
Abstract
Andropausal and depressive symptoms are common in aging males and may be associated with hormone deficiency. We investigated the severity of andropausal and depressive symptoms, as well as their hormonal determinants, in 196 middle-aged and elderly men (age range: 40–80 years) with prediabetes (PD) and in 184 healthy peers. PD was diagnosed according to the definition of the American Diabetes Association. The severity of andropausal and depressive symptoms was assessed using the Aging Males’ Symptoms Rating Scale and the Self-Rating Depression Scale. Total testosterone (TT), calculated free testosterone (cFT), dehydroepiandrosterone sulfate (DHEAS), and insulin-like growth factor 1 (IGF-1) were measured. The prevalence of andropausal syndrome in men with PD was significantly higher than that in healthy men (35% vs 11%, respectively). In men with PD aged 40–59 years, the severity of sexual, psychological, and all andropausal symptoms was greater than in healthy peers, while in elderly men (60–80 years), only the severity of psychological symptoms was greater than in healthy peers. The severity of depressive symptoms in the middle-aged men with PD was greater than in healthy peers, while the severity of depressive symptoms in elderly men with PD and healthy peers was similar. The higher prevalence of andropausal symptoms was independently associated with cFT and IGF-1 in middle-aged men and with TT and DHEAS in elderly men with PD. The more severe depression symptoms were associated with low TT and DHEAS in middle-aged men and with low cFT and DHEAS in elderly men with PD. In conclusion, the prevalence of andropausal symptoms, especially psychological, was higher in prediabetic patients as compared to healthy men, while the severity of depressive symptoms was higher only in middle-aged men with PD. Hormonal determinants of andropausal and depressive symptoms are different in middle-aged and elderly patients, but endocrine tests are necessary in all men with PD.
Introduction
There is growing attention in regard to health disorders in men because advanced age of this population is associated with numerous health problems. Recently, a distinct rise in the incidence of psychological disturbances has been noted among middle-aged and elderly men,Citation1 thus indicating an urgent need for additional studies to investigate this population. One of the conditions associated with aging males is the decreasing of testosterone levels by 1%–2% per year after the age of 40 years.Citation2 The prevalence of “biochemical hypogonadism” is high: 23.3% in 40-year-old to 79-year-old men from the European Male Ageing Study;Citation3 but this does not necessarily mean clinical hypogonadism because the majority of men with low testosterone levels remain asymptomatic.Citation4 However, some aging men do develop symptomatic hypogonadism, which is associated with diffuse symptoms, such as sexual dysfunction, metabolic disorders, overall dissatisfaction, as well as increasing emotional disturbances, moodiness, irritability, nervousness, depression, fatigability, poor concentration, and deteriorating memory. The combination of low testosterone level and an array of the above symptoms has been denoted variously, including andropausal syndrome (AS) or late-onset hypogonadism (LOH).Citation5 The diagnosis of LOH is based on clinical symptoms associated only with sexual functions and low testosterone levels, while AS refers to a clinical syndrome with characteristic psychological, sexual, and somatovegetative signs and symptoms usually attributed to the age-related decline in circulating testosterone, dehydroepiandrosterone sulfate (DHEAS), and insulin-like growth factor 1 (IGF-1).Citation6
Prediabetes (PD) is the condition in which the patients have slight increase in blood glucose concentrations than the normal levels but they are not said to be diabetic. Criteria for diagnosis of PD according to the American Diabetes Association (ADA) are as follows: impaired fasting glucose (IFG), impaired glucose tolerance (IGT), and/or glycated hemoglobin (HbA1c) levels ranging from 5.7% to 6.4%.Citation7 PD status is considered a risk factor for the further development of type 2 diabetes mellitus (T2DM) and cardiovascular disease (CVD).Citation8 The prevalence of PD in Poland is one of the highest in the world; approximately 16% of the population is estimated to have IGT and by the year 2035, the number of people with IGT is projected to increase to ~19%.Citation9
Subnormal testosterone concentrations in T2DM, described in 2004,Citation10 are present in 25%–40% of patients.Citation11 Patients with T2DM have been recognized to have a higher prevalence of major depressive disorders and depressive symptoms than the general population.Citation12 In our previous study,Citation13 we described the high prevalence of testosterone deficiency and LOH among a population of Polish men with PD, but the prevalence of other anabolic hormone deficiency in patients with PD is unknown and probably may have several consequences, such as depressive symptoms, low quality of life, and sexual dysfunctions. Only a few studies have demonstrated relationships between anabolic hormones, sexual functions, and IFGCitation14 or PDCitation15 in men.
