
Abstract
Solid tumors of various etiologies can be treated efficiently by electrochemotherapy (ECT), a combined use of electroporation (EP) and chemotherapeutic drugs, such as bleomycin and cisplatin. EP alone and ECT in particular, induce a profound reduction in tumor blood flow, which contributes to the antitumor effect. After EP and ECT, the time course of blood flow changes and follows the same two-phase pattern. The first rapid and short-lived vasoconstriction phase is followed by the second much longer-lived phase resulting from disrupted cytoskeletal structures and a compromised barrier function of the microvascular endothelium. In the case of ECT, however, tumor vascular endothelial cells are also affected by the chemotherapeutic drug, which leads to irrecoverable damage to tumor vessels and to a further decrease in tumor blood flow within hours after application of ECT. Tumor cells surviving the direct effects of ECT are consequently exposed to lack of oxygen and nutrients and are pushed into the secondary cascade of induced cell death. Clinically, the antitumor effectiveness of ECT has been proven extensively in the treatment of melanoma metastases, with 70–80% complete responses. The antivascular effects of ECT were also exploited for palliative treatment of bleeding melanoma metastases, with immediate cessation of bleeding and very good antitumor effectiveness. The antivascular effect of ECT is of utmost importance for translation of ECT into the treatment of deep-seated tumors, especially in well vascularized organs, such as the liver, where it prevents bleeding of the treated area.
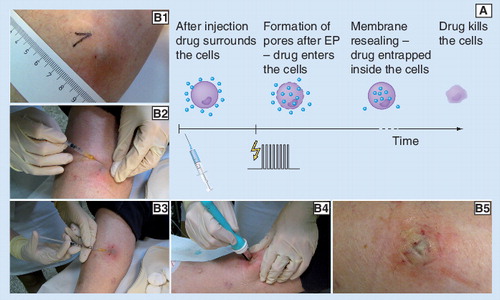
(A) The main mechanism of ECT and (B1–5) an example of a clinical ECT procedure are presented. In this example a subcutaneous melanoma metastasis on the lower leg was treated on an outpatient basis by ECT with cisplatin: (B1) tumor before treatment; (B2) application of local anesthesia; (B3) intratumoral injection of cisplatin; (B4) application of electric pulses using parallel plate electrodes; (B5) treated area immediately after treatment. Note the bluish-pale color of the treated area in the last photograph (indication of locally arrested tumor blood flow and the beginning of edema formation). For an example of the long-term effect of ECT on a bleeding melanoma tumor see .
EP: Electroporation.
(A) An example of rapid decrease in blood flow immediately after application of EP pulses. Movement artifacts caused by electric pulses and respiration can be seen in the unfiltered raw signal. (B–D) The effects of different treatments on blood flow over three different time frames. All data were measured in subcutaneous Sa-1 tumors in anesthetized A/J mice. OxyFlo laser Doppler flowmeter with bare fiber probes was used in A–C (Oxford Optronix, Oxford, UK) and PBV staining technique in D. For electrochemotherapy (ECT) bleomycin (1 mg/kg) was injected intravenously 3 min prior to application of EP. EP (eight pulses, amplitude 1040 V, duration 100 µs, 1 Hz, plate electrodes, 8 mm distance) was delivered at time 0. In B–D the data points represent the mean average blood flow and standard error of the mean (N ≥13 in figures B & C and N ≥3 in figure D). In figures B & C the values are expressed relatively as percentage of the pretreatment value.
EP: Electroporation.
Redrawn from Citation[66] in accordance with the ‘License to publish’ of British Journal of Cancer.
![Figure 2. Changes in tumor blood flow after different treatments.(A) An example of rapid decrease in blood flow immediately after application of EP pulses. Movement artifacts caused by electric pulses and respiration can be seen in the unfiltered raw signal. (B–D) The effects of different treatments on blood flow over three different time frames. All data were measured in subcutaneous Sa-1 tumors in anesthetized A/J mice. OxyFlo laser Doppler flowmeter with bare fiber probes was used in A–C (Oxford Optronix, Oxford, UK) and PBV staining technique in D. For electrochemotherapy (ECT) bleomycin (1 mg/kg) was injected intravenously 3 min prior to application of EP. EP (eight pulses, amplitude 1040 V, duration 100 µs, 1 Hz, plate electrodes, 8 mm distance) was delivered at time 0. In B–D the data points represent the mean average blood flow and standard error of the mean (N ≥13 in figures B & C and N ≥3 in figure D). In figures B & C the values are expressed relatively as percentage of the pretreatment value.EP: Electroporation.Redrawn from Citation[66] in accordance with the ‘License to publish’ of British Journal of Cancer.](/cms/asset/ff80c577-c8c5-484b-a0b8-29e244203687/iery_a_11219500_f0002_b.jpg)
The endothelial cell monolayer was exposed to three electric pulses (duration 100 µs, repetition frequency 1 Hz, amplitude 40 V, interelectrode distance 4 mm) in situ. Microtubules and actin filaments were stained with an anti-β-tubulin antibody and phalloidin respectively and analyzed by fluorescence microscopy. Before EP, cells displayed intact actin filament and microtubule networks. After application of EP, staining of actin fibers with phalloidin appeared diffused demonstrating dissociation of actin fibers, while microtubules became fragmented. Microtubule and microfilament networks recovered their structural composition within 1 h after exposure to electric pulses at amplitude of 40 V.
EP: Electroporation.
Reproduced with permission from Citation[86].
![Figure 3. The effect of EP on human umbilical vein endothelial cells.The endothelial cell monolayer was exposed to three electric pulses (duration 100 µs, repetition frequency 1 Hz, amplitude 40 V, interelectrode distance 4 mm) in situ. Microtubules and actin filaments were stained with an anti-β-tubulin antibody and phalloidin respectively and analyzed by fluorescence microscopy. Before EP, cells displayed intact actin filament and microtubule networks. After application of EP, staining of actin fibers with phalloidin appeared diffused demonstrating dissociation of actin fibers, while microtubules became fragmented. Microtubule and microfilament networks recovered their structural composition within 1 h after exposure to electric pulses at amplitude of 40 V.EP: Electroporation.Reproduced with permission from Citation[86].](/cms/asset/5f509d48-68e7-496f-9a9c-c64ebce264b0/iery_a_11219500_f0003_b.jpg)
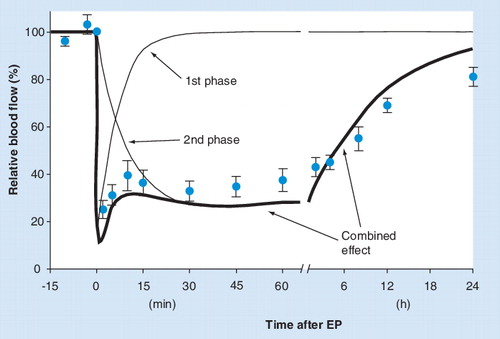
The total perfusion change (thicker line) observed in solid tumors after EP is modeled here as a sum of two simple biexponential functions with different time constants (thin lines). For comparison with experimental data, the data points for EP from are superimposed on the model. A more elaborate mathematical representation of the two components in the model would have to be used to fully describe the actual blood flow data, but the general adequacy of a two-phase model to describe the experimental data is obvious.
EP: Electroporation.
The results of the PBV-staining technique are shown. Symbols represent mean values of at least six mice with standard error of the mean. Time 0 corresponds to the pretreatment value. Bleomycin and cisplatin were injected 3 min prior to EP at doses 5 mg/kg and 4 mg/kg, respectively. EP protocol: eight pulses, amplitude 1040 V, duration 100 µs, 1 Hz, plate electrodes, interelectrode distance 8 mm.
ECT: Electrochemotherapy; EP: Electroporation.
Based on combined data from Citation[67,81,82].
![Figure 5. Electrochemotherapy with cisplatin and bleomycin: comparison of the effects on blood flow in tumors.The results of the PBV-staining technique are shown. Symbols represent mean values of at least six mice with standard error of the mean. Time 0 corresponds to the pretreatment value. Bleomycin and cisplatin were injected 3 min prior to EP at doses 5 mg/kg and 4 mg/kg, respectively. EP protocol: eight pulses, amplitude 1040 V, duration 100 µs, 1 Hz, plate electrodes, interelectrode distance 8 mm.ECT: Electrochemotherapy; EP: Electroporation.Based on combined data from Citation[67,81,82].](/cms/asset/a477a037-9ce9-4535-ad28-46f17a8ca91a/iery_a_11219500_f0005_b.jpg)
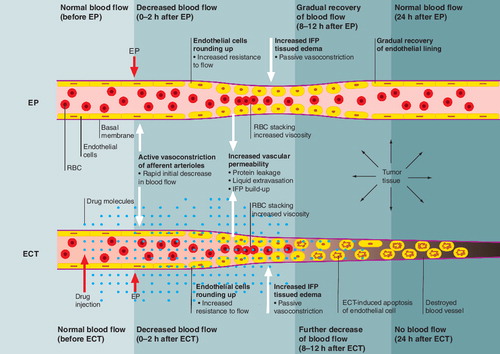
The effects of EP alone and of ECT are presented on the level of a microcirculatory blood vessel. Application of the drug and electric pulses are indicated by the block arrows. The general sequence of physiological changes and their consequences runs from the left to the right.
ECT: Electrochemotherapy; EP: Electroporation.
It can be observed that bleeding of this tumor was stopped immediately after the application of ECT. Gradually a crust was formed in place of the tumor (within 1 week), which fell off 3 weeks after the treatment. This particular tumor reduced in size dramatically and remained in partial response during the 21 weeks observation time.
ECT: Electrochemotherapy.
Reproduced with permission from Citation[100].
![Figure 7. The effect of electrochemotherapy (ECT) with bleomycin on bleeding melanoma metastasis.It can be observed that bleeding of this tumor was stopped immediately after the application of ECT. Gradually a crust was formed in place of the tumor (within 1 week), which fell off 3 weeks after the treatment. This particular tumor reduced in size dramatically and remained in partial response during the 21 weeks observation time.ECT: Electrochemotherapy.Reproduced with permission from Citation[100].](/cms/asset/483086f8-713a-4b89-a147-65b706af4058/iery_a_11219500_f0007_b.jpg)
Electroporation & electrochemotherapy
Cell membrane permeability can be increased nondestructively and transiently by exposing cells to a series of electric pulses of appropriately high voltage and short duration. This technique and phenomenon is called reversible electroporation or electropermeabilization (EP) Citation[1]. EP is highly effective and has attracted considerable attention over the last decade, largely owing to applications in which the uptake of poorly permeant extracellular molecules, (e.g., hydrophilic molecules) by the cells is increased several fold by means of EP. Electrochemotherapy (ECT) is a term used to describe the use of EP after injection of a chemotherapeutic drug, such as bleomycin and cisplatin, to greatly enhance its antitumor effectiveness Citation[2].
