
Abstract
Preventive chemotherapy campaigns against schistosomiasis have progressively scaled-up during the last decade, administering single standard dose praziquantel (40 mg/kg) treatments to millions of African children. Steps taken in securing international advocacy and national level implementation are traced to highlight an international treatment platform set for further expansion, including surveillance of schistosomiasis, school-level targeting with better on-site drug administration and annual reporting of programmatic indicators (i.e., treatment coverage), potentially in real-time. Several shortcomings in need of resolution are identified and efficacy of praziquantel is assessed by a systematic review. If WHO predictions in reduction of schistosomiasis are to be realized, careful international harmonization and tailoring of national resources are required. Maintaining an effective drug distribution system and regularly checking drug efficacy are paramount.
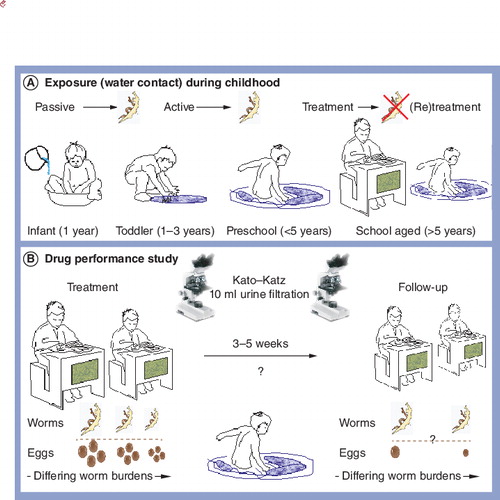
(A) As the child gains independence, exploration of these water bodies continues and infections are accrued. Upon reaching school, where treatment is given, worm burdens are reduced by treatment with praziquantel, however, the child will become re-infected upon subsequent water contact. (B) Conceptualization of treatment study measuring the performance of praziquantel. Children within a school are selected and offered treatment. These same children are re-examined typically 24 days later and cure rate is determined as a percentage of those who have stopped shedding parasite eggs. Cure rates typically range from absolute (100%) down to 75%, but in some instances can be much lower.
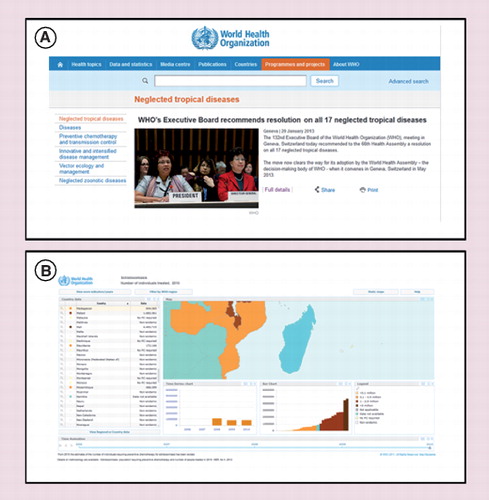
Screen shots of the WHO website that highlight recent decisions taken for disease control (A) and data contained within the Preventive Chemotherapy Database for Madagascar illustrating administered treatments (B).
(A) Front cover of teacher training booklet for deworming school children. (B) On-site tools needed for administration of deworming tablets to children: potable water, drinking cups and praziquantel height pole is needed alongside treatment registers for recording treatments and noting any noncompliance or side effects.Figure taken from Citation[14].
![Figure 4. Generic information, education and communication materials produced by WHO for implementing preventive chemotherapy within schools.(A) Front cover of teacher training booklet for deworming school children. (B) On-site tools needed for administration of deworming tablets to children: potable water, drinking cups and praziquantel height pole is needed alongside treatment registers for recording treatments and noting any noncompliance or side effects.Figure taken from Citation[14].](/cms/asset/35bb7f72-1968-4b2e-8c50-d1018b5eb56a/ierz_a_811931_f0004_b.jpg)
To qualify for inclusion, study design had to be a longitudinal study enrolling individuals (0–22 years of age) infected with Schistosoma haematobium and/or Schistosoma mansoni, as determined microscopically: for S. haematobium, eggs in a standard filtrate of 10 ml of urine, for S. mansoni, eggs in standard Kato–Katz smears (at least a single smear); patients had to be treated with praziquantel, 40 mg/kg single dose; the sample size (number. treated or diagnosed) was reported; the temporal interval between baseline and reassessment had to be reported; the population age ranges were reported and primary outcome (cure rate achieved) had to be reported. Exclusion criteria were: study participants were not human; incomplete information; duplicate publications; full article not accessible; reviews and follow-up period exceeded 90 days or less than 20 days. The following information was independently extracted by two reviewers (AMD Navaratnam and JC Sousa-Figueiredo) and was checked together. The extracted information included: first author’s name and year of publication, country studied, participants age, Schistosoma species, diagnostics methods, follow-up time, raw dichotomous data of efficacy assessment (number. treated/number. positive upon follow-up), cure rate and other outcomes (egg reduction rate). In surveys were the same population was followed-up multiple times, the outcome considered was the one gathered closest to the latest acceptable time period (i.e., 90 days).
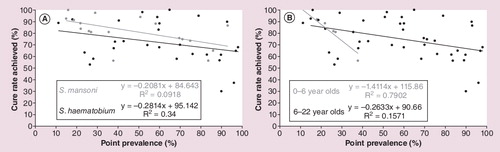
(A) Species cure rates for Schistosoma mansoni and Schistosoma haematobium. (B) Cure rates for children in two age ranges (0–6 years and aged 6 plus) differ with cure rates within younger children decreasing quickly with increasing local prevalence highlighting that for preschool-aged children the performance of praziquantel is to be optimized.
Background on epidemiology & treatment
Schistosomiasis is a waterborne parasitic infection which typically gives rise to a chronic inflammatory disease, as typified by immunopathological lesions around schistosome eggs trapped inside host tissues Citation[1,2]. In Africa, there are two forms of schistosomiasis, intestinal and urogenital, which are caused by different species, Schistosoma mansoni and Schistosoma haematobium, respectively Citation[3–5]. Other schistosome species able to infect man include Schistosoma intercalatum and Schistosoma guineensis but these are of minor public health importance Citation[3]. Although widespread, the geographical distribution of schistosomiasis across Africa is often focalized and difficult to predict locally. This is due to interdependence (as part of the schistosome’s lifecycle) with aquatic snails and site-specific conditions of impoverished sanitation and water hygiene. As schistosome larvae (i.e., cercariae) can penetrate skin directly, and infection with schistosomes takes place upon exposure to water containing viable larvae Citation[5]. This can be from contact with either domestic water drawn from environmental bodies or from activities within these water bodies themselves in passive- or active-like water contact mechanisms, respectively, see Citation[6]. Accurate mapping of schistosomiasis is an ongoing challenge but fundamental for effective control by targeting resources Citation[3,7].
Schistosomiasis is not restricted to humans, with several other schistosome species infecting livestock and wildlife, although these have limited medical importance Citation[8–10]. Nonetheless in West Africa, recent detection of novel hybrids between S. haematobium and Schistosoma bovis and Schistosoma curassoni has revealed an unexpected zoonosis thereby challenging conventional wisdom both on epidemiology and control Citation[11,12]. Equally important has been the detection of schistosomiasis in infants and preschool-aged children that highlights other shortcomings in present control tools for example, in diagnostics and of suitable drug formulations Citation[13]. These instances, although important, should not distract attention from the more obvious disease burden and need for control within school-aged children Citation[14]. In resource-limited settings, typically school-aged children are given prioritization which is in-keeping with their higher burden of parasitemia (i.e., infection prevalence and intensity both peak in childhood), their greater vulnerability to disease (but with better reversibility of morbidity if given prompt treatment), as well as their easier accessibility within educational infrastructure (i.e., by attending primary school) as supported by universal primary education (UPE) Citation[4,14].
In endemic areas, interventions are thus targeted towards mass treatment of school children by large-scale administration of single standard dose praziquantel (PZQ) given out at 40 mg/kg bodyweight dosing following international guidelines for preventive chemotherapy (PC) Citation[4]. Although the exact killing mechanism of PZQ against schistosome worms is still unknown (see section below), its efficacy is typically judged by the cessation of parasite egg excretion in stool or urine samples Citation[14,15]. The specimens are processed by routine parasitological methods and parasitological cure (i.e., the percentage of those children who stop shedding eggs) is judged by inspection of a cohort of children before and after PZQ treatment, as shown in . Unfortunately, as treatment does not prevent or guard against subsequent infection, if water contact is continued, reinfection can take place relatively quickly Citation[16]. However, the pathology that the eggs induce is somewhat diminished by a reduction in their production (i.e., egg reduction rate) such that future morbidity is averted. To balance against the levels of reinfection, a staggered regime of retreatment is offered & ) Citation[14]. Upon careful consideration of all alternatives, PC has come to the fore in the fight against neglected tropical diseases (NTDs) Citation[17] with PZQ, the only drug commercially available for control of schistosomiasis, as the backbone medication Citation[14,15]. In the context of this review the advocacy, policies and practicalities of administration and performance of single dose PZQ treatment are reviewed.
Fostering large-scale treatment campaigns
Despite a daily-adjusted life year or quality-adjusted life year statistic that might suggest otherwise Citation[18], control of schistosomiasis ranks highly within the list of appropriate interventions for improving child health in Africa. Over the last decade, there have been significant steps taken in control Citation[19]; at the national level, for example, a tremendous effort has taken place in the scale-up of PC across several countries in sub-Saharan Africa (SSA) administering single standard dose PZQ to millions of children Citation[4]. This scale-up was with the firm intention of abating present morbidity and averting disease associated with schistosomiasis whereas before access to drug was severely limited and induced unnecessary suffering Citation[19]. Brought about by the fruition of international advocacy, this reality was set down upon WHO guidelines of integrated PC, not forgetting a key ingredient of an international donor landscape receptive to offering comprehensive support either in the provision of funds or in medications against NTDs gratis (e.g., orally taken benzimidazoles, mectizan and zithromax) Citation[20,21]. Consolidated by instigation of several national treatment campaigns, these so-called ‘rapid-impact’ packages make convincing sense within public health settings, with an ‘all in’ cost-per-child treated being often cited as US$0.50 Citation[22,23]. However, while the cost per treated child might be appealing, when scaled across several tens of millions of children needing treatment each year, the surrounding budgets become much more substantive Citation[24,25], not omitting the cost for distribution of the drugs themselves that typically accounts for the majority of the assigned budget Citation[26,27].