Therefore, in this study, we aimed to compare the Self-rating Depression Scale (SDS) and the Aging Males’ Symptoms (AMS) rating scale between patients with PD and a control group, as well as to investigate the clinical and hormonal determinants of the severity of these symptoms in middle-aged and elderly men with PD.
Materials and methods
Study population
This study was performed at the Department of Internal Diseases, Diabetology and Endocrinology, Medical University of Warsaw, Poland, in patients attending the outpatient clinic for glucose metabolism disorders. The inclusion criteria were 1) a laboratory-confirmed PD, 2) age 40–80 years, and 3) no history of depression. The exclusion criteria were as follows: 1) diabetes mellitus type 1 or 2; 2) conditions that contribute to sexual dysfunction, such as history of surgery in the pelvic cavity, hyperprolactinemia, and thyroid function disturbances; 3) recent or current testosterone replacement, androgen deprivation therapy, or any hormonal treatment, either during the study or in history; and 4) lack of informed written consent. We recruited 196 consecutive patients with PD (aged between 40 years and 80 years) from the outpatient clinic. In addition, as a control group, 184 healthy men, matched by age and with a fasting plasma glucose (FPG) <5.55 mmol/L (100 mg/dL) and HbA1c <5.7%, were also included. This study was approved by the local Research Ethics Committee and was conducted in accordance with the Declaration of Helsinki; informed consent was obtained from all participants.
PD was diagnosed in patients with IFG ranging from 100 mg/dL to 125 mg/dL (5.6–6.9 mmol/L) and 2-hour glucose concentration in the oral glucose tolerance test (OGTT) of <140 mg/dL (<7.8 mmol/L) or in patients with IGT (2-hour glucose concentration in OGTT ranging from 140 mg/dL to 200 mg/dL or 7.8–11.0 mmol/L) or in patients with HbA1c ranging from 5.7% to 6.4%.Citation7 Because PD is a transitory state with many individuals on repeated testing showing blood glucose in the normal range, FPG and OGTT measurements were repeated after 2–3 weeks and reevaluated. The diagnosis of metabolic syndrome (MetS) was based on the following criteria: waist circumference ≥94 cm and any two of the following: triglycerides ≥150 mg/dL, high-density lipoprotein (HDL)-cholesterol <40 mg/dL, blood pressure ≥130/85 mmHg, and FPG ≥100 mg/dL.Citation16 Height, weight, and waist circumference were measured and body mass index (BMI) was calculated. Obesity was defined as a BMI of 30 kg/m2 or more. CVD was defined as coronary artery disease, congestive heart failure, or arrhythmia. Hypertension and chronic obstructive pulmonary disease were also considered to be present if the participant reported having received the diagnosis or if he/she was receiving medication for the condition.
