

Abstract
Objective:
This review provides an overview of therapeutic options, with a specific focus on the emerging role of medical options for UF management.
Research design and methods:
PubMed, Google Scholar, and Cochrane Systematic Reviews were searched for articles published between 1980 and 2013. Relevant articles were identified using the following terms: ‘uterine fibroids’, ‘leiomyoma’, ‘heavy menstrual bleeding’, and ‘menorrhagia’. The reference lists of articles identified were also searched for other relevant publications.
Results:
Because of the largely benign nature of UFs, the most conservative options that minimize morbidity/risk and optimize outcomes should be considered. Watchful waiting, or no immediate intervention combined with regular follow-up, is an appropriate option for the majority of UF patients who experience no symptoms. For women with symptomatic UFs, the optimal treatment should restore quality of life through rapid relief of UF signs and symptoms, reduce tumor size for a sustained period, and maintain or improve fertility. Invasive surgical treatments, such as hysterectomy, have historically been the mainstay of UF treatment. Less invasive surgical and interventional techniques, such as myomectomy, uterine artery embolization, endometrial ablation, and myolysis provide alternatives to hysterectomy. Until recently, medical management of UFs was characterized by short-term treatments and therapies that provided symptomatic control. In addition to controlling abnormal uterine bleeding, newer medical therapies, including the recently Health-Canada-approved ulipristal acetate, act directly to shrink the tumor. Although no agent is currently approved for such use, emerging evidence suggests the potential for long-term medical management of UFs.
Conclusions:
The advent of novel medical therapies may diminish the long-held reliance on more invasive surgical UF treatment options.
Introduction
Uterine fibroids (UFs) or leiomyomas are benign tumors that originate from the smooth muscle of the uterus and represent the most common tumor of the female reproductive tractCitation1. UFs affect women of reproductive age and tend to regress following menopauseCitation2,Citation3. Among affected women, UFs can cause significant morbidity, including heavy and/or prolonged menstrual bleeding, pelvic pressure or pain, and possibly reproductive dysfunction; these symptoms can lead to absenteeism and decreased productivity in the workplace, and impairment in activities of daily livingCitation4. However, many women with UFs are asymptomatic, or their symptoms may develop so gradually that they do not think to report them to a physicianCitation5. Hence, UFs may remain undiagnosed unless discovered incidentally during clinical or radiological examinations.
Estimates of UF prevalence are difficult to establish and vary widely according to the method of assessment; those based on self-report tend to bias toward symptomatic cases and are significantly lower than those based on imaging or histological examination. For instance, the self-reported prevalence of UFs among women aged 20–54 years who participated in a national US survey was 12%Citation6. Similarly, only 5.5% of the 2514 Canadian women aged 15–49 years surveyed reported being diagnosed with UFs by their physicianCitation7. However, over half of women with no prior diagnosis of UFs show evidence of UFs during ultrasound imagingCitation5, and detailed analysis of hysterectomy specimens indicates a true UF prevalence as high as 77%Citation2.
Surgical intervention (hysterectomy and myomectomy) has historically been the mainstay of UF treatment. UFs remain the commonest indication for hysterectomy in Canada, accounting for 30% of these proceduresCitation8,Citation9. While hysterectomy provides a definitive cure for UFs, it does so at the expense of future fertility. For women who wish to preserve fertility, myomectomy represents a surgical alternative. If done by laparotomy (the most common approach), both surgical approaches are associated with substantial morbidity and may require postoperative hospital stays of 3–6 days, as well as an extended convalescence periodCitation10,Citation11. Although rarely serious, complications with the laparotomy approach, such as pyrexia and wound complications, can be relatively commonCitation10. Less invasive surgical options are available, such as uterine artery embolization (UAE), endometrial ablation, and myolysis, although access to these procedures may be limited in some regions. Medical management using hormone-based preparations (e.g., oral contraceptives, levonorgestrel-containing intrauterine systems [IUSs], and gonadotropin-releasing hormone [GnRH] agonists) is possible. While these therapies provide varying degrees of control of abnormal uterine bleeding, most do not act directly on the fibroid. In the recent past, the off-label use of GnRH agonists with or without hormonal add-back therapy has been the de facto standard of care. In 2013, ulipristal acetate, a once daily oral agent, became the first approved medical treatment for UFs in CanadaCitation12. Other therapies are being investigated in clinical trials, as discussed below. These additions to the gynecologists’ arsenal are poised to alter the way women with UFs are treated, potentially reducing the reliance on surgical intervention.
Here, we provide an overview of evaluation, diagnosis, and therapeutic options, with a specific focus on the emerging role of medical treatment of UFs.
Methods
Multiple databases including PubMed, Google Scholar, and Cochrane Systematic Reviews were searched for articles published between 1980 and 2013. Relevant articles were identified using the following MeSH terms: ‘uterine fibroids’, ‘leiomyoma’, ‘heavy menstrual bleeding’, and ‘menorrhagia’. The reference lists of articles identified were also searched for other relevant publications. The ClinicalTrials.gov website was searched to identify ongoing trials of medical therapies for UFs. Discussion was limited to treatment options available to Canadian clinicians.
Pathophysiology
UFs are of monoclonal origin, arising from a single neoplastic cell in the myometriumCitation13. The early steps in UF development are not well understood. As illustrated in , mutations in certain candidate genes are common in UF tissue; epigenetic changes also play a role, as do sex hormones and other soluble factors, as well as biochemical changes in the UF extracellular matrixCitation14. Half of UFs carry identifiable chromosomal abnormalities, commonly t(12;14) or del(7)(q22q32)Citation15,Citation16,Citation17, but it is not clear when in UF pathogenesis these alterations occurCitation18.
Figure 1. Factors involved in UF formation and growth. Adapted from Islam et al. 2013Citation14.
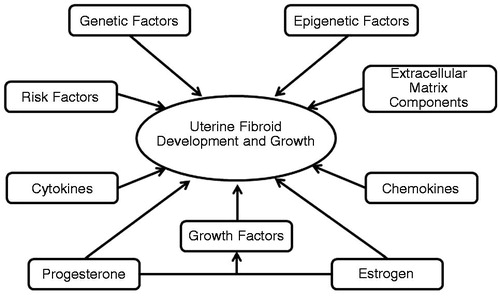
UF growth depends on both progesterone and estrogenCitation19,Citation20, whose actions are partly mediated by growth factors, cytokines, and chemokinesCitation21. The primary role of estrogen in UF growth is to enable tissue to respond to progesterone, by inducing the expression of progesterone receptorsCitation22. The concentration of estrogen and progesterone receptors appears to be significantly higher in UFs in comparison with healthy myometriumCitation23–25 and is positively correlated with the rate of growth of UFsCitation26. Interestingly, progesterone appears to selectively increase the proliferative activity of UF cells but not of normal myometrial cellsCitation27. The molecular basis of this effect is a matter of speculationCitation28,Citation29.