Securing & strengthening political advocacy
Significant steps taken to shape this donor landscape began by obtaining, in 2001, high-level political support by acceptance of the 54th World Health Assembly (WHA) stipulated resolution 54.19 Citation[28]. This stated that member states were urged to attain “a minimum target of regular administration of chemotherapy to at least 75% and up to 100% of all school-aged children at risk of morbidity by 2010.” Building upon this and recalling previous resolutions WHA3.26, WHA28.53 and WHA29.58 led to the most recent endorsement of WHA65.21 by promoting ‘elimination of schistosomiasis’, in 2012. This reaffirmed the need to reach and treat at least 75% of school-age children at risk of morbidity with PC and also envisaged significant reductions in disease endemicity through future scale-up of PC. Subsequently, further recommendations on 16 other NTDs were made at the 132nd Executive Board of WHO, see , that will then be put forward for due consideration at the 66th WHA in 2013. In so doing, a clear agenda for elimination of several NTDs, embellishing the WHO strategic 2012–2020 roadmap for schistosomiasis in the African (AFRO) and Mediterranean (EMRO) regions, is now ratified Citation[4].
Since WHA 54.19, and thanks to the backing from a number of international organizations, donor foundations, bilateral institutions and nongovernmental development organizations (NGDOs), several African governments have taken up the cause Citation[28]. This was significantly boosted by a US$30 million grant from the Bill & Melinda Gates Foundation to set up the Schistosomiasis Control Initiative (SCI) at Imperial College London (UK) in 2002 Citation[19,29]. Originally with its research partners at Harvard University (MA, USA) and then later Danish Bilharziasis Laboratory, Denmark, SCI provided financial, technical and logistical support to six countries in East (Uganda, Tanzania, Zambia) and West (Niger, Burkina Faso, Mali) SSA Citation[29]. Equally as important was an associated monitoring and evaluation research portfolio, as undertaken as ‘implementation science’ alongside while the programme unfolded Citation[30]. The initial 5-year SCI programme later synergized with subsequent funds from USAID in conjunction with the Research Triangle Institute (RTI) International in the 2006–2011 period. This was part of RTI’s coined ‘NTD Control Program’, originally, earmarked US$15 million of funding in the first year of operations, RTI fostered links with other implementation partners for general control of NTDs in: Burkina Faso, Cameroon, Ghana, Mali, Niger, Sierra Leone, South Sudan, Togo and Uganda Citation[28].
Following G8 commitments to NTDs beginning in the UK in 2005, additional funds were provided to SCI by the Department for International Development in 2010 for implementation of Integrated Control of Schistosomiasis in Africa (ICOSA) for Ivory Coast, Liberia, Malawi, Mozambique, Niger, Tanzania, Uganda and Zambia. With Obama’s Expanded Presidential Global Health Initiative further support of NTD control was fostered, most recently additional support from USAID to RTI international has created a new set of implementation partners (Helen Keller International, IMA World Health and Sightsavers International) brought together within the ‘ENVISION’ programme set to run until 2016 with an earmarked annual budget of some US$89 million. Although a more minor international donor player, the END Fund was created as a financial tool with pooled resources, largely from private philanthropy, for assisting the scale-up of NTD control. The most notable coordinating partner of which was Geneva Global, which provided funds to support schistosomiasis control in Burundi and Rwanda as implemented by SCI Citation[31]. Similarly, the END 7 Fund, created by the Sabin Vaccine Institute, was dedicated to raising the awareness, political will and funding necessary to control and eliminate the seven most common NTDs Citation[20].
A need for global communications
During this time keeping abreast of this growing international commitment was solidified in the creation of new communication tools and groups, with the WHO website having a central coordinating importance with Action Against Worms newsletters that brought new focus upon control activities against worm-related NTDs Citation[201]. Perhaps the most important and formalized new communication was in 2007 the production of an open access journal from the PLoS dedicated to NTDs Citation[32]. With external support from the Bill & Melinda Gates Foundation, PLoS NTDs quickly became the leading journal for academic outputs in NTD-related research. In terms of schistosomiasis, there are well over 200 articles reporting on novel aspects in the use PZQ in PC campaigns and on research on the drug itself. Today it has the highest journal impact factor among its equivalents and has been a tremendous achievement when set against the concurrent performance of other journals, for example, the American Journal of Tropical Medicine and Hygiene that has a longer history and broader membership. There has also been new institutional collaborations too numerous to mention, however, most recently in the UK was the launch of the London Centre for Neglected Tropical Diseases, bringing together Imperial College London, London School of Hygiene and Tropical Medicine and the Natural History Museum. Less formal groups include the formation of ‘Global Network for Neglected Tropical Diseases’ in the USA, the ‘International Society for Neglected Tropical Diseases’ and also ‘Developing World Health’ in the UK. The latter having raised over £130,000 GBP by public donations in its 50 pence donation scheme via its website. It should be noted that there is ongoing debate as to how increased donor funds translate into tangible actions, ensuring their use in pragmatic actions is essential in maintaining continued support Citation[33].
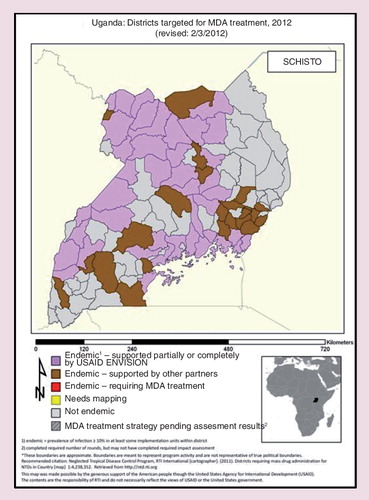
During this time the range and scope of control initiatives and implementation partners against schistosomiasis have evolved to a level never before witnessed Citation[28,31]. This change, although beneficial, has created several unforeseen consequences creating challenging times, such as, co-ordination of ‘basket’ donor funds, global purchase and in-country provision of PZQ, utilization and maintenance of procured in-country resources, as well as, standardization of operational procedures undertaken directly on-the-ground. Percolating from top to bottom and vice versa, these frictions stem at the international level by inducing competition in the selection of countries (and of course those that are not) incurring tensions, then downwards into their unique landscapes of implementation districts Citation[25,34–36]. This administrative landscape is often characterized by decentralized governance, frequently with a confused devolution of responsibilities and budgets as new projects are taken onboard Citation[37]. On the ground further confusion can be augmented by the network of local implementing agencies for example, NGDOs, which often fail to cross-talk regularly and with each sometimes having different health agenda Citation[37]. At the coal-face of control, this inevitably leads to discord in reporting of activities such as drug delivery, parasitological assessment and long-term impact of PC, as witnessed with a specific example of Uganda (see . A country with the longest recent history of integrated campaigns offering PC for NTDs, the landscape of interventions is now not simple with several implementation stakeholders; especially so since 2005 when several new districts were created and with it nascent health and educational infrastructures to dialogue with until fully functional Citation[37]. From a geographical perspective, only until recently have there been any serious attempts to service the treatment needs of marginalized populations on the numerous islands within the Ugandan part of Lake Victoria, notwithstanding movements cross-country into Kenya and Tanzania Citation[38–40]. These itinerant communities are typified as hard-to-reach and difficult-to-access populations, yet they are in greatest need of treatment, for here intestinal schistosomiasis is almost universal and particularly aggressive in pathology Citation[41,42].
In parallel with other NTDs there is, as of yet, no standardized reporting mechanism to measure ‘impact’ of control against schistosomiasis Citation[14]. Even at a simple level, this has led to some confusion on what markers could or should be reported, that is, total number of treatments administered versus percentage treatment coverage as estimated by various geographical or demographic strata (see below). At the national level, much of this has been resolved by the creation of the WHO Preventive Chemotherapy Database (PCD) that has up-to-date information reported by country. Summarizing all data collated from 2006 onwards, the website features interactive maps, summary tabulations and graphical outputs that chart ongoing progress in delivery of medications, see Citation[4]. The central importance of this website will become ever more apparent as it becomes the first point of call in measuring progress towards the 2020 WHO targets and monitoring the global demand for PZQ Citation[20,21] as well as an important archive of past actions to see within country scale-up.
A global picture of praziquantel
From 2006, it became increasingly clear that a major limitation in PC campaigns was the availability of PZQ itself, which potentially weakened the drug supply chain for other NTDs when included Citation[20,21]. Globally, PZQ was in such short supply it could not even service the given need in Africa alone, which was much greater than had been previously realized. In order to nurture this global drug supply, encouraging the future expanded production of PZQ in a coordinated and scaled-up fashion, WHO took the important step to better estimate each country’s treatment needs in a formal rationale and make a projection of future needs throughout the forthcoming decade Citation[4]. This was achieved by scaling the treatment schedules by school; see , by the associated population size of each country and its estimated national prevalence of schistosomiasis. It then became clear that prior control initiatives were only providing just less than 20% of the annual PZQ need in Africa, and some countries were completely overlooked Citation[4]. Indeed, estimating this treatment need for the 2012–2020 period is a fundamental concept in the WHO strategic plan for schistosomiasis. Foremost it is a rally-point for the pharmaceutical sector to act in unison and often in philanthropy Citation[4].
