

Abstract
Probodies are proteolytically activated antibodies engineered to remain inert until activated locally in diseased tissue. In principle, any therapeutic antibody can be converted into Probody™ form. In this perspective, we highlight the emerging therapeutic potential of the Probody approach in the form of conventional IgG-based Probodies as well as in the form of ‘empowered Probody’ formats such as Probody–drug conjugates.
1. Introduction
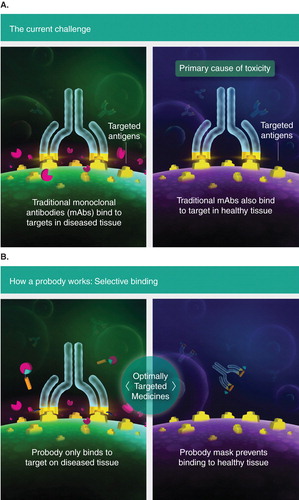
A central problem with antibody-based therapies is that despite the high-affinity antigen binding and highly specific recognition possible in the antigen-combining site of antibody variable domains, the presence of the target antigen in healthy tissues can limit the ability of the antibody to achieve therapeutic effects without inducing unacceptable ‘on-target’ toxicity (). The Probody™ platform leverages the upregulation of protease activity – widely recognized as a hallmark of diseased tissue, particularly in cancer Citation[1] and in inflammatory conditions Citation[2] – to achieve disease-tissue-specific therapeutic activity. The approach is based on the use of an IgG antibody, or fragment thereof, such as a variable region, which has been modified to include a masking peptide linked to the N-terminus of the light chain of the antibody through a protease-cleavable linker peptide. The entire construct is fully biosynthetic: the masking peptide, cleavable linker and antibody light chain comprise one polypeptide chain. In the intact form, the Probody is effectively blocked from binding to the target antigen in healthy tissues; however, once activated by appropriate proteases in the diseased environment, the masking peptide is released, revealing a fully active antibody capable of binding to its target ().
Figure 1. Cartoon illustration of the antibody and Probody platforms. A. A conventional antibody binds to its target in both healthy and diseased tissues; selectivity requires differential expression of the antigen. B. The Probody consists of a fully biosynthetic construct in which a masking peptide (triangle) linked to a selective proteolytically cleavable linker is added to the N-terminus of the antibody light chain. In healthy tissues, the Probody remains intact and thus is blocked from binding to the antigen target. However, once the linker peptide is cleaved by proteases that are selectively activated in the diseased-tissue microenvironment, the masking peptide is released, allowing the active antibody to bind to its target, resulting in tissue-specific activity.
The proteolytically cleavable linker, which contains a substrate sequence that is recognized by one or more proteases at the tumor site, is a key feature of the platform. It appears that the design of the amino acid sequence of this substrate-containing linker peptide to allow recognition and cleavage by multiple proteases, rather than by a single specific protease, is advantageous for the use of Probodies in a wide range of tumors at various stages of development and with a range of protease activities. We have demonstrated this approach using an EGFR Probody Citation[3] and with a method – termed IHZ™ analysis – a zymography-like approach using the Probody itself as a probe of proteolytic activity on frozen tissue sections. In a survey of tumor sections from colorectal and lung cancer patients, a majority of the tumors contained Probody-activating protease activity, while healthy tissues lacked this activity, consistent with previously reported results using an active-site antibody to detect active-site protease in situ Citation[4]. As in the case of cleavable (and non-cleavable) linkers used for the conjugation of payload-linkers in conventional antibody– drug conjugates (ADCs), Probody substrate linkers appear to be relatively portable between Probody constructs, allowing a range of Probodies with different antigen specificities to be constructed with the same set of cleavable substrate linkers. Furthermore, depending on the protease environment of the particular cancer or inflammatory disease, the substrate specificity of the linker can be changed to match the local environment and enhance the disease specificity of the Probody approach.
