
Abstract
Background
Chronic obstructive pulmonary disease (COPD) and farming are two conditions that have been associated with an increased risk of anxiety and depression. Dairy farming is an independent risk factor for COPD.
Objective
To test the hypotheses that the prevalence of anxiety and/or depression is higher in dairy farmers with COPD than in farmers without COPD, and higher in dairy farmers with COPD than in non-farmers with COPD.
Methods
Anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale in 100 dairy farmers with COPD (DF-COPD), 98 dairy farmers without COPD (DF-controls), 85 non-farming patients with COPD (NF-COPD) and 89 non-farming subjects without COPD (NF-controls), all identified by screening in the Franche-Comté region of France. Anxiety and depression were considered present when the Hospital Anxiety and Depression Scale score was ≥8. COPD was defined by a post-bronchodilator forced expiratory volume in 1 second/forced vital capacity ratio <0.7.
Results
The crude prevalence of anxiety did not differ between the four groups, ranging from 36% in NF-controls to 47% in NF-COPD (p=0.15 between groups). Similarly, the prevalence of depression did not differ significantly between the four groups (p=0.16 between groups). In dairy farmers (n=198), the only factors associated with anxiety were quality of life and current smoking. Depression in dairy farmers was associated with airflow limitation (lower forced expiratory volume in 1 second and COPD grade 2 or more) as well as with some COPD-related features (dyspnea severity, current smoking, and poorer quality of life). In non-farmers, both anxiety and depression were associated with airflow limitation and COPD-related features.
Conclusion
In our population, the prevalence of anxiety and/or depression was similar in dairy farmers with and without COPD and in non-farmers with COPD. Nevertheless, the degree of airway obstruction and some COPD-related features were associated with depression among dairy farmers, whereas these factors were not associated with anxiety.
Introduction
Chronic obstructive pulmonary disease (COPD) is currently the most common respiratory disease, affecting between 5% and 10% of subjects over 40 years of age.Citation1 This disease leads to a deterioration of the patient’s quality of lifeCitation2,Citation3 and involves considerable costs due to health care, professional absenteeism and morbidity–mortality.Citation4 COPD primarily affects the lungs, but also has consequences on other organs and functions.Citation5 Anxiety and depression are among the most frequent comorbidities identified in COPD patients.Citation6–Citation8 The causal relationships between COPD and anxiety and/or depression are multifaceted.Citation9,Citation10 Patients with COPD are more likely to develop anxiety and/or depression than control subjects, while COPD patients with anxiety and/or depression have a higher risk of COPD-related mortality than COPD patients without anxiety and/or depression.Citation10,Citation11
Although the main causal risk factor for COPD in developed countries is tobacco smoking, COPD is also attributable to environmental and/or professional exposures.Citation12,Citation13 COPD in dairy farmers is, in this regard, a typical example of COPD attributable to exposure to organic dusts at work.Citation14 A recent study showed that COPD prevalence among farmers is approximately twice as high as in subjects with no occupational exposure.Citation15 Many studies have shown that farming may be associated with an increased risk of anxiety and depression.Citation16–Citation19 This could partly be explained by the fact that in some cases, farmers are daily subjected to multiple stress factors such as economic circumstances, weather conditions, labor problems and social conditions.Citation16,Citation19,Citation20 Nevertheless, the prevalence of anxiety and depression among farmers with COPD is currently unknown.
Given that COPD and dairy farming may both be risk factors for anxiety and/or depression, we aimed to test the hypothesis that a higher prevalence of anxiety and/or depression exists in farmers with COPD than in farmers without COPD, together with a higher prevalence of anxiety and/or depression in farmers with COPD than in non-farmers with COPD. We also aimed to study the relationship between anxiety and/or depression and selected COPD-related features in farmers and in non-farmers. To achieve this aim, we assessed anxiety and depression by the self-administered Hospital Anxiety and Depression Scale (HADS) in four groups of subjects: dairy farmers with and without COPD, as well as non-farmers with and without COPD, all identified by screening.
