
Abstract
Background
Several studies have demonstrated the positive effects of physical activity on skeletal muscle mass and muscle strength in women with osteoporosis. However, the impact of Nordic walking training on sarcopenia-related parameters in women with low bone mass remains unknown. Therefore, the purpose of this study was to evaluate the impact of 12 weeks of Nordic walking training on skeletal muscle index, muscle strength, functional mobility, and functional performance in women with low bone mass.
Materials and methods
The participants were 45 women, aged 63–79 years, with osteopenia or osteoporosis. The subjects were randomly assigned either to an experimental group (12 weeks of Nordic walking training, three times a week) or to a control group. Skeletal muscle mass and other body composition factors were measured with octapolar bioimpedance InBody 720 analyser. Knee extensor and flexor isometric muscle strength were measured using Biodex System 4 Pro™ dynamometers. This study also used a SAEHAN Digital Hand Dynamometer to measure handgrip muscle strength. The timed up-and-go test was used to measure functional mobility, and the 6-minute walk test was used to measure functional performance.
Results
Short-term Nordic walking training induced a significant increase in skeletal muscle mass (P=0.007), skeletal muscle index (P=0.007), strength index of the knee extensor (P=0.016), flexor (P<0.001), functional mobility (P<0.001), and functional performance (P<0.001) and a significant decrease in body mass (P=0<006), body mass index (P<0.001), and percent body fat (P<0.001) in participants. Regarding handgrip muscle strength, no improvement was registered (P=0.315). No significant changes in any of the analyzed parameters were observed in the control group.
Conclusion
Overall, short-term Nordic walking training induces positive changes in knee muscle strength and functional performance in women with low bone mass. This finding could be applied in clinical practice for intervention programs in women with osteopenia and osteoporosis.
Introduction
Osteoporosis and sarcopenia are common among the elderly and are associated with significant morbidity and mortality.Citation1 Given the current secular trends in demographic groups with high longevity, the burden of both osteoporosis and sarcopenia may continue to increase.
In 2011, The International Working Group on Sarcopenia in Older People defined sarcopenia as “the age-associated loss of skeletal muscle mass and function.”Citation2 In 2009, the European Working Group on Sarcopenia in Older People (EWGSOP) had already defined sarcopenia as a syndrome characterized by progressive and generalized loss of skeletal muscle mass (SM) and strength with a risk of adverse outcomes such as physical disability and poor quality of life and death.Citation3
Importantly, sarcopenia is well known to be highly correlated with frailty and an increased risk of falling in the elderly.Citation4 In addition to increasing the risk of falling, sarcopenia might also decrease bone strength by reducing mechanical loading on the skeleton.Citation5,Citation6 Sarcopenic subjects more often experience tiredness during daily activities and have lower fat mass and lean mass.Citation7
Some studies have suggested that sarcopenia is observed in 24% and 50% of individuals aged ≥70 and <80 years, respectively.Citation8 Sarcopenia seems to be associated with many harmful clinical components, making this geriatric syndrome a real public health burden.Citation7 In one American study, sarcopenia and its consequences were estimated to cost the US health care system 18 billion dollars. Sarcopenia is therefore an expensive issue for the health care system.Citation9
It is commonly believed that physical activity can slow down the loss of SM and function. Italian researchers have recommended three types of training for sarcopenic older people: aerobic exercise, resistance exercise, and power training.Citation10 A vast amount of literature has reviewed various training programs in which resistance and power training are engaged.Citation11,Citation12 However, aerobic exercise for osteopenia prevention has not received much attention. These exercises are considered vital as they are specially recommended by the American College of Sports Medicine and the American Heart Association.Citation13
Nordic walking (NW) is one of the aerobic exercises, which has become a highly popular mode of physical activity in Central and Northern Europe.Citation14 NW is an activity oriented with specially designed poles used to push against the ground with each stride to activate the upper body while walking. The results of studies conducted in the Scandinavian countries among younger adults confirm that NW is more effective than walking without sticks.Citation15 NW provides additional benefits in upper body muscular strengthCitation16 and improvement of aerobic capacity.Citation17 Thus, it can be considered as an important tool in the prevention of sarcopenia in older adults. Studies have also proved that practicing NW increases gait speed and cardiovascular metabolism,Citation16 decreases systolic blood pressure in postmenopausal women,Citation18 and reduces blood ferritin levels in elderly women.Citation19
Additionally, the use of poles increases the stability of the body while walking. Therefore, to a certain extent, NW protects against falls, which is particularly important among those who, after undergoing trauma related to a fall, are afraid of walking.
