
Abstract
Background
No epidemiological investigations have previously been conducted in Australia according to the current clinical definitions of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). The aim of this study was to describe sociodemographic and illness characteristics of Australian patients with CFS/ME.
Methods
A cross-sectional survey on the medical history of patients enrolled in an Australian CFS/ME research database between April 2013 and April 2015. Participants were classified according to Fukuda criteria and International Consensus Criteria.
Results
A total of 535 patients diagnosed with CFS/ME by a primary care physician were identified. The mean age of all patients was 46.4 years (standard deviation 12.0); the majority were female (78.61%), Caucasian, and highly educated. Of these, 30.28% met Fukuda criteria. A further 31.96% met both Fukuda criteria and International Consensus Criteria. There were 14.58% reporting chronic fatigue but did not meet criteria for CFS/ME and 23.18% were considered noncases due to exclusionary conditions. Within those meeting CFS/ME criteria, the most common events prior to illness included cold or flu, gastrointestinal illness, and periods of undue stress. Of the 60 symptoms surveyed, fatigue, cognitive, and short-term memory symptoms, headaches, muscle and joint pain, unrefreshed sleep, sensory disturbances, muscle weakness, and intolerance to extremes of temperature were the most commonly occurring symptoms (reported by more than two-thirds of patients). Significant differences in symptom occurrence between Fukuda- and International Consensus Criteria-defined cases were also identified.
Conclusion
This is the first study to summarize sociodemographic and illness characteristics of a cohort of Australian CFS/ME patients. This is vital for identifying potential risk factors and predictors associated with CFS/ME and for guiding decisions regarding health care provision, diagnosis, and management.
Introduction
Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) is a disabling condition that significantly interrupts individuals during critical years of social and economic productivity. The etiology or underlying mechanism of the illness has not been defined, and its diagnosis remains a challenge in the absence of a biological or clinical test. Diagnosis currently relies on differentiating between other diseases and disorders, as well as self-reported symptom-based criteria. It is most often characterized by Fukuda et alCitation1 criteria that include medically unexplained fatigue that may be accompanied by cognitive difficulties, sleep disturbances, and flu-like symptoms. Alternative criteria, such as the International Consensus Criteria (ICC),Citation2 disclose a further range of symptoms pertaining to the neurological, immunological, gastrointestinal, and autonomic systems.
In the UK, Fukuda-defined cases have a prevalence of 0.2%.Citation3 The economic consequence is estimated as GBP120.2 million annually due to lost productivity.Citation4 In the US, the prevalence of Fukuda-defined cases has been reported between 0.2%Citation5 and 0.4%,Citation6 and is estimated to cost USD9.1 billion annually in productivity losses.Citation7 This represents a sizeable economic burden for a select population.
Despite the evidence demonstrating the public health impact abroad, the characteristics of an Australian CFS/ME population have not been summarized. An early study based on a primary care practice survey in the Richmond Valley, a rural district in the state of New South Wales, suggested a prevalence of 0.04%.Citation8 This was based on the author’s case definition that required fatigue of at least 6 months duration, accompanied only by cognitive or short-term memory impairment. This was subsequently estimated to cost AUD59 million annually in both direct health care costs and indirect costs regarding lost productivity.Citation9 In contrast to current case definitions, this study described cognitive disturbance as the hallmark of the illness. On the contrary, the Fukuda and more recent ICC case definitions emphasize the role of postexertional fatigue and describe a multisystem disorder. As a result, the attributes described in the Richmond Valley study may be representative of a significantly different clinical profile. Hence, studies that characterize Australian samples are not available and the Royal Australasian College of Physicians guidelines for clinical practice include limited evidence from Australian-based cohorts.Citation10
The aim of this study was to summarize sociodemographic and illness characteristics in those reporting CFS/ME symptoms according to current case definitions in Australia. A better understanding of these characteristics is important for detecting potential risk factors and predictors associated with CFS/ME and for health care provision. These findings are presented according to guidelines for strengthening the reporting of observational studies in epidemiology.Citation11
Methods
Setting
This cross-sectional study utilized responses to a survey during a 2-year period from April 2013 and April 2015. The survey was delivered to volunteers during their enrollment into a research database for CFS/ME managed by the National Centre for Neuroimmunology and Emerging Diseases within Griffith University. This database serves as a sampling pool for immunological and clinical research on CFS/ME as well as provides a cohort available for longitudinal follow-up. It commenced following approval from Griffith University Human Research Ethics Committee (HREC reference number MSC0413).