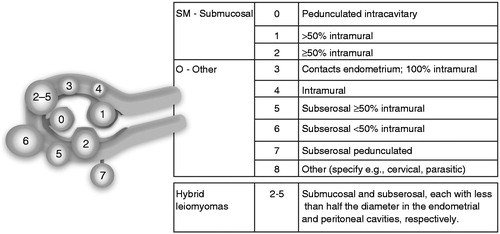
UFs may be solitary but are often multiple, and can range in size from microscopic to massive, sometimes expanding the uterus to fill the abdominal cavityCitation30. The location of UFs plays a role in determining the type and severity of symptoms experienced. UFs can be classified into three subgroups based on their location within the layers of the uterus: intramural (within the myometrium), subserosal (projecting to the outside of the uterus, below the uterine serosa), and submucosal (projecting to the inner cavity of the uterus, located beneath the endometrium). A detailed classification system for causes of abnormal uterine bleeding proposed by Munro and colleaguesCitation31 includes a detailed UF subclassification system based on tumor location ().
Figure 2. Uterine fibroid subclassification within the FIGO abnormal uterine bleeding classification system. Intracavitary lesions are attached to the endometrium by a narrow stalk and are classified as Type 0, whereas Types 1 and 2 require a portion of the lesion to be intramural – with Type 1 having less than 50% involvement and Type 2 at least 50%. Type 3 lesions are totally extracavitary but abut the endometrium. Type 4 lesions are intramural UFs that are entirely within the myometrium, with no extension to the endometrial surface or to the serosa. Subserosal (Types 5–7) UFs represent the mirror image of the submucosal UFs – with Type 5 being at least 50% intramural, Type 6 less than 50% intramural, and Type 7 attached to the serosa by a stalk. An additional category, Type 8, is reserved for UFs that do not relate to the myometrium at all, and would include cervical lesions, those that exist in the round or broad ligaments without direct attachment to the uterus, and other so-called ‘parasitic’ lesions. Hybrid UFs are transmural and are classified by their relationship to both the endometrial and serosal surfaces. Two numbers are separated by a hyphen (e.g., 2–5); the first refers to the relationship with the endometrium, while the second refers to the relationship with the serosa. Reprinted with permission from Munro et al., 2011Citation31.
Risk factors
Risk of UF development is affected by numerous factors (). Self-reported prevalence of UFs increases with age, peaking among women in their 30 s (7.0%) and 40 s (14.1%)Citation7. African American women are two to three times more likely to develop UFs than Caucasian womenCitation32,Citation33. Women of African descent also present with a higher number of fibroids, have a longer average duration of disease, and experience greater severity of symptomsCitation34. Nulliparous women are also at increased risk of developing UFsCitation35, as are those with early menarche or a family history of UFsCitation36,Citation37 and those with specific clinical conditions, such as hypertension or diabetesCitation38,Citation39.
Table 1. Factors associated with the risk of uterine fibroids.
Signs and symptoms
The majority of women with UFs experience no symptoms, or their symptoms may develop so gradually that they do not think to report them to a physicianCitation5. Among those women who develop complications resulting from UFs, symptoms are influenced by the size, number, and location of the tumor. Abnormal uterine bleeding and pelvic pressure are the two most common symptoms leading women to seek medical treatmentCitation7. Specifically, heavy and prolonged menstrual bleeding are reported by 59.8% and 37.3% of women with a UF diagnosis, respectivelyCitation7. Frequently, these symptoms can lead to the development of iron-deficiency anemiaCitation40. Symptoms may be related to pressure exerted by the tumor on adjacent organs, such as the bladder, the ureters, or the bowel. Such ‘bulk symptoms’ include bladder pressure, pelvic pain, painful sexual intercourse, urinary frequency, incontinence, nocturia, and constipationCitation1,Citation7. While submucosal fibroids are plausibly linked with impairment of fertility, the effect of intramural or subserosal fibroids on pregnancy loss or reduced fertility is hotly debatedCitation41–43.
UF symptoms are often detrimental to a woman’s quality of life. In one study, 53.7% of surveyed women with UFs reported a negative impact of their symptoms, influencing their sexual life (42.9%), performance at work (27.7%), and relationships and family (27.2%)Citation7. Symptoms can lead to embarrassment (e.g., uncontrolled bleeding episodes in public places and appearance of pregnancy), pain during intercourse, limited ability to exercise, interruption in work, and sleep disturbanceCitation34. Most worrisome is the finding that women with symptoms of pain and/or bleeding due to benign uterine conditions such as UFs report poorer emotional well-being than women with major chronic health conditions such as diabetes and heart diseaseCitation44.
Diagnosis
At presentation, women may report abnormal menstrual bleeding or bulk symptoms, or they may have laboratory findings or clinical signs or symptoms of anemia. Because such symptoms may worsen steadily over many years, self-report is inconsistent. Most UFs are discovered during routine pelvic examination or incidentally during imaging, the typical sign being an enlarged uterus with an irregular contourCitation45. Suspected UFs should be distinguished from other pelvic masses and characterized in terms of location, size, and number. Imaging techniques, including transvaginal and abdominal ultrasonography, sonohysterography, hysterosalpingography, hysteroscopy, and magnetic resonance imaging (MRI), are helpful in this regard. Pre-intervention mapping of fibroids to determine location and size, as per the FIGO guidelinesCitation31, is a key step in therapeutic counseling of women with UFs.
Nearly all UFs are benign; malignant leiomyosarcoma are found in <0.25% of surgically removed stable or rapidly enlarging fibroidsCitation46. Between 1979 and 2001, the incidence of leiomyosarcoma in the United States has been estimated at 0.36 per 100,000 woman-yearsCitation47. Despite the low absolute risk, all UFs should be suspected of potential malignancy. Unfortunately, there are no reliable preoperative techniques to discriminate between benign and malignant lesionsCitation48,Citation49. Signs that may indicate a potential leiomyosarcoma include lack of tumor response to medical therapy, and rapid or post-menopausal tumor growth. Certain radiologic findings (e.g., large size, tissue signal heterogeneity, central necrosis, and ill-defined margins) may be associated with leiomyosarcomas, but these can also be seen in benign UFsCitation50.
Management: overview
The ideal treatment for UFs should satisfy three goals: relief of signs and symptoms, sustained reduction of fibroid size, and maintenance or improvement of fertility. In addition, treatment should improve quality of life, have minimal side effects, be convenient for patients, and directly target fibroids without systemic unintended effects. As summarized in , various surgical and medical options are available for managing symptomatic UFs, but none has been clearly shown to satisfy all of these goals, largely because it is difficult to exclude possible effects on fertility.