Assessment of depressive and andropausal symptoms
Subjects filled out a self-administered questionnaire. Depressive symptoms were assessed by means of SDS.Citation17 The SDS consists of ten negatively worded items and ten positively worded items on symptoms of depression. The level of depression was classified as normal (20–29), mild (30–39), moderate (40–49), and severe (≥50). Data on the intensity of andropausal symptoms were assessed using the AMS rating scale.Citation18 The AMS scale includes 17 symptoms divided into three groups: psychological (discouraged, depressed, irritable, anxious, and nervous); sexual (disturbed potency, impaired erectility, problems with libido, decrease in beard growth, and feeling of “having passed the zenith of life”); and somatovegetative (joint and muscle complaints, sweating, need for more sleep, sleep disturbances, weakness, exhaustion, and impaired well-being). The intensity of each symptom was rated between one (low) and five points (high). We analyzed the severity of the three subgroups of andropausal symptoms (three subscores for each cluster) and the total severity of andropausal symptoms (total AMS score, sum of three subscores). AS was diagnosed if the total AMS score was 50 points or higher.Citation18 In our study, we did not investigate the occurrence of LOH, which is diagnosed in patients with symptoms of testosterone deficiency such as low libido, diminished frequency of morning erections, and erectile dysfunctions, as well as decreased testosterone levels.Citation5
Laboratory measurements
In all men with PD, venous blood samples were obtained between 8 am and 10 am. After centrifugation, the serum was collected and frozen at −70°C until analysis. FPG was measured with the enzymatic method using BIOSEN 5040 analyzer (EKF-Diagnostic GmbH, Germany), HbA1c with the high-performance liquid chromatography method using Variant analyzer (Bio-Rad Laboratories Inc, USA). HbA1c values were expressed as percentage according to the National Glycohemoglobin Standardization Program. The serum levels of total testosterone (TT), DHEAS, estradiol (E2), and IGF-1 were measured with immunometric assays (Immulite 2000 and RIA CAC; Siemens Medical Solution, Malvern, PA, USA) and expressed in nanomoles per liter for TT, picograms per milliliter for E2, and nanograms per milliliter for DHEAS and IGF-1 (to convert the values for DHEAS to micromoles per liter, multiply by 0.00271; for converting IGF-1 values to nanomoles per liter, multiply by 0.131; and for converting E2 values to picomoles per liter, multiply by 3.671). To estimate the circulating fraction of free testosterone, we measured the serum level of sex hormone-binding globulin (SHBG) using an immunoassay (Diagnostic Products Corp, San Francisco, CA, USA), and SHBG was expressed in nanomoles per liter. The serum level of calculated free testosterone (cFT), expressed in nanomoles per liter, was calculated with the validated equation of Vermeulen et al.Citation19
Statistical analysis
Statistical analyses were performed using the STATISTICA 9.1 data analysis software system (StatSoft, Tulsa, OK, USA). Most continuous variables had a normal distribution and were expressed as a mean ± standard deviation of the mean. The intergroup differences were tested using the t-test for unpaired samples. Serum DHEAS had a skewed distribution, so they were log-transformed to normalize their distribution, expressed as a median with lower and upper quartiles, and the intergroup differences were tested using the t-test for unpaired samples for the normalized values. Categorized variables were expressed as a number and a percentage, and the intergroup differences were tested using the χ2 test. The relationships between andropausal and depressive symptom scores and various factors, including age, BMI, and HbA1c in men with PD were examined by Pearson’s correlation analyses. Univariable and multivariable linear and logistic regression analyses were applied to establish variables determining the severity of andropausal symptoms (subscores for psychological, sexual, and somatovegetative symptoms, as well as a total AMS score) and depression symptoms, as well as the variables associated with the higher prevalence of AS. Regression analyses were performed separately in middle-aged (40–59 years) and elderly (60–80 years) age groups of men with PD. In the univariable analyses, as the potential determinants of the severity of andropausal and depression symptoms and as the potential risk factors for the higher prevalence of AS, we included the following: age, BMI, HbA1c, total cholesterol, TT, cFT, DHEAS, IGF-1, and E2, as well as comorbidities such as CVD, hypertension, and MetS. During the construction of multivariable models, we included all variables that had been shown to be significant (P<0.05) determinants in the univariable analyses. A P-value <0.05 was considered statistically significant.
Results
A total of 196 men with PD (mean age: 58±4 years) and 184 healthy men (mean age: 61±5 years) were evaluated in this study. In the control group, we observed 98 men aged 40–59 years (mean BMI: 28.6±4.7 kg/m2) and 86 men aged 60–80 years (mean BMI: 30.8±4.3 kg/m2). The baseline characteristics of the men with PD are shown in . Patients with PD aged from 60 years to 80 years had lower TT, cFT, and DHEAS levels (P<0.001, P<0.005, and P<0.01, respectively) and higher E2 levels and BMI (both P<0.05). We observed also statistically significant differences in glucose metabolism parameters between the prediabetic groups. Men with PD aged 60–80 years had higher HbA1c, FPG, and glucose levels in the 2-hour OGTT (P<0.02, P<0.001, and P<0.05, respectively). In addition, total cholesterol and uric acid levels were higher in elderly men with PD, while HDL-cholesterol concentrations were lower in this subgroup of prediabetic patients (all P<0.05). Men with PD aged 60–80 years also presented with more common hypertension and CVD (P<0.01 and P<0.001, respectively), but percentage of current smokers was lower in this age group (P<0.05).