To break through this glass ceiling of PZQ production, the producers of the active ingredient of PZQ and others within the pharmaceutical industry were stimulated into action by the London Declaration on Neglected Tropical Diseases in January 2012. This meeting, chaired by Bill Gates, was a round table of 14 CEOs from key organizations with the director general of the WHO in attendance. It led to important pledges of general pharmaceutical support and goodwill, in particular from Merck-KGaA, to expand their donation of from 25 to 250 million tablets of PZQ each year, for the foreseeable future. This will directly service the need for annual treatment of school-aged children greatly facilitating the WHA54.19 target, but it should not be forgotten that additional supplies are needed for treatment of adults, as well as an appropriate formulation for infants and preschool-aged children as being developed by a public–private partnership of Merck-Serono, TI Pharma, Swiss TPH and Astellas. Spurred on by this incredible level of generosity, the WHO report Schistosomiasis progress report 2001–2011 and strategic plan 2012–2020 Citation[4] was fully endorsed by WHA65.21 in May 2012 by adopting these plans for the elimination of schistosomiasis. There is also an allied portfolio of intensified control and associated set of disease-specific targets to be reached as mapped out with specific implementation milestones .
Practicalities of school-based deworming
It is commonly held that many countries in SSA have weak health systems and are largely unable to provide children with sufficient, regular access to PZQ. With the advent of UPE and the recognition that schistosomiasis blights children’s lives, it has been a long-term feature of WHO guidelines and recommendations to co-opt educational infrastructure and staff, that is, teachers to become the first-line distributors of deworming tablets Citation[14]. Moreover, the schools are also centrally important in mapping the distribution of the disease as WHO treatment guidelines typically relate prevalence of disease by surveyed school with local treatment algorithms, . A variety of low cost, pragmatic methods are used to assess disease prevalence upon routine parasitological sampling (i.e., microscopic examination of Kato-Katz fecal smears or urine filtrates), or by questionnaire methods reporting red urine (i.e., macrohaematuria) Citation[14]. Owing to constraints in finances and logistics, however, not all schools within the putative implementation area are actually surveyed, for to do so would incur prohibitively large expenses Citation[3]. Nonetheless, striking the balance on initial survey information against realistic treatment needs is required, even more when set against short and long-term perspectives, in years and decades, respectively. This is especially important for calculations that attempt to demonstrate cost–effectiveness, in all its guises, that need quality disease-specific information at baseline. Simply put, while presumptive annual treatment of schools at-risk may be favored, if, owing to its unusual focality, schistosomiasis was actually absent within the implementation area, then allocated drugs and resources will have had no served purpose. Furthermore, this would continue to do so through time, until resources were made available downstream for retargeting Citation[3].
To include or exclude areas for control?
Addressing the exact treatment needs across a focalized landscape is not trivial Citation[3]. Where possible, rational decisions that classify areas for inclusion and exclusion should be evidence-based Citation[43,44]. Spatial epidemiological methods of disease prediction have been, and are being, used that utilize remotely sensed environmental information, for example, ground temperature or normalized differential vegetation index, to build an informative disease distribution model Citation[45–48]. Predictive models are able to classify areas with some statistical certainty as to being unfavorable, for example, being too cold, and largely unable to sustain disease transmission within the desired school sampling frame. Thus, large regions can be excluded with minimal surveying costs. However, the performance of such methods in terms of their under and over-treatment is being investigated more formally; as there are instances when they have been more miss-leading than informative, as has been discussed elsewhere Citation[42]. In terms of over-treatment, such mistakes lead to poor cost–effectiveness, however, under-treatment has serious ethical ramifications such that withholding treatment from those that need it is inequitable. Thus, failure to treat those that need it is a serious shortcoming of the modeling approach and can only be rectified by additional ‘ground-truthing’ studies to point out the real-world responsibilities to those that deal only with the theoretical. Additionally, ‘ground-truthing’ will become ever more important as future criteria to satisfy elimination will be more vigorous than that taken for initial treatment targeting Citation[42].
Once an area is selected for deworming, usually a decision taken by the Ministry of Health with outside support, a chain of strategic communications and essential dialogue between the Ministry of Education takes place to put into practice the treatment action plan Citation[14]. This is often conducted over an extended period of preparations and negotiations (typically 3–4 months or longer) allowing sufficient time for bespoke workshops for teacher training, provision of drugs and associated materials to conduct the deworming exercise as safely and as professionally as possible. Over and above, supervision of the whole process for reporting is also needed. Before deworming, formal sensitization of the parents and guardians of the children at the school-site is essential, as if not done correctly, it leads to lack of compliance, and even rejection of treatment, which can be disastrous for the control campaign Citation[49,50]. Forward timetabling and meticulous planning is therefore very important remembering to be culturally sensitive in avoiding unnecessary problems, for example, administration of treatments during Ramadan when fasting practices should be respected Citation[14].
Deworming at the school site
In terms of drug delivery, large-scale administration of PZQ at the school sites is perhaps at the lowest level in geographical stratification and key resources are highlighted at school site . It is of course possible to go lower into surrounding villages, and hamlets thereof, but this would be attempted during community-directed treatment initiatives likely using community drug distributors, who may or may not also be local school teachers Citation[14]. An important determinant of the success of deworming at the school-site is naturally the level of school-enrolled versus nonenrolled children from the surrounding area. Ambiguities between these two concepts can further percolate confusion over which denominator is to be used in the calculation of local treatment coverage. For example, treatment coverage at the school site is not the same as treatment coverage of children in the nearby vicinity. If nonenrollment levels are high then reaching the WHA54.19 will be difficult without recourse to community-directed treatment for many children will simply miss out on treatment if entirely school based. It is possible of course to adapt each local treatment strategy balancing either school- and community-based methods into the local area but on-the-ground this is labor intensive and requires accurate household census information. In fishing communities, for example, such census data are difficult to keep up-to-date when people and families are migrating and also in a population where illiteracy is widespread Citation[51].
Another ambiguity in treatment coverage is also assessing treatment coverage through time. At the onset of the SCI was an assertion that children in high endemic areas would be provided with up to three or more annual treatments during their schooling in an effort to diminish morbidity Citation[29]. In Uganda like elsewhere in SSA, school treatment registers are typically started afresh each year, so it is not always possible to capture this information, and as sorting through paper copy lists of names is intensely laborious and error-prone, it can be very difficult to assemble this information of treatments given through time retrospectively. Thus, there is a pressing need to capture these data electronically but unfortunately, there is no field-ready appropriate technology. To some extent an insight into this aspect was provided by the analyses of SCI longitudinal cohort data, however, with an annual drop out typically around 25%, the proportion of children who received three or more treatments quickly erodes Citation[30]. This is widely acknowledged as one of the problems of UPE in SSA, as the majority of children do not complete 7 years of consecutive schooling and also because the formal registration of children at each school can be hampered by illicit practices, for example, where fictitious records are kept such as pupil ghosting to increase UPE budgets allocated to each school Citation[49].
Formalization of recording treatment at the school site, although error-prone, is important for other reasons. Not only does it create a paper chain record for inspection of administered treatments but also acts as a recording mechanism for noncompliance, pharmacovigilance and adverse events Citation[14]. In recent years, this has been given much more importance as capturing the reasons why treatment is rejected when offered freely is very important in the long-term perspective. To reassure the surrounding community, direct-evidence is needed during informed local community-feedback. Once it has been explained and correctly understood that there are side-effects after treatment, owing to intensity of schistosome infections and not due to use of drugs of poor quality, compliance with treatment is usually then raised. By contrast, when these points are not well-explained, it is unsurprising that future demands for treatment quickly drops. At the school site, management of mild side-effects is straight-forward, especially if children have been given food at the time of treatment which mitigates abdominal pain Citation[14]. Later treatment discomfort can be mitigated by simple analgesics, for example, paracetamol, such that symptoms usually resolve 3–4 h after treatment. Where schistosomiasis is particularly rife, there are occasions when children need to be referred to a local health centre for a more detailed assessment. These reactions typically result from an underlying anaphylactic hypersensitivity to worm antigens as released from disturbed and dying worms brought about by PZQ treatment. While the latter can be acutely discomforting, this is most apparent during the first administration of treatment with later administrations in following years being much better tolerated.
On-site tools for treatment
Assuming that there has been satisfactory communication and training, the tools of control used at each school site are relatively simple and robust, see . The height pole or treatment stick, is perhaps the most important as PZQ is administered in 40 mg/kg bodyweight Citation[14]. It is of course possible to dose at 60 mg/kg but this would lead to a height pole of differing divisions. Similarly, the dosing by height induces a level of imprecision so in reality the dose is around 40 ± 10 mg/kg. A recent revision to the height pole to extend it downwards from 94 to 60 cm has been proposed, as was a simultaneous upward revision of the 94 cm threshold to 99 cm threshold for single tablet administration that could lead to significant drug savings, but awaits formal endorsement from WHO Citation[52,53].
At each school, a critical component is on-site access to or provision of potable water. Collecting this information during prior mapping surveys is also important but often neglected in that mapping initiatives are often overly focused on gathering parasitological information alone. Yet a broader platform for essential data capture is desirable to ensure future programmatic success. Lack of water on-site is important for two reasons Citation[14]; first drugs should be taken as safely as possible without risk of water-borne infection; second, there should be sufficient water provided to each child to allow swallowing of medications as comfortably as possible. The 600 mg oblong PZQ tablet is towards the largest range of size that can be safely tolerated in the small mouths of children. PZQ is an unusual bitter tasting medication and it is not uncommon for children to reject this medication owing to its non-palatability, especially for tablets without coatings (see below). Typically, PZQ is administered alongside other deworming drugs, such as albendazole or mebendazole which are smaller single tablets, and are often chewable and have an orange flavored formulation Citation[14].