2. Probodies in IgG form
We have investigated an IgG-based Probody therapeutic approach with a chimeric human IgG1 Probody, termed PB1 or CTX-023, based upon cetuximab as the parental antibody Citation[3]. Cetuximab is a chimeric therapeutic antibody that blocks ligand binding and subsequent mitogenic signaling of the EGFR, a transmembrane glycoprotein whose upregulation in a variety of cancers of epithelial origin correlates with poor prognosis Citation[5]. Although cetuximab has been approved for the treatment of head-and-neck and colorectal cancers, skin rash has been identified as a dose-limiting toxicity, and this on-target side effect may lead to reduced or discontinued cetuximab dosing in 30% of patients Citation[6]. A masking peptide was identified for the antibody, and a multi-specific substrate linker with sensitivity to tumor-associated proteases, including matriptase, urokinase plasminogen activator and legumain, was used to link this mask to the parental antibody Citation[3].
In the intact Probody form, CTX-023 showed reduced EGFR binding and activity based upon ELISA, cell-based FACS assays and cell proliferation assays, and this masking effect was maintained in vivo in the circulation of healthy as well as tumor-bearing mice. However, in vivo imaging and post-dose immunohistochemistry demonstrated that CTX-023 was activated and accumulated in the tumor tissue of mice bearing xenograft tumors, leading to effective slowing of tumor growth. At equal doses (25 mg/kg) as cetuximab, Probody CTX-023 achieved similar efficacy, consistent with the hypothesis that locally activated Probody could effectively block EGFR signaling. Moreover, when cynomolgus monkeys were treated with Probody or cetuximab, the Probody produced reduced skin toxicity compared to cetuximab. In addition, in a preliminary pharmacokinetic analysis, the Probody achieved higher exposure at equal dose versus cetuximab, reflecting the effect of a prolonged elimination half-life. This effect is consistent with a reduction in antigen-dependent clearance for the Probody, resulting from blockade of antigen binding in healthy tissues and highlights an additional pharmacologic benefit of the platform.
Another family of targets well suited to the Probody approach are the ligands and receptors of the Notch pathway such as the ligands Jagged 1 and 2. Current antibody and small-molecule approaches to targeting the Notch pathway have faced challenges with toxicity as observed in preclinical and clinical studies Citation[7]. Preliminary preclinical data that we have generated suggest that an anti-Jagged Probody (CTX-033) targeting Jagged 1 and 2 can achieve anti-tumor activity in mouse tumor models while sparing the toxicity associated with blocking the Notch pathway using a conventional anti-Jagged antibody Citation[8].
3. Probody–drug conjugates
The issue of on-target toxicity in healthy tissue for antibodies becomes even more limiting to empowered antibody formats such as ADCs. These molecules act by concentrating a cytotoxic agent at the site of disease – for example, an antigen overexpressing tumor cell – but can also kill healthy cells that express the antigen at moderate-to-high levels Citation[9]. Although targets for conventional ADCs have typically been selected by identifying selectively overexpressed antigens in tumor versus normal tissues, the number of antigens meeting this requirement appears limited by an unacceptably small therapeutic window, with few targets having the exceptional tumor overexpression observed for human epidermal growth factor receptor 2 Citation[10].
For example, the glycoprotein antigen Lewis Y (LeY) initially appeared promising as a target for an ADC therapeutic approach, with high expression in a variety of epithelial-derived tumors including breast, gastrointestinal (GI), lung, cervix, ovary and melanoma. An ADC constructed from the anti-LeY antibody BR96 conjugated with doxorubicin, a DNA-intercalating anthracycline, produced positive preclinical efficacy and early indications of clinical activity Citation[11]. However, LeY is also expressed at lower levels on normal tissue in the GI tract and pancreas, and perhaps not surprisingly, administration of the ADC to patients resulted in elevation of pancreatic lipase as well as more severe GI toxicities, including severe emesis associated with exudative gastritis and superficial hemorrhage of the upper GI Citation[11]. These ADC-associated toxicities did not resemble those of the free drug doxorubicin (already in use as a cancer therapeutic) and when the unconjugated BR96 antibody was administered to one patient, it resulted in side effects of bloody emesis and diarrhea, consistent with an on-target effect of antibody binding to an antigen expressed in healthy tissues Citation[11].