Table 1 Baseline characteristics of men with prediabetes divided according to age
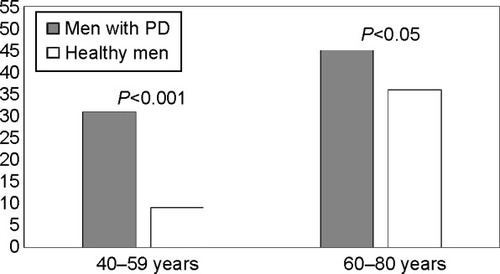
The prevalence of AS in men with PD was significantly higher than in healthy men (35% vs 11%, respectively; P<0.001). Analysis of investigated men after dividing by the age revealed that the prevalence of AS in patients with PD aged 40–59 years was higher compared with that in healthy peers (29% vs 9%, respectively; P<0.001) and that the prevalence of AS in men with PD aged 60–80 years was statistically significantly higher than that observed in healthy peers (43% vs 36%, respectively; P<0.05) (). Among men with PD, the prevalence of AS was significantly higher in subjects aged from 60 years to 80 years when compared with those aged from 40 years to 59 years (43% vs 29%, respectively; P<0.001) ().
Figure 1 Prevalence (%) of andropausal syndrome in men with prediabetes (n=196) and healthy men (n=184).
Abbreviations: AMS, Aging Males’ Symptoms rating scale; PD, prediabetes.
The analysis of severity of andropausal symptoms revealed that in the middle-aged group (40–59 years), the severity of sexual (P<0.001), psychological (P<0.002), and all andropausal symptoms (P<0.001) was greater in prediabetic men compared with the same in healthy peers (). In the elderly group (60–80 years), the severity of sexual, somatovegetative, and all andropausal symptoms was similar in men with PD and healthy peers, while severity of psychological symptoms was greater in elderly men (P<0.01) (). Among men with PD, the severity of sexual, psychological, and all andropausal (but not somatovegetative) symptoms was higher in the elderly group compared with the middle-aged group of patients with PD (all P<0.001) ().
Figure 2 Severity of andropausal symptoms (expressed as points).
Abbreviations: AMS, Aging Males’ Symptoms rating scale; NS, nonsignificant; PD, prediabetes; SDS, Self-rating Depression Scale.
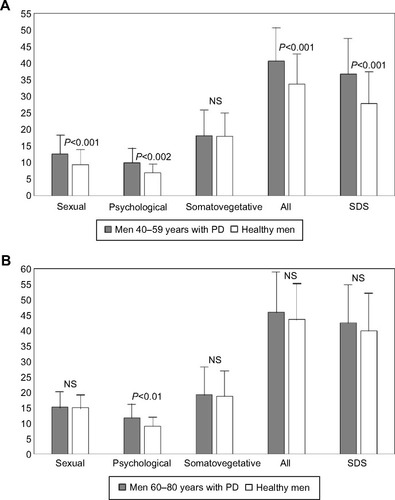
We observed that the severity of depressive symptoms in all men with PD was significantly higher, when compared with healthy men (38.2±7.2 vs 33.5±5.7, respectively; P<0.001). We also showed that the severity of depressive symptoms in the middle-aged group of prediabetic men was significant lower than that observed in elderly patients with PD (36.7±7.7 vs 42.5±7.2, respectively; P<0.002) (). We also showed that the severity of depressive symptoms in the middle-aged men with PD was significantly greater than that in healthy peers (36.7±7.7 vs 27.8±6.8, respectively; P<0.001), while the severity of depressive symptoms in elderly prediabetic and healthy men was similar (42.5±7.2 vs 39.9±6.9, respectively) ().
Analysis of correlations between AMS (total) score and SDS score, as well as the clinical and laboratory variables, in all patients with PD (n=196) revealed that there were only negative, statistically significant correlations between HbA1c and AMS total score (r=−0.3145; P=0.02). We did not observe any additional significant correlations between the analyzed variables, including age and BMI ().
