Immigrants’ voyages to new lands have been among the most exciting and noble of human endeavors Citation[101]. It requires amazing courage to flee oppression, to leave behind everything that is familiar, and to chance the hostility of a completely alien culture in order to find freedom, opportunity and a better life. Every person, every family, has a different story to tell about the reasons for, and the circumstances, surrounding their departure from their native country. Immigrants are moving to a new country for the best of motives: the desire to improve their lives; the urge to leave countries whose governments they could not abide; and the willingness to work for another country where individuals can live in freedom and dignity. Very many immigrants and refugees, including Albert Einstein, Ernst B Chain, Selman A Waksman, Enrico Fermi, Sigmund Freud, Eric Fromm, Bertold Brecht, Jean Gabin, Charles de Gaulle, Thomas Mann, Jean-Jacques Rousseau, François-Marie Arouet (Voltaire), Victor Hugo and Henry A Kissinger, have made a remarkable contribution to the welfare and happiness of mankind.
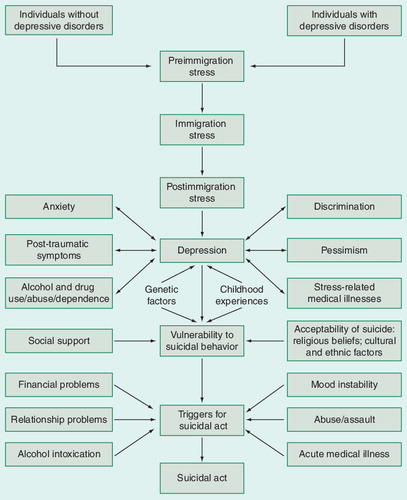
Immigration is difficult and stressful Citation[1]. The sociocultural and political characteristics of the country of origin and the immigration social policy of the host country play important roles in the acculturation process of immigrants. Many immigrants suffer from psychiatric disorders and some immigrants attempt or commit suicide Citation[1–4,101,102]. Here, I propose the following model of suicidal behavior among depressed immigrants .
Future immigrants consist of two groups: individuals without depressive disorders, and individuals with depressive disorders. Possibly, many individuals who did not have depressive disorders in their countries of origin but became depressed and suicidal in a new country had certain maladaptive personality traits and/or some degree of depression, and/or suicidal tendencies, before immigrating to the new country Citation[4]. However, it is very possible that practically healthy individuals become depressed and suicidal as a result of immigration-related chronic stress.
All future immigrants experience preimmigration stress. Preimmigration stress is frequently related to traumatic experiences, loss of home, livelihood, social position, family, friends, community, homeland, familiar language, feeling of an uncertain future and doubts regarding whether the decision to emigrate/immigrate is correct. Preimmigration stress can have a direct influence on mental and physical health status immediately after arrival into a new country.
All immigrants experience immigration stress. The process of relocation is difficult for many people. Immediately upon arrival to a new country, immigrants frequently become targets for abuse, cruelty and corruption.
Postimmigration stress is frequently very severe. Immigrants often face difficulty adjusting to their new home in a new country. This can be for a number of reasons, including coping with trauma experienced in their native country, overcoming cultural and language barriers, and encountering discrimination Citation[1,2,5]. The effects of immigration on psychological and social well being are especially profound for certain populations, including children, women, individuals with disabilities, and those with limited financial resources. Many immigrants are often forced to take low-qualified jobs, even though they have the training and education for professional jobs. They cannot sustain their former economic and social status, which can lead to psychological distress. Language barriers often force otherwise intelligent immigrant children and adolescents to study at one to two grades lower than their peers Citation[6], creating a situation that can be potentially demoralizing.
A combination of pre- and post-immigration stressful situations can lead to severe and long-lasting psychological and behavioral problems, including depression, anxiety, post-traumatic stress disorder, alcohol and/or drug abuse, and a high risk for suicide. Immigrants who experienced more stressful life events presented progressive deterioration in psychological well being Citation[7].
Postimmigration experience is affected by health-related social policy and political factors. For example, US immigration policy programs in the 1960s and 1970s took good care of the Cubans fleeing the Castro regime, and Cubans were among the healthiest of all Latino groups in the USA Citation[8].
Immigrants are frequently depressed Citation[1,9]. Depression in immigrants is associated with anxiety, post-traumatic symptoms, alcohol and/or drug use/abuse/dependence, pessimism, and stress-related medical illnesses such as hypertension, metabolic syndrome and diabetes. For example, a higher prevalence of impaired lipid metabolism in immigrants in comparison with the native population has been observed Citation[9]. A recent study has shown that immigrants who experience downward social mobility are at elevated risk for major depression Citation[10]. Depression in immigrants is often related to discrimination. It is a vicious cycle: discrimination leads to, or aggravates, depression; and depressed immigrants are easier targets for discrimination.
Depressive disorders are associated with a negative bias in information processing Citation[11]. Depressed immigrants are more likely to remember negative than positive emotional information. This may negatively affect their ability to adjust to their new environment.
Substance abuse may be more pronounced if the immigrants acculturate into a more permissive society, abandoning the more traditional or conservative values of their former culture Citation[12]. Genetic factors and childhood experiences play an important role in the pathophysiology of depression and other psychiatric conditions in immigrants.
Depression, associated psychiatric and medical problems, genetic makeup, childhood experiences, availability of social support, cultural acceptability of suicide, the degree of preimmigration, immigration, and postimmigration stress, and other factors, determine the vulnerability for suicidal behavior among depressed immigrants. The suicidal process may be different for individuals of immigrant background compared with people living in the host country.