No research has been found to prove the effect of NW training on sarcopenia-related parameters in women with reduced bone mass. Therefore, the aim of this preliminary study was to evaluate the impact of 12 weeks of NW training on skeletal muscle index (SMI), muscle strength, functional mobility, and functional performance in women with low bone mass.
Materials and methods
Ethics
This study was approved by the Bioethics Commission of Regional Medical Chamber according to the Declaration of Helsinki, under the process number KB-29/14. Before commencing the study, all the subjects received a verbal and written description of the experiment, and they signed an informed consent form before participation.
Participants
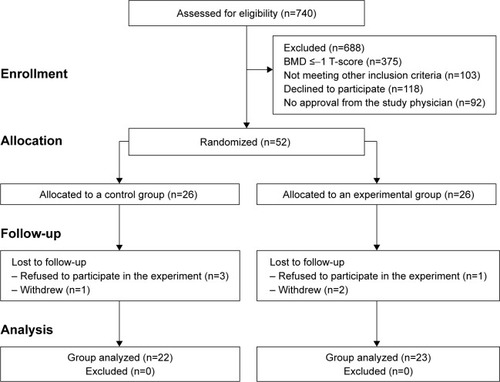
The study sample consisted of 45 postmenopausal women aged 63–79 years (M=68.7 years, ±4.43). All the participants were recruited from a group of 740 women (who agreed to the primary screening), attending various lectures at the University of the Third Age. The recruitment process is illustrated in . The sample was randomly divided into two groups. The first group – the control group (CG) – consisted of 22 women (68.32±4.06 years). Participants in the CG involved in normal daily activities appropriate to their age range. None of the subjects were engaged in an organized physical activity regimen. Women from the second group, called the experimental group (EG), participated in regular NW training (see “Training program” section) (n=23; 69.04±4.81 years).
Figure 1 Recruitment process.
The inclusion criteria were as follows: postmenopausal female (ie, a female who had experienced her last period >12 months ago), nonsmoking female, diagnosed with osteopenia or osteoporosis. Low bone mass was defined by a T-score ≤−1.Citation20
Subjects were excluded according to the following criteria: uncontrolled hypertension, oophorectomy, rheumatoid arthritis, pulmonary disease, and type 2 diabetes treated with insulin.
All the participants had to undergo a compulsory medical examination that revealed no contraindications to physical exercise. They were asked to provide information regarding prescribed medications as part of this study. These data included information regarding medications that may affect bone metabolism, including hormone replacement therapy, corticosteroids, and antiresorptive therapies.
A total of 17 women declared taking medicine (eight people from EG and nine from CG). Examined women were under the permanent care of a medical specialist, who monitored dosed medicines. Additionally, to limit the effects of possible variables on the study results, medicines and their doses were not altered throughout the 12-week study.
Measures
Assessment of body composition and anthropometry
Body mass (BM), SM, and percent body fat (PBF) were measured with an octapolar bioimpedance InBody 720 analyser (Biospace, Seoul, Korea) using standard protocols, with participants wearing light clothing without shoes. This technology employs eight contact electrodes: two are positioned on the palm and thumb of each hand, and the others are placed on the front part of the feet and on the heels. This device supported the study to analyze five basic body parts – left and right upper limb, trunk, and left and right lower limb – independently at frequencies of 1, 5, 50, 250, 500, and 1,000 kHz.
The validity of bioimpedance (BIA) has been documented in several studies. In one study, no statistical difference between magnetic resonance imaging (MRI)-measured and BIA-derived values for SM was observed.Citation21 In other studies, BIA was used to determine skeletal muscle cutpoints for identifying elevated physical disability risk in older adults.Citation22
EWGSOP indicates that BIA may be considered an alternative to Dual-energy X-ray absorptiometry (DXA) for determining SM and, by extension, SMI. To calculate SMI, the following formula recommended by EWGSOP was used: SM/heightCitation2. EWGSOP defines three clinical sarcopenia conditions: 1) pre-sarcopenia, which is characterized by low muscle mass without impact on muscle strength or physical performance; 2) sarcopenia, which is characterized by low muscle mass, plus low muscle strength or low physical performance; and 3) severe sarcopenia, which is identified when all three criteria of the definition are met: low muscle mass, low muscle strength, and low physical performance.Citation3
Body height (in cm) was measured with an accuracy of 0.1 cm. During measurement, each subject was placed barefoot in the orthostatic position. Body mass index (BMI) was calculated as BM/heightCitation2 (kg/m2).