Subjects and methods
Screening programs
Data for this study were collected as part of the BALISTIC project (COPD in dairy farmers: screening, characterization and constitution of a cohort; ClinicalTrials.gov Identifier: NCT2540408) which was conducted from 2011 to 2015 at the University Hospital of Besançon in collaboration with the French national social security system for agricultural workers (Mutualité Sociale Agricole [MSA]) and the federation of community health practices of Franche-Comté (Fédération des Maisons de Santé Comtoises). This study was set up primarily to assess the prevalence and some specific characteristics of COPD in dairy farmers (COPD secondary to organic dust exposure) in comparison with COPD in patients without any occupational exposure and with matched controls without COPD.Citation21
COPD patients and matched controls were recruited through two parallel screening programs (screening phase of the BALISTIC study). Inclusion criteria in the screening programs were: men or women aged between 40 and 74 years, with no history of chronic respiratory disease including asthma and COPD or related conditions (chronic bronchitis, emphysema), and either being a dairy farmer (dairy farmer subgroups) or not being exposed to any occupational hazard associated with COPD (non-farmer subgroups). One of these two programs was conducted during free health checkups organized by the MSA for their affiliated members; COPD screening was proposed to all invited subjects who attended the health checkup and who fulfilled the inclusion criteria. In parallel, general practitioners of the Fédération des Maisons de Santé Comtoises conducted a second program whereby they invited all their patients who met the inclusion criteria to take part in the COPD screening program.
For screening, spirometry was performed as previously described.Citation15 Spirometry outcomes included forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC). A bronchodilation test was performed when the FEV1/FVC ratio was <0.70.Citation22 Predicted values were based on the European Coal and Steel Community equations.Citation23
Study groups
A diagnosis of COPD was retained when the FEV1/FVC ratio post-bronchodilator was <0.70. COPD patients were rated as either grade 1 (FEV1 >80% of the predicted value) or grade 2 or more (FEV1 ≤80% of the predicted value). Spirometry was considered normal when the FEV1/FVC ratio was >0.70 and FEV1 was >80% of the predicted value before bronchodilator administration.
During the study period, all subjects with COPD detected during the screening phase of the BALISTIC study were invited to participate in the characterization phase of the study. Those who agreed to participate in the characterization phase were included in two subgroups, namely, dairy farmers with COPD (DF-COPD) and non-farmers with COPD (NF-COPD). An equivalent number of subjects with normal spirometry (as defined above) who had participated in the screening phase of the study were frequency matched with the COPD subjects in terms of age, body mass index (BMI), tobacco smoking (in pack-years) and gender. These subjects with normal spirometry made up two additional subgroups, namely, dairy farmers without COPD (DF-controls) and non-dairy farmers without COPD (NF-controls).
Subjects from these four subgroups underwent a characterization visit at the University Hospital of Besançon, during which examinations were performed and questionnaires were administered, as described in detail elsewhere.Citation21 The distribution of the study population is detailed in .
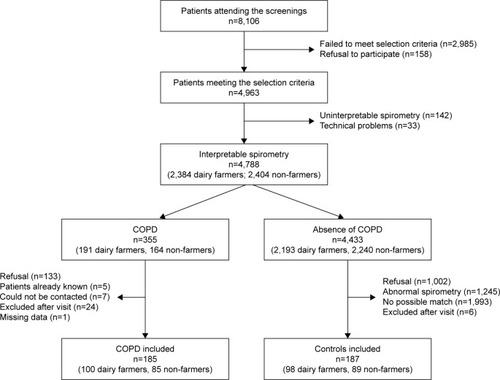
Figure 1 Flowchart of the population.
Ethical approval was received from the local Ethics Committee (Comité de Protection des Personnes Est; authorization 11/617). All participants were informed of the study procedures, and written consent was obtained from all included subjects.
Questionnaires
During the characterization visit, several standardized questionnaires were administered to the four participating subgroups.
A medical questionnaire (completed by the physician) collected data on anthropometric and demographic characteristics, symptoms and smoking history. Each patient was asked about their history of exacerbation, sputum and allergies. Dyspnea was assessed using two scales, namely, the Baseline Dyspnea Index (BDI) and the modified Medical Research Council scale (mMRC). A 6-minute walk test was performed to calculate the BMI, airflow Obstruction, Dyspnea and Exercise capacity (BODE) index. This score combines BMI, FEV1, mMRC and 6-minute walk test.Citation24 Smoking status was recorded and the number of pack-years was calculated. Subjects who smoked on average less than one cigarette (or cigar or pipe) a day for a year were categorized as never-smokers. If the amount smoked was higher than this value, patients were considered as current smokers. Subjects who had stopped smoking for at least 1 month were considered as former smokers.
