The gold standard for the diagnosis of nonconvulsive status epilepticus (NCSE) is EEG Citation[1,2]. Studies on NCSE in the literature often imply that the EEG diagnosis of NCSE is straightforward Citation[3,4]. In reality, NCSE has several different EEG presentations, and some are not specific for NCSE. In particular, generalized periodic patterns or generalized periodic epileptiform discharges (GPEDS) can be seen in NCSE but also in severe nonepileptic encephalopathies such as anoxia or other metabolic disturbances Citation[1–5].
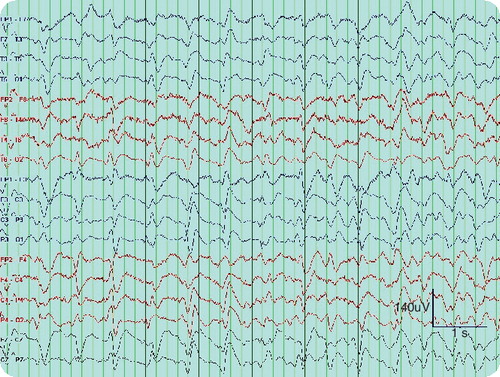
In an informal survey, we sent a single 10-s epoch of EEG and reviewed the interpretations of the readers. We were specifically interested whether the possibility of NCSE would be raised based on this EEG pattern. The history was limited to the following: 60-year-old male found down and admitted with ‘altered mental status’ or ‘coma’. History was intentionally limited, as we were interested in the impression of the EEG sample prior to integrating it with the history. Two groups of reviewers were surveyed; first, epileptologists or electroencephalographers (EEGers) at tertiary epilepsy centers or EEG laboratories (n = 14); and second, general practicing board-certified neurologists (n = 12). In the epileptologists or EEGers sample, 100% mentioned NCSE, in addition to metabolic disorders and other causes of encephalopathies. In the general neurologist sample, 42% mentioned NCSE, while 58% did not and limited the interpretation to severe diffuse encephalopathy. GPEDS are very common in hospital patients who undergo EEGs. However, there is significant variability in the EEG interpretation among nonspecialists, with less than half raising the possibility of NCSE. The reality is that it is often impossible, based on EEG alone, to know for certain whether a given patient with GPEDS is in NCSE Citation[4,5], so this is not very surprising.
However, this finding is important since studies of NCSE, be it for diagnosis Citation[3–5], prognosis or treatment, depend entirely on what EEG patterns ‘confirm’ as diagnosis of NCSE. On the one hand, NCSE should not be missed as a cause of coma since it is treatable; on the other hand, most patients with GPEDS after an anoxic brain injury (e.g., cardiac arrest) will not benefit from treatment for NCSE Citation[3,4]. If all GPEDS EEGs are interpreted as NCSE, then the incidence of NCSE will be artificially high Citation[3,4] and treatment will seem artificially ineffective.
Thus, there is a need for diagnostic criteria as a means to distinguish between NCSE and nonepileptic severe encephalopathies such as anoxia. Some studies have attempted to differentiate between patterns of nonepileptic encephalopathy from those of NCSE, a difficult task. Proposed criteria include morphology of the waveforms and their response to external stimulation Citation[6], and also characteristics of so-called triphasic waves Citation[6]. Another potentially discriminating factor is the impact of benzodiazepines and their effects on the EEG, since intravenous injection of a fast-acting benzodiazepine will abolish or improve an electrographic seizure pattern Citation[4,5]. Unfortunately, triphasic waves in the context of metabolic encephalopathy may have a similar response to benzodiazepines Citation[7], so that even improvement in the EEG after treatment does not imply an epileptic (NCSE) etiology. Another interpretation of this result is that, as we believe, the distinction between GPEDS and triphasic waves is unclear.
The real-life conclusion is that the differentiation of NCSE and nonepileptic severe encephalopathies such as anoxia remains difficult. In the context of anoxia versus status, the GPEDS pattern is consistent with, but unlikely to represent, NCSE. In practice, a treatment trial for NCSE is almost always warranted, but most patients will not respond clinically or electrographically Citation[4,5]. Given that EEG alone often cannot give the answer, one will have to interpret it in the clinical context. We remain clinicians, and no test can substitute for sound clinical judgment.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- Kaplan PW. The EEG of status epilepticus. J. Clin. Neurophysiol.23, 221–229 (2006).
- Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Reviewing the evidence for treatment of periodic epileptiform discharges and related patterns. J. Clin. Neurophysiol.22, 79–91 (2005).
- Towne AR, Waterhouse EJ, Boggs JG et al. Prevalence of nonconvulsive status epilepticus in comatose patients. Neurology54, 340–345 (2000).
- Benbadis SR, Tatum WO 4th. Prevalence of nonconvulsive status epilepticus in comatose patients [Letter]. Neurology55, 1421–1423 (2000).
- Husain AM, Mebust KA, Radtke RA. Generalized periodic epileptiform discharges: etiologies, relationship to status epilepticus, and prognosis. J. Clin. Neurophysiol.16, 51–58 (1999).
- Boulanger JM, Deacon C, Lecuyer D et al. Triphasic waves versus nonconvulsive status epilepticus: EEG distinction. Can. J. Neurol. Sci.33, 175–180 (2006).
- Fountain NB, Waldman WA. Effects of benzodiazepines on triphasic waves. J. Clin. Neurophysiol.18, 345–352 (2001).