

Abstract
Background:
Second-line targeted therapies for metastatic renal cell carcinoma (mRCC) include mammalian target of rapamycin (mTOR) inhibitors and tyrosine kinase inhibitors (TKIs). This study compares the effectiveness of these therapies in a multi-practice chart review and synthesizes the findings with those of a similarly designed study.
Methods:
Medical oncologists/hematologists (N = 36) were recruited to review charts for patients aged ≥18 years, received a first-line TKI and initiated second-line targeted therapy in 2010 or later. The primary outcome was time from second-line initiation to treatment failure (TTF; discontinuation, physician-assessed progression, or death, whichever occurred first). TTF was compared among patients receiving second-line everolimus (EVE), temsirolimus (TEM), or TKI as a class, using a Cox proportional hazards model adjusting for type of initial TKI and response, histological subtype, performance status, and sites of metastasis. Hazard ratios (HRs) for TTF were pooled, in a meta-analysis, with previously reported HRs for progression-free survival from a chart review with a similar design.
Results:
A total of 138, 64 and 79 patients received second-line therapy with EVE, TEM or a TKI, respectively. Adjusting for baseline characteristics, EVE was associated with numerical, but not statistically significant, reductions of 28% (HR = 0.72; 95% CI [0.45–1.16]) and 26% (HR = 0.74; 95% CI [0.48–1.15]) in the hazard of TTF compared to TEM and TKI, respectively. After pooling the HRs from both studies, EVE was associated with significantly reduced hazards of TTF compared to TEM and TKI (HR = 0.73; 95% CI [0.57–0.93]; and HR = 0.75; 95% CI [0.57–0.98], respectively).
Limitations:
Limitations include retrospective analyses with possible missing or erroneous chart data, confounding of unobserved factors due to non-randomization, and limited data for axitinib during the study period.
Conclusions:
In pooled results from two independent multi-practice chart reviews of second-line mRCC treatment, EVE was associated with significantly reduced hazards of treatment failure compared to TEM and to TKIs as a class.
Introduction
Renal cell carcinoma (RCC) is diagnosed in over 65,000 people and leads to over 13,000 deaths per year in the USCitation1. Surgical treatment is recommended for RCCCitation2, and is successful in the majority of cases. However, patients with locally advanced disease and metastases experience high rates of recurrence and disease progressionCitation3,Citation4. A third of RCC cases are diagnosed as non-localized (regional and distant) cancersCitation5, and the 5 year relative survival for metastatic RCC (mRCC) is estimated to be 12.3%Citation1. Although almost all mRCC patients experience progressionCitation6, prognosis for mRCC has significantly improved since 2005, with median overall survival extended from 10 to 40 monthsCitation7–10 following the advent of targeted therapiesCitation10–12.
Currently, seven targeted therapies are indicated for mRCC treatment in the United States: the tyrosine kinase inhibitors (TKIs) sunitinib, sorafenib, axitinib, and pazopanib, the mammalian target of rapamycin (mTOR) inhibitors temsirolimus and everolimus, and bevacizumab, a monoclonal antibody against circulating vascular endothelial growth factor (VEGF) protein, prescribed in combination with IFN-αCitation2. The targets of these therapies, the VEGF and mTOR signaling pathways, play central roles in the upregulation of angiogenesis and cellular proliferation in mRCCCitation10,Citation12–15.
When patients fail first-line therapy, due to non-response or emerging resistance or intolerance to the treatment, sequential treatment with another targeted agent is recommendedCitation16. Current NCCN guidelines based on Category 1 evidence recommend sunitinib, pazopanib and bevacizumab plus IFN-α for first-line treatment of most low- and intermediate-risk patients with clear cell mRCC (which accounts for the large majority of casesCitation2), temsirolimus for high-risk patients, and sorafenib only for selected patientsCitation2. Everolimus and axitinib are recommended for second-line therapy in patients with TKI failure, while axitinib, sorafenib, sunitinib, and pazopanib are recommended after cytokine failureCitation2. There are no third-line treatment recommendations. European guidelines (EAU) follow a similar outline, with the addition that clinical trial enrollment is recommended after mTOR inhibitor failureCitation17,Citation18. Note that, in Europe, temsirolimus is approved only “for the first-line treatment of adult patients with advanced renal cell carcinoma (RCC) who have at least three of six prognostic risk factors”Citation19.
While multiple second-line treatment options are available for mRCC, evidence for the comparative efficacy of these agents is limitedCitation7,Citation9,Citation11,Citation20–25. Due to the rapid emergence of multiple targeted agents within the past 8 years, comparative data from clinical trials is limited (and may never occur due to the cost of such trials). In addition, overall survival (OS) comparisons within clinical trials have been confounded by allowance for crossover after disease progression and differences in post-progression treatments.