Table 2 Correlations between andropausal (total) and depressive symptoms scores and clinical characteristics in 196 men with prediabetes
In patients with PD aged from 40 years to 59 years, in multivariable linear regression models, the more severe somatovegatative symptoms were independently associated with low serum TT, low cFT, low IGF-1, and high HbA1c levels, as well as with presence of MetS; the more severe sexual symptoms were associated with low TT, low cFT, high HbA1c, and presence of CVD; the more severe psychological symptoms were associated with low cFT, low IGF-1, and presence of CVD (all P<0.05); and the more severe andropausal symptoms (in total) were associated with low cFT (P<0.05) (). The more severe depression symptoms were associated with low TT, low DHEAS, and the presence of CVD (all P<0.05) (). In multivariable logistic regression models, the following variables were independently associated with the higher prevalence of AS in middle-aged men: serum cFT (odds ratio [OR]: 0.66, confidence interval [CI]: 0.42–0.79; P<0.05) and IGF-1 (OR: 1.21, CI: 1.03–1.31; P<0.05) (). In patients with PD aged from 60 years to 80 years, in multivariable linear regression models, the more severe somatovegetative symptoms were independently associated with low cFT, low DHEAS, and presence of CVD and MetS; the more severe sexual symptoms with low TT, low cFT, high HbA1c, and the presence of CVD and MetS; the more severe psychological symptoms with low cFT, low IGF-1, and the presence of CVD; and the more severe andropausal symptoms (in total) were associated with low TT and low DHEAS (all P<0.05) (). The more severe depression symptoms were associated with low cFT, low DHEAS, and the presence of CVD (all P<0.05) (). In multivariable logistic regression models, the following variables were independently associated with the higher prevalence of AS in elderly men: serum TT (OR: 1.01, CI: 0.75–1.34; P<0.05) and DHEAS (OR: 1.98, CI: 1.43–4.12; P<0.05) ().
Table 3 Parameters associated with the severity of andropausal and depressive symptoms in men with prediabetes
Table 4 Risk factors associated with the higher prevalence of AS in men with prediabetes
Discussion
In this study, we investigated the prevalence and severity of andropausal and depressive symptoms in men with PD and the clinical and hormonal determinants of the severity of these symptoms in middle-aged (40–69 years) compared with elderly (50–60 years) men with PD. To achieve these goals, we used the AMS rating scale and SDS.
There are three major findings arising from the present study. First, AS was very common in male patients with PD aged 40–80 years. The prevalence of AS in patients with PD aged 40–59 years waŝ3.5 times higher compared with that in control healthy peers (31% vs 9%, respectively), and the prevalence of AS in men with PD aged 60–80 years was higher than that in healthy peers (44% vs 36%, respectively). Among the men with PD, the prevalence of AS was significantly higher in the elderly when compared with middle-aged men (43% vs 29%, respectively). These results allow to propose that the occurrence of AS (except for psychological symptoms) may be accelerated in patients with PD. Second, the severity of almost all (except somatovegetative) andropausal symptoms in the younger patients was greater in prediabetic men compared with the same in healthy men. In contrast, in the elderly group with PD, the severity of only the psychological symptoms was greater than that observed in healthy peers. We observed also that the severity of depressive symptoms in prediabetic men with no history of depression was higher than in healthy men and that the severity of depressive symptoms in the middle-aged men with PD was lower than that in elderly men with PD. It appears that the higher severity of andropausal and depressive symptoms in patients with PD is associated mainly with metabolic disorders because we did not demonstrate significant correlations between age and both AMS and SDS scores in all groups of patients with PD. Third, in regression analyses, we demonstrated that hormonal determinants of andropausal and depressive symptoms are different in middle-aged and elderly men with PD. In middle-aged men, the more severe andropausal symptoms (in total) were associated with low cFT, the more severe depression symptoms were associated with low TT and low DHEAS, while the higher prevalence of AS was independently associated with serum cFT and IGF-1. In elderly men, the more severe andropausal symptoms (in total) were associated with low TT and low DHEAS, the more severe depression symptoms were associated with low cFT and low DHEAS, while the higher prevalence of AS was independently associated with serum TT and DHEAS.