Participants
Recruitment was based on self-identification in response to an advertisement in CFS/ME community support networks across Australia, as well as a general advertisement on local radio and social media. Upon contacting the research center, those interested in enrolling in the research database received an information pack and informed consent was obtained by agreeing to terms and conditions disclosed online or signing a hard copy sent in the mail. To be eligible for this study, participants were required to 1) report a diagnosis of CFS/ME by their primary physician, 2) be between 18 and 65 years of age, and 3) a resident of Australia.
As recruitment relied on self-identification, it is unknown whether there was a difference between responders and non-responders in this study. Rather than aim for a comprehensive population-based screening at this stage, the methods of this study enabled us to summarize potential cases of CFS/ME present in the Australian community.
Survey
Participants completed a self-report survey regarding their medical history. This was made available through an online link or by hard copy in the mail. Items in the study questionnaire were developed by the authors, and participants were asked to disclose sociodemographic details, medical history, and complete a 60-item checklist on their fatigue and concurrent symptoms. Responses were collected using an online survey application known as LimeSurvey (Carsten Schmitz, Hamberg, Germany),Citation12 and stored on a secure server hosted by Griffith University. Data from hard copy versions of the study questionnaire returned to the research center by mail were subsequently entered into the LimeSurvey application by a member of the research team to consolidate all responses. All personal data were encrypted to remove the identity of participants.
Case ascertainment
The disclosed medical history of participants was reviewed by the authors to exclude any potential diagnoses or conditions that may be an alternative explanation for symptoms. This included, but was not limited to, major heart disease, neurological disorders such as multiple sclerosis, autoimmune disease such as rheumatoid arthritis and diabetes, and thyroid disorders. These exclusionary conditions were reviewed by an author of the study who has extensive clinical experience with CFS/ME. If reported, these participants were classified as noncases.
To be reported as a case of CFS/ME, reported symptoms had to comply with study criteria for fatigue and accompanying symptoms according to the Fukuda and/or ICC definitions that are outlined in . For this study, fatigue must have been present for at least 6 months. Patients accompanying symptoms should not have preceded the onset of fatigue and also be persistent or recurring for at least 6 months. The study reported the presence of postexertional malaise and postexertional neuroimmune exhaustion. To meet criteria for postexertional neuroimmune exhaustion, patients must have reported experiencing all of the following after minimal activity: 1) marked postexertional fatigue, 2) postexertional symptom exacerbation, 3) onset of fatigue can be immediate or delayed, 4) prolonged recovery period of usually 24 hours or longer, and 5) lack of stamina (substantial reduction in premorbid activities).
Table 1 Summary of symptom criteria for CFS/ME
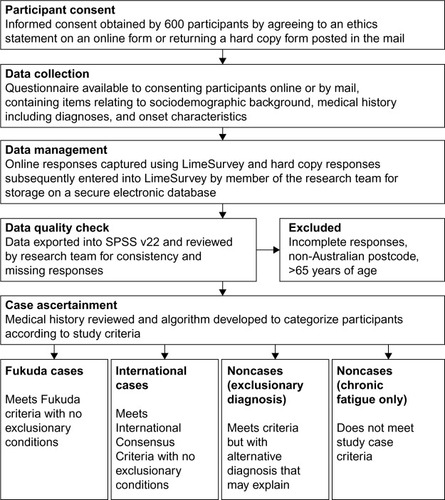
It was observed that participants could be placed in three categories. Fukuda cases were participants who reported symptoms that only fulfilled Fukuda criteria and not the ICC. ICC cases fulfilled both the Fukuda and ICC criteria but for the purposes of comparison were referred to as ICC cases in this study. There was an exception of four participants who only met ICC, but were excluded from analysis due to lack of statistical power. The remainder of participants reported chronic fatigue (CF) for at least 6 months but did not meet either CFS/ME criteria due to lack of accompanying symptoms. These were considered atypical and reported as cases of CF (). Hence, the primary outcome of interest included the frequency of Fukuda cases, ICC cases, CF cases, and noncases.