An intact Probody–drug conjugate (PDC) has the potential to protect normal tissues expressing the target antigen from the biological effects of antibody binding and antigen-dependent uptake of the conjugated toxin, and may also benefit from improved exposure at a given drug dose. By localizing activation and binding to the disease tissue, the PDC format should expand the universe of drug conjugate targets possible, including highly expressed tumor antigens with significant expression in healthy tissue such as EGFR.
4. Conclusion
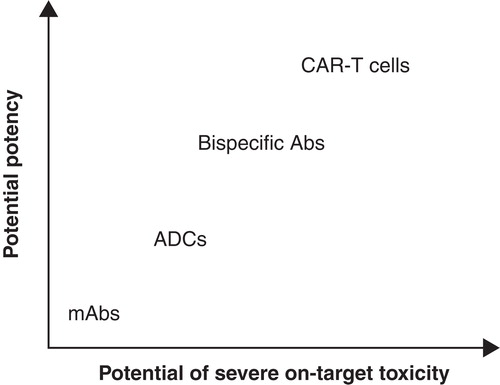
Preclinically, Probodies have demonstrated appropriate mask-linker stability to achieve an improvement in therapeutic index over conventional antibodies. CTX-023, an EGFR Probody, remains masked in vivo and ex vivo in healthy tissue Citation[3]. Probodies can be activated sufficiently within tumor xenografts so as to achieve efficacy similar to that of the parental antibody. These results suggest that Probodies in the IgG format can provide advantages in therapeutic window, and suggest that the Probody concept can be applied in multiple formats, including empowered antibody formats where on-target toxicity is limiting to therapeutic dosing. Indeed, the potential for significant safety liability appears to increase () with empowered antibodies ranging from ADCs to T-cell engaging bispecific antibodies and chimeric antigen receptors Citation[12].
Figure 2. Proposed opportunities for empowered Probody™ formats. The potency and efficacy of antibodies can be enhanced through cytotoxic antibody–drug conjugates (ADCs), T-cell engaging bispecific formats, or chimeric antigen receptors expressed on T cells (CAR-T cells). However, these empowered formats have the potential for more severe on-target toxicity. It is this on-target, but off-tissue toxicity that can be mitigated using the Probody approach. Whereas the number of targets available for antibody-based approaches is limited by antigen expression in normal tissues, the number available for Probody approaches is predicted to be greater in each case.
5. Expert opinion
Preclinical findings suggest that CTX-023 can be dosed to exposures exceeding that of cetuximab as currently administered in the clinic, with the potential to enhance quality of life by reducing toxicities for patients, as well as to improve the effectiveness of anti-EGFR therapy.
Because the clinical dosing of cetuximab is limited by skin toxicity and antigen-dependent pharmacokinetic effects, the potential exists for improved efficacy using CTX-023 as compared to cetuximab because CTX-023 is expected to achieve higher exposure in patients with improved safety at equal or higher doses than cetuximab. The EVEREST trial Citation[13] found a trend toward improved clinical benefit with increased doses of cetuximab. In addition, a pharmacokinetics–pharmacodynamics study of patients treated with cetuximab in combination with irinotecan and 5-fluorouracil found that those patients having higher-than-median cetuximab levels had a statistically significant improvement in progression-free survival Citation[14]. This supports the idea that increased anti-EGFR exposure, if safe, could meaningfully improve clinical outcome.
Probodies also offer the potential for improved clinical outcomes in combination therapy as a result of reducing overlapping toxicities that minimize therapeutic window. Indeed, Regales and co-workers reported that a combination of cetuximab with a tyrosine kinase inhibitor (TKI) could improve anti-tumor efficacy in preclinical models of EGFR-mutant-based acquired TKI resistance Citation[15]. However, the authors also acknowledged that clinical use of a combination of cetuximab with TKIs could be limited by excessive skin toxicity arising from both agents. An EGFR Probody could ameliorate this toxicity, leading to more effective combination therapy.
