
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Existing data on COPD prevalence are limited or totally lacking in many regions of Europe. The geographic information system inverse distance weighted (IDW) interpolation technique has proved to be an effective tool in spatial distribution estimation of epidemiological variables, when real data are few and widely separated. Therefore, in order to represent cartographically the prevalence of COPD in Europe, an IDW interpolation mapping was performed. The point prevalence data provided by 62 studies from 19 countries (21 from 5 Northern European countries, 11 from 3 Western European countries, 14 from 5 Central European countries, and 16 from 6 Southern European countries) were identified using validated spirometric criteria. Despite the lack of data in many areas (including all regions of the eastern part of the continent), the IDW mapping predicted the COPD prevalence in the whole territory, even in extensive areas lacking real data. Although the quality of the data obtained from some studies may have some limitations related to different confounding factors, this methodology may be a suitable tool for obtaining epidemiological estimates that can enable us to better address this major public health problem.
Introduction
COPD is a large, growing public health problem. According to the World Health Organization, its expected burden will increase in the coming decades, mostly due to continued exposure to risk factors, population growth and aging, to become the third leading cause of death by 2030.Citation1
Despite being a major health problem, existing data on COPD prevalence are limited in many countries, and universally high COPD underdiagnosisCitation2 or misdiagnosisCitation3 deprives patients and health authorities of the implementation of adequate preventive and therapeutic measures, in order to avoid its potential serious effects and high costs.Citation4 In fact, of the 50 sovereign European countries, only 19 (38%) of them have available reliable data on COPD prevalence.Citation5
The geographic information system (GIS) is considered a useful tool for reporting the distribution of health-related states, in particular diseases.Citation6,Citation7 Specifically, the GIS inverse distance weighting (IDW) interpolation (or spatial analysis) technique (an informatics mathematical approach of manipulating spatial information to extract new information and meaning from the original data, using points with known values to estimate values at other unknown points) has proved to be an effective tool in spatial distribution estimation of epidemiological variables, when real data are few and widely separated, as might be the case with the COPD prevalence in Europe.Citation8–Citation10
The objective of the present study was to apply the IDW mapping to integrate the existing data from different European areas, in order to represent cartographically the mean percentage of the population affected by COPD in each geographical region of the entire continent, both in studied areas with known data and in many other areas in which no studies have been conducted and consequently with blank data.
Methods
Source of epidemiological studies for COPD prevalence
The vast majority of the data entered in the database used in the IDW interpolation software were taken from the systematic review and meta-analysis recently published by Adeloye et al on the prevalence of COPD across the world from January 1990 to December 2014, based on a confirmed diagnosis of COPD with different formally acknowledged spirometric criteria.Citation5 For the current study, only the variables referring to the place of origin of the samples and the mean COPD prevalence (in percent) of the samples composed of subjects aged ≥40 years were used.Citation11–Citation63 To the initially selected 61 studies, a later one on the prevalence of COPD, as defined by the Global Initiative for Obstructive Lung Disease (GOLD), in a representative sample of northeastern Italy general population was added.Citation64
The application of an age selection criterion of ≥40 years excluded, from the present study, an international study that included young subjects from several cities in Europe aged between 20 and 44 years,Citation65 2 studies performed in 12 Russian regions,Citation66,Citation67 and another study of the Turkish region of Elazig all of them carried out in subjects from the age of 18.Citation68
In addition, to facilitate visual comparisons between Europe and the neighboring regions of Asia and Africa, the available COPD prevalence data from several Middle East and North Africa regions were also included.Citation69–Citation77
IDW multivariate interpolation method
To elaborate colored geographical maps of COPD prevalence, an IDW interpolation process was started through the freely available software QGIS 18.9 in order to link it with the 7.3 64-bit wxPython 3 Geographic Resources Analysis Support System (GRASS).
Then, the geographical longitude and latitude coordinates of the different places were automatically obtained for each point by translating the location of the place of origin of the samples included. The translation was made through the Google Maps application programming interface using the web page of GPS Visualizer (Carleton University Library, Ottawa, ON, Canada).
Then, these geographical coordinates were imported into the database and then exported to a “csv” (comma separated value) text file, which was opened and visualized in QGIS. A shape file containing the contours of all world countries was also loaded.
Finally, the interpolation process was carried out by applying the “v.surf.idw” library included in the GRASS GIS version 7, another free and open source GIS software suite used for geospatial data management and analysis, spatial modeling, image processing, graphics and maps production, and visualization.