The theory of anomie (lack of social regulation) suggests that it is not poverty that causes suicide, but rather declines in socioeconomic status that produce anomie and result in suicide Citation[13]. Thus, immigrant populations that are accustomed to low (or high) socioeconomic status may not be negatively affected by the continuance of this status in their new host country.
Triggers for suicidal behavior among immigrants include financial problems, relationship problems, mood instability (e.g., the onset of a major depressive episode), alcohol intoxication, abuse/assault and acute medical illness.
Suicidal acts can be attributed to the coincidence of a trigger with a vulnerability for suicidal behavior Citation[14]. Suicidal acts include suicide attempts and suicides. Many depressed individuals have suicidal thoughts however they never attempt suicide Citation[15]. Immigrants typically show higher rates of suicide than individuals in their countries of origin and/or from the host country into which they have migrated Citation[2,3,102]. For example, in Sweden, a significant over-representation of immigrants has been reported in the total cases of suicide Citation[3]. It is of interest to note that ethnic immigrant groups subjected to more negative ethnophaulisms, or hate speech, were more likely to commit suicide Citation[16].
Despite the critical need for mental health services, immigrants face significant obstacles to receiving quality mental healthcare, including financial difficulties, the lack of culturally and linguistically appropriate services, and mistrust of mental health providers Citation[1,102]. Suicide prevention among immigrants requires comprehensive, co-ordinated and continuous health and mental health services for immigrant populations provided by culturally competent professionals. It is important to recognize psychiatric disorders in these populations. Social and legal help should also be provided. Suicide prevention hotlines where immigrants can speak their native language may be very important. Special attention should be given to immigrants and refugees who experienced traumatic circumstances, including exposure to war and natural disasters, human trafficking, and physical, sexual and emotional abuse. Suicide prevention in this high-risk population should include the treatment of medical and neurological disorders.
The recognition of the full professional equality of immigrants, their social acceptance and respect for their vocational and cultural aspirations may be the best forms of protection against mental health problems among immigrants. It is critical to create a welcoming environment where immigrants can realize their potential and succeed.
Financial & competing interests disclosure
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- Immigration and Mental Health: Stress, Psychiatric Disorders and Suicidal Behavior Among Immigrants and Refugees. Sher L, Vilens A (Eds). Nova Science Publishers, NY, USA (In press).
- Ferrada-Noli M, Åsberq M, Ormstad K, Nordström P. Definite and undetermined forensic diagnoses of suicide among immigrants in Sweden. Acta Psychiatrica Scand.91(2), 130–135 (2007).
- Burvill PW. Migrant suicide rates in Australia and in country of birth. Psychol. Med.28, 201–208 (1998).
- Sher L. On the role of neurobiological and genetic factors in the etiology and pathogenesis of suicidal behavior among immigrants. Med. Hypotheses53(2), 110–111 (1999).
- Bhugra D. Migration, distress and cultural identity. Brit. Med. Bull.60, 129–141 (2004).
- Sun S, Fung, WW, Kwong K. A Study on Mental Health of New Arrival Children for Their First Two Years of Settlement in Hong Kong. City University of Hong Kong & Christian Action, Hong Kong (2000).
- Slonim-Nevo V, Mirsky J, Rubinstein L, Nauck B. The impact of familial and environmental factors on the adjustment of immigrants: a longitudinal study. J. Fam. Issues30(1), 92–123 (2009).
- Vega W A, Amaro H. Latino outlook: good health, uncertain prognosis. Ann. Rev. Pub. Health15, 39–67 (1994).
- Tselmin S, Korenblum W, Reimann M, Bornstein SR, Schwarz PE. The health status of Russian-speaking immigrants in Germany. Horm. Metab. Res.39(12), 858–861 (2007).
- Nicklett EJ, Burgard SA. Downward social mobility and major depressive episodes among Latino and Asian-American immigrants to the United States. Am. J. Epidemiol.170(6), 793–801 (2009).
- Harmer CJ, O’Sullivan U, Favaron E et al. Effect of acute antidepressant administration on negative affective bias in depressed patients. Am. J. Psychiatry166(10), 1178–1184 (2009).
- De La Rosa M. Acculturation and Latino adolescents’ substance use: a research agenda for the future. Subst. Use Misuse37(4), 429–456 (2002).
- Durkheim E. Suicide: A Study in Sociology. Spalding JA, Simpson G (Eds). Routledge & K Paul, London, UK (1952).
- Sher L. A model of suicidal behavior in war veterans with posttraumatic mood disorder. Med. Hypotheses73(2), 215–219 (2009).
- Sher L, Oquendo MA, Mann JJ. Risk of suicide in mood disorders. Clin. Neurosci. Res.1(5), 337–344 (2001).
- Mullen B, Smyth JM. Immigrant suicide rates as a function of ethnophaulisms: hate speech predicts death. Psychosom. Med.66(3), 343–348 (2004).
Websites
- Schoolland K. Courage, fear, and immigration: the significance of welcoming newcomers in a free economy. Julian Simon Memorial Lecture. Liberty Institute, New Delhi, India. January 10, 2005 www.idfresearch.org/semImmigration.pdf (Accessed May 23 2009)
- American Psychological Association. The mental health needs of immigrants www.apa.org/ppo/ethnic/immigranthealth.html (Accessed May 23 2009)