The prevalence of PD in Poland is one of the highest in the world, with ~16% of the population being estimated to have IGT or IFG;Citation9 therefore, any disorders associated with PD, especially depression and impaired quality of life, are a serious public health problem in Poland. We have previously shownCitation13 that among prediabetic men, LOH was diagnosed in 30% of patients and only in 14% of control group. We also showed inverse relationships between erectile function and cFT levels. These results indicate that PD may have influence on sexual health in men and overall quality of life and mood and that these relationships may be associated with sex hormone levels. The influence of other anabolic hormones, such as DHEAS and IGF-1, on andropausal symptoms in patients with PD is still unknown. Only a few studies have demonstrated relationships between androgens and PD in men. Corona et alCitation14 showed in 1,687 men with sexual dysfunction that 19% of men were classified as IFG and these men had severe erectile dysfunction or hypogonadism more often when compared with normoglycemic men. In the Multi-Ethnic Study of Atherosclerosis (MESA) study, Colangelo et alCitation20 showed that IFG was associated inversely with TT, DHEA, and E2 and that these correlations were significant after adjustment for age and BMI. Ho et alCitation15 demonstrated in 1,306 men that PD was diagnosed in approximately 41% of patients and was associated with an increased risk of subnormal TT compared with healthy individuals (age-adjusted OR =1.87; 95% CI), which was still significant after adjusting for age, BMI, and MetS.
These results clearly indicate that prevalence of testosterone deficiency and hypogonadism among male patients with PD is high and significant. However, the prevalence of andropausal symptoms and depression symptoms in the population of men with PD is still unknown. These symptoms have been documented in men with other chronic diseases. Tkaczyszyn et alCitation6 have shown in a population of 232 men with systolic heart failure that prevalence of AS and the severity of andropausal symptoms in men aged 40–60 years were greater than in healthy peers, while in the age group of 60–80 years, there were no differences in the prevalence of AS and the severity of andropausal symptoms compared with the healthy group. In male patients with T2DM, Corrales et alCitation21 showed high prevalence of low free testosterone and andropausal symptoms in diabetic men and positive correlation between TT and HbA1c levels. Fukui et alCitation22 compared the andropausal symptom scores, such as SDS and the International Index of Erectile Function (IIEF), in 296 men with T2DM with those in healthy peers and showed that SDS and IIEF scores were statistically higher in diabetic patients.
Studies on the relationships between other anabolic hormones and glucose metabolism disturbances have been limited. Colao et alCitation23 demonstrated that IGF1 levels in the low normal range are associated with IFG in males without pituitary diseases, and Kameda et alCitation24 presented association of low DHEAS levels with the progression of male patients with PD to T2DM. These results have suggested that DHEAS and IGF-1 also play an important role in glucose metabolism in men, but their influence on andropausal symptoms in men with PD is still unknown.
As we noted earlier, PD is associated with low testosterone levels; however, the mechanism of this phenomenon is still unclear. Low levels of TT and SHBG (associated with insulin resistance) are independent risk factors in middle-aged men who later developed PD and are inversely correlated with IFG, insulin levels, and IGT.Citation1 But importantly, low testosterone is a risk factor in men who were not initially obese, and low free and bioavailable but not TT levels, after adjustment for age and adiposity, were approximately four times more likely to predict T2DM development. These findings support that the risk does not depend on adiposity.Citation25 Interestingly, men with diabetes type 1 have normal testosterone levels, which is probably due to low insulin levels in patients with diabetes type 1 and high levels in men with T2DM. There is also an inverse relationship between insulin and SHBG, and consequently, plasma levels of TT are lower in men with T2DM.Citation26 Adipose tissue produces cytokines and adipokines, of which leptin is a prominent member. Leptin receptors are present on Leydig cells and inhibit testosterone synthesis, especially in obese men with high leptin levels. In addition, high insulin levels are positively associated with high leptin levels and may contribute to low TT concentrations in patients with PD. On the other hand, hyperinsulinemia, as encountered in insulin resistance, might impair testosterone secretion directly because there are insulin receptors on the Leydig cells.Citation1,Citation27,Citation28
Patients with T2DM are two times as likely to be depressed when compared with healthy people.Citation29 Depression among those with T2DM is associated with increased diabetes complicationsCitation30 and poor glycemic control.Citation31 The associations between low TT levels and depression, loss of libido, and vigor in men are well understood.Citation32 The Rancho Bernardo StudyCitation33 showed that greater prevalence of depression was associated with lower (~17%) bioavailable testosterone levels. Symptoms of hypogonadism may be also include diminished sexual desire and erectile quality, particularly in nocturnal erections, as well as changes in mood with concomitant decreases in intellectual activity and spatial orientation, fatigue, depression, and anger.Citation34,Citation35 These symptoms are the most common, and studies suggest that testosterone replacement may have an antidepressant effect in depressed patients.Citation36,Citation37
In our study, we showed high prevalence of AS, as well as high severity of andropausal symptoms, in all male patients with PD. However, differences between middle-aged prediabetic patients and healthy peers were greater than that observed between elderly men and healthy men: in the elderly group, only the severity of the psychological symptoms was greater than that observed in healthy peers. Probably, these observations are partially associated with the fact that PD, obesity, and MetS comprise a serious disease with strong and multidirectional influence on endocrine and vascular systems, causing serious sexual and psychological symptoms, particularly disadvantaging the younger population.