Over the last decade, numerous studies have been reported that involved the treatment of experimental tumors Citation[3] and tumors in humans by means of ECT Citation[4–6]. The standard operating procedures for the use of ECT in clinical oncology were published Citation[7]. The number of hospitals and veterinary clinics using ECT with the chemotherapeutics bleomycin and cisplatin has been increasing steadily. Solid tumors of various etiologies are being treated successfully. In veterinary medicine several studies have already demonstrated the effectiveness, convenience and safety of ECT with either cisplatin or bleomycin for the treatment of spontaneous tumors, such as soft-tissue sarcomas in cats, mast cell tumors and perianal tumors in dogs and sarcoids in horses Citation[8–14]. In clinical settings ECT is currently used with palliative intent for the treatment of predominantly melanoma cutaneous metastases, as well as in head and neck tumors, basal cell carcinomas, and adenocarcinomas in humans Citation[15–24]. ECT has also been used in the treatment of primary basal cell carcinoma with very high success rate Citation[25,26]. The reports on the treatment of melanoma metastases are numerous, stating complete response rates (complete disappearance of tumors) on average 70–80%, and objective response rates (including complete and partial responses, where the tumor decreased in size by more than 50%) on average 80–100% Citation[23]. Based on these encouraging results, ECT has also been proposed as a treatment modality for skin melanoma metastases Citation[27].
Electroporation is a crucial component of another closely related procedure named electrogene therapy (EGT), which requires electric pulses with characteristics different from those used in ECT. In EGT the electric pulses are used to electropermeabilize the cell membranes (as in ECT) and also to facilitate the electrophoretic transfer of extracellular genetic material into the cells Citation[28–35]. The potential of EGT for local gene therapy without the use of viral vectors has been demonstrated in vivo and in a clinical study for tissues, including muscle, skin, liver and tumors Citation[31,34,36–40].
In contrast to reversible EP used in ECT and EGT, the so-called irreversible electroporation (not the subject of this paper) induces irrecoverable damage to the cell membrane which ultimately leads to cell death and can be used in various applications, including tumor ablation Citation[41–43].
ECT protocol
A typical protocol for ECT of solid tumors consists of an intratumoral injection of the chemotherapeutic drug (bleomycin or cisplatin) or systemic intravenous administration of bleomycin, followed by delivery of a sequence of (typically eight) square monopolar electric pulses to the tumor. presents the principle of ECT along with an example of its practical application in the case of an outpatient treatment of a subcutaneous tumor. Electric pulses can be delivered either noninvasively using a pair of parallel plate electrodes or invasively using several needle-shaped electrodes arranged in various configurations with predefined distances between the electrodes Citation[7,23–25,44]. Plate electrodes are used for the treatment of small and superficial metastases, whereas needle electrodes are used predominantly for deeper-seated nodules or exophytic nodules Citation[23,25,45]. The duration of individual pulses is usually 100 µs and the repetition frequency is set to 1 Hz, although high-frequency (kHz range) frequencies can also be used Citation[5,23,46,47]. When choosing the appropriate amplitude of pulses, both the geometrical distance between the electrodes and the configuration of the electrodes must be considered. In the case of needle electrodes there are usually more than two electrodes in the configuration and, therefore, all pairs of electrodes that will be used for pulse delivery must be taken into account. Even though most authors report the amplitude of pulses simply as the voltage divided by the interelectrode distance (e.g., 1300 V/cm), it is important to realize that this information, without the notion of the particular type and configuration of the electrodes, does not describe the treatment situation in sufficient detail, because it is the electric-field strength reached in various parts of the tissue that determines the success of EP. The inhomogeneous distribution of electric-field strength (also expressed in V/cm) in tissue is a complex function of electrode shape and configuration (among other things) and cannot be described just by dividing the voltage by the interelectrode distance. In principle, the voltage should be set so that the electric-field strength in all parts of the target tissue exceeds the threshold level for the so-called reversible electroporation Citation[1,37,48–53]. Owing to the absence of a skin barrier between the target tissue and the electrodes in the case of needle electrodes, lower voltages are used for invasive EP than for noninvasive EP using plate electrodes Citation[51].
Electric pulses are delivered at the time when the maximum extracellular concentration of the chemotherapeutic drug is expected, so timing of EP is critical for successful ECT. There is a relatively narrow time-window within which EP should be performed. Typically, the optimum effect is obtained 3 min and 8–28 min after systemic intravenous injection in mice and humans, respectively or immediately after intratumoral injection Citation[7,54–57]. The drugs are used at doses much lower than cumulative doses usually used for systemic chemotherapy, and therefore have no systemic side effects. At such low cumulative doses, the therapeutic effect of the drug alone is insignificant. The exact protocols for EP and ECT in various studies are optimized for particular applications (animal species, electrode type, tumor site and size, chemotherapeutic used, aim of the study) and can thus vary from the one outlined here but can be found in the cited references.
Mechanisms of antitumor effectiveness of ECT
The main mechanism responsible for antitumor effectiveness of in vivo ECT is the increased cytotoxicity of the chemotherapeutic drugs bleomycin and cisplatin as a direct consequence of successful reversible electroporation of tumor cells, which increases the intracellular drug concentration. This is a well-known fact supported directly by in vitro studies demonstrating that exposure of tumor cells to EP increases the cytotoxicity of bleomycin several hundred-fold and that of cisplatin tenfold Citation[1,54,58,59], and the fact that both hydrophilic drugs gain increased access to the cytosol by means of EP Citation[54,60], but also indirectly by a clearly increased accumulation of both drugs in tumors treated in vivo with electric pulses (leading to prolonged exposure of tumor cells to high extracellular concentration of the drug) Citation[61,62]. However, the apparent discrepancy between the increased cytotoxicity of cisplatin by EP in vitro (tenfold) and in vivo (20-fold) in the same tumor cell line Citation[62] and some other observations lead to a conclusion that additional mechanisms are involved in antitumor effectiveness of ECT in vivo. The following mechanisms have been proposed: the role of the immune system Citation[63–65], vascular-disrupting effects owing to ECT of endothelial cells Citation[59,66], and tumor blood flow-modifying effects of ECT Citation[66,67].
In studies on immunocompetent and immunodeficient nude mice it was demonstrated that the host immune response is crucial for effective ECT with bleomycin Citation[2] and cisplatin Citation[65]. The growth delay induced by ECT in tumors was greater in immunocompetent than in immunodeficient mice. However, the most important observation was that a tumor can be completely eradicated by ECT exclusively in animals with a normal immune response. The importance of the immune system was also demonstrated by other studies in which a combined use of ECT with various types of immunotherapy resulted in potentiation of ECT effectiveness Citation[63,64,68,69].
The application of ECT or even of EP alone in absence of the drug has been known to induce a decrease in local blood flow. This side-effect was observed on tissue exposed to electric pulses in the early studies involving EP and ECT Citation[70–74], but its significance for antitumor effectiveness of ECT was at that time not fully recognized owing to the fact that in contrast to ECT, the antitumor effect of EP alone without the chemotherapeutic drug was not significant even though the time course and extent of blood flow changes observed immediately after the two treatments (i.e., ECT or application of EP alone) appeared very similar. The differences between the effects of EP and ECT on blood flow become evident only several hours after the treatment, which suggests that EP and ECT share a common blood flow-modifying mechanism (as a result of electric pulses alone) with an important additional vascular-disrupting mechanism present only in the case of ECT. We deal with these two mechanisms separately in the following sections. The new evidence accumulated in later studies provided more insight into this area and it became clear that these observed effects of EP and ECT in particular contribute significantly to the antitumor effectiveness of ECT and that they may even be critical for the final outcome of the treatment.
In the following sections, we first outline general characteristics of tumor vasculature and blood flow. This is followed by the evidence of transient and reversible blood flow-modifying effects common to EP and ECT and of permanent and irreversible vascular-disrupting effect exclusive to ECT. Based on this evidence, we suggest a model of physiological events taking place in a tumor within seconds, minutes, hours and days following the application of EP and ECT. Finally, the clinical relevance of the vascular-disrupting effect of ECT is supported by the review of clinical cases, where ECT was successfully used for the treatment of bleeding melanoma metastases.
General characteristics of blood flow in solid tumors
In general, the physiology of blood flow in solid tumors is different from that of normal tissues from which these tumors arise even though there are also large differences between various tumor types. In spite of large heterogeneity among tumors, several common characteristics of tumor vasculature and blood flow can be outlined Citation[75–78].
Solid tumors are usually poorly perfused and oxygenated in comparison with normal tissues in which they reside. Tumor neovasculature is inadequately developed, its characteristics include irregular and chaotic microvascular networks and branching patterns, irregular shape and length of microvessels, shunts and dead ends, all contributing to increased resistance to blood flow. All this leads to stagnant blood pools inside the tumor and to inefficient and ‘sluggish’ blood flow. Poor perfusion in combination with frequently abnormally large intercapillary distances, contribute to the development of hypoxic regions in the tumor and to acidic tissue environment. In contrast to normal tissues, which are uniformly vascularized and oxygenated across their entire cross-section, many solid tumors exhibit a structure in which the outer rim (the viable advancing part of the tumor) is better vascularized and oxygenated than the center Citation[76,77]. In addition to this cross-sectional variation, local variability in both the density of capillaries and oxygenation levels within the same tumor is also commonly encountered Citation[79].
Tumor blood vessel walls are structurally and functionally abnormal. They are commonly characterized by paucity of smooth-muscle cells and poor sympathetic innervation. As a consequence, local regulation of microcirculatory blood flow in tumors is inferior to that of normal tissue. Tumor capillaries can be described as ‘leaky’ because the permeability of capillary walls for large molecules, such as plasma proteins, is increased owing to an abnormal basal membrane as well as endothelial lining, which exhibits loose intercellular connections or even openings between endothelial cells. The increased extravasation of liquids coupled with an inadequate lymphatic drainage system, contribute to an elevated interstitial fluid pressure (IFP) in tumors Citation[77], which increases with the increasing distance from the outer tumor rim.
These characteristics of tumor blood flow can represent obstacles for antitumor treatments. For example, the hypoxic environment makes tumors resistant to radiotherapy. Effective delivery of chemotherapeutic drug into tumor cells is impeded by the insufficient net blood flow and the elevated IFP, which hinder interstitial transport of drug molecules. However, the abnormal and inadequate tumor vasculature and blood flow also makes tumors vulnerable to further reduction in blood flow and can be exploited in treatment strategies. Tumors are a particularly attractive target for vascular-disrupting therapies and other new treatments specifically designed to take advantage of tumor vasculature’s weaknesses Citation[77,80].