As children report for deworming, class-by-class, registration and recording of treatments administered is usually undertaken by hand. While it is better to register formally all children within the school before deworming and then use this information for a later roll call for issuing treatment, this is often not the case. For example, registration documents are completed as children step forward for treatment without a roll call and then the head count of those treated versus numbers registered in school (typically the annual enrollment) is used as the denominator Citation[14]. Even this simple reporting exercise is not trivial in the context of the time and effort teachers have to set aside to undertake these extra duties. Summary tally sheets within the register are then completed that are reported back, along with any unused drug returned, to the respective implementation agency. Data are thus collected, collated and passed upwardly through the reporting chain for review of programmatic performance. With the advent of mobile phones with digital photographic capture and global positioning system technology, it would be desirable to speed-up collection and collation processes. While such technology is on the developmental horizon, it is likely that several years will pass before units are used routinely in large-scale drug administration settings with future safeguards against being supplanted by other technological upgrades. For the foreseeable future it is likely that achievement PC programmes will continue to report, and their performance be judged upon, a simple total number of children treated. This is a simple fixed yardstick and more favorable perhaps to use of percentage statistics that may alter widely according to which denominators are used, albeit measuring geographical, demographic and (or) temporal coverage.
Monitoring & evaluation with implementation science
One of the unique features of the SCI programme, unlike prior treatment initiatives (and some subsequently), was that a substantial budget was set aside to develop and apply conventional and experimental tools in a new portfolio of monitoring and evaluation Citation[54–56]. A fundamental problem was, however, the need to record and demonstrate changes in morbidity (over and above the dynamics of egg excretion) during the duration of the 5-year project Citation[56,57]. Morbidity research in schistosomiasis has a long history and continues to be perplexing, for at the individual level, reasons why some children progress onto disease rapidly while others do not, is presently not known Citation[57]. Inferring causality for this is complex owing to a multicausal nature of the disease itself, a potpourri of adult worm burden and accumulating numbers of trapped eggs, genetic and phenotypic diversity of the worms themselves alongside host-specific genetic and immunological factors, which is all set within a context of other local diseases, nutritional states and likely maternal effects starting in utero upon the child. Severe morbidity with schistosomiasis is obvious, visually cases of hepatosplenomegaly with ascites are topotypical but its temporal developmental is not Citation[58]. Moreover, it should be noted that morbidity may reverse in a longer time period than that available for programmatic study hence assessing which markers were best to investigate was challenging in the context of the project and available assays in a ready-to-go scenario Citation[56]. Subtle morbidity is difficult to capture but recently fitness tests have attempted to do so with some statistical success Citation[59].
For urogential schistosomiasis the problem is relatively minor as direct measures of morbidity are much more apparent, for example, macro- or micro-levels of hematuria, which in turn reflect the perforation of the bladder wall resultant from the passage of eggs into the lumen. Nonetheless, other aspects of disease recording which require use of advanced imagery, that is, ultrasound, which was often unable to be implemented on the a larger scale, so proxy markers of ultrasound were explored such as levels of excreted urine-albumin or ratios of urine-albumin versus urine-creatine Citation[60,61]. Similarly, the concept of sentinel schools was used where longitudinal child cohorts were followed and became a fundamental tenet within SCI’s monitoring and evaluation programme Citation[56]. While informative in its own right, the shortcoming of this approach included the failure to capture any changes in development of genital schistosomiasis Citation[62–64], either in boys or girls, and address more formally any interplay with other parasitic diseases, for example, malaria, a known shortcoming of vertical disease-specific programmes Citation[55]. As only PZQ and albendazole/mebendazole were being offered, ethically it was judged inappropriate to investigate other diseases without provision of treatment, which would be formally out-of-tune with practices typical of PC. Collection of this cohort data did however, attempt to highlight the importance of soil-transmitted helminthiasis (even though the occurrence of Strongyloides was overlooked due to limitations of fecal sampling methods) Citation[7].
By contrast, the dynamics of morbidity attributable to intestinal schistosomiasis are much more cryptic. Nonetheless, novel attempts were made to record and investigate the occurrence of hepatoplsenomegaly, abdominal distension and liver fibrosis Citation[58]. The latter was detected using portable ultrasonography and in so doing it became clear that in several SCI supported countries the morbidity ascribed to intestinal schistosomiasis developed earlier than previously assumed Citation[13,65]. It was then thought that morbidity was most likely to manifest in early adulthood, however, severe cases of intestinal schistosomiasis could be found in school-aged childhood. These observations were seminal as they pointed toward infection taking place much earlier in life and led to several targeted surveys that began to appreciate the significance of infection in infancy and the need for treatment in pre-school children, as mentioned above Citation[65].
EU-CONTRAST & SCORE
Alongside control operations, international funds were made available for applied research. While there have been several EU-funded projects previously, the most significant in terms of schistosomiasis was EU-CONTRAST (a multi-disciplinary alliance for schistosomiasis control and transmission surveillance), a 4-year project starting in 2006 that brought together 14 research institutes from North–South partnerships. Extensive fieldwork was undertaken, often alongside control teams, and was based in Senegal, Niger, Cameroon, Zambia, Uganda, Tanzania and Kenya. EU-CONTRAST was judged to be very successful with new insights provided into genetic diversity of schistosomes (inclusive of the detection of novel hybrid worms that have a zoonotic cycle) Citation[66,67], innovative mapping and ‘ground-truthing’ studies of disease distributions Citation[68,69], assessment of the performance of PZQ in coinfection settings (i.e., children with both intestinal and urogenital schistosomiasis) Citation[70,71], socio-economic assessments of treatment compliance and participatory hygiene and sanitation transformation method Citation[72] as well as the development of novel DNA assays to detect schistosomes in the aquatic snail stage (essential for transmission detection), with potential in human diagnostics Citation[73].
A later large-scale 5-year research study was initiated in 2008 with a slightly different research agenda, entitled Schistosomiasis Consortium for Operational Research and Evaluation (SCORE), was established from canvassing the schistosomiasis research community Citation[74]. SCORE projects included both field and laboratory-based efforts framed with a concept of ‘gaining and sustaining control’ where different treatment regimes with PZQ were investigated and how these might best synergize with alternatives for example, health education Citation[75]. A flagship project is an ambitious attempt to eliminate urogenital schistosomiasis from Zanzibar where PZQ treatment of school-children is intensified and used alongside molluscicides with the hope of eliminating morbidity and local transmission Citation[76–78]. Nested within these projects are those to evaluate present rapid diagnostic tests, namely the circulating cathodic antigen urine dipstick, which is the only commercially available test for intestinal schistosomiasis, as well as, developing new test formats with other circulating antigens Citation[75]. New diagnostics are essential when considering that present parasitological methods are insensitive and are not always able to judge effectively the performance of PZQ in terms of adult worm death, rather in terms of cessation of egg excretion . Informative reviews by King et al. also pointed to the need for further optimization of repeated PZQ treatments within highly endemic communities which may yield US$153 (S. mansoni) to 211 (S. haematobum) per additional lifetime quality adjusted life year Citation[18,79]. Translating the findings of these schemes into large-scale programmes, of course, enforces a further need for an increase in global stocks of PZQ.
Performance of PZQ
PZQ, [2-(cyclohexylcarbonyl)-1,2,3,5,7,11b-hexahydro-4H-pyrazino[2,1-a]isoquinoline-4-one] is a racemate of dextro and laevo-isomers and was originally marketed as Droncit®, as cestocide. After its activity against schistosomes was later realized, it was remarketed as Biltricide® and subsequently eclipsed in importance all other schistosomicidal drugs Citation[16]. In its original drug licensing schedule, oral dosing is at either 40 or 60 mg/kg bodyweight for adults and children (the latter of 4 years of age and older) and is given as a 600-mg oblong tablet, or in divisions thereof in half- or quarter-tablet units subject to tablet scoring Citation[80,81]. Clinical efficacy (i.e., parasitological cure) was to be judged 21–24 days after treatment and calculated upon the cessation of excretion of schistosome eggs, as detected in either stool or urine Citation[16]. Following from off-patent production of the drug by generic manufacturers, the price of each 600 mg tablet fell by over 90% to be less than US$0.10, making treatment en masse an affordable option Citation[29]. Until recently procurement of PZQ was factored into USAID and DfID budgets and then become somewhat supplanted by the London Declaration on Neglected Tropical Diseases when PZQ was pledged to be donated gratis. For example, Merck-KGaA has now committed to supply 250 million tablets each year to the Merck Praziquantel Donation Program. It is presently unclear how commercial generic producers will respond to this mixed market of donation and retail and how aid budgets will be realigned from procurement of PZQ to supporting direct costs of its distribution within PC Citation[15].
Limitations of PZQ
There are several shortcomings of PZQ, which make it a nonideal medication Citation[82]. Foremost the drug is active against adult worms alone and not juvenile stages exhibiting a biphasic mode of action Citation[83]. Being a racemate of dextro and laevo-isomers has disadvantages, for example, it is commonly held that only the laevo-isomer is active against schistosomes while the inactive dextro-isomer confers the unpleasant, bitter taste Citation[83]. The killing mechanism of the drug is not completely known, but thought to interfere with voltage-gated Ca2+ ion channels, damaging the adult worm tegument which then interacts with immune-dependant attack to the damaged worm surface Citation[16]. From an operational perspective, traditional tablets are rather cumbersome and can be difficult to swallow, which can lead to rejection or incomplete dosing in noncompliant children. It should also be noted that absorption of drug is enhanced with intake of fatty and (or) carbohydrate foods. Similarly, transitory side-effects after treatment, for example, emesis, are known which can discourage others from the treatment, hence efforts to raise acceptance and reassurance of recipients with appropriate health education is important to ensure there is no future erosion of compliance with large-scale administration Citation[15]. This is a non-trivial manner as there are several instances when rural communities have come to reject the health interventions even if well-meaning and carefully planned.