Assessment of muscle strength
Chan et al reported that quadriceps strength and handgrip strength (HS) were independently associated with health outcomes at baseline, including quality of life, disability in daily living, hospitalization, and gait speed.Citation23 The measurements could also aid in the identification of older adults in primary care with the poorest health outcomes.
HS was measured to estimate muscle strength and was performed with a hand dynamometer (SAEHAN Digital Hand Dynamometer, SAEHAN, Changwon, Korea). During the HS test, participants had to hold the dynamometer in their hand with the arm stretched parallel to the body while being instructed to stand upright. This measure was performed three times on the dominant hand with a rest interval of 1 min between measurements; finally, the best performance was used as the maximum peak (PK) of HS (in kg). The statistical analysis also included mean peak (mean PK).
Knee extensor and flexor muscle strength were measured using a Biodex System 4 Pro™ dynamometer (Biodex Medical Systems, Inc., Shirley, NY, USA). Data collection was performed by using a Compaq Desk Pro personal computer and Biodex software using the standard Biodex protocol. After a standardized warm-up, subjects were positioned in the equipment according to the manufacturer’s manual (seated with arms hanging along the body, hands holding the lateral handles, and strap stabilization of trunk, hip, and tested thigh, with the knee flexed to 90°). For testing, the protocol reported by Symons et al with slight modifications was used.Citation24 The isometric strength test was used for three maximal contractions, provided that one single contraction lasted 5 s with 30 s breaks. The seat position was adjusted for the leg length of each tested person. Data were analyzed using the results obtained from the dominant lower limb. The parameters of maximum peak torque (PKTQ) and mean peak torque (mean PKTQ) were analyzed for knee extension/flexion.
In this study, two recommended strength indexes were used. To calculate the first strength index, the following formula was used: PK HS/BM (kg).Citation25 The second strength index was calculated as PKTQ knee extensor muscle strength (Nm)/BM (kg).Citation26
Assessment of functional mobility and functional performance
The EWGSOP also recommends extending sarcopenia diagnosis with an additional component, that is, low physical performance. In this respect, the EWGSOP recommends a wide range of tests of physical performance.Citation3 Two of these tests include the timed up-and-go (TUG) test, which has been proved to be a satisfactory measure of functional mobility in elderly persons,Citation27 and the 6-minute walk test.
The TUG test measures the time(s) required for a subject to rise from a chair, walk 3 m, turn around, walk back to the chair, and sit down. It has been shown to be a predictor of sarcopenia in hospitalized patients with a mean age of 70.4±7.7 years.Citation28
The functional performance of the participants was assessed based on the distance covered in the 6-minute walk test.Citation29 The experimental procedure was as follows: 5 min in sitting position, 6 min of continuous walking at a comfortable self-selected speed, and 5 min for recovery. The tests were performed on an athletic track where the temperature was 17°C. The following instruments were used for the test: a stopwatch, measuring tape, and a Polar RS-400 heart rate monitor (Polar Electro Oy, Kempele, Finland). The 6-minute walk distance (6MWD) covered during the test was recorded in meters.
Training program
All training sessions were conducted by a certified NW coach and were held outdoors, three times a week, for 60 min each, over a period of 12 weeks. Participants used Nordic poles (Exel, Espoo, Finland). According to the recommendation of the International NW Federation (INWA), the pole length was determined by multiplying each subject’s height in centimeter by 0.68 and rounding down to the nearest 5 cm. During the first week of training with poles, the main goal was to improve form during the march.
Each training unit consisted of three phases. During the warm-up phase (10–13 min), women performed isotonic exercises with poles to improve arm, leg, and torso flexibility and static and dynamic body balance.
The main part of the NW training (40 min) consisted in walking with poles over a distance of 3–4 km to reach an average heart rate between 50% and 70% of the age-dependent maximal heart rate; HRmax=206–0.88× age,Citation30 [(HRmax − HRrest) × (0.5–0.7)] + HRrest. During NW, all the subjects used the diagonal-pole back condition technique recommended by INWA.Citation31 According to the aforementioned technique, the correct usage of the poles involves a backward pole position during the loading phase, active and dynamic use of the poles, and control of the poles with the grip and strap.
Every main part of the NW training featured two short active sessions (2 min each). During these sessions, women performed breathing exercises and isometric exercises with an emphasis on the muscles of the lower limbs.
The cool-down exercises (7–10 min) included dynamic and static stretching. Participants’ heart rate was monitored by a Polar RS-400 heart rate monitor.