Effects of EP & ECT on tumor blood flow
In this section, we provide an overview of the known effects of EP and ECT on blood flow and oxygenation in experimental subcutaneous tumors in mice. The explanation of the observed effects along with further supporting experimental evidence is also presented. provides a list and brief description of methods for measurement of blood flow and oxygenation-related parameters referred to in this text.
All effects of EP alone or ECT on tumor blood flow described here were confined only to the tissue subjected to electric pulses. As such, these effects can be regarded as local phenomena with no systemic effects ever reported in any of the studies.
summarizes the main characteristics of blood flow changes observed in experimental subcutaneous Sa-1 fibrosarcoma tumors in immunocompetent A/J mice, a tumor model most extensively used in studies on effects of EP and ECT on tumor blood flow, over a period of 2 days following the application of EP and ECT with bleomycin (at a dose 1 mg/kg) in comparison with blood flow in control tumors and tumors treated with bleomycin alone.
Blood flow-modifying effects of EP
It was demonstrated by a number of authors using several different methods in solid tumor models as well as in normal tissue that the application of electric pulses commonly used in ECT protocols induces rapid and profound reduction in local blood flow of exposed tissue Citation[66,67,70,71,73,81]. The dynamic changes, as rapid as those following the application of EP, can be measured by the laser Doppler flowmetry method (LDF). This is presented in for Sa-1 tumors in A/J mice, where it can be observed that the blood flow reduction started as soon as the first pulse in the series was delivered. The minimum close-to-zero blood flow level was reached within seconds. A partial recovery of microcirculation started approximately 1–2 min after EP , blood flow increased to approximately 40% of the pretreatment perfusion value within 10–15 min as shown in . At that point the reperfusion process appeared to be stalled with no significant further improvement for at least 2 h. Experimental evidence suggests that some minor secondary reduction in blood flow occurred within the first hour after the initial reperfusion . However, on a larger time scale, blood flow actually continued to improve, albeit at a much slower pace and was almost completely restored 24 h after the application of EP. Blood flow in treated tumors was indistinguishable from that in the control tumors 48 h after the treatment was administered Citation[66,67,81]. This can be observed in .
There was a good agreement between the results obtained by using different methods in several studies (LDF, patent blue-violet [PBV] staining, rubidium extraction, contrast-enhanced [CE]-MRI, power Doppler US imaging) on the same tumor model. According to the studies using rubidium extraction or PBV-staining techniques, a reduction of 70% was observed in blood flow of Sa-1 tumors in A/J mice 30 min after EP Citation[72,81]. A similar effect was observed in one of the first studies on the effects of EP on tumor blood flow using CE MRI with contrast agent albumin-(Gd-DTPA)30, in which it was demonstrated that, 30 min after EP, blood flow was severely impeded in comparison with nontreated tumors on the contralateral side in the same animals Citation[70]. In all studies, the blood flow in tumors 1 h after EP was on average less than 50% of the pretreatment value or when compared with the control tumors Citation[66,67,72,82]. The rapid initial decrease in blood flow and its duration observed in subcutaneous murine tumors was consistent with observations in normal tissues such as liver, spleen and pancreas as well as internal liver tumors in rabbits where the effect lasted for 10–15 min after EP before gradual reperfusion Citation[71]. The results of CE-MRI, PBV staining and power Doppler ultrasonographic imaging also provided clear evidence of heterogeneous distribution of blood flow in tumors with the periphery being considerably better perfused than the center Citation[66,81,83].
Reapplying the same EP treatment 24 h after the first treatment induced a blood flow decrease very similar to that after the first application, but the recovery 24 h after the second treatment was somewhat less complete than after the first treatment Citation[72]. The impact of the duration, amplitude, and number of EP pulses on tumor blood flow has also been studied. The level of blood flow reduction observed 30 min after EP in subcutaneous murine tumors was positively correlated with the number of pulses between 1 and 10 at amplitude and duration of pulses 1040 V (8 mm interelectrode distance) and 100 µs, respectively Citation[67,72]. However, it should be noted that even a single EP pulse was enough to provoke the same rapid and extreme initial decrease in blood flow as a regular sequence of eight pulses, but the total effect was much shorter-lived in comparison with eight pulses, disappearing completely over a period of just a few minutes after EP Citation[84]. The reduction in tumor blood flow appeared to be a threshold phenomenon as far as the amplitude of pulses was concerned. With the number and duration of pulses fixed at eight and 100 µs respectively, it was found that 30 min after EP the decreased blood flow could be detected only for amplitudes at and above 640 V at 8 mm interelectrode distance (value consistent with the threshold for the onset of reversible EP in tumors Citation[85]). The level of decrease 30 min after treatment appeared positively dose dependent up to 1040 V with no further decrease at 1200 V.
Based on the details outlined so far, it is safe to conclude that the decrease in tumor blood flow after EP typically used in ECT consists of two distinct phases, most likely connected to two distinct physiological mechanisms. The first phase is rapid (within seconds), profound (blood flow shutdown) and short-lived (lasting only a few minutes). The second phase is slower to develop fully (minutes to tens of minutes) and relatively long-lived (lasting for at least 24 h, see ). The actual duration and extent of the second phase are positively correlated with the number, amplitude and duration of electric pulses.
Results strikingly similar to those in tumors were observed in a study on characterization of blood flow effects of EP on thigh muscles in mice Citation[73], even though the characteristics of tumor and normal tissue vasculatures are known to differ in many significant aspects. In the study by Gehl et al. these effects were measured qualitatively by means of the PBV-staining technique in relation to membrane EP and resealing dynamics. For the amplitude and duration of EP pulses above the threshold for reversible EP, the vascular response of muscles to EP was also described as a two-phase phenomenon. The first rapid, profound and short-lived phase (lasting 1–3 min) was attributed to sympathetically-mediated reflex vasoconstriction of afferent arterioles as a reaction to electroporation of muscle and/or vascular endothelial cells. The direct effect of pulses on smooth vascular musculature was, however, not significantly involved in this response Citation[73]. The kinetics of this phase observed in tumors and muscles were identical and the direct vasoconstrictive effect on tumor-supplying arterioles has also been reported as the main mechanism of action of some chemical vascular-disrupting agents (VDAs) Citation[77]. Therefore, the sympathetically mediated constriction of smooth vascular musculature is most probably the main mechanism of this first rapid phase of blood flow reduction in tumors treated with EP.
As in tumors, the second phase of vascular response to EP in muscles was slower to develop and of much longer duration than the first phase Citation[73]. It lasted up to 30 min, which, however, was considerably less than observed in studies involving tumors. The dependence of this phase on the amplitude and duration of EP pulses was progressively more significant for combinations leading to irreversible EP or very slow membrane resealing kinetics of muscle and vascular endothelial cells. It was speculated that the resolution of this long-lived phase followed the kinetics of observed membrane resealing after EP Citation[73].
A more definitive explanation for the second phase of the vascular response observed in tumors and muscles can be derived from an in vitro study on the effects of EP on the cytoskeleton of cultured primary endothelial cells and on the permeability of the endothelial monolayer Citation[86]. Namely, the cell cytoskeleton is composed of three major types of structures (microtubules, actin microfilaments and intermediate filaments) and is essential for maintaining cell shape and function. The contractility and the integrity of intercellular junctions between vascular endothelial cells is responsible for the regulation of vascular permeability. In the study by Kanthou et al., human umbilical vein endothelial cells (HUVECs) were exposed to EP in situ. Immunofluorescence staining for F-actin, β-tubulin, vimentin and vascular endothelial cadherin (VE-cadherin) and western blotting for levels of phosphorylated myosin light chain and cytoskeletal proteins, were performed. Endothelial monolayer permeability was determined by monitoring the passage of fluorescein isothiocyanate (FITC)-coupled dextran through the endothelial monolayer. Exposure of endothelial cells to electric pulses led to disruption of the microfilament and microtubule cytoskeletal networks, loss of contractility and loss of VE-cadherin from cell-to-cell junctions. These cytoskeletal effects of EP were paralleled by a rapid rise in endothelial monolayer permeability. Changes were reversible and all cytoskeletal structures recovered within 1–2 h after EP, without a loss of endothelial cell viability Citation[86]. As an example, the effect of EP at 40 V is presented in , demonstrating rapid dissolution of actin filaments and a fragmentation of microtubules (within 5 min after EP) with recovery 1 h post-EP.
The reported disruption of the endothelial cytoskeleton and intercellular junctions leading to swelling and rounding of endothelial cells and to a compromised barrier function of the endothelial lining have important implications for blood flow in vivo. Change in the shape of endothelial cells increases vascular resistance for blood flow. The increased permeability of vascular walls to macromolecules is followed by protein leakage and leads to a decrease in oncotic pressure between the intra- and extra-vascular compartments and to extravasation of liquids. The results are development of interstitial edema, increased IFP, and decreased intravascular pressure, which all contribute to compromised blood flow in a way similar to that seen after the application of chemical VDAs Citation[77]. It should be noted that swelling of cells after EP with similar dynamics as seen for endothelial cells was also observed in some other types of cells in vitroCitation[87].
The effect on endothelial cells in vitro was reported to be rapid since it developed within 5 min Citation[86], but not fast enough to be involved in the first phase of blood flow decrease observed in vivo. In it can be seen that the recovery of blood flow in tumors was arrested 10–15 min after EP. This indicates a fully developed second phase of blood flow reduction. The resolution of this second phase was gradual and slow meaning that blood flow remained decreased up to 24 h after the treatment in tumors Citation[67,72,81] but for a significantly shorter period in muscles Citation[73]. In the study of Kanthou et al., it was shown that when the voltage was high enough to induce a significant drop in endothelial cell viability, the restoration of the perturbed cytoskeleton was severely impeded. In in vivo conditions, such an effect would lead to a prolonged recovery period for the affected vasculature. Owing to inherent differences between normal and tumor vasculature, it can be expected that the cytoskeletal networks and intercellular junctions in tumor vasculature would be affected more profoundly by EP and would take longer to recover their functions than in normal vasculature. This may explain the observed differences in the duration of the second phase of blood flow reduction between tumors and muscles. We suggest that the kinetics of re-establishment of the endothelial cytoskeleton and especially the barrier function of the endothelial lining may be the most important determinants of duration of the second phase of blood flow decrease after EP.