The present study examined a large sample of mRCC patients who received a TKI or mTOR inhibitor for second-line treatment after prior TKI failure in real-world practice from 2010 to 2012. Patients were sampled from multiple community oncology practices throughout the US. We compared the effectiveness of everolimus, temsirolimus, and TKIs as a class (sunitinib, sorafenib, axitinib and pazopanib) by assessing the time to treatment failure (TTF) and overall survival (OS) associated with these treatments. We further assessed the comparative results by pooling findings with those of a previous chart review studyCitation26, which included treatments and outcomes from 2009 to 2011 and had a similar design, but which included different treating physicians and patients.
Methods
Sample selection
2010–2012 chart review
Community-based medical oncologists and hematologists were recruited from a nation-wide oncology network of over 4500 physicians, whose geographic coverage includes the Northeast, Southeast, Midwest, and West regions of the US. Eligible physicians were required to have access to the complete medical records of at least five metastatic RCC patients initiated on second-line therapy since January 2010, and to participate in a live meeting to review the chart data. After screening, 36 oncologists each abstracted information from the medical charts of up to 15 patients who met all the eligibility criteria, sequentially selecting the patients most recently initiating second-line treatment. Specifically, patients were required to be at least 18 years of age; to have had an mRCC diagnosis; and to have initiated second-line treatment for mRCC anytime between January 2010 and 19 June 2012. For the current analysis, we further defined the analytical sample as the subset of patients who had received a first-line TKI (sunitinib, sorafenib, axitinib or pazopanib); had discontinued first-line treatment for medical reasons (e.g., disease progression with imaging evidence, disease progression without imaging evidence, non-response without progression, drug toxicity/drug intolerance, and other medical reasons); and had been initiated on second-line targeted therapy for mRCC with everolimus, temsirolimus, or a TKI (sunitinib, sorafenib, axitinib, or pazopanib).
2009–2011 chart review
Details of the 2009–2011 chart review study have been reported in Wong et al.Citation27; this chart review study was conducted in a separate US population from the 2010–2012 study. Briefly, 159 oncologists or oncologists/hematologists (85% in community practices) were recruited from a nation-wide panel of physicians. These physicians provided chart data in an online chart review for 534 mRCC patients initiating second-line treatment treated between October 2009 and June 2010 with everolimus, sorafenib, or temsirolimus as their second targeted therapy after initial TKI failure. Outcomes were assessed up to the time of chart review (September through December 2011), or up to an earlier loss to follow-up. Up to five eligible patients were randomly selected by each physician by sequentially evaluating records for patients who last names began with a randomly generated letter.
Data elements
Similar data elements were collected in both chart review studies. These included patient demographics (age, gender), metastatic disease at the time of RCC diagnosis, first targeted therapy and response, duration of first targeted therapy, and treatments before first targeted therapy. At the time of second targeted therapy initiation, duration of mRCC, the type of RCC (clear cell RCC subtype or non-clear cell), patient comorbidities, sites of metastasis, and performance status (ECOG status, MSKCC and KPS scores) data were collected. Dates of patient death, physician-assessed progression, second-line treatment discontinuation, and last contact with the patient were also collected.
The outcomes assessed in this study included TTF and OS. TTF was defined in the 2010–2012 chart review as the time from initiation of the second targeted therapy to physician-assessed disease progression, treatment discontinuation, or death, whichever occurred first. TTF was defined in the 2009–2011 chart review as the time to progression of disease, or death from any cause at any time after initiation of the second targeted therapy (i.e. reported as PFS in the 2009–2011 study). Assessment of progression in both studies was made by participating physicians based on symptoms, radiographic, or other relevant evidence. OS was defined in both chart reviews as the time from initiation of the second targeted therapy to death from any cause. Patients without recorded death, progression, or discontinuation during the study period were censored at the last follow-up date.
In both studies a standardized case report form was designed by all study authors (M.K.W., H.Y., J.E.S., X.W., Z.L., N.S.L., C.Z.Q., and D.J.G. in the 2009–2011 study; J.E.S., N.J.V., S.K.P., P.L.L., D.J.G., M.K.W., Z.L., X.W., K.C., J.A.S., and E.J. in the 2010–2012 study), and all data extracted by the participating physicians were entered into the electronic case report forms (eCRFs) via a secure online portal. Data entries of ‘unknown/missing’ were allowed. The eCRFs were pilot tested with two physicians to ensure the interpretability of the questions and appropriate patient selection criteria and data entry. To protect patient confidentiality, all data collected in the eCRFs were de-identified in accordance with the Health Insurance Portability and Accountability Act of 1996 (HIPAA): no personally identifiable information was collected and only relative dates for clinical events were provided to investigators. The case report forms and study synopses were reviewed by the New England Institutional Review Board, which granted exemption from a full review for both retrospective, non-interventional studies of non-identifiable data.