Judging the efficacy of PZQ treatment can therefore be confounded by a variety of factors, that is, from malabsorption to counterfeit drugs Citation[80]. Low cure rates and observed treatment failures can be explained in part by the presence of immature worms, which then later mature to egg-patent fecundity during the intervening period between treatment and parasitological follow-up. Similarly, in those unable to mount an immunological response that fails to synergize with the effect of treatment will manifest itself in poor cure even though the drug-specific part was satisfactory, for example, this might explain poor drug performance in very young children Citation[13,84]. It is also known that poor cure rates are reported in communities with a heavy intensity of infections Citation[85], thus even if the drug is killing the vast majority of worms, there may still be residual worms that survive initial treatment Citation[15]. Also different isolates of schistosomes have variable levels of tolerance to PZQ Citation[86], likely due to extensive genetic variation within and between worms Citation[66,67]. Hence, regular assessment of the performance of PZQ is recommended by WHO with new standard operating procedures that have been designed as a first-line guard to detect worrisome performance Citation[15]. Throughout the 2010–2012 period there were several workshops, as coordinated by WHO-Geneva, that solicited expert opinions from those involved in worm control, inclusive of representatives from the veterinary sector (where anthelmintic resistance to nematodes is well-known) Citation[55], to develop pragmatic in-field guidelines for programme managers. Novel treatment regimes using double PZQ treatment separated by 2-weeks to improve cure Citation[71,87] were discussed, as was recourse to slightly higher dosing at 60 mg/kg, although recent findings from Cochrane Reviews appear to be equivocal in terms of increased performance Citation[85]. While these research findings are important, it should not be forgotten that large-scale interventions have different programmatic bottlenecks. For example, if 60 mg/kg dosing were to be implemented then the existing 40 mg/kg height pole would be inappropriate and could be confusing to those on the ground Citation[13]. At a wider level, this increase in dosing would inflate present PZQ needs by 150%, which would further strain the global supply chain, and even more by doubling it if two separated PZQ dosing were also envisaged Citation[51].
A systematic review of PZQ performance
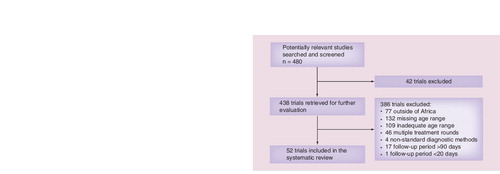
To set perhaps a formal yardstick for subsequent review in 2020 perhaps, a more formal assessment of the performance of PZQ was conducted by a computer-aided systematic search of literature of studies on antihelminthic therapies based on single standard dose praziquantel (40 mg/kg) against human schistosomiasis (with no date or language restrictions). Literature databases searched included PubMed (MEDLINE), ISI Web of Science, EMBASE and the Cochrane, up to December 2012. The following search terms were used to identify and initially select the most relevant literature: ‘schistosomiasis + praziquantel + cure rate*’ (167 hits), ‘schistosomiasis + praziquantel + efficacy’ (259 new hits), ‘Schistosoma + praziquantel + treatment’ (1831 hits) and ‘Schistosoma + praziquantel + cure rate’ (78 hits). A customized form was used to record the name of the authors, title, the year of publication, the location of the trial, the parasite species, the human population number, the age range, the study design the outcomes (cure rate and egg reduction rate), the intensity of infection (geometric or arithmetic), the study design, and dosage. Both S. mansoni and S. haematobium were included in this systematic review. The participants included schoolchildren and preschool children surveyed during targeted or community surveys. The main outcome measure was cure rate (the proportion of individuals negative for eggs in their urine/stool at follow-up). The secondary parameter was egg reduction rate and was analyzed using weighted mean difference with standard error.
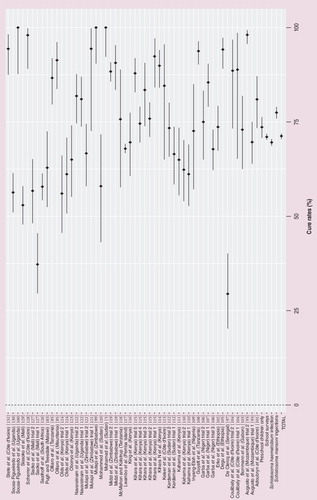
The numbers of papers initially selected and then included in the formal analysis is shown in . Statistical analysis was conducted on PZQ (40 mg/kg) administered as monotherapy (single round). Sub-group analyses were conducted according to parasite species and age-group (preschool children only vs school-based survey). All statistical analysis was performed using R-statistical package. Work conducted over the past few decades on PZQ has unveiled how complex it is to identify the actual efficacy of PZQ, as the observed efficacy of PZQ is dependent on many factors such as, parasite species Citation[88], genotype Citation[89] and developmental stage Citation[90], drug quality Citation[91] host-dependent factors Citation[84,92], transmission seasonality Citation[93,94] and infection intensity Citation[95,96]. Using a systematic review approach, we have identified 52 trials from 38 publications involving single dose (40 mg/kg) of PZQ as chemotherapy for urogenital or intestinal schistosomiasis in African children (see for selection process and for details). Cure rates achieved by these trials varied widely from 29.5% in Senegal Citation[97] to 100% in Sudan Citation[98], Zimbabwe Citation[99] and Uganda Citation[100], with an overall average cure rate of 71.3% (number treated: 13,932; 95% CI: 70.5–72.0%) .
Explanatory factors in treatment performance
When looking at the two species separately, of the trials selected 32 trials studied drug performance against urogenital schistosomiasis and 20 against intestinal schistosomiasis. Overall, drug performance against S. haematobium was 69.6% (number. treated 5048; 95% CI: 68.7–70.5%), significantly lower (p < 0.0001) than the average achieved against S. mansoni was 77.5% (number treated: 8884; 95% CI: 75.9–79.0%). For those papers eligible for inclusion, there appeared to be a negligible effect with child age, nine trials included preschool-aged children (≤6 years of age) and 43 trials included children from any age (0–23 years of age); average drug performances achieved among preschool-aged children was 73.6% (number treated: 1026; 95% CI: 70.8–76.3%) and among school-aged children was 71.1% (number treated: 12,906; 95% CI: 70.3–71.9%).
Furthermore, we have found that cure rates achieved by praziquantel are incredibly sensitive to the baseline prevalence of infection, in that the higher the prevalence the lower the cure rate . This was true according to species and age class . Interestingly, cure rates among preschool-aged children were far more affected by baseline prevalence than among school-aged children, although perhaps this was influenced by the number of trials available with prevalence data described (six trials that included preschoolers only and 40 trials that included children of any age), it has been previously noted that several factors influence cure in younger children Citation[65].
Expert commentary & five-year view
For control of schistosomiasis, it is unequivocal that performance towards reaching the target of regular single standard dose PZQ treatment to at least 75% of school-aged children, as endorsed by WHA54.19, fell well short of the 2010 mark. Should this be considered a dismal failure? We think not, for can a simple treatment coverage statistic such as this encapsulate the health benefits to those children that had access to treatment against those that had not? Can such a single target ever be relevant to capture the build-up, philanthropic support and general goodwill resultant from the international advocacy that grew from its adoption? Clearly not, as a target it acted foremost as magnet to draw in multisectoral support from those who without it would not have chosen to act. Thus fostering and nurturing this international treatment landscape has been an impressive achievement and a lasting legacy, which is set to endure, perhaps, longer than the life span of PZQ itself. If WHO predictions in reduction of schistosomiasis are to be realized, careful international harmonization and tailoring of national resources are required and maintaining an effective drug distribution system with regular drug efficacy checks is paramount. If the 2010 target is reached by 2020 then it can be safely assumed that the lives of hundreds of million children will have been improved; a laudable target we should all strive for.
Table 1. WHO-recommended treatment strategy for schistosomiasis.
Table 2. WHO vision, goals and objective for control of schistosomiasis.
Table 3. List of key needs and resources for deworming at the school site.
Table 4. Summary of characteristics of trials selected after systematic review evaluating single dose praziquantel (40 mg/kg) treating urogenital and intestinal schistosomiasis in children.
Key issues
• To secure sufficient donor funds to finance the costs of distribution of praziquantel (PZQ).
• To develop contingency planning to reduce bottlenecks in global PZQ supply.
• Reaching and sustaining treatment coverage of at least 75% in school-aged children.
• To develop the wide-scale use of mobile phone technologies for coordinating and reporting drug delivery.
• To service the treatment needs of preschool-aged children with an appropriate PZQ formulation.
• To encourage the field-use of direct morbidity markers for both forms of schistosomiasis.
• To foster application of better diagnostics for disease mapping and elimination.
• To safe-guard large-scale PZQ performance with regular drug efficacy checks.
• To advance drug discovery and treatment developments to provide future alternatives to PZQ.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- King CH. Parasites and poverty: the case of schistosomiasis. Acta Trop. 113(2), 95–104 (2010).
- Pearce EJ, MacDonald AS. The immunobiology of schistosomiasis. Nat. Rev. Immunol. 2(7), 499–511 (2002).
- Stothard JR. Improving control of African schistosomiasis: towards effective use of rapid diagnostic tests within an appropriate disease surveillance model. Trans. R. Soc. Trop. Med. Hyg. 103(4), 325–332 (2009).
- WHO. SCHISTOSOMIASIS progress report 2001–2011 Strategic Plan 2012–2020. WHO, Geneva, Switzerland (2012).
- Steinmann P, Keiser J, Bos R, Tanner M, Utzinger J. Schistosomiasis and water resources development: systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 6(7), 411–425 (2006).
- Stothard JR, Gabrielli AF. Schistosomiasis in African infants and preschool children: to treat or not to treat? Trends Parasitol. 23(3), 83–86 (2007).
- Brooker S, Kabatereine NB, Gyapong JO, Stothard JR, Utzinger J. Rapid mapping of schistosomiasis and other neglected tropical diseases in the context of integrated control programmes in Africa. Parasitology 136(13), 1707–1718 (2009).
- Emery AM, Allan FE, Rabone ME, Rollinson D. Schistosomiasis collection at NHM (SCAN). Parasit. Vectors 5, 185 (2012).