Patients completed the self-administered HADS to assess anxiety and depression. The HADS is composed of 14 questions, 7 for the anxiety subscale and 7 for the depression subscale. Each question has four responses rated on a scale of 0–3, with a maximum score of 21 for each subscale (indicating a high level of distress). For each subscale, a score of 0–7 corresponds to an absence of symptoms of anxiety and/or depression, a score between 8 and 11 corresponds to borderline symptoms of anxiety and/or depression and a score >11 corresponds to the certain presence of symptoms of anxiety and/or depression.Citation17,Citation25,Citation26
Quality of life was assessed by the St George’s Respiratory Questionnaire (SGRQ). The SGRQ is a questionnaire of 50 items designed to measure the quality of life in patients with obstructive lung disease. A high score indicates a significant impairment of quality of life.Citation27 It is assumed that a difference of 4 points in the SGRQ is clinically relevant to differentiate groups of subjects.Citation28
Statistical analysis
Data are presented as number (percent) and mean ± standard deviation for qualitative and quantitative variables, respectively.
Anxiety and depression variables were dichotomized with a cutoff at 8 for absence of anxiety or depression symptoms vs possible/certain presence of anxiety or depression symptoms.Citation17,Citation25,Citation26 Hereinafter, these two conditions are designated as absence and presence of anxiety and depression, for simplification.
Characteristics of COPD and control subjects, stratified by professional status (dairy farmers vs non-farmers), were compared using Student’s t-test and chi-square test for quantitative and qualitative variables, respectively. Characteristics of DF-COPD and NF-COPD subjects were compared using the same methodology.
The prevalence of anxiety and depression was compared in the four groups using the chi-square test. Logistic regressions adjusted for post-bronchodilator FEV1 (% predicted value) were performed to compare the prevalence of anxiety between dairy farmers and non-farmers. The same methodology was used to compare the prevalence of depression between dairy farmers and non-farmers.
To identify factors associated with anxiety among dairy farmers and non-farmers, bivariate logistic regressions for all candidate factors were performed. Odds ratios (ORs) were presented using forest plots. The same methodology was used to identify factors associated with depression.
A p-value <0.05 was considered statistically significant. Analyses were performed using SAS software (version 9.3; SAS Institute, Inc., Cary, NC, USA).
Results
Population characteristics
Among the 8,106 subjects who underwent screening, 4,963 met the inclusion criteria for the study (61.2%). In total, 355 patients with COPD (191 dairy farmers and 164 non-farmers) were identified (7.4% of all subjects with interpretable spirometry) and 4,433 had normal spirometry. A total of 210 COPD patients and 193 non-COPD matched controls agreed to participate in the characterization phase of the study. Thirty patients were excluded, mainly owing to a history of asthma or occupational exposure other than dairy farming (). In addition, one DF-COPD patient was not included in this analysis because of missing HADS data. Finally, the DF-COPD, DF-controls, NF-COPD and NF-controls groups comprised 100, 98, 85 and 89 patients, respectively ( and ).
Table 1 Population characteristics
The DF-COPD and NF-COPD subgroups were composed mainly of mild COPD with preserved FEV1 (). The number of current smokers and former smokers was lower among farmers than among non-farmers (). The proportion of men was higher among farmers than among non-farmers. Dyspnea was more frequent and quality of life scores were lower among COPD patients than among control subjects without COPD ().
Prevalence of anxiety and depression
The crude prevalence of anxiety (HADS-anxiety subscale score ≥8, indicating possible/probable symptoms of anxiety) was similar in the four subgroups. Neither COPD nor dairy farming was associated with an increased frequency of anxiety ().
Figure 2 Prevalence of anxiety and depression among dairy farmers with COPD (DF-COPD), dairy farmers without COPD (DF-controls), non-farmers with COPD (NF-COPD) and non-farmers without COPD (NF-controls). ORs are adjusted (adjOR) on FEV1 post-bronchodilator.
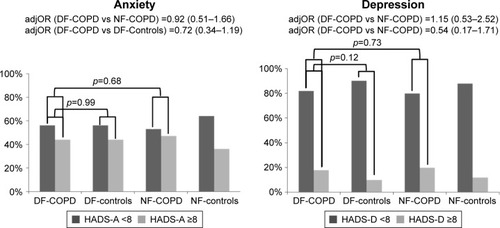
Similarly, the prevalence of depression (HADS-depression subscale score ≥8, indicating possible/probable depression) was similar in the four subgroups ().