Table 2. Summary of treatment options for uterine fibroids.
provides a general treatment algorithm for UFs, listing common therapeutic options. Because of the largely benign nature of UFs, the most conservative options that minimize morbidity/risk and optimize outcomes should be considered. Watchful waiting – that is, no immediate intervention, combined with regular follow-up – is an appropriate option for the majority of UF patients who experience minimal symptoms.
Figure 3. Uterine fibroid treatment algorithm. Please refer to for advantages and disadvantages of the different therapeutic approaches.
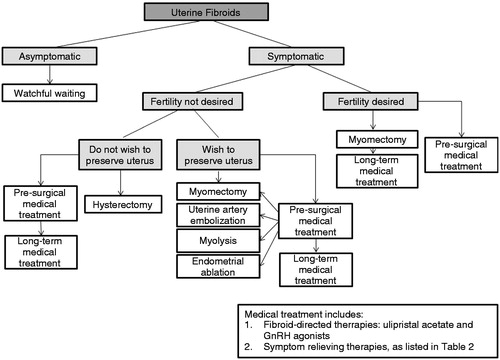
The first consideration in the management of patients with symptomatic UFs is the determination of the patient’s wish for future fertility. Many women are deferring childbearing to later in their reproductive yearsCitation51 when UF symptoms become most pronouncedCitation7. As a result, the demand for therapeutic options that preserve the uterus are becoming increasingly more relevant. Finally, hysterectomy is reserved for the patient who wants a definitive cure of UF symptoms, does not desire to preserve her fertility, and has no preference for retaining her uterus. Medical therapy can be used to prepare the patient for surgical intervention (discussed below), or in continuous or intermittent long-term management.
Treatment options
Watchful waiting
Since medical treatment is mainly geared toward alleviation of signs and symptoms, it is considered unnecessary for women with asymptomatic UFsCitation52. There is also insufficient evidence to substantiate the use of surgical interventions, such as hysterectomy, in asymptomatic UFsCitation53,Citation54. Finally, watchful waiting may be particularly useful among women approaching menopause, since there is limited time to develop new symptoms, bleeding stops and UFs naturally regress following menopauseCitation55.
Medical therapy
Selective progesterone receptor modulators
Ulipristal acetate is indicated for the treatment of moderate to severe signs and symptoms of UFs in adult women of reproductive age who are eligible for surgeryCitation12. As per the Health Canada indication, the duration of treatment is limited to 3 months of continuous use. Ulipristal acetate is an orally administered agent that belongs to the group of selective progesterone receptor (PR) modulators (SPRMs), progesterone-receptor ligands whose biological activity is tissue selectiveCitation56. On binding to the PR in target tissues, ulipristal acetate displays antagonist and partial agonist effectsCitation57. Ulipristal acetate does not activate proliferation of healthy uterine tissue and, unlike progestins, it actively suppresses mammary cell proliferation in preclinical studiesCitation56. In UF tissue, this SPRM induces a number of desirable changes, including a suppression of neovascularization and cell proliferation, as well as induction of apoptosisCitation58.
The efficacy of ulipristal acetate has been demonstrated in three European phase III studies (PEARL I, II, and III)Citation59–61. PEARL I compared treatment for up to 13 weeks with ulipristal acetate at 5 mg or 10 mg/day versus placebo in patients with UFs, heavy menstrual bleeding, and anemia. In this trial, uterine bleeding was assessed using the pictorial blood-loss assessment chart (PBAC), which ranges from 0 to >500 (with no defined upper limit), with higher scores indicating greater severity of bleeding. Approximately 50% of patients in the 5 mg ulipristal acetate group and 70% in the 10 mg group became amenorrheic within the first 10 days of treatment. At 13 weeks, uterine bleeding was controlled (defined as a score of less than 75 on the PBAC) in nearly all patients receiving ulipristal acetate (91% with 5 mg and 92% with 10 mg), but only in 19% of the women receiving placeboCitation60. Median changes in MRI-assessed total fibroid volume in response to 5 mg and 10 mg ulipristal acetate and placebo were −21%, −12%, and +3%, respectively.
PEARL II was a double-blind, non-inferiority trial that compared 3 months of daily therapy with ulipristal acetate (5 mg or 10 mg) and once monthly intramuscular injections of the GnRH analog leuprolide acetate (3.75 mg). At 3 months, uterine bleeding was controlled (defined as a score of less than 75 on the PBAC) in an equal proportion of patients receiving ulipristal acetate 5 mg and 10 mg and leuprolide acetate (90%, 98%, and 89%, respectively); however, bleeding was controlled significantly sooner among patients receiving either dose of ulipristal acetate than those receiving leuprolide acetateCitation59. Indeed, median times to amenorrhea in patients receiving 5 mg of ulipristal acetate, 10 mg of ulipristal acetate, and leuprolide acetate were 7, 5, and 21 days, respectively. Amenorrhea was reversed after an average of 31 to 34 days following treatment discontinuation with ulipristal acetate. Uterine volume change was significantly smaller with either dose of ulipristal acetate than with leuprolide acetate (−20% and −22% vs. −47% respectively). However, as determined by ultrasound, median volume change in the three largest UFs were similar between treatment groups (−36%, −42%, and −53%, respectively)Citation59.
In a prespecified exploratory analysis of PEARL II, ulipristal acetate was found to produce a more prolonged UF volume reduction by comparison to leuprolide acetate. Specifically, UFs began to enlarge by 1 month following the last dose of leuprolide acetate, whereas fibroid reduction was maintained in most patients at 6 months following cessation of ulipristal acetate treatmentCitation59. This evidence suggested the possibility of long-term medical management of UFs, achieved by alternating ulipristal acetate treatment cycles with treatment-free periods.
Such an approach was tested in the long-term, open-label, PEARL III extension trial, in which 209 women with symptomatic UFs received up to four 3 month courses of ulipristal acetate 10 mg daily, each separated by an off-treatment periodCitation61. Every off-treatment period included a full menstrual cycle up to the start of the second menstruation. By the end of the first ulipristal acetate treatment course 78.5% of women became amenorrheic; this rate rose to 88.5%, 88.2%, and 89.7% following the second, third, and fourth treatment courses, respectivelyCitation61. Similarly, while the first ulipristal acetate treatment course resulted in a 45.1% median reduction in the combined volume of the three largest UFs, women who underwent four treatment courses showed a median volume reduction of 72.1%. These results highlight the potential for long-term management of UFs using medical therapy, which, in some cases, could eliminate the need for surgical intervention.