- Rollinson D, Webster JP, Webster B, Nyakaana S, Jørgensen A, Stothard JR. Genetic diversity of schistosomes and snails: implications for control. Parasitology 136(13), 1801–1811 (2009).
- Standley CJ, Mugisha L, Dobson AP, Stothard JR. Zoonotic schistosomiasis in non-human primates: past, present and future activities at the human-wildlife interface in Africa. J. Helminthol. 86(2), 131–140 (2012).
- Huyse T, Webster BL, Geldof S et al. Bidirectional introgressive hybridization between a cattle and human schistosome species. PLoS Pathog. 5(9), e1000571 (2009).
- Webster BL, Rollinson D, Stothard JR, Huyse T. Rapid diagnostic multiplex PCR (RD-PCR) to discriminate Schistosoma haematobium and S. bovis. J. Helminthol. 84(1), 107–114 (2010).
- Stothard JR, Sousa-Figueiredo JC, Betson M et al. Closing the praziquantel treatment gap: new steps in epidemiological monitoring and control of schistosomiasis in African infants and preschool-aged children. Parasitology 138(12), 1593–1606 (2011).
- WHO. Helminth control in school-age children: a guide for control programmes 2nd edition. (2011).
- Montresor A, Gabrielli AF, Chitsulo L et al. Preventive chemotherapy and the fight against neglected tropical diseases. Expert Rev. Anti. Infect. Ther. 10(2), 237–242 (2012).
- Doenhoff MJ, Cioli D, Utzinger J. Praziquantel: mechanisms of action, resistance and new derivatives for schistosomiasis. Curr. Opin. Infect. Dis. 21(6), 659–667 (2008).
- Hotez PJ, Molyneux DH, Fenwick A et al. Control of neglected tropical diseases. N. Engl. J. Med. 357(10), 1018–1027 (2007).
- King CH, Olbrych SK, Soon M, Singer ME, Carter J, Colley DG. Utility of repeated praziquantel dosing in the treatment of schistosomiasis in high-risk communities in Africa: a systematic review. PLoS Negl. Trop. Dis. 5(9), e1321 (2011).
- Fenwick A, Rollinson D, Southgate V. Implementation of human schistosomiasis control: challenges and prospects. In: Advances in Parasitology, Vol 61: Control of Human Parasitic Diseases. (2006).
- Hotez PJ, Engels D, Fenwick A, Savioli L. Africa is desperate for praziquantel. Lancet 376(9740), 496–498 (2010).
- Hotez PJ, Fenwick A. Schistosomiasis in Africa: an emerging tragedy in our new global health decade. PLoS Neglect. Trop. Dis. 3(9), e485 (2009).
- Hotez PJ, Fenwick A, Savioli L, Molyneux DH. Rescuing the bottom billion through control of neglected tropical diseases. Lancet 373(9674), 1570–1575 (2009).
- Hotez PJ, Molyneux DH, Fenwick A, Ottesen E, Ehrlich Sachs S, Sachs JD. Incorporating a rapid-impact package for neglected tropical diseases with programs for HIV/AIDS, tuberculosis, and malaria. PLoS Med. 3(5), e102 (2006).
- Fleming FM, Fenwick A, Tukahebwa EM et al. Process evaluation of schistosomiasis control in Uganda, 2003 to 2006: perceptions, attitudes and constraints of a national programme. Parasitology 136(13), 1759–1769 (2009).
- Garba A, Touré S, Dembelé R et al. Present and future schistosomiasis control activities with support from the Schistosomiasis Control Initiative in West Africa. Parasitology 136(13), 1731–1737 (2009).
- Brooker S, Kabatereine NB, Fleming F, Devlin N. Cost and cost–effectiveness of nationwide school-based helminth control in Uganda: intra-country variation and effects of scaling-up. Health Policy Plan. 23(1), 24–35 (2008).
- Leslie J, Garba A, Oliva EB et al. Schistosomiasis and soil-transmitted helminth control in Niger: cost–effectiveness of school based and community distributed mass drug administration [corrected]. PLoS Negl. Trop. Dis. 5(10), e1326 (2011).
- Savioli L, Gabrielli AF, Montresor A, Chitsulo L, Engels D. Schistosomiasis control in Africa: 8 years after World Health Assembly Resolution 54.19. Parasitology 136(13), 1677–1681 (2009).
- Fenwick A. New initiatives against Africa’s worms. Trans. R. Soc. Trop. Med. Hyg. 100(3), 200–207 (2006).
- Zhang Y, Koukounari A, Kabatereine N et al. Parasitological impact of 2-year preventive chemotherapy on schistosomiasis and soil-transmitted helminthiasis in Uganda. BMC Med. 5, 27 (2007).
- Hotez P, Raff S, Fenwick A, Richards F Jr, Molyneux DH. Recent progress in integrated neglected tropical disease control. Trends Parasitol. 23(11), 511–514 (2007).
- Hotez P. A new voice for the poor. Plos Negl. Trop. Dis. 1(1), (2007).
- Allen T, Parker M. Will increased funding for neglected tropical diseases really make poverty history? Lancet 379(9821), 1097–1098; author reply 1098 (2012).
- Kabatereine NB, Fleming FM, Nyandindi U, Mwanza JC, Blair L. The control of schistosomiasis and soil-transmitted helminths in East Africa. Trends Parasitol. 22(7), 332–339 (2006).
- Kolaczinski JH, Kabatereine NB, Onapa AW, Ndyomugyenyi R, Kakembo AS, Brooker S. Neglected tropical diseases in Uganda: the prospect and challenge of integrated control. Trends Parasitol. 23(10), 485–493 (2007).
- Tchuente LAT, N’goran EK. Schistosomiasis and soil-transmitted helminthiasis control in Cameroon and Cote d’Ivoire: implementing control on a limited budget. Parasitology 136(13), 1739–1745 (2009).
- Kabatereine NB, Malecela M, Lado M, Zaramba S, Amiel O, Kolaczinski JH. How to (or not to) integrate vertical programmes for the control of major neglected tropical diseases in sub-Saharan Africa. PLoS Negl. Trop. Dis. 4(6), e755 (2010).
- Kabatereine NB, Standley CJ, Sousa-Figueiredo JC et al. Integrated prevalence mapping of schistosomiasis, soil-transmitted helminthiasis and malaria in lakeside and island communities in Lake Victoria, Uganda. Parasit. Vectors 4, 232 (2011).
- Standley CJ, Adriko M, Arinaitwe M et al. Epidemiology and control of intestinal schistosomiasis on the Sesse Islands, Uganda: integrating malacology and parasitology to tailor local treatment recommendations. Parasit. Vectors 3(1), 64 (2010).
- Standley CJ, Adriko M, Besigye F, Kabatereine NB, Stothard RJ. Confirmed local endemicity and putative high transmission of Schistosoma mansoni in the Sesse Islands, Lake Victoria, Uganda. Parasit. Vectors 4, 29 (2011).
- Parker M, Allen T, Pearson G, Peach N, Flynn R, Rees N. Border parasites: schistosomiasis control among Uganda’s fisherfolk. J. Eastern African Studies 6(1), 98–123 (2012).
- Standley CJ, Stothard JR. Towards defining appropriate strategies for targeted NTD control. Trop. Med. Int. Health 15(6), 772–773 (2010).
- Sturrock HJW, Gething PW, Ashton RA, Kolaczinski JH, Kabatereine NB, Brooker S. Planning schistosomiasis control: investigation of alternative sampling strategies for Schistosoma mansoni to target mass drug administration of praziquantel in East Africa. Int. Health 3(3), 165–175 (2011).
- Sturrock HJ, Gething PW, Clements AC, Brooker S. Optimal survey designs for targeting chemotherapy against soil-transmitted helminths: effect of spatial heterogeneity and cost-efficiency of sampling. Am. J. Trop. Med. Hyg. 82(6), 1079–1087 (2010).
- Clements AC, Bosqué-Oliva E, Sacko M et al. A comparative study of the spatial distribution of schistosomiasis in Mali in 1984–1989 and 2004–2006. PLoS Negl. Trop. Dis. 3(5), e431 (2009).
- Clements ACA, Brooker S, Nyandindi U, Fenwick A, Blair L. Bayesian spatial analysis of a national urinary schistosomiasis questionnaire to assist geographic targeting of schistosomiasis control in Tanzania, East Africa. Int. J. Parasitol. 38(3–4), 401–415 (2008).
- Clements AC, Deville MA, Ndayishimiye O, Brooker S, Fenwick A. Spatial co-distribution of neglected tropical diseases in the east African great lakes region: revisiting the justification for integrated control. Trop. Med. Int. Health 15(2), 198–207 (2010).
- Clements AC, Garba A, Sacko M et al. Mapping the probability of schistosomiasis and associated uncertainty, West Africa. Emerging Infect. Dis. 14(10), 1629–1632 (2008).
- Parker M, Allen T. Does mass drug administration for the integrated treatment of neglected tropical diseases really work? Assessing evidence for the control of schistosomiasis and soil-transmitted helminths in Uganda. Health Res. Policy Systems 9, 3 (2011).
- Parker M, Allen T, Hastings J. Resisting control of neglected tropical diseases: dilemmas in the mass treatment of schistosomiasis and soil-transmitted helminths in north-west Uganda. J. Biosoc. Sci. 40(2), 161–181 (2008).
- Stothard JR, Chitsulo L, Kristensen TK, Utzinger J. Control of schistosomiasis in sub-Saharan Africa: progress made, new opportunities and remaining challenges. Parasitology 136(13), 1665–1675 (2009).
- Sousa-Figueiredo JC, Betson M, Stothard JR. Treatment of schistosomiasis in African infants and preschool-aged children: downward extension and biometric optimization of the current praziquantel dose pole. Int. Health 4(2), 95–102 (2012).
- Sousa-Figueiredo JC, Day M, Betson M, Kabatereine NB, Stothard JR. An inclusive dose pole for treatment of schistosomiasis in infants and preschool children with praziquantel. Trans. R. Soc. Trop. Med. Hyg. 104(11), 740–742 (2010).