Factors associated with anxiety and depression
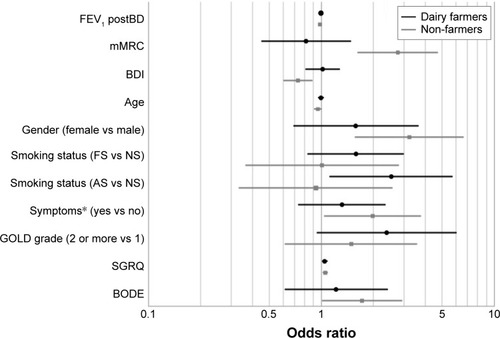
Among farmers, anxiety was associated with current smoking (OR: 2.53 [1.12–5.70], p=0.03) and with poorer quality of life as measured by the SGRQ score (OR: 1.05 [1.02–1.08], p=0.003), which is shown in . Among non-farmers, anxiety was associated with lower FEV1 (OR: 0.98 [0.97–0.99], p=0.03), more severe dyspnea (higher mMRC score [OR: 2.76 {1.62–4.69}] and lower BDI [OR: 0.73 {0.61–0.89}], p<0.001 for both), female gender (OR: 3.23 [1.58–6.60], p=0.001), younger age (OR: 0.95 [0.91–0.99], p=0.03), presence of COPD-related symptoms (OR: 1.98 [1.05–3.74], p=0.04), lower quality of life as evaluated by the SGRQ (OR: 1.06 [1.03–1.08], p<0.001) and higher BODE score (OR: 1.72 [1.02–2.91], p=0.04).
Figure 3 Factors associated with anxiety among dairy farmers and non-farmers.
Abbreviations: AS, active smoker; BDI, Baseline Dyspnea Index; BODE, Body mass index, airflow Obstruction, Dyspnea and Exercise capacity index; FEV1 post-BD, forced expiratory volume in 1 second post-bronchodilator; FS, former smoker; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, modified Medical Research Council scale; NS, non-smoker; SGRQ, St George’s Respiratory Questionnaire.
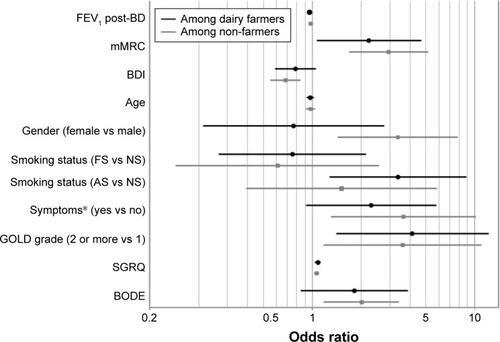
Depression among dairy farmers was associated with lower FEV1 (OR: 0.96 [0.94–0.98], p<0.001), more severe COPD grades, that is, grade 2 or more (OR: 4.13 [1.41–12.07], p=0.003), more severe dyspnea on the mMRC scale (OR: 2.23 [1.07–4.65], p=0.03), lower quality of life as measured by the SGRQ score (OR: 1.08 [1.04–1.12], p<0.001) and current smoking (OR: 3.37 [1.29–8.81], p<0.01), as shown in . Among non-farmers, depression was associated with lower FEV1 (OR: 0.98 [0.96–0.99], p=0.02), grade 2 or more COPD (OR: 3.59 [1.18–10.93], p=0.02), more severe dyspnea using either the mMRC scale (OR: 2.94 [1.69–5.12], p<0.001) or the BDI score (OR: 0.68 [0.56–0.84], p=0.006), presence of symptoms (OR: 3.63 [1.31–10.09], p=0.009), female gender (OR: 3.35 [1.44–7.80], p=0.004), poorer quality of life (OR: 1.06 [1.03–1.09], p=0.001) and a higher BODE score (OR: 2.00 [1.19–3.39], p=0.01).
Figure 4 Factors associated with depression among dairy farmers and non-farmers.
Abbreviations: AS, active smoker; BDI, Baseline Dyspnea Index; BODE, Body mass index, airflow Obstruction, Dyspnea and Exercise capacity index; FEV1 post-BD, forced expiratory volume in 1 second post-bronchodilator; FS, former smoker; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, modified Medical Research Council scale; NS, non-smoker; SGRQ, St George’s Respiratory Questionnaire.