Statistical analysis
Standard statistical methods were used to calculate mean values and standard deviations (mean ± standard deviation). The Shapiro–Wilk statistical analysis test was used to verify the normality of the data. For normally distributed results, a paired t-test analysis was performed to identify different results significantly. For results that were not normally distributed, a Wilcoxon signed-rank test was applied. The paired t-test or the Wilcoxon test was used for within-group comparisons.
The Brown–Forsyth test was used to verify the homogeneity of the variance. The between-group comparisons were performed using analysis of variance (ANOVA) tests. For homogeneous results, an ANOVA for repeated measurements and post hoc honestly significant difference Tukey test for equal sample sizes were performed to identify different results significantly. For heterogeneous results, an ANOVA Friedman’s test and a right post hoc test were applied. In addition, Cohen’s effect size (ES) was calculated to quantify the magnitude of statistical significance. All data were analyzed using the statistical package Statistica 10 (StatSoft, 2010), and the level of significance was P<0.05.
Results
Results pertaining to anthropometry, body composition, SMI, muscle strength, functional mobility, and performance in participants during the study are shown in .
Table 1 Results of the participant variables analyzed in this study
This study did not indicate the presence of sarcopenia in the tested women. The SMI was ≥6.76 kg/m2. At baseline, no statistically significant differences were observed between EG and CG with respect to the analyzed parameters.
For the within-group analysis, after the 12-week training period, SMI (ES=0.22) and SM (ES=0.18) showed significant increases in EG. Moreover, NW training significantly improved knee extensor and flexor muscle strength. Statistically significant increases were observed for knee extensor muscle strength for PKTQ (ES=0.37), mean PKTQ (ES=0.36), and PKTQ/BM (ES=0.47) and knee flexor muscle strength for PKTQ (ES=0.62), mean PKTQ (ES=0.65), and PKTQ/BM (ES=0.70).
After the training period, in the EG, the study also noted statistically significant increases in TUG (ES=0.79) and 6MWD (ES=1.15) and decreases in BM (ES=0.11), BMI (ES=0.10), and PBF (ES=0.30). However, statistical tests did not indicate significant changes in handgrip muscle strength among women in the EG.
In the CG, no significant differences in the analyzed parameters were observed after 12 weeks. However, an ANOVA test showed that after 12 weeks, changes in functional performance – 6MWD (ES=1.07), knee extensor muscle strength for PKTQ/BM (ES=0.62), knee flexor muscle strength for PKTQ (ES=0.71), mean PKTQ (ES=0.65), and PKTQ/BM (ES=0.92) – were statistically significant between the EG and the CG.
Discussion
The current study has shown that 12-week NW training is effective in decreasing BM, BMI, and PBF and increasing SM (2.1%) and SMI (2.08%). Similar results were obtained by South Korean scientists who analyzed changes in body composition among three groups of elderly women (NW group, normal walking group, and CG) after practice of three times a week (60 min long) over a 12-week study period.Citation32 In this study, the NW and normal walking groups showed significant changes in SM (P<0.001 in both groups), in contrast to the results obtained for the CG. Results also indicated significant decreases in weight (P<0.001), BMI (P=0.001), and PBF (P=0.008) after the NW intervention. However, the normal walking group showed significant decreases in weight (P=0.02) and PBF (P=0.005) but not in BMI.
A recent study presented the results obtained after 8 weeks of NW training relative to normal walking training.Citation33 The findings revealed a significantly greater improvement in SM in the elderly group. However, no evidence of a significant decrease in BM or BMI in postmenopausal women was obtained following a shorter (8 weeks) NW training period.Citation18
The aforementioned results are in agreement with those reported in other studies, indicating that NW provides an advantage over general walking because it engages more muscles and results in 20% higher calorie consumption.Citation16
The reported data confirm that 12 weeks of NW training is effective in decreasing weight, PBF, and BMI; thus, the study is worth continuing in patients with sarcopenic obesity. Undertaking such efforts is important because, as other studies indicate, sarcopenic obesity has been associated with a greater risk of incidents of cardiovascular disease and disability than sarcopenia or obesity alone.Citation34,Citation35 Sarcopenic obesity has also been linked to an increased risk of falling in older adults.Citation36
The current study additionally showed that short-term NW training is effective in improving knee muscle strength, as opposed to handgrip muscle strength, in women with osteopenia and osteoporosis.
After 3 months of walking with poles, a statistically significant improvement in knee muscle strength was observed. The greatest improvement was noted in knee flexion muscles, amounting to PKTQ (22.4%), mean PKTQ (24.9%), and PKTQ/BM (22.6%). An improvement in knee extension muscle strength was also observed (PKTQ [11.2%], mean PKTQ [11.1%], and PKTQ/BM [12.4%]).