The v.surf.idw library provided surface interpolation from vector point data by filling out a raster matrix with interpolated values generated from a set of irregularly spaced data points, using numerical approximation (weighted averaging) techniques. The interpolated value of a cell was determined by the values of the nearby data points and the distance of the cell from those input points.
An implementation of an IDW technique, as defined by Shepard,Citation7 is as follows: the way to find an interpolated value u at a given (arbitrary) point x based on N known samples ui=u(xi) for i=1, 2, …, N is:
The “N known samples” is the N closest ones to the interpolation point. In our study, the usual N value of 4 (N=4) was chosen. This means that a sample point takes the 4 closest pixel centers and linearly interpolates their color values according to their distance from the sample point; p is called the power parameter, which has a default value of 2, which was the value used in this study.
To express the range of values in the maps, a progressive gradient (low–high) range scale of 10 colors, creating a diverging low–mid–high color gradient, with dark blue tones representing the lowest values, yellow and green representing the intermediate ones, and brown and dark red representing the highest ones, was used.
Geographical regions of Europe
Although there is not a universally accepted definition of the boundaries and countries of the European regions, to facilitate the description of findings, we used a simple and conventional classification of the regions of Europe into 5 major subregions, namely Northern Europe, Western Europe, Central Europe, Southern Europe, and Eastern Europe.Citation79
Northern Europe consists approximately of the Europe regions above the 52nd parallel north, and in this geographical area, the following countries have been included for this study: Iceland, Denmark, Norway, Sweden, Finland, Estonia, Latvia, and Lithuania.
In Western Europe, the following countries have been included: the Netherlands, Belgium, Luxembourg, France, Ireland, and UK.
In Central Europe, the following countries have been included: Germany, Austria, Poland, Slovakia, Czech Republic, Hungary, Slovenia, and Switzerland.
In Southern Europe, the following countries have been included: Spain, Portugal, Italy, Greece, Malta, Cyprus, and Turkey.
Although there is no consensus on the precise area covered by Eastern Europe, because the term has a wide range of geopolitical, geographical, cultural, and socioeconomic connotations, the following countries have been included in this region: the Balkan Peninsula countries (Albania, Croatia, Bosnia and Herzegovina, Montenegro, Serbia, and Macedonia), Romania, Moldova, Bulgaria, Ukraine, Belarus, and European Russia.
Statistical analysis
Descriptive statistics were used to summarize study sites. Quantitative variables were expressed as mean and SD, 95% CI for the mean, and range, and they were analyzed using the analysis of variance. A p<0.05 was considered statistically significant. Statistical calculations were performed using the analytical software SPSS 19 (IBM Corp., Armonk, NY, USA).
Results
The cohorts
A total of 62 studies from 19 countries (21 from 5 Northern European countries, 11 from 3 Western European countries, 14 from 5 Central European countries, and 16 from 6 Southern European countries) were selected (–). As mentioned previously, no prevalence data were available for any of the 12 countries from Eastern Europe.
Table 1 Mean prevalence of COPD in 21 studies from 5 Northern Europe countries
Table 2 Mean prevalence of COPD in 11 studies from 3 Western Europe countries
Table 3 Mean prevalence of COPD in 14 studies from 5 Central Europe countries
Table 4 Mean prevalence of COPD in 15 studies from 6 Southern Europe countries
Numbers of point estimates by individual countries (from high to less) were as follows: Sweden, 8; United Kingdom, 7; Norway, 5; Finland, Germany, and Turkey, 4 each; the Netherlands, Austria, Poland, Portugal, and Spain, 3 each; Italy and Greece, 2; and other remaining countries, 1.
Accordingly, a total of 329,413 subjects from the 4 regions of Europe with published data were studied; they were distributed as follows: 39,836 in Northern Europe; 229,083 in Western Europe; 25,553 in Central Europe; and 34,941 in Southern Europe.
The size of the selected samples was significantly different in the 4 European regions, with a mean (minimum and maximal values in parentheses) of 1,897 (548–6,525) subjects in Northern Europe; 20,751 (246–185,325) in Western Europe; 1,825 (432–6,126) in Central Europe; and 2,329 (500–9,061) in Southern Europe.