Statistical analyses
Patient characteristics were described and compared prior to initiation of second-line therapy. Comparisons of outcomes were made among three groups: patients who received second-line everolimus, temsirolimus, or TKIs as a class (sunitinib, sorafenib, pazopanib or axitinib). The individual TKIs were grouped as a class due to the small sample sizes for each second-line TKI. A multivariable Cox proportional hazards model was used to compare the effectiveness of second-line everolimus, temsirolimus, and TKIs in terms of TTF and OS. The Cox model adjusted for baseline characteristics, including age, gender, whether the disease was metastasized at the time of RCC diagnosis, duration of mRCC, first targeted therapy and response, duration of first targeted therapy, treatments before first targeted therapy, comorbidities, sites of metastasis, number of metastatic sites, RCC histologic subtype (clear cell vs. others), ECOG status and KPS score at the time of second targeted therapy initiation. The proportional hazards assumption was verified. Adjusted hazard ratios (HRs) and adjusted median time to treatment failure for each treatment group were estimated. Due to missing values for some of the reported dates, imputation and sensitivity analyses were used to assess their impact on comparisons of TTF and OS (see Appendix A).
In the 2009–2011 study (Wong et al., 2013)Citation27, pair-wise Cox proportional hazards models were used to compare OS and PFS between everolimus and sorafenib, and between temsirolimus and sorafenib. Patients who used sorafenib as the first targeted therapy were excluded from the pair-wise comparisons of everolimus versus sorafenib and temsirolimus versus sorafenib. For pair-wise comparison of everolimus versus temsirolimus, patients who used sorafenib as the first targeted therapy were included. The Cox models adjusted for age, gender, race, whether the disease was metastasized at the time of RCC diagnosis, duration of mRCC, first targeted therapy, its duration and response, treatments before first targeted therapy, comorbidities, number and sites of metastasis, tumor characteristics (sarcomatoid differentiation, non-clear cell RCC), KPS score, physician’s year of practice and practice setting; and the proportional hazards assumption was verified.
HRs for TTF and OS from the 2010–2012 chart review study were pooled with HRs from the 2009–2011 study in a meta-analysis. Although the two study designs were largely consistent, there are some differences. First, TTF was defined in the 2009–2011 chart review as the time to progression of disease, or death from any cause at any time after initiation of second targeted therapy, while it was defined as the time to progression of disease, discontinuation of second-line therapy, or death from any cause in the 2010–2012 chart review study. Also, TKIs in the 2009–2011 chart review study included only sorafenib, while TKIs in the 2010–2012 chart review study included sorafenib, sunitinib, pazopanib, and axitinib. The meta-analysis was based on fixed-effects inverse variance weighting to obtain pooled hazard ratios for TTF and OS in pair-wise comparisons of everolimus versus temsirolimus, everolimus versus TKIs as a class, and temsirolimus versus TKIs as a class.
Results
2010–2012 chart review: patient characteristics and comparison of outcomes
Among the 433 patients who were initially diagnosed with mRCC and initiated a second-line treatment after January 2010, 281 met all of the eligibility criteria for the current analysis (). Of these, 138, 64 and 79 patients received second-line therapy with everolimus, temsirolimus or a TKI, respectively ().
Figure 1. Sample selection (2010–2012 chart review). mRCC: metastatic renal cell carcinoma; TKI: tyrosine kinase inhibitor.
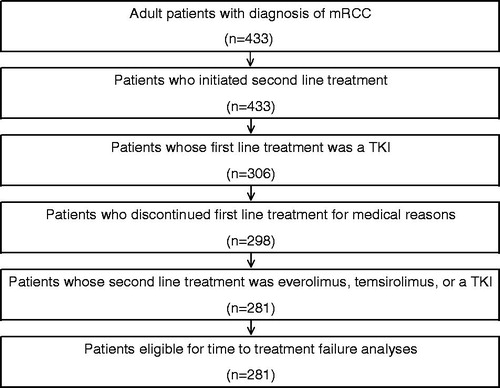
Table 1. Patient baseline characteristics (2010–2012 chart review study)a.
The majority of patients were male (65%), the mean age was 63 years, and 41% of patients had metastases at the time of RCC diagnosis. At second therapy initiation, the majority (84%) had clear cell RCC, about 41% of patients had a mean mRCC duration of 12 months or more, and the average KPS score for the study sample was 79.5 (). Hypertension (64%) and hypercholesterolemia (42%) were the most common comorbidities at second therapy initiation, and the most common sites of metastases were lung (83%), lymph node (54%), and bone (53%) (). Of the 281 patients in the analytical sample, 206 (73%) received sunitinib for first targeted therapy, 49 (17%) sorafenib, and 26 (9%) pazopanib. The mean duration of first targeted therapy was approximately 11 months, 66% of patients responded to or had stable disease with the first targeted therapy, and 84% eventually experienced disease progression while taking the first targeted therapy. During the study period, 58 deaths occurred (21% of total), and the median follow-up was 5.8 months for those on second-line everolimus or temsirolimus and 7.2 months for those on second-line TKIs ().
Table 2. Survival and follow-up time summary for second-line treatments in both (2009–2011 and 2010–2012) chart review studies.