- Fenwick A, Webster JP, Bosque-Oliva E et al. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002-2008. Parasitology 136(13), 1719–1730 (2009).
- Basáñez MG, French MD, Walker M, Churcher TS. Paradigm lost: how parasite control may alter pattern and process in human helminthiases. Trends Parasitol. 28(4), 161–171 (2012).
- Brooker S, Whawell S, Kabatereine NB, Fenwick A, Anderson RM. Evaluating the epidemiological impact of national control programmes for helminths. Trends Parasitol. 20(11), 537–545 (2004).
- Webster JP, Koukounari A, Lamberton PH, Stothard JR, Fenwick A. Evaluation and application of potential schistosome-associated morbidity markers within large-scale mass chemotherapy programmes. Parasitology 136(13), 1789–1799 (2009).
- Balen J, Stothard JR, Kabatereine NB et al. Morbidity due to Schistosoma mansoni: an epidemiological assessment of distended abdomen syndrome in Ugandan school children with observations before and 1-year after anthelminthic chemotherapy. Trans. R. Soc. Trop. Med. Hyg. 100(11), 1039–1048 (2006).
- Bustinduy AL, Thomas CL, Fiutem JJ et al. Measuring fitness of Kenyan children with polyparasitic infections using the 20-meter shuttle run test as a morbidity metric. PLoS Negl. Trop. Dis. 5(7), e1213 (2011).
- Sousa-Figueiredo JC, Basáñez MG, Khamis IS, Garba A, Rollinson D, Stothard JR. Measuring morbidity associated with urinary schistosomiasis: assessing levels of excreted urine albumin and urinary tract pathologies. PLoS Negl. Trop. Dis. 3(10), e526 (2009).
- Stothard JR, Sousa-Figueiredo JC, Simba Khamis I, Garba A, Rollinson D. Urinary schistosomiasis-associated morbidity in schoolchildren detected with urine albumin-to-creatinine ratio (UACR) reagent strips. J. Pediatr. Urol. 5(4), 287–291 (2009).
- Stoever K, Molyneux D, Hotez P, Fenwick A. HIV/AIDS, schistosomiasis, and girls. Lancet 373(9680), 2025–2026 (2009).
- Kjetland EF, Leutscher PD, Ndhlovu PD. A review of female genital schistosomiasis. Trends Parasitol. 28(2), 58–65 (2012).
- Stothard JR. Female genital schistosomiasis – icebergs of morbidity ahead? Trends Parasitol. 28(5), 174–175 (2012).
- Stothard JR, Sousa-Figueiredo JC, Betson M, Bustinduy A, Reinhard-Rupp J. Schistosomiasis in African infants and preschool children: let them now be treated! Trends Parasitol. 29(4), 197–205 (2013).
- Webster BL, Culverwell CL, Khamis IS, Mohammed KA, Rollinson D, Stothard JR. DNA barcoding of Schistosoma haematobium on Zanzibar reveals substantial genetic diversity and two major phylogenetic groups. Acta Tropica doi:10.1371/journal.pntd.0001882 (2012) (In Press).
- Webster BL, Webster JP, Gouvras AN et al. DNA ‘barcoding’ of Schistosoma mansoni across sub-Saharan Africa supports substantial within locality diversity and geographical separation of genotypes. Acta Tropica (2012) (In Press).
- Stothard JR, Ameri H, Khamis IS et al. Parasitological and malacological surveys reveal urogenital schistosomiasis on Mafia Island, Tanzania to be an imported infection. Acta Trop. doi:10.1016/j.actatropica.2012.09.006 (2012) (In Press).
- Schur N, Hürlimann E, Stensgaard AS et al. Spatially explicit Schistosoma infection risk in eastern Africa using Bayesian geostatistical modelling. Acta Trop. doi:10.1016/j.actatropica.2011.10.006 (2011) (Epub ahead of print).
- Gouvras AN, Kariuki C, Koukounari A et al. The impact of single versus mixed Schistosoma haematobium and S. mansoni infections on morbidity profiles amongst school-children in Taveta, Kenya. Acta Trop. doi:10.1016/j.actatropica.2013.01.001 (2013) (Epub ahead of print).
- Webster BL, Diaw OT, Seye MM et al. Praziquantel treatment of school children from single and mixed infection foci of intestinal and urogenital schistosomiasis along the Senegal river basin: monitoring treatment success and re-infection patterns. Acta Trop. (2012) In Press.
- Mwanga JR, Lwambo NJS. Pre- and post-intervention perceptions and water contact behaviour related to schistosomiasis in north-western Tanzania. Acta Tropica doi:10.1016/j.actatropica.2012.09.017 (2012) (In Press).
- Kane RA, Stothard JR, Rollinson D et al. Detection and quantification of schistosome DNA in freshwater snails using either fluorescent probes in real-time PCR or oligochromatographic dipstick assays targeting the ribosomal intergenic spacer. Acta Trop. doi:10.1016/j.actatropica.2011.10.019 (2011) (Epub ahead of print).
- Colley DG, Secor WE. A schistosomiasis research agenda. PLoS Negl. Trop. Dis. 1(3), e32 (2007).
- King C, Colley D, Binder S, Campbell C. A progress report from score, the schistosomiasis consortium for operational research and evaluation. Trop. Med. Int. Health 16, 330 (2011).
- Rollinson D, Knopp S, Levitz S et al. Time to set the agenda for schistosomiasis elimination. Acta Trop. doi:10.1016/j.actatropica.2012.04.013 (2012) (Epub ahead of print).
- Knopp S, Stothard JR, Rollinson D et al. From morbidity control to transmission control: time to change tactics against helminths on Unguja Island, Zanzibar. Acta Tropica doi:10.1016/j.actatropica.2011.04.010 (2011) (In Press)
- Knopp S, Mohammed KA, Ali SM et al. Study and implementation of urogenital schistosomiasis elimination in Zanzibar (Unguja and Pemba islands) using an integrated multidisciplinary approach. BMC Public Health 12, 930 (2012).
- King CH, Bertino AM. Asymmetries of poverty: why global burden of disease valuations underestimate the burden of neglected tropical diseases. PLoS Negl. Trop. Dis. 2(3), e209 (2008).
- Doenhoff MJ, Pica-Mattoccia L. Praziquantel for the treatment of schistosomiasis: its use for control in areas with endemic disease and prospects for drug resistance. Expert Rev. Anti. Infect. Ther. 4(2), 199–210 (2006).
- Fenwick A, Savioli L, Engels D, Robert Bergquist N, Todd MH. Drugs for the control of parasitic diseases: current status and development in schistosomiasis. Trends Parasitol. 19(11), 509–515 (2003).
- Cioli D, Valle C, Angelucci F, Miele AE. Will new antischistosomal drugs finally emerge? Trends Parasitol. 24(9), 379–382 (2008).
- Cioli D, Basso A, Valle C, Pica-Mattoccia L. Decades down the line: the viability of praziquantel for future schistosomiasis treatment. Expert Rev. Anti. Infect. Ther. 10(8), 835–837 (2012).
- Doenhoff MJ, Modha J, Lambertucci JR, McLaren DJ. The immune dependence of chemotherapy. Parasitol. Today (Regul. Ed.) 7(1), 16–18 (1991).
- Olliaro PL, Vaillant MT, Belizario VJ et al. A multicentre randomized controlled trial of the efficacy and safety of single-dose praziquantel at 40 mg/kg vs. 60 mg/kg for treating intestinal schistosomiasis in the Philippines, Mauritania, Tanzania and Brazil. PLoS Negl. Trop. Dis. 5(6), e1165 (2011).
- Melman SD, Steinauer ML, Cunningham C et al. Reduced susceptibility to praziquantel among naturally occurring Kenyan isolates of Schistosoma mansoni. PLoS Negl. Trop. Dis. 3(8), e504 (2009).
- Garba A, Lamine MS, Barkiré N et al. Efficacy and safety of two closely spaced doses of praziquantel against Schistosoma haematobium and S. mansoni and re-infection patterns in school-aged children in Niger. Acta Trop. doi:10.1016/j.actatropica.2012.08.008 (2012) (In Press).
- Wegner DH. The profile of the trematodicidal compound praziquantel. Arzneimittelforschung. 34(9B), 1132–1136 (1984).
- Lamberton PH, Hogan SC, Kabatereine NB, Fenwick A, Webster JP. In vitro praziquantel test capable of detecting reduced in vivo efficacy in Schistosoma mansoni human infections. Am. J. Trop. Med. Hyg. 83(6), 1340–1347 (2010).
- Doenhoff MJ, Hagan P, Cioli D et al. Praziquantel: its use in control of schistosomiasis in sub-Saharan Africa and current research needs. Parasitology 136(13), 1825–1835 (2009).
- Sulaiman SM, Traoré M, Engels D, Hagan P, Cioli D. Counterfeit praziquantel. Lancet 358(9282), 666–667 (2001).
- Mutapi F, Ndhlovu PD, Hagan P, Woolhouse ME. A comparison of humoral responses to Schistosoma haematobium in areas with low and high levels of infection. Parasite Immunol. 19(6), 255–263 (1997).
- Augusto G, Magnussen P, Kristensen TK, Appleton CC, Vennervald BJ. The influence of transmission season on parasitological cure rates and intensity of infection after praziquantel treatment of Schistosoma haematobium-infected schoolchildren in Mozambique. Parasitology 136(13), 1771–1779 (2009).
- Abu-Elyazeed RR, Mansour NS, Youssef FG et al. Seasonality as a determinant of the efficacy of praziquantel in population-based chemotherapy: lessons from the practice. J. Egypt. Soc. Parasitol. 28(1), 1–7 (1998).
- Utzinger J, N’Goran EK, N’Dri A, Lengeler C, Tanner M. Efficacy of praziquantel against Schistosoma mansoni with particular consideration for intensity of infection. Trop. Med. Int. Health 5(11), 771–778 (2000).