Figure 1 Flowchart for case ascertainment.
Study variables
Sociodemographic data included location of residency, age, sex, body mass index (BMI), ethnicity, education, and employment. Postcodes were used to verify Australian residency and classified according to the Australian Bureau of Statistics (ABS) Australian Standard Geographical Classification definition for urban and rural areas.Citation13 This classifies populations of 100,000 or more as major urban areas, 1,000–99,999 as other urban, and remaining postcodes as rural. The distribution of participants in the registry was examined per state and reported together with the distribution of the Australian population per state, according to the ABS Australian demographic statistics for June quarter 2015.Citation14
BMI was classified according to the World Health OrganizationCitation15 global database on BMI. Accordingly, underweight was considered <18.5 kg/m2, normal 18.5–24.9 kg/m2, overweight 25.0–29.9 kg/m2, and obese ≥30.0 kg/m2. With regard to ethnicity, participants were classified according the ABS Australian classification for cultural and ethnic groups.Citation16 This included nonindigenous Australian, indigenous Australian, Oceanian (New Zealand, Melanesian, Papuan, Micronesian, and Polynesian), North West European, Southern and Eastern European, North African and Middle Eastern, South East Asian, North East Asian, Southern and Central Asian, People of the Americas, and Sub-Saharan African. Participant education was categorized according to the highest level of education completed. In terms of employment, full-time hours were defined as 35 hours per week or more and part-time hours were considered <35 hours per week in accordance with the ABS Labour Force Survey.Citation17 Participants were further classified as those on disability pension, retired, and unemployed.
Outcomes of interest regarding onset of illness included age of onset (age since first experienced symptoms), age of diagnosis by a primary care physician, and duration of illness (time in years elapsed since onset of illness). Furthermore, participants were asked to identify residency during onset by state within Australia and by country if overseas. Participants were asked whether their symptoms had a sudden or gradual onset. The study also surveyed infectious and noninfectious events and exposures that participants associated with prior to their illness suggested by the ICC Consensus Primer for Medical Practitioners.Citation18
Statistical analysis
The study includes descriptive statistics of the aforementioned characteristics. Pearson’s chi-squared analysis was used to compare the frequency of symptoms between Fukuda-and ICC-defined cases with significance set at P<0.05 using SPSS v22 (IBM Corporation, Armonk, NY, USA).Citation19
Result
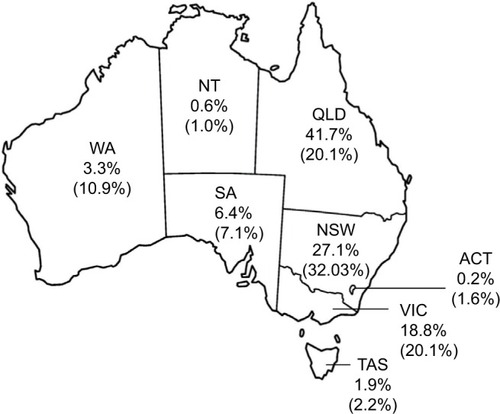
Of 600 respondents, a total of 535 participants met the inclusion criteria. presents the distribution of participants per state as well as the distribution of the Australian population per state for comparison. The majority of participants were from Queensland, followed by New South Wales, and Victoria and 91.89% had postcodes corresponding to major urban regions of Australia.
Figure 2 Frequency of participants in the CFS/ME registry by state.
Abbreviations: ACT, Australian Capital Territory; CFS/ME, chronic fatigue syndrome/myalgic encephalomyelitis; NT, Northern Territory; NSW, New South Wales; QLD, Queensland; TAS, Tasmania; VIC, Victoria; SA, South Australia; WA, Western Australia.