Empowered Probody formats represent a greatly expanded opportunity for targets and effective therapeutic strategies in oncology. The fact that the corresponding empowered antibody formats – ADCs and bispecifics – have shown impressive clinical efficacy, provides the promise of new generations of more effective therapeutics. Yet the number of targets that can be addressed with these potent modalities may be quite limited by the fact that tumor antigens can often be found in healthy tissue at levels that preclude empowered antibody use. Probodies add a new dimension in tissue-specific therapeutic targeting that makes many more targets available for therapeutic intervention. Ultimately, the advantage of Probody therapeutics should translate to patients, allowing them to realize the benefit of more potent therapies without experiencing the severe side effect associated with traditional monoclonal antibody-based therapies.
Declaration of interest
Both authors are paid employees and shareholders of CytomX Therapeutics, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Bibliography
- Edwards D, Hoyer-Hansen G, Blasi F, Sloane BF. The cancer degradome: proteases and cancer biology. Springer; New York, NY; 2009
- Vergnoble N, Chignard M. Proteases and their receptors in inflammation. Springer; New York, NY; 2011
- Desnoyers LR, Vasiljeva O, Richardson JH, et al. Tumor-specific activation of an EGFR-targeting probody enhances therapeutic index. Sci Transl Med 2013;5:164-73
- LeBeau AM, Lee M, Murphy ST, et al. Imaging a functional tumorigenic biomarker in the transformed epithelium. Proc Natl Acad Sci USA 2013;110:93-8
- Baselga J, Arteaga CL. Critical update and emerging trends in epidermal growth factor receptor targeting in cancer. J Clin Oncol 2005;23:2445-59
- Boone SL, Rademaker A, Liu D, et al. Impact and management of skin toxicity associated with anti-epidermal growth factor receptor therapy: survey results. Oncology 2007;72:152-9
- Aster JC. Targeting the Notch pathway: twists and turns on the road to rational therapeutics. J Clin Oncol 2012;30:2418-20
- Sagert J, West J, Vasiljeva O, et al. Tumor-specific inhibition of jagged-dependent Notch signaling using a probody™ therapeutic. In: Proceedings of the AACR-NCI-EORTC International Conference: Molecular Targets and Cancer Therapeutics; 19 – 23 October 2013; Boston, Philadelphia: AACR. Mol Cancer Ther 2013;12(11 Suppl):abstract C158
- Panowski S, Bhakta S, Raab H, et al. Site-specific antibody conjugates for cancer therapy. MAbs 2014;6:1-12
- Gerber H-P, Koehn FE, Abraham RT. The antibody-drug conjugate: an enabling modality for natural product-based cancer therapeutics. Nat Prod Rep 2013;30:625-39
- Saleh MN, Sugarman S, Murray J, et al. Phase I trial of the anti-Lewis Y drug immunoconjugate BR96-doxorubicin in patients with Lewis Y-expressing epithelial tumors. J Clin Oncol 2000;18:2282-92
- Stone JD, Aggen DH, Schietinger A, et al. A sensitivity scale for targeting T cells with chimeric antigen receptors (CARs) and bispecific T-cell engagers (BiTEs). Oncoimmunology 2012;1:863-73
- Van Cutsem E, Tejpar S, Vanbeckevoort D, et al. Intrapatient cetuximab dose escalation in metastatic colorectal cancer according to the grade of early skn reactions: the randomized EVEREST study. J Clin Oncol 2012;10:2861-8
- Azzopardi N, Lecomte T, Ternant D, et al. Cetuximab pharmacokinetics influences progression-free survival of metastatic colorectal cancer patients. Clin Cancer Res 2011;17:6329-37
- Regales L, Gong Y, Shen R, et al. Dual targeting of EGFR can overcome a major drug resistance mutations in mouse models of EGFR mutant lung cancer. J Clin Invest 2009;119:3000-10