The two-phase perfusion changes observed in solid tumors after EP can be modeled as suggested schematically in . Both phases are represented by simple bi-exponential functions with different time constants. The experimental data for blood flow after EP from are superimposed on the model. Obviously, a more elaborate mathematical representation of the two phases in the model should be used to fully describe the actual blood flow data, but the general adequacy of a two-phase model to describe the experimental data is clear.
Blood flow reduction after EP is, therefore, a reversible process. The relatively short period of blood flow reduction (24 h) contributes to tumor growth delay, which is usually detected after treatment with EP alone, but which is insignificant in terms of antitumor treatment. See also for a comparison of antitumor effectiveness of different treatments expressed as the induced tumor growth delay and the percentage of cured tumors.
Vascular-disrupting effects of ECT
From it follows that within the first hour after treatment, the effects of ECT with bleomycin on tumor blood flow could not be distinguished from the effects of EP alone in the absence of the drug. Both the extent and time course of changes were virtually the same, which was demonstrated in several studies using either bleomycin at different doses or cisplatin as the chemotherapeutic drug Citation[66,67,81]. The differences, however, became evident 4–8 h after treatment as can be seen in . By that time, perfusion of EP-treated tumors had partially recovered. On the other hand, blood flow in tumors treated with ECT demonstrated no further improvement (dose 1 mg/kg). With a higher dose of bleomycin (5 mg/kg), further deterioration was observed so that 12 h after ECT a practically complete arrest in blood flow was achieved, as demonstrated by PBV and rubidium extraction data and further supported by power Doppler US imaging. No recovery in blood flow was seen 5 days after the treatment at this dose of bleomycin Citation[67]. The time course of blood flow changes after ECT with cisplatin at a dose of 4 mg/kg was similar to that in the case of ECT with bleomycin but the reduction in blood flow observed over the course of 5 days was less extreme than with bleomycin at either dose Citation[81]. By contrast, treatment of tumors with either bleomycin or cisplatin alone at the same doses as used in ECT with these two drugs (but in the absence of EP) produced only minor and transient changes in blood flow and the blood flow status of these tumors was the same as that in control tumors over a period of 5 days after the treatment. compares the response of subcutaneous Sa-1 tumors to treatment with EP, bleomycin (5 mg/kg), cisplatin (4 mg/kg), and ECT with both chemotherapeutic drugs over the course of 1 week after the treatment. The antitumor effectiveness of these treatments in addition to ECT with bleomycin at the lower dose of 1 mg/kg in terms of induced tumor growth delay and number of cured tumors is summarized in .
In contrast to EP, which induces profound but essentially transient and reversible decline in blood flow of tumors, ECT induces long-lived blood flow reduction. The situation can further deteriorate in the days following therapy (depending on the drug dosage) even to the point of complete arrest of tumor blood flow, as demonstrated for ECT with bleomycin at the higher of the two doses used in the reported experimental studies.
The process of EP is not selective in the sense that all cells exposed to electric field densities above a certain threshold level (including the endothelial cells lining the tumor vessels) are electropermeabilized Citation[82]. The vascular endothelial cells may be even more susceptible to the effects of EP than the primary target of ECT – the tumor cells. Both the theoretical considerations and experimental results in vitro support this hypothesis.
When electrical properties of different tissue constituents and realistic microcirculatory blood vessel dimensions are taken into account, the electric-field strength at the boundary between the blood and blood vessel wall (the very location of endothelial cells) was estimated to be up to 40% higher than in the surrounding tissue because of higher conductivity of blood in comparison with the tissue constituents Citation[66]. The shape and relative orientation of endothelial cells in an electric field may also render them more susceptible to the effects of EP owing to a larger induced transmembrane voltage Citation[88]. Furthermore, endothelial cells, being in direct contact with the blood compartment, are exposed to the highest concentration of the chemotherapeutic drug reached in blood vessels after intravenous injection. From this reasoning it follows that endothelial cells can be expected to be affected by ECT to an even higher degree than tumor cells. The killing of endothelial cells by ECT leads to obstruction of tumor blood flow and consequently, to ischemic death of all cells supplied by the affected vessels.
In vitro studies on human dermal microvascular endothelial cells HMEC-1 have demonstrated that these cells are highly sensitive to ECT. Application of EP increased the cytotoxicity of cisplatin tenfold and that of bleomycin even 5000-fold in these cells. Sensitivity of HMEC-1 cells to ECT with bleomycin was even greater than sensitivity of some tested tumor cell lines Citation[59], which means that the effect of ECT on endothelial cells should be more important in the treatment of tumors with bleomycin than with cisplatin. The differences in the response of HMEC-1 cells to ECT between the two drugs in vitro were in perfect agreement with the differences in blood flow reduction observed in tumors treated with ECT using the same two drugs.
The effects of EP and ECT on endothelial cells observed in vitro are also in agreement with histological observations from tumors treated by EP and ECT with bleomycin Citation[66]. It was reported that 1 h after EP alone or ECT, the endothelial cells appeared swollen and rounded with a narrowed lumen of blood vessels, an observation consistent with both the observed blood flow changes in vivo and the demonstrated effects of EP on the endothelial cytoskeleton and endothelial monolayer Citation[86]; 8 h after treatment, the apoptotic morphological changes in endothelial cells and extravasation of erythrocytes were observed only in tumors treated with ECT, a direct evidence of damaged blood vessels, which was, however, not detected in tumors treated with either EP or bleomycin alone.
Tumor oxygenation after EP & ECT
Tissue oxygenation is closely related to local-tissue blood flow. Tumors in general are characterized by lower pO2 values than normal tissues, which was also confirmed for the Sa-1 tumor model in A/J mice by electron paramagnetic resonance (EPR) oximetry, Citation[89], polarographic oximetry Citation[90] and luminescence-based fiber-optic oximetry Citation[91].
The time-course and extent of pO2 decrease after EP alone or after ECT with cisplatin (4 mg/kg) and bleomycin (1 mg/kg) was found to be similar to that of the blood flow. The maximum reduction in pO2 (70%) was observed 2 h after treatment and was followed by a slow recovery. The pretreatment pO2 values were reached 8 h after EP and 2 days after ECT Citation[66,81,89]. In the case of ECT, this was a surprising result since the blood flow in ECT-treated tumors showed no improvement for at least 5 days following the treatment (see also ). It is possible that the recovery of oxygenation was due to a decreased demand for oxygen in tumors as a result of ECT killing a major proportion of tumor cells. In such conditions, the damaged but not completely destroyed tumor vasculature may be sufficient for recovery of oxygenation of the remaining tumor to the pretreatment level. In the EPR studies on tumor oxygenation Citation[66,89], bleomycin at a dose of 1 mg/kg was used which was five-times less than in some previous studies Citation[67,82] in which an almost complete shut-down of tumor blood flow after ECT with bleomycin was maintained over a course of 7 days . It is reasonable to expect that, at a bleomycin dose of 5 mg/kg, oxygenation would not be recovered.
Further evidence of tumor hypoxia induced by EP and ECT was provided in studies involving the use of an exogenous hypoxia marker pimonidazole Citation[66] and an endogenous hypoxia marker glucose transporter 1 (Glut-1) Citation[92]. Histological preparations of control tumors and tumors treated with bleomycin alone contained only moderate pimonidazole-positive areas (~10%) while the tumors treated with EP alone or ECT developed larger hypoxic regions (up to 40%) immediately after the treatment, reaching the maximum extent of hypoxia in 2 h (the same time frame as observed with EPR oximetry) and recovering to pretreatment values within 24 h. The recovery was slower in tumors treated with ECT Citation[66]. The increase in hypoxic regions was not as extreme as the observed blood flow changes and again the recovery of pO2 was in contrast the lack of no recovery observed in tumor blood flow Citation[92]. In addition to the explanation suggested in the previous paragraph, it is also possible that the hypoxic regions may have been underestimated by pimonidazole staining owing to inadequate blood flow in some regions of tumors (large temporal and spatial heterogeneity in blood flow is typical for tumors). Pimonidazole also could not reach necrotic regions owing to lack of blood flow thus resulting in falsely nonstained regions and therefore, in the extent of hypoxia being underestimated.
The extensive decrease in oxygenation after ECT can be expected to induce further tumor cell death due to hypoxia. The progression of necrosis in tumors to 90% of the total tumor area correlated with the oxygenation changes and the overall tumor growth pattern Citation[81]. These effects were more pronounced with bleomycin than with cisplatin, which is consistent with higher in vitro sensitivity of endothelial cells to bleomycin Citation[59,67,82].
Model summary of effects of EP & ECT
Based on the evidence described in the previous sections, we can summarize the sequence of events that take place in tumor blood flow after application of EP and ECT in .
There are at least two distinct mechanisms by which the effects of EP and ECT on blood flow contribute to antitumor effectiveness of the treatment, a vascular lock and a vascular-disrupting effect.
The vascular-lock effect – induced transiently by EP alone and to an even larger extent by ECT – leads to an effective entrapment or at least impeded wash-out of the drug accumulated within a tumor due to reduced blood flow. Tumor cells are consequently exposed to a high drug concentration for an extended period of time. In addition, the vascular-lock effect induces severe tumor hypoxia, which could be exploited for treatments involving drugs that are activated in a hypoxic environment (e.g., bioreductive drugs) Citation[93].
The vascular-disrupting effect – the severely damaged tumor vasculature due to ECT of endothelial cells – leads to an additional cascade of tumor cell death as a result of long-term lack of oxygen and nutrients and accumulation of waste products in the tumor. This effect brings ECT into the realm of the so-called vascular-targeted therapies, which have already been exploited in several studies using different approaches to affect tumor vasculature Citation[77]. It is probably also very important for complete elimination of the tumor in the case of ECT because it helps to kill those tumor cells that were not destroyed directly by the drug, either because some tumor regions were not exposed to a high enough electric field for successful EP, or because the extracellular drug concentration was not sufficiently high in some areas.
Both the vascular lock and the vascular-disrupting effect of EP and ECT contribute to antitumor effectiveness. Through these effects we can explain the apparent discrepancy between the increased cytotoxicity of drugs in vitro and in vivo in the same tumor cell line Citation[62]. The role of blood flow-modifying (vascular lock) and vascular-disrupting effects of EP and ECT is estimated to be significant, and also contributes, in addition to the involvement of the immune response, to the often-observed complete and long-lasting responses of tumors treated by ECT at the preclinical and clinical level. Furthermore, these effects can be directly exploited in the treatment of bleeding metastases, for immediate cessation of bleeding and reduction in size of the treated tumors.