Similar results were reported by Kocur et al, who studied the effect of 3 weeks (five sessions per week) of NW training and traditional walking on exercise capacity and functional fitness in patients after acute coronary syndrome.Citation37 These studies showed improvements in lower body strength (assessed with “chair stand test”) and coordination of movement and dynamic balance (in “up-and-go test”) in both the training groups. Scores on the chair stand test and up-and-go test increase by 17.9% and 10.2% in the NW group and by 16.1% and 5.8% in the normal walking group, respectively. However, the results (in both tests) were significantly better for the NW group than for the normal walking group.
Parkatti et al showed that 9 weeks of walking with poles led to a moderate increase of 15% in the muscle strength of the lower extremities among the sedentary older people.Citation38 Similarly, Eyigor et al demonstrated an increase in knee extensor muscle strength of 17% after 8 weeks of resistance training combined with walking, balance and flexibility exercises in 20 elderly women.Citation39
A precise comparison of our results with those reported in the aforementioned studies is difficult because the authors used different training periods and tests. Certain studies also suggest that the effects of resistance training on muscle strength in older people rest entirely on neural factors in the absence of significant muscle hypertrophy.Citation40 Certain similar adaptive mechanisms are likely to occur during NW training as well. This study shows that the increases in strength are greater than those observed for SM. These results are supported by available data demonstrating greater effects of exercise on muscle strength than on muscle mass in the elderly.Citation41
The results of this study concerning the increase in knee muscle strength can be essential in treating sarcopenic therapy in women with low bone mass because osteoporosis associated with the postmenopausal period can negatively affect the increase in lower limb strength in physically active women. Moreover, the loss of strength in the knee extensor muscles is of particular interest because these muscles have been consistently demonstrated to be associated with physical function in daily activities such as climbing stairs, walking, and rising from a chair.Citation42 Brech et al reported that women with postmenopausal osteoporosis presented diminished knee extensor and flexor muscle strength compared with women without postmenopausal osteoporosis.Citation43
The current study did not indicate any significant effect of the 12-week NW training period on handgrip muscle strength in participants. Similar results were noted by Lee and Park, who did not register significant improvements in upper extremity muscle strength in frail people aged ≥70 years.Citation44
As NW is a walking-based exercise, it is possible that it is more effective in improving the strength of the legs than the arms. However, certain studies showed that 12 weeks of NW training significantly increased handgrip muscle strength (by 10.57%) in elderly.Citation30
The differences between the results of this study and those reported in the literature may be due to the technique used during the march. Scientists from Korea report that women use a modified technique while walking with poles, whereas our training involved full NW technique (pole back condition). The relationship between the technique used and equipment-related factors and their effect on training have also been highlighted in other studies.Citation37,Citation45–Citation47
In the CG, there were no statistically significant changes in muscle strength among the analyzed parameters (for knee and handgrip). These findings are in agreement with those reported by other authors.Citation30,Citation34
It is generally known that elderly women with low bone mineral density show changes in gait,Citation48 greater postural imbalance, and a greater predisposition to falls.Citation49 Therefore, exercises aimed at strengthening muscles, tai chi, and general walking are recommended to increase balance and functional mobility. The present study demonstrated that NW is effective in improving functional mobility in women with reduced bone mass. The improvement in the EG was 9.29%, which was statistically significant.
The findings of Kocur et al suggest that a 12-week NW training program has a positive impact on selected gait parameters and may improve the postural control of women aged >65 years, according to the results of selected functional tests.Citation50 Willson et al showed that using walking poles increased walking speed (P=0.0001–0.0004), stride length (P<0.0001), and stance time (P<0.0001) relative to those measures when no poles were used.Citation51 However, in another study, no improvement in gait parameters pertaining to walking speed was observed after a 9-week NW intervention.Citation38
The functional mobility improvement in the participating women could also be related to an improvement in knee muscle strength under the effects of NW training. Wiacek et al showed a correlation between the strength of the lower body and postural balance in women aged 65–94 years living in long-term care facilities.Citation52
Another study showed that a 10-week NW program significantly improved balance, functional mobility, and aerobic endurance (P=0.001, P=0.04, and P<0.0001, respectively) in older adults aged >60 years.Citation53 An improvement in functional mobility was also reported following a 12-week aerobic resistance training period in healthy older adults.Citation54
However, Takeshima et al reported a lack of improvement in balance (measured using the Balance Master Platform System and an 8-foot up-and-go test) after 12 weeks of NW training in older adults (8 men and 9 women; 70±5 years).Citation17 Although functional mobility improved in the NW group, it should also be noted that there was a discrepancy between the training effects indicated by previous research and the lack of a difference in balance improvement between the EG and CG. This finding prevents us from recommending NW as a superior exercise for functional mobility improvement in women with low bone mass.