- Raso G, N’Goran EK, Toty A et al. Efficacy and side effects of praziquantel against Schistosoma mansoni in a community of western Côte d’Ivoire. Trans. R. Soc. Trop. Med. Hyg. 98(1), 18–27 (2004).
- De Clercq D, Vercruysse J, Kongs A, Verlé P, Dompnier JP, Faye PC. Efficacy of artesunate and praziquantel in Schistosoma haematobium infected schoolchildren. Acta Trop. 82(1), 61–66 (2002).
- Mohamed AA, Mahgoub HM, Magzoub M et al. Artesunate plus sulfadoxine/pyrimethamine versus praziquantel in the treatment of Schistosoma mansoni in eastern Sudan. Trans. R. Soc. Trop. Med. Hyg. 103(10), 1062–1064 (2009).
- Mutapi F, Ndhlovu PD, Hagan P, Woolhouse ME. Changes in specific anti-egg antibody levels following treatment with praziquantel for Schistosoma haematobium infection in children. Parasite Immunol. 20(12), 595–600 (1998).
- Sousa-Figueiredo JC, Pleasant J, Day M et al. Treatment of intestinal schistosomiasis in Ugandan preschool children: best diagnosis, treatment efficacy and side-effects, and an extended praziquantel dosing pole. Int. Health 2(2), 103–113 (2010).
- Adoubryn KD, Kouadio-Yapo CG, Ouhon J, Aka NA, Bintto F, Assoumou A. Intestinal parasites in children in Biankouma, Ivory Coast (mountaineous western region): efficacy and safety of praziquantel and albendazole. Med. Sante. Trop. 22(2), 170–176 (2012).
- Erko B, Degarege A, Tadesse K, Mathiwos A, Legesse M. Efficacy and side effects of praziquantel in the treatment of Schistosomiasis mansoni in schoolchildren in Shesha Kekele elementary school, Wondo Genet, Southern Ethiopia. Asian Pacific J. Trop. Biomed. 235–239 (2012).
- Borrmann S, Szlezák N, Faucher JF et al. Artesunate and praziquantel for the treatment of Schistosoma haematobium infections: a double-blind, randomized, placebo-controlled study. J. Infect. Dis. 184(10), 1363–1366 (2001).
- Coulibaly JT, N’gbesso YK, Knopp S, Keiser J, N’Goran EK, Utzinger J. Efficacy and safety of praziquantel in preschool-aged children in an area co-endemic for Schistosoma mansoni and S. haematobium. PLoS Negl. Trop. Dis. 6(12), e1917 (2012).
- Degu G, Mengistu G, Jones J. Praziquantel efficacy against schistosomiasis mansoni in schoolchildren in north-west Ethiopia. Trans. R. Soc. Trop. Med. Hyg. 96(4), 444–445 (2002).
- Garba A, Lamine MS, Djibo A et al. Safety and efficacy of praziquantel syrup (Epiquantel(®)) against Schistosoma haematobium and Schistosoma mansoni in preschool-aged children in Niger. Acta Trop. doi:10.1016/j.actatropica.2012.12.003 (2012) (Epub ahead of print).
- Garba A, Tohon Z, Sidiki A, Chippaux JP, de Chabalier F. [Efficacity of praziquantel in school-aged children in a hyperendemic zone for Schistoma haematobium (Niger, 1999)]. Bull. Soc. Pathol. Exot. 94(1), 42–45 (2001).
- Guyatt HL, Brooker S, Kihamia CM, Hall A, Bundy DA. Evaluation of efficacy of school-based anthelmintic treatments against anaemia in children in the United Republic of Tanzania. Bull. World Health Organ. 79(8), 695–703 (2001).
- Inyang-Etoh PC, Ejezie GC, Useh MF, Inyang-Etoh EC. Efficacy of a combination of praziquantel and artesunate in the treatment of urinary schistosomiasis in Nigeria. Trans. R. Soc. Trop. Med. Hyg. 103(1), 38–44 (2009).
- Kahama AI, Vennervald BJ, Kombe Y et al. Parameters associated with Schistosoma haematobium infection before and after chemotherapy in school children from two villages in the coast province of Kenya. Trop. Med. Int. Health 4(5), 335–340 (1999).
- Kahama AI, Odek AE, Kihara RW et al. Urine circulating soluble egg antigen in relation to egg counts, hematuria, and urinary tract pathology before and after treatment in children infected with Schistosoma haematobium in Kenya. Am. J. Trop. Med. Hyg. 61(2), 215–219 (1999).
- Kardaman MW, Fenwick A, el Igail AB, el Tayeb M, Daffalla AA, Dixon HG. Treatment with praziquantel of schoolchildren with concurrent Schistosoma mansoni and S. haematobium infections in Gezira, Sudan. J. Trop. Med. Hyg. 88(2), 105–109 (1985).
- Keiser J, N’Guessan NA, Adoubryn KD et al. Efficacy and safety of mefloquine, artesunate, mefloquine-artesunate, and praziquantel against Schistosoma haematobium: randomized, exploratory open-label trial. Clin. Infect. Dis. 50(9), 1205–1213 (2010).
- Kihara JH, Njagi EN, Kenya EU et al. Urinary soluble egg antigen levels in Schistosoma haematobium infection in relation to sex and age of Kenyan schoolchildren following praziquantel treatment. Trans. R. Soc. Trop. Med. Hyg. 103(10), 1024–1030 (2009).
- Kihara JH, Muhoho N, Njomo D et al. Drug efficacy of praziquantel and albendazole in school children in Mwea Division, Central Province, Kenya. Acta Trop. 102(3), 165–171 (2007).
- King CH, Muchiri EM, Mungai P et al. Randomized comparison of low-dose versus standard-dose praziquantel therapy in treatment of urinary tract morbidity due to Schistosoma haematobium infection. Am. J. Trop. Med. Hyg. 66(6), 725–730 (2002).
- Lwambo NJ, Savioli L, Kisumku UM, Alawi KS, Bundy DA. The relationship between prevalence of Schistosoma haematobium infection and different morbidity indicators during the course of a control programme on Pemba Island. Trans. R. Soc. Trop. Med. Hyg. 91(6), 643–646 (1997).
- McMahon JE, Kolstrup N. Praziquantel: a new schistosomicide against Schistosoma haematobium. Br. Med. J. 2(6202), 1396–1399 (1979).
- Midzi N, Sangweme D, Zinyowera S et al. Efficacy and side effects of praziquantel treatment against Schistosoma haematobium infection among primary school children in Zimbabwe. Trans. R. Soc. Trop. Med. Hyg. 102(8), 759–766 (2008).
- Mohammed EH, Eltayeb M, Ibrahim H. Haematological and biochemical morbidity of Schistosoma haematobium in school children in Sudan. Sultan Qaboos Univ. Med. J. 6(2), 59–64 (2006).
- Mutapi F, Rujeni N, Bourke C et al. Schistosoma haematobium treatment in 1–5 year old children: safety and efficacy of the antihelminthic drug praziquantel. PLoS Negl. Trop. Dis. 5(5), e1143 (2011).
- Navaratnam AM, Sousa-Figueiredo JC, Stothard JR, Kabatereine NB, Fenwick A, Mutumba-Nakalembe MJ. Efficacy of praziquantel syrup versus crushed praziquantel tablets in the treatment of intestinal schistosomiasis in Ugandan preschool children, with observation on compliance and safety. Trans. R. Soc. Trop. Med. Hyg. 106(7), 400–407 (2012).
- Obonyo CO, Muok EM, Mwinzi PN. Efficacy of artesunate with sulfalene plus pyrimethamine versus praziquantel for treatment of Schistosoma mansoni in Kenyan children: an open-label randomised controlled trial. Lancet Infect. Dis. 10(9), 603–611 (2010).
- Olds GR, King C, Hewlett J et al. Double-blind placebo-controlled study of concurrent administration of albendazole and praziquantel in schoolchildren with schistosomiasis and geohelminths. J. Infect. Dis. 179(4), 996–1003 (1999).
- Pugh RN, Teesdale CH. Single dose oral treatment in urinary schistosomiasis: a double blind trial. Br. Med. J. (Clin. Res. Ed). 286(6363), 429–432 (1983).
- Saathoff E, Olsen A, Magnussen P, Kvalsvig JD, Becker W, Appleton CC. Patterns of Schistosoma haematobium infection, impact of praziquantel treatment and re-infection after treatment in a cohort of schoolchildren from rural KwaZulu-Natal/South Africa. BMC Infect. Dis. 4, 40 (2004).
- Sacko M, Magnussen P, Traoré M et al. The effect of single dose versus two doses of praziquantel on Schistosoma haematobium infection and pathology among school-aged children in Mali. Parasitology 136(13), 1851–1857 (2009).
- Scherrer AU, Sjöberg MK, Allangba A et al. Sequential analysis of helminth egg output in human stool samples following albendazole and praziquantel administration. Acta Trop. 109(3), 226–231 (2009).
- Sissoko MS, Dabo A, Traoré H et al. Efficacy of artesunate + sulfamethoxypyrazine/pyrimethamine versus praziquantel in the treatment of Schistosoma haematobium in children. PLoS ONE 4(10), e6732 (2009).
- Sousa-Figueiredo JC, Betson M, Atuhaire A et al. Performance and safety of praziquantel for treatment of intestinal schistosomiasis in infants and preschool children. PLoS Negl. Trop. Dis. 6(10), e1864 (2012).
- Stete K, Krauth SJ, Coulibaly JT et al. Dynamics of Schistosoma haematobium egg output and associated infection parameters following treatment with praziquantel in school-aged children. Parasit. Vectors 5, 298 (2012).
Website
- Newsletter – ‘Action Against Worms’. www.who.int/neglected_diseases/preventive_chemotherapy/pctnewsletter/en/