Discussion
This study performed in dairy farmers and in subjects with no occupational exposure in the French Franche-Comté region shows that 1) the prevalence of anxiety and depression as assessed by the HADS was similar in dairy farmers and non-farmers, whether with or without COPD; 2) some COPD-associated features, such as COPD severity, dyspnea and quality of life, were associated with depression in dairy farmers as well as in subjects with no occupational exposure; and 3) there was no relationship between anxiety and COPD-associated features among dairy farmers.
Several studies have shown that the farming population is at higher risk of anxiety, depression and even suicide than the general population. In a study conducted in the USA, male farmers, fishermen and foresters had the highest age-adjusted suicide rates (476 per 100,000), well above those of non-farmers (113 per 100,000, p<0.05).Citation29 In another study using the HADS, male farmers (n=1,100) had a higher prevalence of depression than non-farming male workers (n=10,026), with an age-adjusted OR of 1.49 (95% CI: 1.22–1.83).Citation17 Nevertheless, in this latter study, the prevalence of anxiety was similar in farmers and non-farmers.Citation17 Although our study was not designed to compare anxiety and/or depression between healthy farmers and healthy non-farmers, we did not observe any difference between these two groups. A point of note is that similar prevalences of anxiety and depression were found in our study in dairy farmers with COPD and in non-farmers with COPD (p=0.68 and p=0.73 for anxiety and depression, respectively). This may be due to the particular situation of dairy farmers in the Franche-Comté region. They sell their milk to the cheese manufacturing sector, in particular, for the production of the highly reputed Comté cheese, which is safeguarded by a protected designation of origin, guaranteeing a higher selling price for the milk. It may also be related to the design of our study, in which 1) only subjects who agreed to undergo a health checkup were included in the COPD screening program and 2) only half of the subjects who had COPD detected by screening agreed to attend the hospital visit for characterization. It has previously been reported that among all subjects who are invited for the health checkups organized by the French agricultural health insurance system (MSA), those who attend these checkups and those who do not have different health characteristics.Citation30 It is, therefore, possible that our population was not representative of the whole population of dairy farmers.
Some data have previously highlighted the association between COPD and anxiety and/or depression. More than 15 years ago, a study reported that among 79 patients with grade 2 or more COPD, 50% had anxiety and 28% had depression as assessed by a HADS score ≥8.Citation25 More recently, a study of 302 COPD patients (106 in grade 1 and 196 in grade 2 or more) showed that 53% had anxiety and 45% had depression, also assessed by a HADS score ≥8.Citation26 In this study, anxiety and depression were not limited to the most severe forms of COPD, since 34% of patients with anxiety and 28% of patients with depression had grade 1 COPD.Citation26 Nevertheless, large differences in the prevalence of anxiety and depression in COPD have been observed from one study to another, ranging from 10% to 55% for anxiety and from 15% to 36% for depression.Citation7,Citation8 In our study, we failed to find any difference in anxiety and/or depression prevalence between COPD patients detected by screening – the majority being Global Initiative for Chronic Obstructive Lung Disease grade 1 – and selected controls matched for age, gender and tobacco habits. Again, this finding might be due to a selection bias secondary to the study design. The discrepancy with the literature could also be due to the choice of the threshold value of 8 for the HADS. In our population, most subjects with a score >8 had a score <11, placing them in the borderline category, and only a minority had a score >11 (probable anxiety and/or depression). Nonetheless, a robust literature review revealed an optimal balance between sensitivity and specificity for a threshold of 8, for both anxiety and depression.Citation31
In our population, anxiety and depression were associated with higher SGRQ scores, reflecting poorer quality of life. The mean difference in SGRQ between patients with vs without anxiety was 5–8 points, and the average difference between depressed and non-depressed patients was more than 10 points. These differences are well above the 4-point threshold defining the minimum clinically important difference. For a similar level of anxiety and depression, the impact on the quality of life measured by the SGRQ tended to be greater among non-farmers than among farmers, despite similar mean FEV1 values in both groups. In addition, anxiety and depression were associated with more severe dyspnea scores among non-farmers only. These results are consistent with studies conducted in the general population, which observed a link between intensity of depression and severity of dyspnea.Citation32,Citation33 A point of note is that this association suggests that there is an overlap between symptoms of anxiety and depression on the one hand, and symptoms of COPD on the other hand; this overlap may explain at least in part the association observed in the study. Nevertheless, this result also suggests that among farmers, anxiety and depression are associated with factors other than dyspnea, which may not have been explored in our study.