The most commonly reported adverse events associated with ulipristal acetate treatment included headache and breast tenderness, both of which occurred in a similar proportion of placebo-treated patientsCitation60. Among women receiving multiple 3 month courses of ulipristal acetate in the long-term PEARL III study, the incidence of adverse events did not increase with successive treatment coursesCitation61. In contrast to leuprolide acetate monotherapy, treatment with ulipristal acetate was associated with maintenance of estradiol levels within the mid-follicular rangeCitation59. Consequently, ulipristal acetate treatment was associated with a lower prevalence of menopausal symptoms, such as hot flashes, and no evidence of increased bone resorptionCitation59. Thus, unlike GnRH agonists, ulipristal acetate does not require concurrent hormonal add-back therapy.
As with other SPRMs, ulipristal acetate is associated with the development of apparently benign, non-physiological endometrial changes, termed progesterone-receptor-modulator-associated endometrial changes (PAEC), in over half of treated patients (range: 57–62%)Citation59,Citation60. These endometrial changes, which are associated with cystic glandular dilatationCitation62, appear to be fully reversible within 6 months of discontinuing treatmentCitation60. Additionally, treatment duration and cumulative dose of ulipristal acetate does not appear to influence the development of PAEC; when measured approximately 6 weeks following the end of the first and fourth 3 month treatment course, the rates of PAEC were nearly identical (26% and 25%, respectively)Citation61.
The PEARL III study investigated the impact of a 10 day course of progestin norethisterone acetate (NETA) on the incidence of PAEC, as well as on the timing and magnitude of the next menstruation during the off-treatment periodCitation61. By comparison to placebo treatment, NETA was associated with a significantly reduced magnitude of menstrual bleeding and also expedited the return of menstrual bleeding in the off-treatment period. Specifically, women receiving NETA experienced the return of menstrual periods after a median of 15 days following the end of the fourth ulipristal acetate treatment course, by contrast to 30 days among women receiving placebo (p < 0.001). However, NETA treatment had no impact on the incidence of PAECCitation61.
Mifepristone is another SPRM that has been extensively researched but is not yet available in Canada for the treatment of UF. Various doses of mifepristone (2.5–50 mg) have been tested in the treatment of UFs, with reported reduction of UF size of up to 57% by 3 months of therapyCitation63,Citation64. As with ulipristal acetate, mifepristone therapy is associated with the development of PAECCitation64,Citation65. Long-term follow-up is needed to confirm the safety and efficacy of this agent.
Gonadotropin-releasing hormone agonists
In the US, GnRH agonists have been approved for short-term pre-surgical treatment of UFs since 1999; in Canada they continue to be widely used in patients proceeding to surgical intervention or being managed medically. During the first week or two of treatment, patients may experience a flare of symptoms due to the initial increase of follicle-stimulating hormone and corresponding rise in estradiolCitation66; this trend is subsequently reversed, leading to a markedly hypogonadal state. Within 3 to 6 months of treatment, GnRH agonists cause a significant reduction in UF volume (30–50%) and an improvement in UF-related symptomsCitation59,Citation67,Citation68,Citation69.
GnRH agonist monotherapy has been associated with side effects that may limit its acceptability for long-term use. Because of the production of a marked hypoestrogenic state, patients often experience menopausal symptoms, such as hot flashes, vaginal dryness, mood changes, and reduced bone densityCitation70. Accordingly, patients may receive hormonal add-back therapy concurrently with leuprolide acetate in an effort to offset these symptoms. This combination therapy may allow long-term treatment, as has been shown in endometriosis managementCitation71. Finally, fibroids treated with GnRH agonists typically regrow within 3 months following cessationCitation59,Citation68,Citation72.
Other
Other medical options, not specifically indicated for treating UFs, are sometimes used to control heavy menstrual bleeding or other symptoms. These include oral contraceptives, levonorgestrel-releasing intrauterine systems (LNG-IUSs), antifibrinolytics, non-steroidal anti-inflammatory drugs (NSAIDs), and danazol. Oral contraceptives may be used to reduce heavy menstrual bleeding associated with UFs over the short termCitation52. Additionally, limited evidence suggests that oral contraceptive use may reduce the risk of developing UFsCitation35,Citation73. Similarly, small studies show that the LNG-IUSs can reduce bleeding and improve hemoglobin levels in women with heavy menstrual bleeding caused by UFsCitation74. In this regard, the LNG-IUSs are superior to other medical treatments, such as NSAIDs and antifibrinolyticsCitation75. Tranexamic acid is a non-hormonal antifibrinolytic agent that helps to reduce menstrual blood loss by 30% to 59%Citation76–78, but is associated with an elevated risk of UF necrosis and intralesional thrombosisCitation79. NSAIDs have been shown to reduce menstrual blood loss by 33% to 55% by comparison to placeboCitation80, but they are less effective in objectively reducing menstrual bleeding than other medical optionsCitation52,Citation76. While danazol has been shown to reduce UF symptoms in the short-term, it is less effective than GnRH agonists and is associated with significantly more adverse effects than other medical therapies, including weight gain, acne, and androgenic effectsCitation52,Citation81.
Future options
Various other therapeutics are currently being studied for potential treatment of UFsCitation14. Aromatase inhibitors, including letrozole, anastrozole, and fadrozole, are a class of agents that block the synthesis of estrogen. Aromatase inhibitors have been shown to readily reduce UF size (up to 71% in 2 months)Citation82 and ameliorate UF symptoms, including a reduction in menstrual volume and duration of menstruation, and urinary retentionCitation82–84. The most common side effects of aromatase inhibitors include hot flashes, vaginal dryness, and musculoskeletal painCitation14. GnRH antagonists that have been studied in treating UFs include cetrorelix acetate and ganirelix; both agents are available in Canada for other indications but are rarely used to treat UFs. By contrast to GnRH agonists, which act by inducing GnRH receptor down-regulation, GnRH antagonists compete with endogenous GnRH for pituitary binding sites. Limited evidence suggests that these agents lead to a rapid reduction in UF size (e.g., 31.3% reduction by 14 days of treatment) that is unaccompanied by a flare-up in gonadotropin secretion commonly seen with initiation of GnRH-agonist therapyCitation85–87. A phase III study of vilaprisan (BAY 1002670/15788), an alternative SPRM, is set to begin recruiting in Europe (EudraCT Number: 2013-003945-40). Studies of other GnRH antagonists, such as elagolix, are currently ongoing (ClinicalTrials.gov identifier: NCT01441635). Since the use of GnRH antagonists leads to a hypoestrogenic state, hormonal add-back is necessaryCitation85. The selective estrogen receptor modulator (SERM) raloxifene has also been investigated in the treatment of symptomatic UFs; however, the few studies that are available are of low quality and provide inconsistent resultsCitation88.