Of 535 individuals assessed, CFS/ME as characterized by the Fukuda criteria was evident in 30.3%. A further 32.0% met both Fukuda criteria and the ICC and referred to as ICC-defined cases for comparison. In all, 23.2% were classified as CF, as they met criteria for CF but did not report sufficient symptoms to meet the Fukuda or ICC definitions. The remaining 14.6% reported an alternative physical or psychological diagnosis that accounted for their symptom profile and were thus classified as noncases.
The sociodemographic characteristics of Fukuda cases, ICC cases, CF, and noncases are summarized in . In total, the highest proportion of participants were non-indigenous Australian (total 74.4%), female (total 78.6%), with a mean age of 46.4 years (standard deviation 12.0). A total of 47.5% of participants were within a normal range for BMI. A higher proportion of individuals had completed either undergraduate (27.9%) or postgraduate (18.1%) university degrees. The majority of participants were on disability pension (34.2%) or unemployed (26.7%), while the lowest proportion maintained full-time roles (9.7%). The distribution of the aforementioned characteristics was similar between study groups.
Table 2 Sample demographic characteristics
summarizes the onset characteristics of Fukuda, ICC, and CF cases. The mean age of illness onset for Fukuda (P=0.030)- and ICC (P<0.001)-defined cases was significantly younger in comparison to CF. Across all groups, the highest proportion of cases originated in Queensland. More than 5% of cases across all groups originated overseas. The most common reported infectious events were cold and flu, upper respiratory infections, and gastrointestinal illness. Furthermore, the most common noninfectious trigger reported was periods of undue stress.
Table 3 Sample onset characteristics for CFS/ME and CF cases
Reported symptoms of Fukuda, ICC, and CF cases are included in . The most common symptoms reported by more than two-thirds of both Fukuda- and ICC-defined cases included fatigue; cognitive overload; difficulty making decisions; short-term memory problems; headaches; muscle pain; joint pain; unrefreshed sleep; sensitivities to light, noise, vibration, odors, taste, and/or touch; light headedness; and intolerances to extremes of temperature. A significantly higher proportion of ICC-defined cases reported postexertional neuroimmune exhaustion, postexertional malaise, disorientation, slowed speech, abdominal pain, reversed sleep cycles, vivid dreams or nightmares, sensitivities, poor depth perception, feeling unsteady on their feet, sore throat, food intolerances, urinary disturbances, light headedness, abnormal body temperature, recurrent feverishness, and cold extremities.
Table 4 Frequency of reported symptoms for CFS/ME and CF cases
Discussion
This study was performed to review the sociodemographic and illness characteristics of CFS/ME patients within Australia. The key findings of this study include 1) the frequency of Fukuda-, ICC-, and CF-defined cases; 2) sociodemographic characteristics that have not been previously reported in an Australian sample according to current definitions of CFS/ME; 3) the average age of onset, diagnosis, and common infectious and noninfectious events prior to onset; and 4) a high frequency of varied symptoms experienced by patients and significant differences between Fukuda- and ICC-defined patient sets.