ECT of bleeding melanoma metastates
The treatment of recurrent cutaneous or subcutaneous tumors is a common clinical problem, due to unresectability and relative insensibility to conventional systemic therapies Citation[23]. Recurrent melanoma metastases pose a treatment problem for physicians, and are also a distress to patients, because of the psychological burden, inflicted pain, ulceration and often, bleeding Citation[22,23,94].
Unresectable and in-transit melanoma can be treated either systemically or locoregionally. Different approaches include systemic or regional chemotherapy either by hyperthermic limb perfusion or isolated limb infusion, radiotherapy, carbon dioxide laser ablation, cryosurgery, intralesional chemotherapy with Bacillus Calmette–Guerin, local gene therapy with TNF-erade or IL-12 and human recombinant IL-2 or IFN-α, as well as cell vaccines using melanoma cell lysates. All these treatment approaches have individual limitations and variable response rates Citation[23].
Electrochemotherapy is yet another treatment option that has been recommended for unresectable and in-transit melanoma Citation[23,27]. The results of the multicenter ‘European Standard Operating Procedures of ECT’ (ESOPE) study demonstrated a clinical response of 81% objective responses for melanoma with 66% complete responses, that are comparable to previously published results Citation[4,23]. Subsequent studies of ECT in the treatment of melanoma continue to demonstrate the efficacy of treatment with response rates ranging from 46 to 100% Citation[6,95,96]. The treatment has become widely accepted. Currently, over 50 institutions in Europe and the USA offer ECT to patients as palliative treatment of a diversity of recurrent and metastatic tumors, including melanoma, basal and squamous cell carcinoma, breast cancer, sarcomas and other metastatic lesions.
As hemorrhaging cutaneous metastases are quite a common clinical problem, several reports on successful treatment with ECT have already been described. Kubota et al. revealed its palliative effect in the management of skin metastases from bladder cancer Citation[97], while Gehl et al. described two cases of successful management of bleeding melanoma skin metastases. The first case established the effectiveness of ECT in the treatment of nine bleeding, ulcerated nodules on the chest wall, with immediate cessation of bleeding after administration of electric pulses and 100% complete regression of nodules Citation[98]. The second case demonstrated a palliative effect of ECT in dealing with eight metastases on the head and scalp, with cessation of bleeding and complete remission of all but one of the metastases (87%) Citation[99]. Furthermore, Snoj et al. reported on effective treatment of melanoma bleeding metastasis, 3.5 cm in diameter, by ECT Citation[100]. In this case, all standard treatment modalities were reported to be employed, but none of them provided a long-term result. Thus, amputation of the lower limb was considered. A single session of ECT with bleomycin, however, provided an immediate clinical benefit; the bleeding stopped and did not recur, as can be seen in . In addition, a crust developed and a reduction in size was noticed. It was concluded that ECT should be considered both as an effective treatment in palliation of bleeding melanoma skin metastases and as an effective modality for limb-sparing treatment of refractory bleeding melanoma nodules Citation[100].
Therefore, ECT represents a novel approach in the palliation of bleeding metastases. At present, several treatments can be used for the treatment of bleeding metastases. These include surgery, which can be suitable for the management of small bleeding lesions, but with larger or multiple lesions only amputation is possible Citation[101]. Some clinical benefit in the treatment of bleeding metastases was reported by isolated limb perfusion with TNF-α and melphalan Citation[102–104]. Intra-arterial embolization could also be a treatment of choice in the management of bleeding melanoma Citation[105]. However, no studies have been performed so far to establish the palliative effect of radiotherapy on bleeding melanoma nodules.
A comparison of the discussed treatment modalities for bleeding metastases to ECT points to its many advantages. Regarding the patients’ poor physical condition, ECT offers an excellent alternative owing to its once-only treatment strategy, high probability of immediate relief, its outpatient basis and modest patient discomfort. Currently, the main use of ECT remains restricted to palliative treatment of cutaneous and subcutaneous tumor nodules refractory to conventional treatment. However, owing to its vascular-disrupting effect, ECT could be considered as a treatment modality in patients with refractory bleeding melanoma nodules.
Expert commentary
Application of EP pulses to tumors induces transient structural changes in the membranes of tumor cells (cell-membrane permeabilization), which allows otherwise poorly permeant extracellular molecules (e.g., chemotherapeutic drugs) to enter the cells in vastly increased quantities. This is the primary mechanism of antitumor action of ECT. By this mechanism, the chemotherapeutic drugs, such as bleomycin and cisplatin, can become highly effective at very low cumulative doses (so low that no therapeutic effect would be achieved if the drug alone was applied). An additional benefit of ECT is that its effects are localized to the target area (only electropermeabilized cells are affected) and there are, therefore, no systemic side effects owing to the very low cumulative dose of the drug used.
However, application of EP pulses to tumors also induces two distinct vascular effects, which manifest themselves in a two-phase blood flow decrease: a rapid, powerful, yet short-lived reflexory vasoconstriction of afferent arterioles leading into the tumor, which is mediated by the SNS as a result of EP of endothelial and possibly other cells in the tumor; a slower and much longer-lived phase, mainly as a result of disrupted endothelial cytoskeletal structures and increased endothelial monolayer permeability, which result in leakage of fluids and molecules from blood vessels and from permeabilized cells into the extracellular space, leading to increased IFP and decreased intravascular pressure. It is suggested that the resolution of this later phase depends predominantly on the dynamics of recovery of the endothelial lining’s physiological function.
The local vascular-disrupting effect of ECT brought about by destruction of tumor vessels’ endothelial lining is a very important additional mechanism, which contributes to antitumor efficiency of ECT. The killing of endothelial cells by ECT leads to permanent obstruction of tumor blood flow and consequently to ischemic death of all remaining cells supplied by the affected vessels.
There are two major practical reasons for interest in the blood flow-modifying effects of EP and ECT. The first reason is that understanding various physiological aspects and consequences of EP and ECT will enable further optimization and fine-tuning of the existing treatment modalities. The local nature of the effects of EP and ECT coupled with the understanding of their role in the overall antitumor effectiveness of ECT, can lead to more individualized protocol treatments for ECT and hence to even more successful tumor treatment. The second reason is that the ability to modify local blood flow in tissue exposed to EP and ECT without significant systemic effects can also be exploited for other therapies.
The vascular-disrupting effect of ECT is already being beneficially employed in the treatment of bleeding melanoma metastases and other types of bleeding tumors. Immediately after ECT, the bleeding stops and does not recur. Furthermore, the vascular-disrupting effect of ECT is of utmost importance for translation of ECT to treatment of deep-seated tumors, also in well vascularized organs, such as the liver, where this effect helps to minimize bleeding of the treated area.
Five-year view
Treatments based on EP are currently used in medicine for ECT and EGT. However, there are several other emerging treatments that use electric fields for membrane permeabilization, such as irreversible electroporation for ablation of normal and neoplastic tissue Citation[106,107] and use of extremely short electric pulses (the so-called nanopulses) for the treatment of cancer Citation[108]. Since all these treatments use electric pulses, it has to be taken into account that sets of pulses with parameters different from the ones considered in this paper may also induce vascular changes in normal tissues and tumors, but to a different extent. How the vascular changes affect the outcome of these new treatments has yet to be explored, and treatment approaches must be optimized so that treatment effectiveness is not hampered by reduced blood flow and the resulting hypoxia in tissues.
The suggested mechanisms of blood flow-modifying and vascular-disrupting effects of EP and ECT are currently based partly on in vitro studies. However, developments of noninvasive in vivo imaging and intravital microscopy open new possibilities, so that vascular effects of EP and ECT can be further studied in intact normal and tumor blood vessels to confirm our explanation.
The induced blood flow changes after EP may be of special concern for EGT. Similar changes in tumor perfusion were noticed in tumors exposed to different sets of pulses used for gene electrotransfer; either eight EP pulses at 640 V amplitude (interelectrode distance 8 mm) Citation[109] or the combination of high- and low-voltage pulses Citation[109,110]. The observed vascular changes may affect the transfection efficiency of the plasmids and also their expression. In addition, an antiangiogenic therapeutic gene AMEP delivered by EP for treatment of cutaneous melanoma metastases is currently in a clinical trial Citation[111].
Electrochemotherapy has also been used in combination with radiation therapy. As known, hypoxic cells are radioresistant and special attention has to be taken into account when scheduling the combined treatment. Our recent studies have shown that both drugs used in ECT, bleomycin and cisplatin, are also radiosensitizing drugs, and are significantly more radiosensitizing when used in ECT Citation[112,113]. The effects of radiosensitization were also demonstrated in a fractionated radiation regimen without major potentiating effect on radiation-induced skin damage Citation[114].
Since EP induces transient hypoxia in tumors, this can be an advantage in combination with bioreductive drugs that exert their cytotoxic effect specifically in hypoxic tissues. As already indicated in a preliminary study, the antitumor effectiveness of tirapazamine was potentiated by exposure of tumors to electric pulses Citation[93]. However there are other bioreductive drugs that could be used in combination with EP.
Drugs other than bleomycin and cisplatin were tested in combination with electroporation Citation[115]. Until recently, however, only these two had been demonstrated to have significantly increased cytotoxicity in vitro and in vivo. New antitumor drugs containing metals have been developed with the aim of obtaining a broader spectrum of activity and reduced side effects Citation[116]. Of these new drugs, ruthenium compounds gained a particular interest for their potential application on tumors which developed resistance to cisplatin or in which cisplatin is inactive. Moreover, some ruthenium complexes show strong activity against metastases of solid metastasing tumors Citation[117]. Although NAMI-A has a very limited direct cytotoxic effect on tumor cells, when combined with EP, its cytotoxicity was potentiated significantly. Citation[118]. Local potentiation of chemotherapeutic drugs being effective systemically by means of EP can thus be a promising approach Citation[119].
The effects of EP and ECT have the potential to be exploited in the so-called vascular-targeted treatments. This class of antitumor treatments aims to destroy the malignant cells indirectly by preventing effective blood supply to the tumor. This can be done on two levels, by destroying the existing tumor vessels (vascular-disrupting effect) and by preventing formation of new ones (anti-angiogenic effect) Citation[77,79]. EP can be combined with other VDAs that target tumor endothelial cells. Some of them, combretastatins and 5,6-dimethylxanthenone-4-acetic acid (DMXAA) are already in clinical trials and EP could potentiate their effectiveness by increasing their intracellular concentration Citation[77,80].