Pre-surgical medical approaches
Optimizing a patient’s physical and mental condition is an important goal in preparation for significant gynecological interventions. Medical treatments are often used to control bleeding, shrink UFs, reduce uterine volume, and increase the hemoglobin level prior to surgeryCitation54. Ulipristal acetate is currently indicated in Canada for use in women who are eligible for surgery, while leuprolide acetate is used, as stated in its US indication, for the preoperative improvement of anemia due to heavy menstrual bleeding caused by UFsCitation66. Timing of medical administration is more critical with GnRH agonists due to the well documented regrowth of fibroids within 3 months; ulipristal acetate treatment produces persistent tumor shrinkage beyond this time. Preoperative use of GnRH agonists is associated with a softening of the UF and destruction of tissue planes for myomectomyCitation89,Citation90; it is unclear whether pre-surgical use of ulipristal acetate is associated with the same drawback.
Surgical and interventional approaches
Minimally invasive surgical and interventional approaches for UF treatment include uterine artery embolization (UAE), endometrial ablation, and myolysis. UAE is most commonly accomplished by the injection of occluding agents into one or both of the uterine arteries, effectively limiting blood supply to the uterus and UFs. The procedure is performed by interventional radiologists while the patient is awake. UAE should be considered for women with symptomatic UFs who might otherwise be advised to undergo surgeryCitation91, although some have cautioned against the use of UAE in patients with solitary submucosal or pedunculated subserosal UFs because of the risk of complicationsCitation52. According to a Canadian multicenter study of over 500 patients, UAE results in a 42% mean reduction in the size of the dominant UF, a 35% reduction in uterine volume, and improvements in UF symptoms among 77% to 86% of patients at 3 monthsCitation92. By comparison to hysterectomy and myomectomy, UAE is associated with similar patient satisfaction, a shorter hospital stay, a faster return to normal activity, but a higher rate of minor complicationsCitation93. Long-term studies indicate a reoperation rate of 20% to 33% within 1.5 to 5 years of UAECitation94–96. While successful pregnancies can occur following UAECitation97, complications with abnormal placentation have been describedCitation98.
Endometrial ablation (i.e., transcervical destruction of the uterine endometrium using electrosurgery, heat, laser, radiofrequency or other approaches) is used mainly to manage heavy uterine bleeding and is limited to women with a normal-sized uterus and UFs <3 cm in diameterCitation99. By comparison to hysterectomy, endometrial ablation is associated with shorter intraoperative time, shorter convalescence period, and fewer adverse events, but inferior reduction in menstrual bleeding and lower patient satisfactionCitation100. Due to the high risk of miscarriage, ectopic pregnancy, and invasive placental disorders, pregnancy following endometrial ablation is not recommendedCitation52,Citation99. Effective contraception is advised, and sterilization should be consideredCitation52. Over time, the endometrial lining may grow back in some women, requiring repeated treatmentCitation99.
Myolysis (i.e., the destruction of the UF and/or its blood supply via ultrasound, laser, cryotherapy, or other methods) has been suggested as a conservative alternative to myomectomy or hysterectomy for women with symptomatic intramural or subserous fibroids who want to preserve their uterus but not fertilityCitation53. Candidates for myolysis include women with a maximum of three small UFs (≤5 cm or largest UF is <10 cm in diameter)Citation53. As the integrity of the uterine wall post-myolysis may be compromised, potentially leading to uterine rupture during pregnancyCitation101, myolysis is not recommended for women who wish to become pregnant in the futureCitation53. Of the available myolysis techniques, magnetic-resonance-guided focused ultrasound surgery (MRgFUS) appears to be the most effective and least aggressiveCitation52 and has been found to reduce UF symptoms among 71% and 51% of women at 6 and 12 months postprocedure, respectivelyCitation102,Citation103. The widespread adoption of this technique may be limited by the need for costly, specialized equipment, and limited data on efficacy and safetyCitation52. Finally, since the preoperative identification of malignant lesions remains an ongoing challenge, a patient for whom surgery is under consideration should be informed of the rare possibility that her UF may, in fact, be a leiomyosarcoma.
Myomectomy is the surgical removal of select UFs and reconstruction of the uterus. Myomectomy, if done by laparotomy, may be associated with postoperative complications among many patients; however, the vast majority of these complications, such as pyrexia (reported by 33.5% of patients), are rarely seriousCitation10. Although most myomectomies were originally performed by laparotomy, endoscopic options (laparoscopy/hysteroscopy) are associated with reduced blood loss, reduced patient pain and analgesic use, and a quicker recoveryCitation104. However, laparotomy may be preferred for UFs that are larger, more numerous, or intramurally locatedCitation53,Citation54. An estimated 15% and 33% of UFs recur following myomectomy via a laparotomy or laparoscopy, respectivelyCitation105,Citation106. Approximately 10% of women undergoing myomectomy will require a hysterectomy within 5 to 10 yearsCitation106. Rarely, intraoperative complications during myomectomy necessitate an unplanned hysterectomyCitation107.
Hysterectomy provides a definite cure for women with symptomatic UF who do not wish to preserve their fertilityCitation53. In Canada, UFs represent the main indication for hysterectomyCitation8. This procedure is associated with near complete resolution of symptoms and an improved quality of lifeCitation108,Citation109. However, approximately one in 10 women may experience new symptoms following hysterectomy, including hot flashes, weight gain, depression, and decreased sexual driveCitation109. At least some of these symptoms, namely hot flashes, may be explained by the concurrent oophorectomy that is performed on many womenCitation109.
Conclusion
Although many women with UFs may be free of symptoms and require no immediate intervention, those who develop symptoms can experience significant morbidity and a deterioration of their quality of life. The goals of UF therapy include the restoration of quality of life through rapid relief of UF signs and symptoms, sustained reduction in tumor size, and maintenance or improvement of fertility. Because of the largely benign nature of UFs, the most conservative options should be considered first. Unfortunately, invasive surgical treatments have long been the mainstay of UF treatment. While prior medical management of UFs, characterized by various off-label treatments, provided symptomatic control, most patients eventually received some form of surgical treatment. The maturation of medical UF management is a hopeful sign, with clinical studies on various investigational therapeutics, and most recently, the arrival of ulipristal acetate, the first Health-Canada-approved medication for the treatment of UF. Although the current indication for ulipristal acetate is the short-term treatment of women with UFs who are eligible for surgery, recent evidence suggests the agent may hold potential utility in the long-term management of UFs. It is hoped that, along with continued use of minimally invasive surgical approaches, the introduction of new medical therapies for UF will reduce reliance on hysterectomy and other invasive treatment options.
Transparency
Declaration of funding
Editorial support for this review was funded by Actavis Canada.