It seems difficult to characterize anxiety and depression by a single score. It might have been appropriate to use other scores in addition to the HADS, such as the Beck Depression Inventory, Beck Anxiety Inventory and State–Trait Anxiety Inventory.Citation34,Citation35 A diagnostic questionnaire, such as the Mini-International Neuropsychiatric Interview or the Composite International Diagnostic Interview questionnaire, could have been administered to our positive cases to confirm the presence of anxiety and/or depression.Citation36,Citation37 Finally, a clinical evaluation of anxiety and depression could also have been performed because it can lead to results differing from those of the HADS. For example, in our population, being a woman was associated with the level of anxiety and depression only among non-farmers. In general, the prevalence, incidence and morbidity of depression are higher among women than among men, as early as in their teenage years.Citation38 Nevertheless, several studies have reported that the depression component of the HADS score was higher in men than in women.Citation39 This finding raises questions about the gender-specific validity of the HADS questionnaire. However, it also reinforces the results observed in our population of non-farmers regarding the link between anxiety and/or depression and female gender.
In conclusion, we have shown that dairy farmers with COPD have prevalences of anxiety and depression that are similar to those of dairy farmers without COPD. In accordance with previous reports, we also found that depression was associated with some COPD-related features, such as COPD severity, dyspnea and quality of life, and that this association was similar in dairy farmers and in subjects with no occupational exposure. In contrast, no association between anxiety and COPD-related features was found in our population of dairy farmers. In view of the particular situation of dairy farmers from Franche-Comté in terms of milk selling price, the observation that dairy farming is not associated with increased risk of anxiety and/or depression needs additional studies with other populations.
Availability of data and material
The data that support the findings of this study are available from the corresponding author.
Acknowledgments
The authors thank Stéphane Jouneau (Service de Pneumologie, CHU de Rennes, Rennes, France), Henri Simon (Mutualité Sociale Agricole, Besançon, France) and Martial Botebol (FeMaSaC, Besançon, France) for their intellectual contribution.
This study was supported by Novartis Pharma, Mutualité Sociale Agricole, Fédération des Maisons de Santé Comtoises, Don du Souffle and Association Santé Éducation et Prévention sur les Territoires Franche-Comté Bourgogne.
Disclosure
The authors report no conflicts of interest in this work.
References
- VestboJHurdSSAgustiAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- MonteagudoMRodriguez-BlancoTLlagosteraMFactors associated with changes in quality of life of COPD patients: a prospective study in primary careRespir Med2013107101589159723786889
- JonesPWBrusselleGDal NegroRWHealth-related quality of life in patients by COPD severity within primary care in EuropeRespir Med20111051576620932736
- PasqualeMKSunSXSongFHartnettHJStemkowskiSAImpact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare populationInt J Chron Obstruct Pulmon Dis2012775776423152680
- LaforestLRocheNDevouassouxGFrequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: a population-based cohort studyRespir Med2016117333927492511
- van den BemtLSchermerTBorHThe risk for depression comorbidity in patients with COPDChest2009135110811418689578
- MatteDLPizzichiniMMHoepersATPrevalence of depression in COPD: A systematic review and meta-analysis of controlled studiesRespir Med201611715416127492526
- WillgossTGYohannesAMAnxiety disorders in patients with COPD: a systematic reviewRespir Care201358585886622906542
- MaurerJRebbapragadaVBorsonSACCP Workshop Panel on Anxiety and Depression in COPDAnxiety and depression in COPD: current understanding, unanswered questions, and research needsChest20081344 Suppl43S56S
- SchneiderCJickSSBothnerUMeierCRCOPD and the risk of depressionChest2010137234134719801582
- AtlantisEFaheyPCochraneBSmithSBidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysisChest2013144376677723429910
- RyuJYSunwooYELeeSYChronic obstructive pulmonary disease (COPD) and vapors, gases, dusts, or fumes (VGDF): a meta-analysisCOPD201512437438025255043