Electrochemotherapy is currently used for the treatment of cutaneous and subcutaneous tumors Citation[5]. However, a new generation of electric pulse generators has been developed that can produce electric fields for the treatment of larger treatment areas Citation[23,120,121]. With the use of long needle electrodes, deep-seated tumors, such as melanoma, sarcoma or bone metastases, can be treated intraoperatively in the liver or percutaneously in the limbs Citation[121]. In such situations, the electrodes are 1.2 mm in diameter, having a 3- or 4-mm long uninsulated part. In such cases, the retraction of the electrodes from the treated tissue after the procedure could result in bleeding. However, bleeding is largely reduced thanks to the described vascular lock and vascular-disrupting effects of EP and ECT.
Table 1. Short description of the experimental methods for assessment of blood flow and related parameters in tumors referred to in the text.
Table 2. Antitumor effectiveness of electroporation and electrochemotherapy with bleomycin (at doses of 1 and 5 mg/kg) and cisplatin (at a dose of 4 mg/kg) on Sa-1 tumors in A/J mice.
Key issues
• Electroporation (EP) is the process of induction of transient increase in cell membrane permeability by exposing cells to a series of very short but high-voltage electric pulses. It is sometimes also referred to as electropermeabilization.
• Electrochemotherapy (ECT) is an antitumor therapy in which intravenous or intratumoral administration of a poorly permeant chemotherapeutic drug (currently bleomycin or cisplatin) is followed by local application of EP. EP facilitates the uptake of the drug by the affected cells and, thus, potentiates locally the cytotoxicity of the drug by several orders of magnitude.
• Electrochemotherapy is an effective treatment for cutaneous and subcutaneous tumors of various tumor types. For melanoma, ECT is being accepted as a treatment modality for unresectable or in-transit metastases with response rates reaching up to 100%.
• Application of EP induces a rapid, profound but transient two-phase decrease in local blood flow. The first phase is instantaneous, extreme (almost complete shut-down of blood flow), but short-lived (several minutes) and is a result of vasoconstriction of afferent arterioles. The second component is slower, less extreme, but longer-lived (24 h) and is a result of transient disruption of cytoskeletal structures and compromised barrier function of the microvascular endothelium.
• In addition to the effects seen after EP, ECT induces profound long-term (from several days to permanent) decrease in local blood flow as a result of largely irrecoverable damaged tumor vasculature due to exposure of endothelial cells to ECT.
• The effects of EP and ECT on tumor blood flow contribute to the overall antitumor effect in two ways: by the vascular-lock effect (causing a prolonged exposure of tumor cells to the drug owing to drug entrapment); and by the vascular-disrupting effect (causing a secondary cascade of tumor cell death as a result of long-term lack of oxygen and nutrients and accumulation of waste products in the tumor).
• The effects of EP and ECT on tumor blood flow and oxygenation can be further exploited in new vascular-targeted therapies and in therapies involving drugs that are activated in a hypoxic environment, such as bioreductive drugs.
• The blood flow-modifying (vascular lock) and vascular-disrupting effect of ECT are already being beneficially employed in treatment of bleeding melanoma metastases and other types of bleeding tumors. Immediately after ECT, the bleeding stops and does not recur.
• The vascular lock and vascular-disrupting effects of ECT is of utmost importance for translation of ECT to treatment of deep-seated tumors, especially in well-vascularized organs, such as the liver, because it can prevent bleeding of the treated area.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- Orlowski S, Belehradek J, Paoletti C, Mir LM. Transient electropermeabilization of cells in culture – increase of the cyto-toxicity of anticancer drugs. Biochem. Pharmacol.37(24), 4727–4733 (1988).
- Mir LM, Orlowski S, Belehradek J, Paoletti C. Electrochemotherapy potentiation of antitumor effect of bleomycin by local electric pulses. Eur. J. Cancer27(1), 68–72 (1991).
- Sersa G, Cemazar M, Miklavcic D, Rudolf Z. Electrochemotherapy of tumours. Radiol. Oncol.40(3), 163–174 (2006).
- Sersa G. The state-of-the-art of electrochemotherapy before the ESOPE study; advantages and clinical uses. EJC Suppl.4(11), 52–59 (2006).
- Marty M, Sersa G, Garbay JR et al. Electrochemotherapy – an easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. EJC Suppl.4(11), 3–13 (2006).
- Quaglino P, Mortera C, Osella-Abate S et al. Electrochemotherapy with intravenous bleomycin in the local treatment of skin melanoma metastases. Ann. Surg. Oncol.15(8), 2215–2222 (2008).
- Mir LM, Gehl J, Sersa G et al. Standard operating procedures of the electrochemotherapy: instructions for the use of bleomycin or cisplatin administered either systemically or locally and electric pulses delivered by the Cliniporator™ by means of invasive or non-invasive electrodes. EJC Suppl.4(11), 14–25 (2006).
- Mir LM, Devauchelle P, Quintin-Colonna F et al. First clinical trial of cat soft-tissue sarcomas treatment by electrochemotherapy. Br. J. Cancer76(12), 1617–1622 (1997).
- Rols MP, Tamzali Y, Teissie J. Electrochemotherapy of horses. A preliminary clinical report. Bioelectrochemistry55(1–2), 101–105 (2002).
- Tozon N, Kodre V, Sersa G, Cemazar M. Effective treatment of perianal tumors in dogs with electrochemotherapy. Anticancer Res.25(2A), 839–845 (2005).
- Spugnini EP, Vincenzi B, Baldi F, Citro G, Baldi A. Adjuvant electrochemotherapy for the treatment of incompletely resected canine mast cell tumors. Anticancer Res.26(6B), 4585–4589 (2006).
- Spugnini EP, Baldi A, Vincenzi B et al. Intraoperative versus postoperative electrochemotherapy in high grade soft tissue sarcomas: a preliminary study in a spontaneous feline model. Cancer Chemother. Pharmacol.59(3), 375–381 (2007).
- Cemazar M, Tamzali Y, Sersa G et al. Electrochemotherapy in veterinary oncology. J. Vet. Intern. Med.22(4), 826–831 (2008).
- Kodre V, Cemazar M, Pecar J, Sersa G, Cor A, Tozon N. Electrochemotherapy compared to surgery for treatment of canine mast cell tumours. In Vivo23(1), 55–62 (2009).
- Allegretti JP, Panje WR. Electroporation therapy for head and neck cancer including carotid artery involvement. Laryngoscope111(1), 52–56 (2001).
- Rodriguez-Cuevas S, Barroso-Bravo S, Almanza-Estrada J, Cristobal-Martinez L, Gonzalez-Rodriguez E. Electrochemotherapy in primary and metastatic skin tumors: Phase II trial using intralesional bleomycin. Arch. Med. Res.32(4), 273–276 (2001).
- Rols MP, Bachaud JM, Giraud P, Chevreau C, Roche H, Teissie J. Electrochemotherapy of cutaneous metastases in malignant melanoma. Melanoma Res.10(5), 468–474 (2000).
- Burian M, Formanek M, Regele H. Electroporation therapy in head and neck cancer. Acta Otolaryngol. (Stockh.)123(2), 264–268 (2003).
- Bloom DC, Goldfarb PM. The role of intratumour therapy with electroporation and bleomycin in the management of advanced squamous cell carcinoma of the head and neck. Eur. J. Surg. Oncol.31(9), 1029–1035 (2005).
- Byrne CM, Thompson JF, Johnston H et al. Treatment of metastatic melanoma using electroporation therapy with bleomycin (electrochemotherapy). Melanoma Res.15(1), 45–51 (2005).
- Tijink BM, De Bree R, Van D, Leemans CR. How we do it: chemo-electroporation in the head and neck for otherwise untreatable patients. Clin. Otolaryngol.31(5), 447–451 (2006).
- Sadadcharam M, Soden DM, O’Sullivan GC. Electrochemotherapy: an emerging cancer treatment. Intl. J. Hyperthermia24(3), 263–273 (2008).
- Möller MG, Salwa S, Soden DM, O’Sullivan GC. Electrochemotherapy as an adjunct or alternative to other treatments for unresectable or in-transit melanoma. Exp. Rev. Anticancer Ther.9(11), 1611–1630 (2009).
- Heller R, Gilbert R, Jaroszeski MJ. Clinical applications of electrochemotherapy. Adv. Drug Deliv. Rev.35(1), 119–129 (1999).
- Heller R, Jaroszeski MJ, Reintgen DS et al. Treatment of cutaneous and subcutaneous tumors with electrochemotherapy using intralesional bleomycin. Cancer83(1), 148–157 (1998).
- Gothelf A, Mir LM, Gehl J. Electrochemotherapy: results of cancer treatment using enhanced delivery of bleomycin by electroporation. Cancer Treat. Rev.29(5), 371–387 (2003).
- Testori A, Rutkowski P, Marsden J et al. Surgery and radiotherapy in the treatment of cutaneous melanoma. Ann. Oncol.20, 22–29 (2009).
- Titomirov AV, Sukharev S, Kistanova E. In vivo electroporation and stable transformation of skin cells of newborn mice by plasmid DNA. Biochim. Biophys. Acta1088(1), 131–134 (1991).
- Rols MP, Delteil C, Golzio M, Dumond P, Cros S, Teissie J. In vivo electrically mediated protein and gene transfer in murine melanoma. Nat. Biotechnol.16(2), 168–171 (1998).
- Aihara H, Miyazaki J. Gene transfer into muscle by electroporation in vivo. Nat. Biotechnol.16(9), 867–870 (1998).
- Mir LM, Bureau MF, Gehl J et al. High-efficiency gene transfer into skeletal muscle mediated by electric pulses. Proc. Natl Acad. Sci. USA96(8), 4262–4267 (1999).
- Satkauskas S, Bureau MF, Puc M et al. Mechanisms of in vivo DNA electrotransfer: respective contributions of cell electropermeabilization and DNA electrophoresis. Mol. Ther.5(2), 133–140 (2002).
- Satkauskas S, Andre F, Bureau MF, Scherman D, Miklavcic D, Mir LM. Electrophoretic component of electric pulses determines the efficacy of in vivo DNA electrotransfer. Hum. Gene Ther.16(10), 1194–1201 (2005).
- Cemazar M, Golzio M, Sersa G, Rols MP, Teissie J. Electrically-assisted nucleic acids delivery to tissues in vivo: where do we stand? Curr. Pharm. Des.12(29), 3817–3825 (2006).
- Kanduser M, Miklavcic D, Pavlin M. Mechanisms involved in gene electrotransfer using high- and low-voltage pulses – an in vitro study. Bioelectrochemistry74(2), 265–271 (2009).
- Neumann E, Schaeferridder M, Wang Y, Hofschneider PH. Gene-transfer into mouse lyoma cells by electroporation in high electric-fields. EMBO J.1(7), 841–845 (1982).