Case ascertainment
In this study, 62.2% of our participants reported symptoms that met Fukuda diagnostic criteria without exclusionary conditions. Of these, approximately half also fulfilled the ICC definition. This supports previous findings that ICC-defined cases represent a subgroup within the broad spectrum of Fukuda-defined CFS/ME.Citation20,Citation21 Accordingly, it has been demonstrated that ICC-defined cases have reported decreased physical and social functioning in comparison to Fukuda-defined cases.Citation20,Citation21 A significant proportion (24.1%) of participants in this study reporting a diagnosis of CFS/ME were not considered cases due to concurrent conditions that would explain their symptoms. This finding is highly consistent with the UK prevalence study, in which 24% of general practitioner-diagnosed cases did not fulfill their study criteria for CFS/ME using similar methods of case ascertainment.Citation3
In the absence of a reliable diagnostic test, CFS/ME remains a challenging diagnosis and illness to identify. General practitioners’ attitudes toward CFS/ME are diverse regarding their opinions and management of CFS/ME.Citation22–Citation24 Indeed, the significant variability found between case definitions for CFS/ME is an immediate cause of confusion for clinicians and researchers alike.Citation25 Further reasons include limited knowledge, lack of recognition for the disorder, and limited contact with CFS/ME patients who do not access care due to the severity of their condition as well as their low expectations for receiving adequate care and support.Citation26
Sociodemographic characteristics
The findings of our study suggest the CFS/ME predominantly affects those between 45 and 55 years; however, the range in our cohort extended from 18 to 65 years and thus CFS/ME was not exclusive to any age set. The profiles of patients in this study are similar to early US studies on the primary care prevalence on CFS/ME led by the Centers for Disease Control and Prevention in that the majority of participants were Caucasian females and highly educated.Citation27 A higher ratio of females is commonly reported within CFS/ME;Citation6,Citation8,Citation28 however, it has been suggested that females are more likely to access all levels of health services than males.Citation29 While the majority of participants in this study identified as nonindigenous Australians, community-based studies in the US suggest that the prevalence of CFS/ME may actually be higher among their minority populations; for example, rates have been reported as higher among African-Americans and Latinos in comparison to Caucasians.Citation6
As a cross-sectional study, it cannot be determined whether weight and obesity were significant predictors for CFS/ME or the reverse. However, a high proportion of Fukuda and ICC cases were considered overweight or obese (41.3% and 43.3%, respectively). This is considerably less than previously reported in a US Fukuda-defined sample with 75%. Though this was a population-based sample, these patients were required to meet further criteria for sleep disturbance that may have been more obese than those not meeting this additional criterion. In a Dutch survey, CFS participants were more likely to be obese (odds ratio =4.1) in comparison to nonfatigued participants.Citation30 This could be associated with the debilitating and chronic nature of the illness that may result in significantly decreased mobility as severe cases are often housebound or bedridden. Accordingly, overweight and obese individuals with CFS/ME have demonstrated significantly poorer physical functioning than controls of similar weight.Citation31
The functional impact of the illness is also evident in the significantly high proportion of individuals who are unemployed, on disability pension, or maintain part-time roles. This is of particular concern considering many are still in the most economically and socially productive years of their lives and, thus, represents significant economic losses at both the population and patient level. This reduced economic position adds further to the stress, anxiety, or depression that may develop with a chronic condition, particularly in those patients who are bedridden or housebound for protracted periods of time and receive limited support.
Illness characteristics
The peak onset of CFS/ME was relatively young in this sample between the ages of 25 and 35 years. The majority of cases also identified having a sudden onset to their symptoms (59.3% and 64.9% for Fukuda- and ICC-defined cases, respectively) compared to a gradual onset. In a natural history study, patients with a sudden onset reported a high frequency of symptoms compared to those with a gradual onset.Citation32 The largest proportion of both Fukuda- and ICC-defined cases (more than 40%) identified infectious events prior to the onset of their fatigue, such as respiratory infections including cold, flu, sinusitis, and pneumonia. Gastrointestinal illness was the second most common (Fukuda 15.4%; ICC 28.7%, respectively). Further, a considerable number of cases began overseas as a result of an unknown infection (Fukuda 6.8%; ICC 11.1%). Though this study did not identify specific infections, an Australian prospective cohort study found that 11% of those who acquired an acute infection of Epstein–Barr virus (glandular fever), Coxiella burnetii (Q fever), or Ross River virus (epidemic polyarthritis) went on to fulfill Fukuda et alCitation1 symptom criteria.Citation33 With regard to noninfectious events prior to illness, periods of undue stress was the most common (Fukuda 48.2%; ICC 46.2%). It was common for cases to report experiencing both an infection as well as significant periods of undue stress. This does align with the proposed pathophysiology that CFS/ME presents as a multi-system disorder involving interactions between the immune and central nervous system, and that stress may potentially reactivate or replicate a latent virus, such as Epstein–Barr developing symptoms of CFS/ME.Citation34
This study identified the most common symptoms reported by patients representing Fukuda- and ICC-defined cases. Cognitive issues such as difficulty processing information, muscle pain and muscle weakness, sleep disturbances, and sensitivities to light, noise, vibration, odor, and/or touch in particular were the most common issues reported by more than two-thirds of both Fukuda- and ICC-defined cases. Food intolerances, urinary disturbances, and intolerance of extreme temperature were also highly prevalent among ICC-defined cases (more than two-thirds) and could be considered distinguishing features in comparison to Fukuda-defined cases.