Overall, the three second-line treatment groups (everolimus, temsirolimus, and TKIs as a class) had similar baseline characteristics, except for differences in the type of first targeted therapy, the site of metastasis at second targeted therapy initiation, and KPS at second therapy initiation. Specifically, more temsirolimus patients had received sunitinib as the first targeted therapy, while TKI patients were more likely to have received sorafenib, and everolimus patients more likely to have used pazopanib (p = 0.046). Out of the three groups, everolimus patients were the least likely and temsirolimus patients were the most likely to have bone metastasis (p = 0.027). Finally, TKI patients had a significantly better mean KPS than the two mTOR groups at the initiation of the second targeted therapy (p = 0.002).
In unadjusted analyses of outcomes, everolimus patients had the lowest rate of treatment failure among the three groups (45% of everolimus patients versus 52% for temsirolimus and 57% for TKIs). After adjusting for baseline characteristics, everolimus was associated with a 28% reduction in the hazard of second-line treatment failure compared to temsirolimus (HR = 0.72; 95% CI [0.45–1.16]; p = 0.182), though the effect was not statistically significant. Similarly, everolimus was associated with a 26% reduction in the hazard of second-line treatment failure compared to TKIs (HR = 0.74; 95% CI [0.48–1.15]; p = 0.177), though the effect was again not statistically significant. TTF differences between temsirolimus and TKI were not significant (HR = 1.02; 95% CI [0.61–1.73]; p = 0.936) (). The characteristics strongly associated with an increased risk of second-line treatment failure after first-line TKI therapy are presence of CNS metastases at the time of second targeted therapy initiation (HR = 3.56; 95% CI [1.70–7.46]; p < 0.001), and an ECOG score of 1 or more (HR = 1.91; 95% CI [1.04–3.50]; p = 0.036) (). The hazard ratios from the adjusted Cox model resulted in an adjusted median TTF of 9.1 months for everolimus and 7.2 months for both temsirolimus and TKIs.
Table 3. Adjusted comparisons of time to treatment failure and overall survival (2010–2012 chart review study)a,b.
Table 4. Multivariable Cox proportional hazards model for time to treatment failure (2010–2012 chart review).
In the unadjusted analysis, all three second-line treatments had a similar percentage of patients experiencing a death event (21% of everolimus patients versus 20% for temsirolimus and 20% for TKIs). After adjustment, everolimus was associated with a 37% reduction in the hazard of death compared to temsirolimus (HR = 0.63; 95% CI [0.30–1.31]; p = 0.212), but a 16% increase in the hazard of death compared to TKIs (HR = 1.16; 95% CI [0.55–2.42]; p = 0.700). OS differences between temsirolimus and TKI were not significant (HR = 1.85; 95% CI [0.75–4.51]; p = 0.180) (). The hazard ratios from the adjusted Cox model resulted in an adjusted median OS of 27.4 months for everolimus and 18.8 months for temsirolimus. Median OS for TKI patients was not reached ().
2009–2011 chart review: patient characteristics and comparison of outcomes
The patient sample from the 2009–2011 chart review, comprising 534 eligible patients, had similar baseline characteristics to the 2010–2012 chart review study on factors such as age (64 years), sex (70% male), and tumor histology - the majority (89%) had clear cell RCC. A similar number of patients (84%) experienced disease progression during the first targeted therapyCitation26,Citation27. In terms of disease burden profiles: 82% patients had a KPS score higher than 70%, 53% suffered from hypertension, and 58% had metastatic disease at diagnosis, with lung and bone being the most likely sites of metastasisCitation26,Citation27. On the other hand, differences in the earlier study included having more patients (86%) treated with sunitinib for first targeted therapy, and overall fewer patients (58%) responded to or had stable disease with the first targeted therapy. The mean duration of first targeted therapy for this set of patients was 7.9 months – shorter by approximately 3.1 months than that of patients treated in 2010–2012. The median follow-up was 12.9, 9.9, and 12.1 months, respectively, for 2009–2011 chart patients on second-line everolimus, temsirolimus and sorafenib.
In the 2009–2011 chart review, the number of observed deaths during the study period was 233 (43.6%), and the median study follow-up duration was 11.7 months (). The adjusted median OS for everolimus, temsirolimus and sorafenib were 19.0, 12.9 and 13.8 months, respectivelyCitation26,Citation27. The study found that everolimus treatment was associated with a 40% lower risk of death (OS HR = 0.60; 95% CI [0.42–0.85]; p = 0.004) and a 27% lower risk of progression (PFS HR = 0.73; 95% CI [0.54–0.97]; p = 0.032) than temsirolimus treatment, a numerically 25% lower risk of progression (HR = 0.75; 95% CI [0.53–1.07]; p = 0.110) and a 34% lower risk of death (OS HR = 0.66; 95% CI [0.44–0.99]; p = 0.045) than sorafenib treatment.