- Pavselj N, Preat V. DNA electrotransfer into the skin using a combination of one high- and one low-voltage pulse. J. Control Release106(3), 407–415 (2005).
- Heller LC, Heller R. In vivo electroporation for gene therapy. Hum. Gene Ther.17(9), 890–897 (2006).
- Prud’homme GJ, Glinka Y, Khan AS, Draghia-Akli R. Electroporation-enhanced nonviral gene transfer for the prevention or treatment of immunological, endocrine and neoplastic diseases. Curr. Gene Ther.6(2), 243–273 (2006).
- Daud AI, DeConti RC, Andrews S et al. Phase I trial of interleukin-12 plasmid electroporation in patients with metastatic melanoma. J. Clin. Oncol.26(36), 5896–5903 (2008).
- Al-Sakere B, Bernat C, Andre F et al. A study of the immunological response to tumor ablation with irreversible electroporation. Technol. Cancer Res. Treat.6(4), 301–305 (2007).
- Al-Sakere B, Andre F, Bernat C et al. Tumor ablation with irreversible electroporation. PLoS ONE2(11), e1135 (2007).
- Miller L, Leor J, Rubinsky B. Cancer cells ablation with irreversible electroporation. Technol. Cancer Res. Treat.4(6), 699–705 (2005).
- Puc M, Rebersek S, Miklavcic D. Requirements for a clinical electrochemotherapy device – electroporator. Radiol. Oncol.31, 816–827 (1997).
- Sersa G, Miklavcic D, Cemazar M, Rudolf Z, Pucihar G, Snoj M. Electrochemotherapy in treatment of tumours. Eur. J. Surg. Oncol.34(2), 232–240 (2008).
- Miklavcic D, Pucihar G, Pavlovec M et al. The effect of high frequency electric pulses on muscle contractions and antitumor efficiency in vivo for a potential use in clinical electrochemotherapy. Bioelectrochemistry65(2), 121–128 (2005).
- Snoj M, Cemazar M, Kolar BS, Sersa G. Effective treatment of multiple unresectable skin melanoma metastases by electrochemotherapy. Croat. Med. J.48(3), 391–395 (2007).
- Miklavcic D, Semrov D, Mekid H, Mir LM. A validated model of in vivo electric field distribution in tissues for electrochemotherapy and for DNA electrotransfer for gene therapy. Biochim. Biophys. Acta Gen. Subj.1523(1), 73–83 (2000).
- Corovic S, Pavlin M, Miklavcic D. Analytical and numerical quantification and comparison of the local electric field in the tissue for different electrode configurations. Biomed. Eng. Online6, 37 (2007).
- Corovic S, Zupanic A, Miklavcic D. Numerical modeling and optimization of electric field distribution in subcutaneous tumor treated with electrochemotherapy using needle electrodes. IEEE Trans. Plasma Sci.36(4), 1665–1672 (2008).
- Miklavcic D, Corovic S, Pucihar G, Pavselj N. Importance of tumour coverage by sufficiently high local electric field for effective electrochemotherapy. EJC Suppl.4(11), 45–51 (2006).
- Sel D, Cukjati D, Batiuskaite D, Slivnik T, Mir LM, Miklavcic D. Sequential finite element model of tissue electropermeabilization. IEEE Trans. Biomed. Eng.52(5), 816–827 (2005).
- Zupanic A, Corovic S, Miklavcic D. Optimization of electrode position and electric pulse amplitude in electrochemotherapy. Radiol. Oncol.42(2), 93–101 (2008).
- Sersa G, Cemazar M, Miklavcic D. Antitumor effectiveness of electrochemotherapy with cis-diamminedichloroplatinum(II) in mice. Cancer Res.55(15), 3450–3455 (1995).
- Domenge C, Orlowski S, Luboinski B et al. Antitumor electrochemotherapy – new advances in the clinical protocol. Cancer77(5), 956–963 (1996).
- Heller R, Jaroszeski M, Perrott R, Messina J, Gilbert R. Effective treatment of B16 melanoma by direct delivery of bleomycin using electrochemotherapy. Melanoma Res.7(1), 10–18 (1997).
- Cemazar M, Milacic R, Miklavcic D, Dolzan V, Sersa G. Intratumoral cisplatin administration in electrochemotherapy: antitumor effectiveness, sequence dependence and platinum content. Anticancer Drugs9(6), 525–530 (1998).
- Jaroszeski MJ, Dang V, Pottinger C, Hickey J, Gilbert R, Heller R. Toxicity of anticancer agents mediated by electroporation in vitro. Anticancer Drugs11(3), 201–208 (2000).
- Cemazar M, Parkins CS, Holder AL, Chaplin DJ, Tozer GM, Sersa G. Electroporation of human microvascular endothelial cells: evidence for an anti-vascular mechanism of electrochemotherapy. Br. J. Cancer84(4), 565–570 (2001).
- Mir LM, Orlowski S. Mechanisms of electrochemotherapy. Adv. Drug Delivery Rev.35(1), 107–118 (1999).
- Belehradek J, Orlowski S, Ramirez LH, Pron G, Poddevin B, Mir LM. Electropermeabilization of cells in tissues assessed by the qualitative and quantitative electroloading of bleomycin. Biochim. Biophys. Acta Biomembr.1190(1), 155–163 (1994).
- Cemazar M, Miklavcic D, Scancar J, Dolzan V, Golouh R, Sersa G. Increased platinum accumulation in SA-1 tumour cells after in vivo electrochemotherapy with cisplatin. Br. J. Cancer79(9–10), 1386–1391 (1999).
- Mir LM, Orlowski S, Poddevin B, Belehradek J. Electrochemotherapy tumor treatment is improved by interleukin-2 stimulation of the host’s defenses. Eur. Cytokine Netw.3(3), 331–334 (1992).
- Sersa G, Cemazar M, Menart V, GabercPorekar V, Miklavcic D. Anti-tumor effectiveness of electrochemotherapy with bleomycin is increased by TNF-α on SA-1 tumors in mice. Cancer Lett.116(1), 85–92 (1997).
- Sersa G, Miklavcic D, Cemazar M, Belehradek J, Jarm T, Mir LM. Electrochemotherapy with CDDP on LPB sarcoma: comparison of the anti-tumor effectiveness in immunocompetent and immunodeficient mice. Bioelectrochem. Bioenerg.43, 279–283 (1997).
- Sersa G, Jarm T, Kotnik T et al. Vascular disrupting action of electroporation and electrochemotherapy with bleomycin in murine sarcoma. Br. J. Cancer98(2), 388–398 (2008).
- Sersa G, Cemazar M, Miklavcic D, Chaplin DJ. Tumor blood flow modifying effect of electrochemotherapy with bleomycin. Anticancer Res.19(5B), 4017–4022 (1999).
- Mir LM, Roth C, Orlowski S et al. Systemic antitumor effects of electrochemotherapy combined with histoincompatible cells secreting interleukin-2. J. Immunother.17(1), 30–38 (1995).
- Heller L, Pottinger C, Jaroszeski M-L, Gilbert R, Heller R. In vivo electroporation of plasmids encoding GM-CFS or interleukin-2 into exisiting B16 melanomas combined with electrochemotherapy induces long-term antitumour immunity. Melanoma Res.10, 577–583 (2000).
- Sersa G, Beravs K, Cemazar M, Miklavcic D, Demsar F. Contrast enhanced MRI assessment of tumor blood volume after application of electric pulses. Electro. Magnetobiol.17, 299–306 (1998).
- Ramirez LH, Orlowski S, An D et al. Electrochemotherapy on liver tumours in rabbits. Br. J. Cancer77(12), 2104–2111 (1998).
- Sersa G, Cemazar M, Parkins CS, Chaplin DJ. Tumour blood flow changes induced by application of electric pulses. Eur. J. Cancer35(4), 672–677 (1999).
- Gehl J, Skovsgaard T, Mir LM. Vascular reactions to in vivo electroporation: characterization and consequences for drug and gene delivery. Biochim. Biophys. Acta Gen. Subj.1569(1–3), 51–58 (2002).
- Dujardin N, Staes E, Kalia Y, Clarys P, Guy R, Preat V. In vivo assessment of skin electroporation using square wave pulses. J. Control. Release79(1–3), 219–227 (2002).
- Jain RK. Transport of molecules across tumor vasculature. Cancer Metastasis Rev.6(4), 559–593 (1987).
- Vaupel P, Hockel M. Blood supply, oxygenation status and metabolic micromilieu of breast cancers: characterization and therapeutic relevance. Int. J. Oncol.17(5), 869–879 (2000).
- Tozer GM, Kanthou C, Baguley BC. Disrupting tumour blood vessels. Nat. Rev. Cancer5(6), 423–435 (2005).
- Folkman J. Opinion – angiogenesis: an organizing principle for drug discovery? Nat. Rev. Drug Discov.6(4), 273–286 (2007).
- Chaplin DJ, Hill SA, Bell KM, Tozer GM. Modification of tumor blood flow: current status and future directions. Semin. Radiat. Oncol.8(3), 151–163 (1998).
- Siemann DW, Horsman MR. Vascular targeted therapies in oncology. Cell Tissue Res.335(1), 241–248 (2009).
- Sersa G, Krzic M, Sentjurc M et al. Reduced blood flow and oxygenation in SA-1 tumours after electrochemotherapy with cisplatin. Br. J. Cancer87(9), 1047–1054 (2002).
- Sersa G, Cemazar M, Miklavcic D. Tumor blood flow modifying effects of electrochemotherapy: a potential vascular targeted mechanism. Radiol. Oncol.37(1), 43–48 (2003).
- Ivanusa T, Beravs K, Cemazar M, Jevtic V, Demsar F, Sersa G. MRI macromolecular contrast agents as indicators of changed tumor blood flow. Radiol. Oncol.35(2), 139–147 (2001).
- Jarm T, Cemazar M, Sersa G. Tumor blood flow-modifying effects of electroporation and electrochemotherapy – experimental evidence and implications for the therapy. In: Advanced Electroporation Techniques in Biology and Medicine. Pakhomov, AG, Miklavcic D, Markov MS (Eds). CRC Press, USA 401–424 (2010).
- Pavselj N, Bregar Z, Cukjati D, Batiuskaite D, Mir LM, Miklavcic D. The course of tissue permeabilization studied on a mathematical model of a subcutaneous tumor in small animals. IEEE Trans. Biomed. Eng.52(8), 1373–1381 (2005).
- Kanthou C, Kranjc S, Sersa G, Tozer G, Zupanic A, Cemazar M. The endothelial cytoskeleton as a target of electroporation-based therapies. Mol. Cancer Ther.5(12), 3145–3152 (2006).