The present study demonstrated that 12 weeks of NW training improved functional performance in women with low bone mass. A significant increase in the distance covered during a 6-minute walk is not surprising because previous results have suggested that NW is more effective than conventional walking in increasing oxygen consumption in healthy adults.Citation16
Figueiredo et al demonstrated that NW training and traditional walking training improved the gait speed and endurance of the elderly. NW ES were moderate for a 6-minute walk (ES=0.53) and large for gait speed (ES=0.68). Walking demonstrated a moderate ES for a 6-minute walk (ES=0.53) but a small size for gait speed (ES=0.33).Citation55
Other scientists have observed that regular NW training (8–13 weeks) in women increases high-density lipoprotein levels and maximal oxygen uptake and reduces total cholesterol, low-density lipoprotein, and triglyceride levels.Citation19,Citation56,Citation57 The results of the current study are worth highlighting because they can be essential in constructing training programs targeted at fall prevention in women with lower bone mass. Park et al reported that a decline in physical performance leads to a deterioration in the ability to cope with physical challenges on a daily basis and may increase one’s fear of falling regardless of previous experience with falls.Citation58 Moreover, in women with decreased bone mass, the loss of muscle strength may have worse clinical implications because of the relationship between reduced mobility and a possible fall and its consequences. Brech et al indicate that knee extensor or muscle strengthening through physical activity programs may be an alternative for preventing falls.Citation43
Hence, specific physical activity programs targeting muscle strength and postural balance should be encouraged and should be commenced before menopause or at the onset of menopause.Citation42
Limitations
This study was limited by various factors. First, the sample size for analysis was small owing to the number of participants who were excluded. The recruitment process aimed to minimalize the effects of variables that could impact the main purpose of the study. Thus, ultimately, only 45 of 740 women were involved in the research project. Second, the subjects who participated in this study were recruited from the University of the Third Age and voluntarily attended a health examination. Women with fragile health did not take part in this study, which might have affected the results. Third, this study did not indicate the presence of sarcopenia in the tested women. However, all the participants had low bone mass, consistent with the aim of the study. These limitations may have contributed to the underestimation of certain relationships.
Conclusion
The current study showed that 12 weeks of NW training induced significant increases in SM, SMI, knee isometric muscle strength, functional performance, and functional mobility. Moreover, NW training was effective in decreasing BM, BMI, and percent fat mass in older women with low bone mass.
The results could provide important clinical implications for therapists to pay more attention to NW training when selecting appropriate therapeutic methods, particularly in increasing knee muscle strength and functional performance in women with osteopenia and osteoporosis.
Acknowledgments
The researchers gratefully acknowledge all of the research participants. This research was funded by the Gdansk University of Physical Education and Sport within the framework of the European Union project entitled “Active lifestyles and predictors of risk for incapacity on senior population – RISINC2013”. Additionally reserach was supported by National Science Centre (Poland), project no 2014/15/B/NZ7/00976.
Disclosure
The authors report no conflicts of interest in this work.