Synthesis of comparative effectiveness
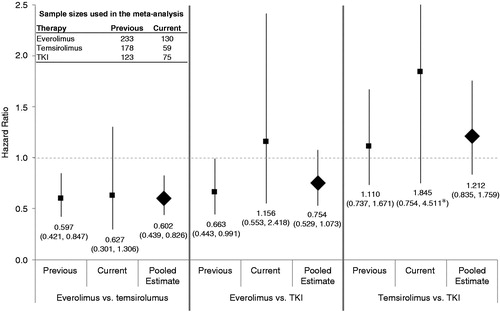
Combining results from both studies in a meta-analysis, everolimus was associated with significantly reduced hazards of treatment failure compared to temsirolimus (HR = 0.73; 95% CI [0.57–0.93]) and compared to TKI (HR = 0.75; 95% CI [0.58–0.97]) (). No difference was found in treatment failure risk between temsirolimus and TKIs (HR = 1.04; 95% CI [0.78–1.38]). For OS, the pooled HR estimates indicated that everolimus was associated with a significantly reduced hazard of death compared with temsirolimus (HR = 0.60; 95% CI [0.44–0.83]), but not statistically reduced compared with TKI therapy (HR = 0.75; 95% CI [0.53–1.07]) (). There was also no statistically significant difference in the hazard of death between temsirolimus and TKI (HR = 1.21; 95% CI [0.84–1.76]) ().
Figure 2. Meta-analysis of targeted agent effects on time to treatment failure. Fixed-effects inverse variance weighting was performed to obtain the pooled hazard ratio for each comparison of time to treatment failure. TKIs in the 2009–2011 chart review included sorafenib only, while TKIs in the 2010–2012 chart review included sorafenib, sunitinib, pazopanib, and axitinib. TKI: tyrosine kinase inhibitor.
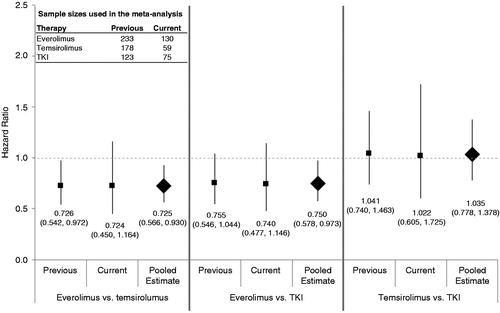
Figure 3. Meta-analysis of targeted agent effects on overall survival. Fixed-effects inverse variance weighting was performed to obtain the pooled hazard ratio for overall survival for everolimus vs. temsirolimus, everolimus vs. TKIs as a class, and temsirolimus vs. TKIs as a class. TKIs in the previous (2009–2011) dataset included sorafenib only, while TKIs in the current (2010–2012) dataset included sorafenib, sunitinib, pazopanib, and axitinib. Overall survival was defined as the time from the initiation of second targeted therapy to death from any cause. Patients without recorded death events during the study period were censored at the last follow-up date. *The upper bound of the 95% confidence interval for the hazard ratio for everolimus vs. TKI extends past the area of the graph and has been truncated for display purposes.
Discussion
Since a large proportion of mRCC patients are refractory to primary treatment with anti-angiogenic TKIsCitation28, or eventually develop resistance to first-line therapy and progressCitation16, it is important that clinicians have evidence of effectiveness for second-line treatments. While current NCCN and EAU guidelines suggest several agents for second-line treatmentCitation2,Citation17, there is no consensus on the optimal targeted agent sequence. In this study, we examined real-world patient chart data from community oncology practices in the US and assessed the comparative effectiveness of everolimus, temsirolimus, and TKIs as a class in a second-line treatment setting.
This study pooled findings from two retrospective chart reviews. The 2010–2012 chart review of patients treated in community practice identified statistically non-significant numerical trends in which everolimus was associated with reduced hazards of second-line treatment failure, compared to temsirolimus and TKIs, as well as prolonged OS when compared to temsirolimus. To further investigate the comparative effectiveness of second-line treatments for mRCC, we conducted a meta-analysis that pooled the results of the 2010–2012 analysis with those from a previous chart review study covering 2009–2011, which had a similar design but was conducted in a separate US populationCitation26. In this meta-analysis, everolimus was associated with a statistically significant reduction in the hazard of treatment failure compared to second-line temsirolimus or TKIs. The meta-analysis also demonstrated that everolimus was significantly associated with improved OS compared to temsirolimus. No statistical differences in OS were observed between everolimus and TKIs as a class in the pooled results from these two studies. However, the findings on OS should be interpreted with caution, given the following considerations: (1) some of the patient subgroups in the meta-analysis had small sample sizes (e.g., the temsirolimus group in the current chart review only included 59 patients, and the combined TKI group 75 patients); (2) the number of observed death events was small in certain subgroups of the sample, particularly in the 2010–2012 chart review; and (3) the confidence intervals for some of the pooled HRs in the OS analysis were rather wide, e.g., those for the everolimus vs. TKI, or the temsirolimus vs. TKI analysis. Further analysis with larger sample sizes is recommended to confirm the overall trends found in this study.