- Usaj M, Trontelj K, Hudej R, Kanduser M, Miklavcic D. Cell size dynamics and viability of cells exposed to hypotonic treatment and electroporation for electrofusion optimization. Radiol. Oncol.43(2), 108–119 (2009).
- Valic B, Golzio M, Pavlin M et al. Effect of electric field induced transmembrane potential on spheroidal cells: theory and experiment. Eur. Biophys. J. Biophys. Lett.32(6), 519–528 (2003).
- Sentjurc M, Cemazar M, Sersa G. EPR oximetry of tumors in vivo in cancer therapy. Spectrochim. Acta A Mol. Biomol. Spectrosc.60, 1379–1385 (2004).
- Jarm T, Cemazar M, Steinberg F, Streffer C, Sersa G, Miklavcic D. Perturbation of blood how as a mechanism of anti-tumour action of direct current electrotherapy. Physiol. Meas.24(1), 75–90 (2003).
- Jarm T, Sersa G, Miklavcic D. Oxygenation and blood flow in tumors treated with hydralazine: evaluation with a novel luminescence-based optic sensor. Technol. Health Care10, 363–380 (2002).
- Cör A, Cemazar M, Plazar N, Sersa G. Comparison between hypoxic markers pimonidazole and glucose transporter 1 (Glut-1) in murine fibrosarcoma tumours after electrochemotherapy. Radiol. Oncol.43(3), 195–202 (2009).
- Cemazar M, Parkins CS, Holder AL, Kranjc S, Chaplin DJ, Sersa G. Cytotoxicity of bioreductive drug tirapazamine is increased by application of electric pulses in SA-1 tumours in mice. Anticancer Res.21(2A), 1151–1156 (2001).
- Larkin JO, Collins CG, Aarons S et al. Electrochemotherapy – aspects of preclinical development and early clinical experience. Ann. Surg.245(3), 469–479 (2007).
- Campana LG, Mocellin S, Basso M et al. Bleomycin-based electrochemotherapy: clinical outcome from a single institution’s experience with 52 patients. Ann. Surg. Oncol.16(1), 191–199 (2009).
- Byrne CM, Thompson JF. Role of electrochemotherapy in the treatment of metastatic melanoma and other metastatic and primary skin tumors. Expert Rev. Anticancer Ther.6(5), 671–678 (2006).
- Kubota Y, Mir LM, Nakada T, Sasagawa I, Suzuki H, Aoyama N. Successful treatment of metastatic skin lesions with electrochemotherapy. J. Urol.160(4), 1426–1426 (1998).
- Gehl J, Geertsen PF. Efficient palliation of haemorrhaging malignant melanoma skin metastases by electrochemotherapy. Melanoma Res.10(6), 585–589 (2000).
- Gehl J, Geertsen PF. Palliation of haemorrhaging and ulcerated cutaneous tumours using electrochemotherapy. EJC Suppl.4(11), 35–37 (2006).
- Snoj M, Cemazar M, Srnovrsnik T, Kosir SP, Sersa G. Limb sparing treatment of bleeding melanoma recurrence by electrochemotherapy. Tumori95(3), 398–402 (2009).
- Fletcher WS, Pommier RF, Lum S, Wilmarth TJ. Surgical treatment of metastatic melanoma. Am. J. Surg.175(5), 413–417 (1998).
- Fraker DL, Alexander HR, Andrich M, Rosenberg SA. Palliation of regional symptoms of advanced extremity melanoma by isolated limb perfusion with melphalan and high-dose tumor necrosis factor. Cancer J. Sci. Am.1, 104–105 (1995).
- Noorda EM, Vrouenraets BC, Nieweg OE, van Geel A, Eggermont AM, Kroon BB. Repeat isolated limb perfusion with TNF a and melphalan for recurrent limb melanoma after failure of previous perfusion. Eur. J. Surg. Oncol.32(3), 318–324 (2006).
- Grunhagen DJ, de Wilt JH, Graveland WJ, van Geel AN, Eggermont AM. The palliative value of tumor necrosis factor α-based isolated limb perfusion in patients with metastatic sarcoma and melanoma. Cancer106(1), 156–162 (2006).
- Sasso CM, Hubner C, Wall S. Intraarterial embolization of bleeding melanoma. J. Vasc. Nurs.13(1), 27–28 (1995).
- Lavee J, Onik G, Mikus P, Rubinsky B. A novel nonthermal energy source for surgical epicardial atrial ablation: irreversible electroporation. Heart Surg. Forum10(2), E162–E167 (2007).
- Rubinsky J, Onik G, Mikus P, Rubinsky B. Optimal parameters for the destruction of prostate cancer using irreversible electroporation. J. Urol.180(6), 2668–2674 (2008).
- Nuccitelli R, Chen X, Pakhomov AG et al. A new pulsed electric field therapy for melanoma disrupts the tumor’s blood supply and causes complete remission without recurrence. Int. J. Cancer125(2), 438–445 (2009).
- Cemazar M, Golzio M, Sersa G et al. Control by pulse parameters of DNA electrotransfer into solid tumors in mice. Gene Ther.16(5), 635–644 (2009).
- Andre FM, Gehl J, Sersa G et al. Efficiency of high- and low-voltage pulse combinations for gene electrotransfer in muscle, liver, tumor, and skin. Hum. Gene Ther.19(11), 1261–1271 (2008).
- Trochon-Joseph V, Martel-Renoir D, Mir LM et al. Evidence of antiangiogenic and antimetastatic activities of the recombinant disintegrin domain of metargidin. Cancer Res.64(6), 2062–2069 (2004).
- Kranjc S, Cemazar M, Grosel A, Scancar J, Sersa G. Electroporation of LPB sarcoma cells in vitro and tumors in vivo increases the radiosensitizing effect of cisplatin. Anticancer Res.23(1A), 275–281 (2003).
- Sersa G, Kranjc S, Cemazar M. Improvement of combined modality therapy with cisplatin and radiation using electroporation of tumors. Int. J. Radiat. Oncol. Biol. Phys.46(4), 1037–1041 (2000).
- Kranjc S, Tevz G, Kamensek U, Vidic S, Cemazar M, Sersa G. Radiosensitizing effect of electrochemotherapy in a fractionated radiation regimen in radiosensitive murine sarcoma and radioresistant adenocarcinoma tumor model. Radiat. Res.172(6), 677–685 (2009).
- Pendas S, Jaroszeski MJ, Gilbert R et al. Direct delivery of chemotherapeutic agents for the treatment of hepatomas and sarcomas in rat models. Radiol. Oncol.32, 53–64 (1998).
- Metal Complexes in Cancer Chemotherapy. Keppler BK (Ed.). Weinheim, Germany Wiley-VCH (1993).
- Sava G, Alessio E, Bergamo A, Mestroni G. Sulfoxide ruthenium complexes: non-toxic tools for the selective treatment of solid tumour metastases. In: Biological Inorganic Chemistry 1. Clarke MJ, Sadler PJ (Eds). Springer, Berlin, Germany (1999).
- Bicek A, Turel I, Kanduser M, Miklavcic D. Combined therapy of the antimetastatic compound NAMI-A and electroporation on B16F1 tumour cells in vitro. Bioelectrochemistry71(2), 113–117 (2007).
- Hudej R, Turel I, Kanduser M et al. The influence of electroporation on cytotoxicity of anticancer ruthenium(III) complex KP1339 in vitro and in vivo. Anticancer Res. (2010) (In press).
- Bertacchini C, Margotti PM, Bergamini E, Lodi A, Ronchetti M, Cadossi R. Design of an irreversible electroporation system for clinical use. Technol. Cancer Res. Treat.6(4), 313–320 (2007).
- Miklavcic D, Snoj M, Zupanic A et al. Towards treatment planning and treatment of deep-seated solid tumors by electrochemotherapy. Biomed. Eng. Online9, 10 (2010).
- Schmiedl U, Ogan M, Paajanen H et al. Albumin labeled with GD-DTPA as an intravascular, blood pool enhancing agent for MR imaging – biodistribution and imaging studies. Radiology162(1), 205–210 (1987).
- Demsar F, Roberts TPL, Schwickert HC et al. A MRI spatial mapping technique for microvascular permeability and tissue blood volume based on macromolecular contrast agent distribution. Magn. Reson. Med.37(2), 236–242 (1997).
- Sapirstein LA. Regional blood flow by fractional distribution of indicators. Am. J. Physiol.193, 161–168 (1958).
- Shepherd AP, Öberg PÅ. Laser-Doppler blood flowmetry.Kluwer Academic Publishers, MA, USA (1990).
- Delorme S, Krix M. Contrast-enhanced ultrasound for examining tumor biology. Cancer Imaging6(1), 148–152 (2006).
- Sersa G, Krzic M, Sentjurc M et al. Reduced tumor oxygenation by treatment with vinblastine. Cancer Res.61(10), 4266–4271 (2001).
- O’Hara JA, Blumenthal RD, Grinberg OY et al. Response to radioimmunotherapy correlates with tumor pO2 measured by EPR oximetry in human tumor xenografts. Radiat. Res.155(3), 466–473 (2001).
- Swartz HM, Clarkson RB. The measurement of oxygen in vivo using EPR techniques. Phys. Med. Biol.43(7), 1957–1975 (1998).
- Collingridge DR, Young WK, Vojnovic B et al. Measurement of tumor oxygenation: A comparison between polarographic needle electrodes and a time-resolved luminescence-based optical sensor. Radiat. Res.147(3), 329–334 (1997).
- Vaupel P, Schlenger K, Knoop C, Hockel M. Oxygenation of human tumors – evaluation of tissue oxygen distribution in breast cancers by computerized O2 tension measurements. Cancer Res.51(12), 3316–3322 (1991).
- Menon C, Fraker DL. Tumor oxygenation status as a prognostic marker. Cancer Lett.221(2), 225–235 (2005).
- Raleigh JA, Chou SC, Bono EL, Thrall DE, Varia MA. Semiquantitative immunohistochemical analysis for hypoxia in human tumors. Int. J. Radiat. Oncol. Biol. Phys.49, 569–574 (2001).
- Chen CH, Pore N, Behrooz A, Ismail-Beigi F, Maity A. Regulation of glut1 mRNA by hypoxia-inducible factor-1 – interaction between H-ras and hypoxia. J. Biol. Chem.276(12), 9519–9525 (2001).
- Cooper R, Sarioglu S, Sokmen S et al. Glucose transporter-1 (GLUT-1): a potential marker of prognosis in rectal carcinoma? Br. J. Cancer89(5), 870–876 (2003).