Declaration of financial/other relationships
S.S.S. has disclosed that he is on the speaker bureau for Abbvie Corporation, Actavis, Bayer Canada, and Ethicon Endosurgery. He also has ongoing research grants with Abbvie Corporation. L.B. has disclosed that she is on the speaker bureau for Abbvie Corporation, Actavis, Bayer Canada and Olympus Canada.
Acknowledgments
The authors thank Actavis Canada for their support of this project from its inception and also Peter Janiszewski PhD and John Ashkenas PhD, both of SCRIPT in Toronto, ON, for editorial assistance.
References
- Evans P, Brunsell S. Uterine fibroid tumors: diagnosis and treatment. Am Fam Physician 2007;75:1503-8
- Cramer SF, Patel A. The frequency of uterine leiomyomas. Am J Clin Pathol 1990;94:435-8
- Fields KR, Neinstein LS. Uterine myomas in adolescents: case reports and a review of the literature. J Pediatr Adolesc Gynecol 1996;9:195-8
- Downes E, Sikirica V, Gilabert-Estelles J, et al. The burden of uterine fibroids in five European countries. Eur J Obstet Gynecol Reprod Biol 2010;152:96-102
- Baird DD, Dunson DB, Hill MC, et al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003;188:100-7
- Weuve J, Hauser R, Calafat AM, et al. Association of exposure to phthalates with endometriosis and uterine leiomyomata: findings from NHANES, 1999–2004. Environ Health Perspect 2010;118:825-32
- Zimmermann A, Bernuit D, Gerlinger C, et al. Prevalence, symptoms and management of uterine fibroids: an international internet-based survey of 21,746 women. BMC Women's Health 2012;12:6
- Canadian Institute for Health Information. Age-Standardized Hysterectomy Rates by Indication and Urban/Rural Dwelling, Canada, 2008–2009. 2013. Available at: https://secure.cihi.ca/free_products/Healthindicators2010_en.pdf [Last accessed 11 November 2013]
- Millar WJ. Hysterectomy, 1981/82 to 1996/97. Health Rep 2001;12:9-22
- Kunde K, Cortes E, Seed P, Khalaf Y. Evaluation of perioperative morbidity associated with single and multiple myomectomy. J Obstet Gynaecol 2009;29:737-41
- Makinen J, Johansson J, Tomas C, et al. Morbidity of 10110 hysterectomies by type of approach. Hum Reprod 2001;16:1473-8
- Watson Laboratories Inc. FIBRISTAL (Ulipristal acetate) Product Monograph. Salt Lake City, UT. June 2013
- Hashimoto K, Azuma C, Kamiura S, et al. Clonal determination of uterine leiomyomas by analyzing differential inactivation of the X-chromosome-linked phosphoglycerokinase gene. Gynecol Obstet Investig 1995;40:204-8
- Islam MS, Protic O, Giannubilo SR, et al. Uterine leiomyoma: available medical treatments and new possible therapeutic options. J Clin Endocrinol Metabol 2013;98:921-34
- Rein MS, Friedman AJ, Barbieri RL, et al. Cytogenetic abnormalities in uterine leiomyomata. Obstet Gynecol 1991;77:923-6
- Kiechle-Schwarz M, Sreekantaiah C, Berger CS, et al. Nonrandom cytogenetic changes in leiomyomas of the female genitourinary tract. A report of 35 cases. Canc Genet Cytogenet 1991;53:125-36
- Ligon AH, Morton CC. Genetics of uterine leiomyomata. Gene Chromosome Canc 2000;28:235-45
- Mashal RD, Fejzo ML, Friedman AJ, et al. Analysis of androgen receptor DNA reveals the independent clonal origins of uterine leiomyomata and the secondary nature of cytogenetic aberrations in the development of leiomyomata. Gene Chromosome Canc 1994;11:1-6
- Rein MS. Advances in uterine leiomyoma research: the progesterone hypothesis. Environ Health Perspect 2000;108(Suppl 5):791-3
- Andersen J. Growth factors and cytokines in uterine leiomyomas. Semin Reprod Endocrinol 1996;14:269-82
- Chegini N. Proinflammatory and profibrotic mediators: principal effectors of leiomyoma development as a fibrotic disorder. Semin Reprod Med 2010;28:180-203
- Ishikawa H, Ishi K, Serna VA, et al. Progesterone is essential for maintenance and growth of uterine leiomyoma. Endocrinology 2010;151:2433-42
- Englund K, Blanck A, Gustavsson I, et al. Sex steroid receptors in human myometrium and fibroids: changes during the menstrual cycle and gonadotropin-releasing hormone treatment. J Clin Endocrinol Metabol 1998;83:4092-6
- Brandon DD, Erickson TE, Keenan EJ, et al. Estrogen receptor gene expression in human uterine leiomyomata. J Clin Endocrinol Metabol 1995;80:1876-81
- Brandon DD, Bethea CL, Strawn EY, et al. Progesterone receptor messenger ribonucleic acid and protein are overexpressed in human uterine leiomyomas. Am J Obstet Gynecol 1993;169:78-85
- Ichimura T, Kawamura N, Ito F, et al. Correlation between the growth of uterine leiomyomata and estrogen and progesterone receptor content in needle biopsy specimens. Fertil Steril 1998;70:967-71
- Maruo T, Matsuo H, Samoto T, et al. Effects of progesterone on uterine leiomyoma growth and apoptosis. Steroids 2000;65:585-92
- Conneely OM, Mulac-Jericevic B, Lydon JP. Progesterone-dependent regulation of female reproductive activity by two distinct progesterone receptor isoforms. Steroids 2003;68:771-8
- Lora V, Grings AO, Capp E, et al. Gene and protein expression of progesterone receptor isoforms A and B, p53 and p21 in myometrium and uterine leiomyoma. Arch Gynecol Obstet 2012;286:119-24
- Bulun SE. Uterine fibroids. N Engl J Med 2013;369:1344-55
- Munro MG, Critchley HO, Broder MS, Fraser IS; Figo Working Group on Menstrual Disorders. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet 2011;113:3-13
- Wise LA, Palmer JR, Stewart EA, Rosenberg L. Age-specific incidence rates for self-reported uterine leiomyomata in the Black Women's Health Study. Obstet Gynecol 2005;105:563-8
- Marshall LM, Spiegelman D, Barbieri RL, et al. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet Gynecol 1997;90:967-73
- Pron G, Cohen M, Soucie J, et al. The Ontario Uterine Fibroid Embolization Trial. Part 1. Baseline patient characteristics, fibroid burden, and impact on life. Fertil Steril 2003;79:112-19