This study’s comparative effectiveness findings for everolimus vs. TKIs are consistent with those of other adjusted comparisons of second-line mTOR vs. TKI treatment outcomes in retrospective cohort studies. In a study of US claims data, Chen et al. (2012)Citation29 reported that second-line everolimus was associated with the lowest risk of treatment failure when compared to temsirolimus and sorafenib (HR for temsirolimus versus everolimus was 2.05; 95% CI [1.26–3.35]; p = 0.004; and HR for sorafenib versus everolimus was 1.77; 95% CI [1.02–3.07]; p = 0.043). In a global, prospectively followed cohort of mRCC patients, Heng et al. (2012)Citation30 found that a first-line VEGF inhibitor followed by a second-line mTOR inhibitor was associated with a numerically lower hazard of death when compared to treatment with a first-line VEGF TKI followed by a second-line VEGF TKI, after adjusting for the Heng prognostic score, clear cell histology, and nephrectomy status. Although the present study did not identify a statistically significant difference in OS between everolimus and TKIs, the 95% confidence interval for the hazard ratio is wide and does not indicate any inconsistency with the findings of Heng et al. Though other retrospective studies comparing the use of TKIs versus mTORs in a second-line setting existCitation24,Citation28,Citation31–34, it is not clear that the findings can be compared, due to the main limitation of sample size for these studies (and some other study design and analysis limitations – for example, Iacovelli et al. (2014)Citation34 only included patients who have received three lines of treatment, which introduced a significant selection bias).
The consistency of the comparative findings between everolimus and temsirolimus, for both TTF and OS, reported in the present study and in Wong et al. (2014)Citation27 indicate the need to consider the specific effects of these drugs, rather than considering them as a class. The numerical differences in OS for patients treated with everolimus compared to those treated with temsirolimus are notable (27.4 months versus 18.8 months, respectively), with the caveat that the 2010–2012 chart study had a short follow-up time, and relatively few deaths occurred during the study period. In a recently published phase III study by Hutson et al., second-line temsirolimus did not demonstrate a PFS advantage compared to sorafenib, and sorafenib had a significant favorable OS (HR = 1.31; 95% CI [1.05–1.63]; p = 0.01; OS 16.6 and 12.3 months, respectively)Citation35. While the Hutson et al. (2014)Citation35 study raises concerns about the use of mTOR inhibitors in the second line setting, it is clear from studies comparing the toxicity profiles of everolimus and temsirolimus that the two agents are not interchangeableCitation36,Citation37. The results of the current study lend further credence to the possibility that the two mTOR inhibitors are indeed distinctly acting agents.
Limitations
Our study is subject to several limitations inherent to retrospective analyses. In particular, there may be missing or erroneous data in the information extracted from patient records. Since this applies to all treatment groups, we do not expect missing or inaccurate data to result in systematic bias among the different treatments. Secondly, since patients were not randomized to second-line treatments, confounding due to unobserved factors is possible. In our multivariable analyses, we attempted to adjust for known risk factors that are typically recorded in charts and used to inform treatment decisions, including age, gender, ECOG, KPS, and MSKCC scores, comorbidities, metastatic sites (number and location), mRCC histological subtype (clear cell or non-clear cell), duration of mRCC, duration of first targeted therapy, prior treatments, and response to first targeted therapy. Only a well-conducted randomized trial can avoid confounding due to unobserved factors.
This study did not collect tolerability data. In addition, due to the recent approval of axitinib in 2012, limited data were available for this treatment. Furthermore, the sample sizes for each individual TKI were small and insufficient for comparisons of specific TKIs. Analyses of OS in the 2010–2012 study were also limited by small numbers of observed events, due to small sample sizes and short follow-up. This limited the precision of treatment comparisons for OS, as is evident in the wide confidence intervals for the 2012 study outcomes.
Finally, though overall study designs were similar, there were differences between the present chart analyses and the study of Wong et al., (2014)Citation27 which were pooled in the current meta-analysis. In particular, there were differences in patient populations (e.g., inclusion of academic practice settings), the specific (TKI) agents included, and the definitions of time to treatment failure. Since these differences are balanced between treatment groups within studies, they would not be expected to bias the comparative analyses, but should be considered as sources of heterogeneity when interpreting the results of the meta-analysis.
Conclusion
In a recent large-scale, practice-based chart review study of second-line treatment efficacy in mRCC patients, spanning 2010–2012, everolimus was associated with a trend for reduced hazards of second-line treatment failure and death compared to temsirolimus and TKI. In a meta-analysis combining this data with that from a similarly designed study spanning 2009–2011, everolimus was associated with significantly reduced hazards of second-line treatment failure when compared to temsirolimus and TKIs, and with decreased hazard of death when compared to temsirolimus. This study raises testable hypotheses about the impact of second-line treatments for mRCC in clinical practice.