Our methodological model has enabled us to investigate potential associations of hormonal milieu, including anabolic androgen deficiencies, with andropausal and depressive symptoms. The results of our study showed that different hormonal mechanisms are involved in the regulation of sexual and psychological status in middle-aged and elderly patients with PD.
It should be noted that in our study, PD was diagnosed also in patients with HbA1c ranging from 5.7% to 6.4%.Citation7 Currently, an intermediate HbA1c range is not considered as PD by the World Health Organization; however, the ADA definition probably indicates a wider range of subjects at risk of T2DM development, and HbA1c of 5.7%–6.4% detects, in part, different individuals with intermediate hyperglycemia, compared with IFG and IGT.Citation38 It should be also emphasized that we did not investigate the severity and prevalence of LOH, which is recognized in patients with symptoms of hypogonadism and low TT or cFT levels.Citation5 We focused only on associations between andropausal and depressive symptoms in patients with PD, as well as the clinical and hormonal risk factors. Our model in no way established a causal link between anabolic hormone deficiency and PD; these conditions might simply overlap and they have probably separate pathophysiologic pathways.
Conclusion
The prevalence and severity of andropausal and depressive symptoms are higher in patients with PD as compared with the same in healthy men. Hormonal determinants of these symptoms are different in middle-aged and elderly patients. Further studies are needed to establish whether androgen replacement therapy would be beneficial in prediabetic men.
Disclosure
The authors report no conflicts of interest in this work.
References
- SaadFGoorenLJThe role of testosterone in the etiology and treatment of obesity, the metabolic syndrome, and diabetes mellitus type 2J Obes20112011110
- FeldmanHALongcopeCDerbyCAAge trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging studyJ Clin Endocrinol Metab200287258959811836290
- TajarAHuhtaniemiITO’NeillTWCharacteristics of androgen deficiency in late-onset hypogonadism: results from the European Male Aging Study (EMAS)J Clin Endocrinol Metab20129751508151622419720
- WuFCTajarABeynonJMIdentification of late-onset hypogonadism in middle-aged and elderly menN Engl J Med2010363212313520554979
- LunenfeldBMskhalayaGKalinchenkoSTischovaTRecommendations on the diagnosis, treatment and monitoring of late-onset hypogonadism in men – a suggested updateAging Male201316414315024188520
- TkaczyszynMNegaKŁopuszańskaMAndropausal syndrome in men with systolic heart failurePol Arch Med Wew20131234156169
- American Diabetes AssociationDiagnosis and classification of diabetes mellitusDiabetes Care201437suppl 1S81S9024357215
- RheeSYWooJTThe prediabetic period: review of clinical aspectsDiabetes Metab J201135210711621738892
- ChoNHWhitingDGuariguataLIDF Diabetes Atlas6th edBelgiumInternational Diabetes Federation20133949
- DhindsaSPrabhakarSSethiMBandyopadhyayAChaudhuriADandonaPFrequent occurrence of hypogonadotropic hypogonadism in type 2 diabetesJ Clin Endocrinol Metab200489115462546815531498
- KapoorDAldredHClarkSChannerKSJonesTHClinical and biochemical assessment of hypogonadism in men with type 2 diabetes: correlations with bioavailable testosterone and visceral adiposityDiabetes Care200730491191717392552
- GavardJALustmanPJClouseREPrevalence of depression in adults with diabetes: an epidemiological evaluationDiabetes Care1993168116711788375247
- RabijewskiMPapierskaLPiątkiewiczPLate-onset hypogonadism among old and middle-aged males with prediabetes in Polish populationAging Male2015181162125657079
- CoronaGRastrelliGBalerciaGHormonal association and sexual dysfunction in patients with impaired fasting glucose: a cross-sectional and longitudinal studyJ Sex Med2012961669168022489756