References
- EdwardsMHDennisonEMAihie SayerAFieldingRCooperCOsteoporosis and sarcopenia in older ageBone20158012613025886902
- FieldingRAVellasBEvansWJSarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International Working Group on SarcopeniaJ Am Med Dir Assoc20111224925621527165
- Cruz-JentoftAJBaeyensJPBauerJMEuropean Working Group on Sarcopenia in Older PeopleSarcopenia. European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older PeopleAge Ageing201039441242320392703
- TopinkováEAging, disability and frailtyAnn Nutr Metab200852Suppl 1S6S11
- RochefortGYPalluSBenhamouCLOsteocyte: the unrecognized side of bone tissueOsteoporos Int20102191457146920204595
- Di MonacoMValleroFDi MonacoRTapperoRPrevalence of sarcopenia and its association with osteoporosis in 313 older women following a hip fractureArch Gerontol Geriatr2011521717420207030
- BeaudartCReginsterJYPetermansJQuality of life and physical components linked to sarcopenia: The SarcoPhAge studyExp Gerontol20156910311025979160
- BaumgartnerRNKoehlerKMGallagherDEpidemiology of sarcopenia among the elderly in New MexicoAm J Epidemiol19981477557639554417
- JanssenIShepardDSKatzmarzykPTRoubenoffRThe healthcare costs of sarcopenia in the United StatesJ Am Geriatr Soc2004521808514687319
- IolasconGDi PietroGGimiglianoFPhysical exercise and sarcopenia in older people: position paper of the Italian Society of Orthopaedics and Medicine (OrtoMed)Clin Cases Miner Bone Metab201411321522125568656
- PetersonMDSenAGordonPMInfluence of resistance exercise on lean body mass in aging adults: a meta-analysisMed Sci Sports Exerc201143224925820543750
- PuthoffMLNielsenDHRelationships among impairments in lower extremity strength and power, functional limitations, and disability in older adultsPhys Ther200787101334134717684086
- NelsonMERejeskiWJBlairSNPhysical activity and public health in older adults. Recommendation from the American College of Sports Medicine and the American Heart AssociationCirculation20071161094110517671236
- TurkZVidensekSMicetic TurkDNordic walking: a new form of physical activity in the elderlyActa Med Croatica200761Suppl 1S33S36
- TschentscherMNiederseerDNiebauerJHealth benefits of Nordic walking: a systematic reviewAm J Prev Med2013441768423253654
- ChurchTSEarnestCPMorssGMField testing of physiological responses associated with Nordic walkingRes Q Exerc Sport200273329630012230336
- TakeshimaNIslamMMRogersMEEffects of Nordic walking compared to conventional walking and band-based resistance exercise on fitness in older adultsJ Sports Sci Med201312342243024149147
- LatosikEZubrzyckiIZOssowskiZPhysiological responses associated with Nordic-walking training in systolic hypertensive postmenopausal womenJ Hum Kinet20144318519025713659
- KortasJPrusikKFlisDEffect of Nordic walking training on iron metabolism in elderly womenClin Interv Aging2015101889189626664101
- CzerwinskiEBadurskiJEMarcinowska-SuchowierskaEOsieleniecJCurrent understanding of osteoporosis according to the position of the World Health Organization (WHO) and International Osteoporosis FoundationOrtop Traumatol Rehabil2007933735617882114
- ChienMYHuangTYWuYTPrevalence of sarcopenia estimated using a bioelectrical impedance analysis prediction equation in community-dwelling elderly people in TaiwanJ Am Geriatr Soc2008561710171518691288
- JanssenIBaumgartnerRNRossRRosenbergIHRoubenoffRSkeletal muscle cutpoints associated with elevated physical disability risk in older men and womenAm J Epidemiol200415941342114769646
- ChanOYvan HouwelingenAHGusseklooJBlomJWden ElzenWPComparison of quadriceps strength and handgrip strength in their association with health outcomes in older adults in primary careAge (Dordr)2014365971425280549
- SymonsTBVandervoortAARiceCLOverendTJMarshGDReliability of a single-session isokinetic and isometric strength measurement protocol in older menJ Gerontol A Biol Sci Med Sci200560111411915741293
- DongRWangXGuoQClinical relevance of different handgrip strength indexes and mobility limitation in the elderly adultsJ Gerontol A Biol Sci Med Sci20167119610226409067
- ChoquetteSBouchardDRDoyonCYSénéchalMBrochuMDionneIJRelative strength as a determinant of mobility in elders 67–84 years of age, a nuage study: nutrition as a determinant of successful agingJ Nutr Health Aging201014319019520191251
- PodsiadloDRichardsonSThe timed “Up & Go”: a test of basic functional mobility for frail elderly personsJ Am Geriatr Soc19913921421481991946
- MartinezBPGomesIBOliveiraCSAccuracy of the timed up and go test for predicting sarcopenia in elderly hospitalized patientsClinics (Sao Paulo)201570536937226039955
- American Thoracic Society StatementGuidelines for the six-minute walk testAm J Respir Crit Care Med200216611111712091180
- GulatiMShawLJThistedRABlackHRBairey MerzCNArnsdorfMFHeart rate response to exercise stress testing in asymptomatic women: the St. James women take heart projectCirculation201012213013720585008