Transparency
Declaration of funding
Research was funded by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA.
All authors participated in the design of the study and contributed to the manuscript development. J.E.S. and P.L.L. conducted analyses.
Declaration of financial/other relationships
J.E.S. and P.L.L. have disclosed that they are employees of Analysis Group Inc., a company that received funding from Novartis Pharmaceuticals Corporation to conduct this study. Z.L., X.W., and K.C. have disclosed that they are employees of Novartis Pharmaceuticals Corporation. S.K.P. has disclosed that he has been a consultant for Novartis, Pfizer, Aveo, Denelneon, and Myriad; and has spoken at Novartis, Pfizer and Medivation. N.J.V. has disclosed that he has been a consultant for Novartis, Amgen, Celgene, Medivation, Eisai, Exelixis, Roche; has spoken at Novartis, Astellas, Johnson and Johnson, Pfizer, Dendreon, Bayer/Algeta, GSK, and Veridex/Janssen; and has received research support from Novartis, Bayer, Exelixis, Progenics, Bavarian Nordic, and Viamet. D.J.G. has disclosed that he has been a consultant for Bayer, Exelixis, GSK, and Aveo as well as received grant funding from Novartis, Pfizer, GSK, Genentech, Exelixis, and BMS; and spoken at Novartis and Pfizer. E.J. has disclosed that he has been a consultant for Novartis, GSK, and Pfizer, as well as has received grant funding from Exelixis, GSK, Novartis, and Pfizer. M.K.W. and J.A.S. have disclosed that they have no significant relationships with or financial interests in any commercial companies related to this study or article.
CMRO peer reviewers on this manuscript have received an honorarium from CMRO for their review work, but have no relevant financial or other relationships to disclose.
Supplementary Material
Download PDF (12.1 KB)Acknowledgments
The authors thank Ana Bozas PhD, an employee of Analysis Group Inc., for helping with the drafting and subsequent revision of the manuscript.
References
- Howlader N, Noone A, Krapcho M, et al., eds. Cancer of the Kidney and Renal Pelvis – SEER Stat Fact Sheets. SEER Cancer Statistics Review, 1975–2010. 2010. Available at: http://seer.cancer.gov/statfacts/html/kidrp.html [Last accessed 25 June 2013]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Kidney Cancer, version 1.2013. Fort Washington, PA: National Comprehensive Cancer Network, 2013:1-35. Available at: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf [Last accessed 21 May 2013]
- Oudard S, George D, Medioni J, Motzer R. Treatment options in renal cell carcinoma: past, present and future. Ann Oncol 2007;18(Suppl 10):x25-31
- Chin AIA, Lam JJSJ, Figlin RARRA, Belldegrun AAS. Surveillance strategies for renal cell carcinoma patients following nephrectomy. Rev Urol 2006;8:1-7
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin 2013;63:11-30
- National Cancer Institute. Renal Cell Cancer Treatment (PDQ®) – Stage IV and Recurrent Renal Cell Cancer. Cancer.gov. 2013:1-8. Available at: http://www.cancer.gov/cancertopics/pdq/treatment/renalcell/HealthProfessional/page8 [Last accessed 24 June 2013]
- Iacovelli R, Cartenì G, Sternberg CN, et al. Clinical outcomes in patients receiving three lines of targeted therapy for metastatic renal cell carcinoma: results from a large patient cohort. Eur J Cancer 2013;49:2134-42
- Escudier B, Goupil MG, Massard C, Fizazi K. Sequential therapy in renal cell carcinoma. Cancer 2009;115(10 Suppl):2321-6
- Levy A, Menard J, Albiges L, et al. Second line treatment of metastatic renal cell carcinoma: the Institut Gustave Roussy experience with targeted therapies in 251 consecutive patients. Eur J Cancer 2013;49:1898-904
- Sun M, Lughezzani G, Perrotte P, Karakiewicz PI. Treatment of metastatic renal cell carcinoma. Nat Rev Urol 2010;7:327-38
- Iacovelli R, Palazzo A, Trenta P, et al. Management of metastatic renal cell carcinoma progressed after sunitinib or another antiangiogenic treatment. Am J Clin Oncol 2013: published online 5 February, 2013, doi:10.1097/COC.0b013e31827de888
- Escudier B, Albiges L, Sonpavde G. Optimal management of metastatic renal cell carcinoma: current status. Drugs 2013;73:427-38
- Clark PE. The role of VHL in clear-cell renal cell carcinoma and its relation to targeted therapy. Kidney Int 2009;76:939-45
- Audenet F, Yates DR, Cancel-Tassin G, et al. Genetic pathways involved in carcinogenesis of clear cell renal cell carcinoma: genomics towards personalized medicine. BJU Int 2012;109:1864-70
- Heldwein FL, Escudier B, Smyth G, et al. Metastatic renal cell carcinoma management. Int Braz J Urol 2009;35:256-70