- Ross RK, Pike MC, Vessey MP, et al. Risk factors for uterine fibroids: reduced risk associated with oral contraceptives. Br Med J 1986;293:359-62
- Vikhlyaeva EM, Khodzhaeva ZS, Fantschenko ND. Familial predisposition to uterine leiomyomas. Int J Gynaecol Obstet 1995;51:127-31
- Marshall LM, Spiegelman D, Goldman MB, et al. A prospective study of reproductive factors and oral contraceptive use in relation to the risk of uterine leiomyomata. Fertil Steril 1998;70:432-9
- Luoto R, Kaprio J, Rutanen EM, et al. Heritability and risk factors of uterine fibroids – the Finnish Twin Cohort study. Maturitas 2000;37:15-26
- Faerstein E, Szklo M, Rosenshein NB. Risk factors for uterine leiomyoma: a practice-based case–control study. II. Atherogenic risk factors and potential sources of uterine irritation. Am J Epidemiol 2001;153:11-19
- Van Voorhis B. A 41-year-old woman with menorrhagia, anemia, and fibroids: review of treatment of uterine fibroids. JAMA 2009;301:82-93
- Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril 2009;91:1215-23
- Donnez J, Jadoul P. What are the implications of myomas on fertility? A need for a debate? Hum Reprod 2002;17:1424-30
- Farquhar C. Do uterine fibroids cause infertility and should they be removed to increase fertility? BMJ 2009;338:b126
- Rowe MK, Kanouse DE, Mittman BS, Bernstein SJ. Quality of life among women undergoing hysterectomies. Obstet Gynecol 1999;93:915-21
- Bradley LD. Leiomyomas. In: Sokol AI, Sokol ER, eds. General Gynecology: The Requisites in Obstetrics and Gynecology. Mosby, 2007:459-80
- Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol 1994;83:414-18
- Toro JR, Travis LB, Wu HJ, et al. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the surveillance, epidemiology and end results program, 1978–2001: an analysis of 26,758 cases. Int J Canc 2006;119:2922-30
- Rha SE, Byun JY, Jung SE, et al. CT and MRI of uterine sarcomas and their mimickers. Am J Roentgenol 2003;181:1369-74
- Russell DJ. The female pelvic mass. Diagnosis and management. Med Clin 1995;79:1481-93
- AAGL Practice Report: Morcellation During Uterine Tissue Extraction. J Minim Invasive Gynecol 2014; 21(4):517-30
- Statistics Canada. Births. 2009. Available at: http://www.statcan.gc.ca/pub/84f0210x/2009000/aftertoc-aprestdm1-eng.htm [Last accessed 24 October 2013]
- Marret H, Fritel X, Ouldamer L, et al. Therapeutic management of uterine fibroid tumors: updated French guidelines. Eur J Obstet Gynecol Reprod Biol 2012;165:156-64
- Lefebvre G, Vilos G, Allaire C, et al. The management of uterine leiomyomas. J Obstet Gynaecol Canada 2003;25:396-418, quiz 19-22
- American College of Obstetricians and Gynecologists. ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol 2008;112(2 Pt 1):387-400
- Cramer SF, Marchetti C, Freedman J, Padela A. Relationship of myoma cell size and menopausal status in small uterine leiomyomas. Arch Pathol Lab Med 2000;124:1448-53
- Chwalisz K, Perez MC, Demanno D, et al. Selective progesterone receptor modulator development and use in the treatment of leiomyomata and endometriosis. Endocr Rev 2005;26:423-38
- McKeage K, Croxtall JD. Ulipristal acetate: a review of its use in emergency contraception. Drugs 2011;71:935-45
- Talaulikar VS, Manyonda IT. Ulipristal acetate: a novel option for the medical management of symptomatic uterine fibroids. Adv Ther 2012;29:655-63
- Donnez J, Tomaszewski J, Vazquez F, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med 2012;366:421-32
- Donnez J, Tatarchuk TF, Bouchard P, et al. Ulipristal acetate versus placebo for fibroid treatment before surgery. N Engl J Med 2012;366:409-20
- Donnez J, Vazquez F, Tomaszewski J, et al. Long-term treatment of uterine fibroids with ulipristal acetate. Fertil Steril 2014,101:1565-73
- Spitz IM. Clinical utility of progesterone receptor modulators and their effect on the endometrium. Curr Opin Obstet Gynecol 2009;21:318-24
- Murphy AA, Kettel LM, Morales AJ, et al. Regression of uterine leiomyomata in response to the antiprogesterone RU 486. J Clin Endocrinol Metabol 1993;76:513-17
- Carbonell Esteve JL, Acosta R, Heredia B, et al. Mifepristone for the treatment of uterine leiomyomas: a randomized controlled trial. Obstet Gynecol 2008;112:1029-36
- Fiscella J, Bonfiglio T, Winters P, et al. Distinguishing features of endometrial pathology after exposure to the progesterone receptor modulator mifepristone. Hum Pathol 2011;42:947-53
- AbbVie Inc. Lupron Depot 3.75 mg (leuprolide acetate for depot suspension) Prescribing information. North Chicago, IL. October 2013
- Friedman AJ, Rein MS, Harrison-Atlas D, et al. A randomized, placebo-controlled, double-blind study evaluating leuprolide acetate depot treatment before myomectomy. Fertil Steril 1989;52:728-33
- Schlaff WD, Zerhouni EA, Huth JA, et al. A placebo-controlled trial of a depot gonadotropin-releasing hormone analogue (leuprolide) in the treatment of uterine leiomyomata. Obstet Gynecol 1989;74:856-62
- Golan A. GnRH analogues in the treatment of uterine fibroids. Hum Reprod 1996;11(Suppl 3):33-41
- Stovall TG, Muneyyirci-Delale O, Summitt RL Jr, Scialli AR. GnRH agonist and iron versus placebo and iron in the anemic patient before surgery for leiomyomas: a randomized controlled trial. Leuprolide Acetate Study Group. Obstet Gynecol 1995;86:65-71
- Leyland N, Casper R, Laberge P, Singh SS; The Society of Obstetricians and Gynaecologists of Canada. Endometriosis: diagnosis and management. J Obstet Gynaecol Canada 2010;32(7 Suppl 2):S1-32
- Friedman AJ, Hoffman DI, Comite F, et al. Treatment of leiomyomata uteri with leuprolide acetate depot: a double-blind, placebo-controlled, multicenter study. The Leuprolide Study Group. Obstet Gynecol 1991;77:720-5
- Chiaffarino F, Parazzini F, La Vecchia C, et al. Use of oral contraceptives and uterine fibroids: results from a case–control study. Br J Obstet Gynaecol 1999;106:857-60