- AlifSMDharmageSCBowatteGOccupational exposure and risk of chronic obstructive pulmonary disease: a systematic review and meta-analysisExpert Rev Respir Med201610886187227187563
- MarescauxADeganoBSoumagneTThaonILaplanteJJDalphinJCImpact of farm modernity on the prevalence of chronic obstructive pulmonary disease in dairy farmersOccup Environ Med201673212713326675204
- GuillienAPuyraveauMSoumagneTPrevalence and risk factors for COPD in farmers: a cross-sectional controlled studyEur Respir J20164719510326453630
- GregoireAThe mental health of farmersOccup Med (Lond)200252847147612488518
- TorskeMOHiltBGlasscockDLundqvistPKrokstadSAnxiety and depression symptoms among farmers: The HUNT Study, NorwayJ Agromedicine2016211243326488439
- HounsomeBEdwardsRTHounsomeNEdwards-JonesGPsychological morbidity of farmers and non-farming population: results from a UK surveyCommunity Ment Health J201248450351021556782
- FraserCESmithKBJuddFHumphreysJSFragarLJHendersonAFarming and mental health problems and mental illnessInt J Soc Psychiatry200551434034916400909
- Lunner KolstrupCKallioniemiMLundqvistPKymalainenHRStallonesLBrumbySInternational perspectives on psychosocial working conditions, mental health, and stress of dairy farm operatorsJ Agromedicine201318324425523844791
- DeganoBBouhaddiMLaplanteJJBPCO des producteurs laitiers: dépistage, caractérisation et constitution d’une cohorte. Étude BALISTIC [COPD in dairy farmers: Screening, characterization and constitution of a cohort. The BALISTIC study]Rev Mal Respir201229911491156 French23200591
- MillerMRHankinsonJBrusascoVATS/ERS Task ForceStandardisation of spirometryEur Respir J200526231933816055882
- QuanjerPHTammelingGJCotesJEPedersenOFPeslinRYernaultJCLung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory SocietyEur Respir J Suppl1993165408499054
- CelliBRCoteCGMarinJMThe body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary diseaseN Engl J Med2004350101005101214999112
- DowsonCLaingRBarracloughRThe use of the Hospital Anxiety and Depression Scale (HADS) in patients with chronic obstructive pulmonary disease: a pilot studyN Z Med J2001114114144744911700772
- JácomeCFigueiredoDGabrielRCruzJMarquesAPredicting anxiety and depression among family carers of people with chronic obstructive pulmonary diseaseInt Psychogeriatr20142671191119924621411
- WeatherallMMarshSShirtcliffePWilliamsMTraversJBeasleyRQuality of life measured by the St George’s Respiratory Questionnaire and spirometryEur Respir J20093351025103019164350
- JonesPWSt George’s Respiratory Questionnaire: MCIDCOPD200521757917136966
- StallonesLDoengesTDikBJValleyMAOccupation and suicide: Colorado, 2004–2006Am J Ind Med201356111290129523873359
- PelcADanguyVGosselinSValléeCLes invités aux instants sante en 2011: profil de consommation de soins des participants et des non participants [Health check up invited people in 2011: healthcare profile of participants and non participants]2013 Available from: http://www.msa.fr/lfr/documents/98830/9488297/Les+invit%C3%A9s+aux+Instants+Sant%C3%A9en+2011.pdfAccessed November 28, 2017
- BjellandIDahlAAHaugTTNeckelmannDThe validity of the hospital anxiety and depression scale. An updated literature reviewJ Psychosom Res2002522697711832252
- NeumanAGunnbjornsdottirMTunsaterADyspnea in relation to symptoms of anxiety and depression: a prospective population studyRespir Med2006100101843184916516455
- SharmaPMorrisNRAdamsLEffect of experimental modulation of mood on perception of exertional dyspnea in healthy subjectsJ Appl Physiol (1985)2016120211412026565017
- DoyleTPalmerSJohnsonJAssociation of anxiety and depression with pulmonary-specific symptoms in chronic obstructive pulmonary diseaseInt J Psychiatry Med201345218920223977821
- PhanTCarterOAdamsCDiscriminant validity of the hospital anxiety and depression scale, beck depression inventory (II) and beck anxiety inventory to confirmed clinical diagnosis of depression and anxiety in patients with chronic obstructive pulmonary diseaseChron Respir Dis201613322022826944070
- SheehanDVLecrubierYSheehanKHThe Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10J Clin Psychiatry199859Suppl 202233 quiz 34–57
- KesslerRCUstunTBThe World Mental Health (WMH) Survey Initiative Version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI)Int J Methods Psychiatr Res20041329312115297906
- FaravelliCAlessandra ScarpatoMCastelliniGLo SauroCGender differences in depression and anxiety: the role of agePsychiatry Res201321031301130324135551
- NortvedtMWRiiseTSanneBAre men more depressed than women in Norway? validity of the hospital anxiety and depression scaleJ Psychosom Res200660219519816439273