, Niesters M, Aarts L, et al. Ketamine for the treatment of chronic non-cancer pain. Expert Opin Pharmacother 2010;11:2417-29
- Correll GE, Maleki J, Gracely EJ, et al. Subanesthetic ketamine infusion therapy: a retrospective analysis of a novel therapeutic approach to complex regional pain syndrome. Pain Med 2004;5:263-75
- Song GH, Venkatraman V, Ho KY, et al. Cortical effects of anticipation and endogenous modulation of visceral pain assessed by functional brain MRI in irritable bowel syndrome patients and healthy controls. Pain 2006;126:79-90
- Pertovaara A, Almeida A. Descending inhibitory systems. In: Cervero F, Jensen TS (eds.) Handbook of Clinical Neurology. Amsterdam, The Netherlands: Elsevier, 2006:179-92
- Bielefeldt K, Davis B, Binion DG. Pain and inflammatory bowel disease. Inflamm Bowel Dis 2009;15:778-88
- Niesters M, Hoitsma E, Sarton E, et al. Offset analgesia in neuropathic pain patients and effect of treatment with morphine and ketamine. Anesthesiology 2011;115:1063-71
- Merskey H, Bogduk N. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. Seattle, WA: IASP Press, 1994
- Müller-Schwefe GHH, Jacksch W, Morlion B, et al. Make a CHANGE: optimising communication and pain management decisions. Curr Med Res Opin 2011;27:481-8
- Widerström-Noga EG, Finnerup NB, Siddall PJ. Biopsychosocial perspective on a mechanisms-based approach to assessment and treatment of pain following spinal cord injury. J Rehab Res Dev 2009;46:1-12
- Von Korff M, Dunn KM. Chronic pain reconsidered. Pain 2008;138:267-76
- Freynhagen R, Baron R, Gockel U, et al. PainDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin 2006;22:1911-20
- Attal N, Perrot S, Fermanian J, et al. The neuropathic components of chronic low back pain: a prospective multicenter study using the DN4 questionnaire. J Pain 2011;12:1080-9
- Scholz J, Mannion RJ, Hord DE, et al. A novel tool for the assessment of pain: validation in low back pain. PLoS Med 2009;6:e1000047
- Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain 2006;123:231-43
- Fila M, Bogucki A. Laser evoked potentials as a method of evaluating the function of small fibres – application technique and clinical implications. Neurol Neurochir Pol 2009;43:368-81
- Atherton DD, Facer P, Roberts KM, et al. Use of the novel contact heat evoked potential stimulator (CHEPS) for the assessment of small fibre neuropathy: correlations with skin flare responses and intra-epidermal nerve fibre counts. BMC Neurology 2007;7:21
- Mellgren SI, Lindal S. Nerve biopsy – some comments on procedures and indications. Acta Neurol Scand (Suppl) 2011;191:64-70
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science 1977;196:129-36
- Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Turk DC, Gatchel RJ (eds.) Psychological Approaches to Pain Management: A Practitioner’s Handbook. New York: Guilford Press, 2002:3-32
- Grotle M, Foster NE, Dunn KM, et al. Are prognostic indicators for poor outcome different for acute and chronic low back pain consulters in primary care? Pain 2010;151:790-7
- Dunn KM, Jordan KP, Croft PR. Contributions of prognostic factors for poor outcome in primary care low back pain patients. Eur J Pain 2011;15:313-19
- Grotle M, Brox JI, Veierød MB, et al. Clinical course and prognostic factors in acute low back pain: patients consulting primary care for the first time. Spine (Phila Pa 1976) 2005;30:976-82
- Mallen CD, Peat G, Thomas E, et al. Prognostic factors for musculoskeletal pain in primary care: a systematic review. Br J Gen Pract 2007;57:655-61
- Deyo RA, Diehl AK. Psychosocial predictors of disability in patients with low back pain. J Rheumatol 1988;15:1557-64
- van Tulder MW, Ostelo R, Vlaeyen JW, et al. Behavioral treatment for chronic low back pain: a systematic review within the framework of the Cochrane Back Review Group. Spine 2001;26:270-81
- Guzman J, Esmail R, Karjalainen K, et al. Multidisciplinary bio-psycho-social rehabilitation for chronic low back pain. Cochrane Database Syst Rev 2002;1:CD000963
- Rasmussen C, Nielsen GL, Hansen VK, et al. Disc surgery before and after implementation of multidisciplinary nonsurgical spine clinics. Spine 2005;30:2469-73
- Hoffman BM, Papas RK, Chatkoff DK, et al. Meta-analysis of psychological intervention for chronic low back pain. Health Psychol 2007;26:1-9
- Peng P, Stinson JN, Choiniere M, et al. Role of health care professionals in multidisciplinary pain treatment facilities in Canada. Pain Res Manag 2008;13:484-8
- Chen PP. Multidisciplinary approach to chronic pain management. Hong Kong Med J 1996;2:401-4
- Onkelinx L. Foreword to the Proceedings of the Symposium ‘Societal Impact of Pain’, held in Brussels, Belgium, on May 4th and 5th, 2010. Available at: http://www.sip-meetings.org/cmsdata/grt-sip/en_EN/pdf/SIP_2010_proceedings.pdf [Last accessed 7 July 2011]
- Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain 1992;49:221-30
- Carbonell-Baeza A, Aparicio VA, Ortega FB, et al. Does a 3-month multidisciplinary intervention improve pain, body composition and physical fitness in women with fibromyalgia? Br J Sports Med 2011;45:1189-95
- Gardea MA, Gatchel RJ, Mishra KD. Long-term efficacy of biobehavioral treatment of temporomandibular disorders. J Behav Med 2001;24:341-59
- Savigny P, Watson P, Underwood M; Guideline Development Group. Early management of persistent non-specific low back pain: summary of NICE guidance. BMJ 2009;338:b1805
- The care and management of osteoarthritis in adults. London, UK: National Institute for Health and Clinical Excellence. Available at: http://www.nice.org.uk/nicemedia/pdf/CG59NICEguideline.pdf [Last accessed 17 April 2012]
- Jensen IB, Busch H, Bodin L, et al. Cost effectiveness of two rehabilitation programmes for neck and back pain patients: a seven year follow-up. Pain 2009;142:202-8
- Luk KD, Wan TW, Wong YW, et al. A multidisciplinary rehabilitation programme for patients with chronic low back pain: a prospective study. J Orthop Surg (Hong Kong) 2010;18:131-8
- Jensen MP, Turner JA, Romero JM. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J Consult Clin Psychol 2001;69:655-62
- Patrick LE, Altmaier EM, Found EM. Long-term outcomes in multidisciplinary treatment of chronic low back pain: results of a 13-year follow-up. Spine (Phila Pa 1976) 2004;29:850-5
- Hart O, McMullan J, Ritchie M, et al. NHS management of chronic pain associated with osteoarthritis and low back pain. Poster presented at the Annual Scientific Meeting of the British Pain Society in Edinburgh, June 21st to June 24th, 2011
- Fernandez M, Bell P, Davies R, et al. Management of chronic pain in secondary care pain clinics. Poster presented at the Annual Scientific Meeting of the British Pain Society in Edinburgh, June 21st to June 24th, 2011
- Survey of undergraduate pain curricula for healthcare professionals in the United Kingdom: a short report. The Pain Education Special Interest Group of the British Pain Society. The British Pain Society, London, UK, 2009. Available at: http://www.britishpainsociety.org/members_sig_edu_short_report_survey.pdf [Last accessed 8 May 2012]