Limitations and recommendations
The results of this study may not be representative of all CFS/ME patients in the general population given that the sample was not from a community-based survey. As this study summarized patients who are currently experiencing illness, those who consider themselves recovered are not represented by this study. Such a sample may exhibit different illness characteristics that have not been well summarized in the literature. Due to the cross-sectional design of this study, it is also not known whether participants who were not considered cases of CFS/ME developed exclusionary conditions after an initial diagnosis of CFS/ME by a physician. As such, reporting on improvement, recovery, and development of other conditions will be a future aim as this cohort become available longitudinally.
Limitations
A limitation is reliance on reported symptoms for case ascertainment; however, the methods of this study remain important as an initial screening tool to identify cases of CFS/ME. Methods such as the recruitment of patients from general practitioner databases may not have been as successful as self-identification of a largely unrecognized and misdiagnosed condition. Furthermore, contrary to typical patterns of chronic disease where the most severe cases present to primary care, severe cases of CFS/ME may be less likely to present to primary care due to being bedridden. Further, a consultation with a primary care professional is limited as there currently remains no successful therapy for the illness.
This information is intended to guide decision makers and clinicians on what patient and illness characteristics may be expected when potential cases of CFS/ME arise. To improve understanding on the prognosis of CFS/ME, future directions aim to follow-up those patients recruited in this study longitudinally as a prospective cohort. This will capture not only changes in employment status but also the pattern of symptomatology. Symptom severity and the functional impact of the illness will also be monitored. The alignment of this clinical severity with laboratory findings will be particularly valuable for identifying potential biological markers and the etiology or pathomechanism behind this illness.
Conclusion
This study has identified a significant cohort of Australians who fulfill CFS/ME definitions having substantially low rates of full-time employment and in high need of improved health care support. Respiratory infections and gastrointestinal illness, as well as periods of undue stress, were common events prior to the onset of their illness. Those meeting the ICC definition further appear to represent a distinct clinical group with distinguishing symptoms. The improved characterization of Australian CFS/ME will help guide decisions in diagnosis, management, and health service provision.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by the Alison Hunter Memorial Foundation, Change for ME, Mason Foundation, the Stafford Fox Medical Research Foundation, the Edward P Evans Foundation, and the Queensland Government Co-Investment Program.
Disclosure
The authors report no conflicts of interest in this work.
References
- FukudaKStrausSEHickieISharpeMCDobbinsJGKomaroffAThe chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study GroupAnn Intern Med1994121129539597978722
- CarruthersBMvan de SandeMIDe MeirleirKLMyalgic encephalomyelitis: International Consensus CriteriaJ Intern Med2011270432733821777306
- NaculLCLacerdaEMPhebyDPrevalence of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) in three regions of England: a repeated cross-sectional study in primary careBMC Med201199121794183
- CollinSMCrawleyEMayMTSterneJAHollingworthWUK CFS/ME National Outcomes Database. The impact of CFS/ME on employment and productivity in the UK: a cross-sectional study based on the CFS/ME national outcomes databaseBMC Health Serv Res201111121721923897
- ReyesMNisenbaumRHoaglinDCPrevalence and incidence of chronic fatigue syndrome in Wichita, KansasArch Intern Med2003163131530153612860574
- JasonLARichmanJARademakerAWA community-based study of chronic fatigue syndromeArch Intern Med1999159182129213710527290