- International Nordic Walking AssociationINWA Instructor Manual3rd edHelsinkiSuomen Latu2005
- SongMSYooYKChoiCHKimNCEffects of Nordic walking on body composition, muscle strength, and lipid profile in elderly womenAsian Nurs Res20137117
- ParkSDYuSHThe effects of Nordic and general walking on depression disorder patients’ depression, sleep, and body compositionJ Phys Ther Sci20152782481248526357429
- ZamboniMMazzaliGFantinFRossiADi FrancescoVSarcopenic obesity: a new category of obesity in the elderlyNutr Metab Cardiovasc Dis20081838839518395429
- StephenWCJanssenISarcopenic-obesity and cardiovascular disease risk in the elderlyJ Nutr Health Aging200913546046619390754
- KimJHChoiSHLimSSarcopenia and obesity: gender-different relationship with functional limitation in older personsJ Korean Med Sci2013281041104723853487
- KocurPDeskur-SmieleckaEWilkMDylewiczPEffects of Nordic walking training on exercise capacity and fitness in men participating in early, short-term inpatient cardiac rehabilitation after an acute coronary syndrome – a controlled trialClin Rehabil20092311995100419786418
- ParkattiTPerttunenJWackerPImprovements in functional capacity from Nordic walking: a randomized-controlled trial among elderly peopleJ Aging Phys Act20122019310521949243
- EyigorSKarapolatHDurmazBEffects of a group-base exercise program on the physical performance, muscle strength and quality of life in older womenArch Gerontol Geriatr20074525927117303264
- FlaniganKMGiuseppeLGriffinJKRalphWAge related biology and disease of muscle and nerveNeurol Clin1998166596689666043
- FronteraWRMeredithCNO’ReillyKPKnuttgenHGEvansWJStrength conditioning in older men: skeletal muscle hypertrophy and improved functionAm Physiol Soc19886410381043
- HenwoodTRRiekSTaaffeDRStrength versus muscle power-specific resistance training in community-dwelling older adultsJ Gerontol A Biol Sci Med Sci2008631839118245765
- BrechGCAlonsoACLunaNMGreveJMCorrelation of postural balance and knee muscle strength in the sit-to-stand test among women with and without postmenopausal osteoporosisOsteoporos Int20132472007201323376968
- LeeHSParkJHEffects of Nordic walking on physical functions and depression in frail people aged 70 years and aboveJ Phys Ther Sci20152782453245626357424
- Figard-FabreHFabreNLeonardiASchenaFPhysiological and perceptual responses to Nordic walking in obese middle-aged women in comparison with the normal walkEur J Appl Physiol201010861141115120091181
- HansenEASmithGEnergy expenditure and comfort during Nordic walking with different pole lengthsJ Strength Cond Res2009231187119419528847
- DziubaAKŻurekGGarrardIWierzbicka-DamskaIBiomechanical parameters in lower limbs during natural walking and Nordic walking at different speedsActa Bioeng Biomech2015179510125951842
- ElDeebAMKhodairASThree-dimensional analysis of gait in postmenopausal women with low bone mineral densityJ Neuroeng Rehabil2014115524720866
- SilvaRBCosta-PaivaLMoraisSSMezzaliraRFerreiraNDPinto-NetoAMPredictors of falls in women with and without osteoporosisJ Orthop Sports Phys Ther201040958258820508328
- KocurPWiernickaMWilskiMDoes Nordic walking improves the postural control and gait parameters of women between the age 65 and 74: a randomized trialJ Phys Ther Sci201527123733373726834341
- WillsonJTorryMRDeckerMJKernozekTSteadmanJREffects of walking poles on lower extremity gait mechanicsMed Sci Sports Exerc200133114214711194099
- WiacekMHagnerWHagner-DerengowskaMCorrelations between postural stability and strength of lower body extremities of women population living in long-term care facilitiesArch Gerontol Geriatr200948334634918440656
- VirágAKarócziCKJakabAVassZKovácsEGondosTShort-term and long-term effects of Nordic walking training on balance, functional mobility, muscle strength and aerobic endurance among Hungarian community-living older people: a feasibility studyJ Sports Med Phys Fitness201455111285129225303166
- Desjardins-CrépeauLBerrymanNFraserSAEffects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adultsClin Interv Aging2016111287129927698558
- FigueiredoSFinchLMaiJAhmedSHuangAMayoNENordic walking for geriatric rehabilitation: a randomized pilot trialDisabil Rehabil2013351296897523066879
- HagnerWHagner-DerengowskaMWiacekMZubrzyckiIZChanges in level of VO2 max, blood lipids and waist circumference in the response to moderate endurance training as a function of ovarian agingMenopause20091651009101319339904
- Kukkonen-HarjulaKHiilloskorpiHMänttäriASelf-guided brisk walking training with or without poles: a randomized-controlled trial in middle-aged womanScand J Med Sci Sports2007171431632317038158
- ParkJHChoHShinJHRelationship among fear of falling, physical performance, and physical characteristics of the rural elderlyAm J Phys Med Rehabil20149337938624196975