- Mercorio F, De Simone R, Di Spiezio Sardo A, et al. The effect of a levonorgestrel-releasing intrauterine device in the treatment of myoma-related menorrhagia. Contraception 2003;67:277-80
- Bayer. Mirena (Levonorgestrel-releasing Intrauterine System) Product Monograph. Pointe-Claire, QC. June 2006
- Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev 2000;(4):CD000249
- Gleeson NC, Buggy F, Sheppard BL, Bonnar J. The effect of tranexamic acid on measured menstrual loss and endometrial fibrinolytic enzymes in dysfunctional uterine bleeding. Acta Obstet Gynecol Scand 1994;73:274-7
- Lakhani KP, Marsh MS, Purcell W, Hardiman P. Uterine artery blood flow parameters in women with dysfunctional uterine bleeding and uterine fibroids: the effects of tranexamic acid. Ultrasound Obstet Gynecol 1998;11:283-5
- Ip PP, Lam KW, Cheung CL, et al. Tranexamic acid-associated necrosis and intralesional thrombosis of uterine leiomyomas: a clinicopathologic study of 147 cases emphasizing the importance of drug-induced necrosis and early infarcts in leiomyomas. Am J Surg Pathol 2007;31:1215-24
- Lethaby A, Augood C, Duckitt K, Farquhar C. Nonsteroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev 2007;(4):CD000400
- Singh S, Best C, Dunn S, et al.; The Society of Obstetricians and Gynaecologists of Canada. Abnormal uterine bleeding in pre-menopausal women. J Obstet Gynaecol Canada 2013;35:473-9
- Shozu M, Murakami K, Segawa T, et al. Successful treatment of a symptomatic uterine leiomyoma in a perimenopausal woman with a nonsteroidal aromatase inhibitor. Fertil Steril 2003;79:628-31
- Hilario SG, Bozzini N, Borsari R, Baracat EC. Action of aromatase inhibitor for treatment of uterine leiomyoma in perimenopausal patients. Fertil Steril 2009;91:240-3
- Gurates B, Parmaksiz C, Kilic G, et al. Treatment of symptomatic uterine leiomyoma with letrozole. Reprod Biomed Online 2008;17:569-74
- Flierman PA, Oberye JJ, van der Hulst VP, de Blok S. Rapid reduction of leiomyoma volume during treatment with the GnRH antagonist ganirelix. BJOG: an International Journal of Obstetrics and Gynaecology 2005;112:638-42
- Felberbaum RE, Germer U, Ludwig M, et al. Treatment of uterine fibroids with a slow-release formulation of the gonadotrophin releasing hormone antagonist cetrorelix. Hum Reprod 1998;13:1660-8
- Gonzalez-Barcena D, Alvarez RB, Ochoa EP, et al. Treatment of uterine leiomyomas with luteinizing hormone-releasing hormone antagonist cetrorelix. Hum Reprod 1997;12:2028-35
- Deng L, Wu T, Chen XY, et al. Selective estrogen receptor modulators (SERMs) for uterine leiomyomas. Cochrane Database Syst Rev 2012;10:CD005287
- Campo S, Garcea N. Laparoscopic myomectomy in premenopausal women with and without preoperative treatment using gonadotrophin-releasing hormone analogues. Hum Reprod 1999;14:44-8
- Dubuisson JB, Fauconnier A, Fourchotte V, et al. Laparoscopic myomectomy: predicting the risk of conversion to an open procedure. Hum Reprod 2001;16:1726-31
- Society of Obstetricians and Gynaecologists of Canada. SOGC clinical practice guidelines. Uterine fibroid embolization (UFE). Int J Gynaecol Obstet 2005;89:305-18
- Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril 2003;79:120-7
- Gupta JK, Sinha AS, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev 2006;(1):CD005073
- Broder MS, Goodwin S, Chen G, et al. Comparison of long-term outcomes of myomectomy and uterine artery embolization. Obstet Gynecol 2002;100(5 Pt 1):864-8
- Spies JB, Bruno J, Czeyda-Pommersheim F, et al. Long-term outcome of uterine artery embolization of leiomyomata. Obstet Gynecol 2005;106(5 Pt 1):933-9
- Mara M, Fucikova Z, Maskova J, et al. Uterine fibroid embolization versus myomectomy in women wishing to preserve fertility: preliminary results of a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol 2006;126:226-33
- Dutton S, Hirst A, McPherson K, et al. A UK multicentre retrospective cohort study comparing hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids (HOPEFUL study): main results on medium-term safety and efficacy. BJOG: an International Journal of Obstetrics and Gynaecology 2007;114:1340-51
- Pron G, Mocarski E, Bennett J, et al. Pregnancy after uterine artery embolization for leiomyomata: the Ontario multicenter trial. Obstet Gynecol 2005;105:67-76
- National Collaborating Centre for Women’s and Children’s Health. Heavy Menstrual Bleeding. Clinical Guideline. 2007. Available at: http://www.nice.org.uk/nicemedia/pdf/CG44FullGuideline.pdf [Last accessed October 2014]
- Lethaby A, Shepperd S, Cooke I, Farquhar C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev 2000;(2):CD000329
- Vilos GA, Daly LJ, Tse BM. Pregnancy outcome after laparoscopic electromyolysis. J Am Assoc Gynecologic Laparoscopists 1998;5:289-92
- Hindley J, Gedroyc WM, Regan L, et al. MRI guidance of focused ultrasound therapy of uterine fibroids: early results. Am J Roentgenol 2004;183:1713-19
- Stewart EA, Rabinovici J, Tempany CM, et al. Clinical outcomes of focused ultrasound surgery for the treatment of uterine fibroids. Fertil Steril 2006;85:22-9
- Alessandri F, Lijoi D, Mistrangelo E, et al. Randomized study of laparoscopic versus minilaparotomic myomectomy for uterine myomas. J Minim Invasive Gynecol 2006;13:92-7
- Nezhat FR, Roemisch M, Nezhat CH, et al. Recurrence rate after laparoscopic myomectomy. J Am Assoc Gynecologic Laparoscopists 1998;5:237-40
- Garcia CR. Management of the symptomatic fibroid in women older than 40 years of age. Hysterectomy or myomectomy? Obstet Gynecol Clin N Am 1993;20:337-48
- LaMorte AI, Lalwani S, Diamond MP. Morbidity associated with abdominal myomectomy. Obstet Gynecol 1993;82:897-900
- Kjerulff KH, Rhodes JC, Langenberg PW, Harvey LA. Patient satisfaction with results of hysterectomy. Am J Obstet Gynecol 2000;183:1440-7
- Carlson KJ, Miller BA, Fowler FJ Jr. The Maine Women's Health Study: I. Outcomes of hysterectomy. Obstet Gynecol 1994;83:556-65