- Oudard S, Elaidi R-T. Sequential therapy with targeted agents in patients with advanced renal cell carcinoma: optimizing patient benefit. Cancer Treat Rev 2012;38:981-7
- Ljungberg B, Cowan NC, Hanbury DC, et al. EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol 2010;58:398-406
- Ljungberg B, Bensalah K, Bex A, et al. Guidelines on renal cell carcinoma. European Association of Urology, 2013:1-56. Available at: http://www.uroweb.org/gls/pdf/10_Renal_Cell_Carcinoma_LR.pdf [Last accessed 13 May 2014]
- Pfizer Limited. Torisel (Temsirolimus) – Summary of Product Characteristics. European Medicines Agency (EMA), 2007:1-43. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000799/WC500039912.pdf [Last accessed 12 May 2014]
- Larkin J, Paine A, Tumur I, et al. Second-line treatments for the management of advanced renal cell carcinoma: systematic review and meta-analysis. Expert Opin Pharmacother 2013;14:27-39
- Felici A, Bria E, Tortora G, et al. Sequential therapy in metastatic clear cell renal carcinoma: TKI–TKI vs TKI–mTOR. Expert Rev Anticancer Ther 2012;12:1545-57
- Motzer RJ, Escudier B, Tomczak P, et al. Axitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: overall survival analysis and updated results from a randomised phase 3 trial. Lancet Oncol 2013;14:552-62
- Busch J, Seidel C, Kempkensteffen C, et al. Sequence therapy in patients with metastatic renal cell carcinoma: comparison of common targeted treatment options following failure of receptor tyrosine kinase inhibitors. Eur Urol 2011;60:1163-70
- Park K, Lee J-L, Park I, et al. Comparative efficacy of vascular endothelial growth factor (VEGF) tyrosine kinase inhibitor (TKI) and mammalian target of rapamycin (mTOR) inhibitor as second-line therapy in patients with metastatic renal cell carcinoma after the failure of first-line VE. Med Oncol 2012;29:3291-7
- Al-Marrawi MY, Rini BI, Harshman LC, et al. The association of clinical outcome to first-line VEGF-targeted therapy with clinical outcome to second-line VEGF-targeted therapy in metastatic renal cell carcinoma patients. Target Oncol 2013;8:203-9
- Yang H, Wong MKK, Signorovitch JE, et al. Overall and progression-free survival with everolimus, temsirolimus, or sorafenib as second targeted therapies for metastatic renal cell carcinoma: A retrospective U.S. chart review. J Clin Oncol 2012;30(Suppl):abstr 4612
- Wong MK, Yang H, Signorovitch JE, et al. Comparative outcomes of everolimus, temsirolimus and sorafenib as second targeted therapies for metastatic renal cell carcinoma: a US medical record review. Curr Med Res Opin 2014;30:537-45
- Heng DY, Mackenzie MJ, Vaishampayan UN, et al. Primary anti-vascular endothelial growth factor (VEGF)-refractory metastatic renal cell carcinoma: clinical characteristics, risk factors, and subsequent therapy. Ann Oncol 2012;23:1549-55
- Chen C-C, Hess GP, Liu Z, et al. Second-line treatment outcomes after first-line sunitinib therapy in metastatic renal cell carcinoma. Clin Genitourin Cancer 2012;10(4):256-61
- Heng DYC, Lee J, Harshman LC, et al. A population-based overview of sequences of targeted therapy in metastatic renal cell carcinoma (mRCC). J Clin Oncol 2012;30(suppl 5):abstr 387
- Vickers MM, Choueiri TK, Rogers M, et al. Clinical outcome in metastatic renal cell carcinoma patients after failure of initial vascular endothelial growth factor-targeted therapy. Urology 2010;76:430-4
- Pasini F, Fraccon AP, Barile C, et al. Targeted therapies (TT) in metastatic renal cell carcinoma (mRCC): an Italian survey of 902 pts. J Clin Oncol 2013;31(Suppl):abstr e15514
- Busch J, Seidel C, Erber B, et al. Retrospective comparison of triple-sequence therapies in metastatic renal cell carcinoma. Eur Urol 2013;64:62-70
- Iacovelli R, Cartenì G, Milella M, et al. Clinical outcomes in patients with metastatic renal cell carcinoma receiving everolimus or temsirolimus after sunitinib. Can Urol Assoc J 2014;8:E121-5
- Hutson TE, Escudier B, Esteban E, et al. Randomized phase III trial of temsirolimus versus sorafenib as second-line therapy after sunitinib in patients with metastatic renal cell carcinoma. J Clin Oncol 2014;32:760-7
- Soulières D. Side-effects associated with targeted therapies in renal cell carcinoma. Curr Opin Support Palliat Care 2013;7:254-7
- Atkinson BJ, Cauley DH, Ng C, et al. Mammalian target of rapamycin (mTOR) inhibitor-associated non-infectious pneumonitis in patients with renal cell cancer: predictors, management, and outcomes. BJU Int 2014;113:376-82