- ReynoldsKJVernonSDBoucheryEReevesWCThe economic impact of chronic fatigue syndromeCost Eff Resour Alloc200421415210053
- LloydARHickieIBoughtonCRSpencerOWakefieldDPrevalence of chronic fatigue syndrome in an Australian populationMed J Aust199015395225282233474
- LloydARPenderHThe economic impact of chronic fatigue syndromeMed J Aust199215795996011406420
- Working Group of the Royal Australasian College of PhysiciansChronic fatigue syndrome clinical practice guidelinesMed J Aust2002176S2312056987
- VandenbrouckeJPvon ElmEAltmanDGStrengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaborationAnn Intern MedOct 1620071478W16319417938389
- LimeSurvey: An Open Source Survey Tool [computer program]2012CarstenSchmitzHamberg, Germany
- Australian Bureau of StatisticsAustralian Statistical Geography Standard: Significant Urban Areas, Urban Centres and LocalitiesCanberraAustralian Government2012
- Australian Bureau of StatisticsAustralian Demographic StatisticsCanberraAustralian Government2015
- World Health OrganizationGlobal Database on Body Mass Index2006 Available from: http://apps.who.int/bmi/index.jsp?introPage=intro_3.htmlAccessed August 24, 2015
- Australian Bureau of StatisticsAustralian Standard Classification of Cultural and Ethnic GroupsCanberraAustralian Government2011
- Australian Bureau of StatisticsLabour Force Commentary92013CanberraAustralian Government2013
- CarruthersBMvan de SandeMDe MeirleirKMyalgic Encephalomyelitis – Adult & Paediatric: International Consensus Primer for Medical PractitionersCanadaCarruthers & van de Sande2012
- IBM Statistics Package for Social Sciences for Windows Version 220 [computer program]Armonk, NYIBM Corp2013
- BrownAAJasonLAEvansMAFloresSContrasting case definitions: The ME International Consensus Criteria vs. the Fukuda et al. CFS CriteriaN Am J Psychol201315110312025364305
- JohnstonSCBrenuEWHardcastleSLHuthTKStainesDRMarshall-GradisnikSMA comparison of health status in patients meeting alternative definitions for chronic fatigue syndrome/myalgic encephalomyelitisHealth Qual Life Outcomes2014126424886213
- StevenIDMcGrathBQureshiFWongCChernIPearn-RoweBGeneral practitioners’ beliefs, attitudes and reported actions towards chronic fatigue syndromeAust Fam Physician2000291808510721550
- BowenJPhebyDCharlettAMcNultyCChronic fatigue syndrome: a survey of GPs’ attitudes and knowledgeFam Pract200522438939315805128
- RaineRCarterSSenskyTBlackNGeneral practitioners’ perceptions of chronic fatigue syndrome and beliefs about its management, compared with irritable bowel syndrome: qualitative studyBMJ200432874521354135715169743
- JohnstonSCBrenuEWStainesDRMarshall-GradisnikSMThe role of clinical guidelines for chronic fatigue syndrome/myalgic encephalomyelitis in research settingsFatigue201422839
- DrachlerMLLeiteJCHooperLThe expressed needs of people with chronic fatigue syndrome/myalgic encephalomyelitis: a systematic reviewBMC Public Health20099145820003363
- ReyesMGaryHEJrDobbinsJGSurveillance for chronic fatigue syndrome – four U.S. cities, September 1989 through August 1993MMWR CDC Surveill Summ199746211312412768
- LawrieSMPelosiAJChronic fatigue syndrome in the community. Prevalence and associationsBr J Psychiatry199516667937977663830
- GaldasPMCheaterFMarshallPMen and health help seeking behaviour: literature reviewJ Adv Nurs200549661662315737222
- van’t LevenMZielhuisGAvan der MeerJWVerbeekALBleijenbergGFatigue and chronic fatigue syndrome-like complaints in the general populationEur J Pub Health201020325125719689970
- FloresSBrownAAdeoyeSJasonLAEvansMExamining the impact of obesity on individuals with chronic fatigue syndromeWorkplace Health Saf201361729930723799656
- ReyesMDobbinsJGNisenbaumRSubedarNSRandallBReevesWCChronic fatigue syndrome progression and self-defined recovery: evidence from the CDC surveillance systemJ Chronic Fatigue Syndr1999511727
- HickieIDavenportTWakefieldDPost-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort studyBMJ2006333756857516950834
- GlaserRKiecolt-GlaserJKStress-associated immune modulation: relevance to viral infections and chronic fatigue syndromeAm J Med1998105335S42S9790480