- HoCHYuHJWangCYPrediabetes is associated with an increased risk of testosterone deficiency, independent of obesity and metabolic syndromePLoS One201389e7417324069277
- AthyrosGVGanotakisESElisafMMikhailidisDOThe prevalence of the metabolic syndrome using the National Cholesterol Educational Program and International Diabetes Federation definitionsCurr Med Res Opin20052181157116416083523
- ZungWWKA cross-cultural survey of symptoms in depressionAm J Psychiatry19691261161215798374
- DaigIHeinemannLAKimSThe aging males’ symptoms (AMS) scale: review of its methodological characteristicsHealth Qual Life Outcomes20031778414675485
- VermeulenAVerdonckLKaufmanJMA critical evaluation of simple methods for the estimation of free testosterone in serumJ Clin Endocrinol Metab199984103666367210523012
- ColangeloLAOuyangPLiuKAssociation of endogenous sex hormones with diabetes and impaired fasting glucose in men: multi-ethnic study of atherosclerosisDiabetes Care20093261049105119289858
- CorralesJJBurgoRMGarca-BerrocalBPartial androgen deficiency in aging type 2 diabetic men and its relationship to glycemic controlMetabolism200453566667215131775
- FukuiMTanakaMTodaHAndropausal symptoms in men with type 2 diabetesDiabet Med20122981036104222248017
- ColaoADi SommaCCascellaTRelationships between serum IGF1 levels, blood pressure, and glucose tolerance: an observational, exploratory study in 404 subjectsEur J Endocrinol2008159438939718603571
- KamedaWDaimonMOizumiTAssociation of decrease in serum dehydroepandrosterone sulfate levels with the progresstion to type 2 diabetes in men of a Japanese population: the Funagata StudyMetabolism200554566967615877298
- CheungKKLukAOSoWYTestosterone level in men with type 2 diabetes mellitus and related metabolic effects: a review of current evidenceJ Diabetes Investig201562112123
- ChandelADhindsaSTopiwalaSChaudhuriADandonaPTestosterone concentration in young patients with diabetesDiabetes Care200831102013201718650372
- StanworthRDJonesTHTestosterone in obesity, metabolic syndrome and type 2 diabetesFront Horm Res200937749019011290
- PitteloudNHardinMDwyerAAIncreasing insulin resistance is associated with a decrease in Leydig cell testosterone secretion in menJ Clin Endocrinol Metab20059052636264115713702
- AndersonRJClouseREFredlandKELustmanPJThe prevalence of comorbid depression in adults with aiabetesDiabetes Care20012461069107811375373
- de GrootMAndersonRFreedlandKEClouseRELustmanPJAssociation of depression and diabetes complications: a meta-analysisPsychosom Med200163461963011485116
- LustmanPJAndersonRJFreedlandKEde GrootMCarneyRMClouseREDepression and poor glycemic control: a meta-analytic review of the literatureDiabetes Care200023793494210895843
- ZitzmannMFaberSNieschlagEAssociation of specific symptoms and metabolic risks with serum testosterone in older menJ Clin Endocrinol Metab200691114335434316926258
- Barrett-ConnorEVon MuhlenDGKritz-SilversteinDBioavailable testosterone and depressed mood in older men: the Rancho Bernardo StudyJ Clin Endocrinol Metab199984257357710022418
- LejeuneHHuygheEDroupySHypoactive sexual desire and testosterone deficiency in menProg Urol201323962162823830256
- JohnsonJMNachtigallLBSternTAThe effect of testosterone levels on mood in men: a reviewPsychosomatics201354650951424016385
- BorstSEYarrowJFFernandezCCognitive effects of testosterone and finasteride administration in older hypogonadal menClin Interv Aging2014121327133325143719
- ZarroufFAArtzSGriffithJSirbuCKommorMTestosterone and depression: systematic review and meta-analysisJ Psychiatr Pract200915428930519625884
- SaukkonenTCederbergHJokelainenJLimited overlap between intermediate hyperglycemia as defined by A1C 5.7%–6.4%, impaired fasting glucose, and impaired glucose toleranceDiabetes Care201134102314231621816975