Most of the studies were conducted in isolated cities or localized regions of a particular country, while only a few were carried out on samples representative of the adult general population of an entire country, such as those performed in the Netherlands,Citation33 UK,Citation39 Switzerland,Citation50 Portugal,Citation52 Spain,Citation54,Citation55 and Cyprus.Citation60
According to the study base of the samples, 23 of them were classified as urban (7 from Northern Europe, 4 from Western Europe, 7 from Central Europe, and 5 from Southern Europe), 9 (6 from Northern Europe, 1 from Central Europe, and 2 from Southern Europe) were classified as rural, and the remaining 30 were catalogued as mixed.
The mean age of the subjects from the 62 selected samples was 55.9 years (SD =6.1), without significant differences between regions ().
Table 5 Ages of selected samples, descriptive statistics
In 80% of the studies, the diagnosis of COPD was made by using the GOLD spirometric criteria of the postbronchodilator (post-BD) fixed ratio FEV1/FVC <0.70; in the remaining 12 studies, other spirometric criteria (not post-BD) endorsed by different scientific societies were used, such as the lower limit of normal, the British Thoracic Society, the American Thoracic Society, and European Respiratory Society criteria.
COPD prevalence
The global mean prevalence of COPD (expressed in percent) was 12.38 (SD =6.2) without significant differences among the 4 European regions with available data ().
Table 6 COPD prevalence in Europe, descriptive statistics
The highest values of prevalence were found in 2 samples from the cities of Manchester and Salzburg (26% each), followed by those of Ashington and Copenhagen (with 25% each); the COPD subjects from Glasgow, the Po Delta area of Italy, and the southern Poland region of Malopolska (with 24%, 23%, and 22%, respectively); and the COPD subjects from the metropolitan areas of Stockholm and Vienna (with 20% each).
Prevalence rates between ≥15% and ≤20% were found in the cities of Bergen and Maastricht and in the Turkish province of Adana (all with 19%), in the metropolitan areas of Reykjavik and Thessaly (both 18%), and in Berlin (with 16%).
Prevalence ranges between ≥10% and ≤15% were found in a sample from Luleå (in the northernmost county of Sweden) with 14%, followed by 2 samples from Barton-upon-Humber (England) and Hannover (Germany) both with 13% and the patients’ samples from the Danish cities of Aarhus and Aalborg and the Dutch city of Rotterdam (with 12%). Prevalence value of 11% was found in Warsaw, in the Polish region of Lublin, and in the Swedish counties of Norrbotten and Örebro. Prevalence values slightly >10% were found in Slovenia, Spain, and Portugal and in the general population of the UK.
In practically all of the remaining places with available data, prevalence ranged from 5 to <10%. Anecdotally, a young rural cohort, with a mean age of 45 years, from the Swedish county of Värmland showed the lowest prevalence of COPD in Europe, with a percentage slightly >2%.
IDW interpolation maps
In the IDW interpolation map of , the prevalence rates of COPD of all European countries are represented by a red–blue scale. Black spots indicate the places of origin of the samples.
Figure 1 COPD mean prevalence in Europe.
Abbreviation: IDW, inverse distance weighting.
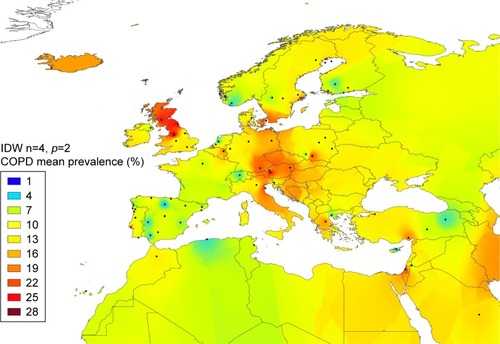
In a simplified way, since there is no exact equivalence between the qualitative data provided by the color scale and the quantitative ones provided by the numerical values, it can be interpreted with reasonable certainty that red tones represent the maximum values >20%; brown and orange colors symbolize high but lower values of ~15%–20%; shades of yellow and green tones represent intermediate values of ~10%–15%; and blue tones represent minimal values of 0%–5%.
The greatest numbers of black spots are located in the Iberian Peninsula, Great Britain, Central Europe, and the coastal regions bordering the North and the Baltic Seas. In contrast, spots are in general scattered and scanty in most of the remaining parts of the continent and absolutely absent in the Mediterranean islands of Corsica, Sardinia, Sicily and Greek islands, southern Italy, Balkan Peninsula, and regions belonging to Eastern Europe.
Some black spots can also be seen in some nearby countries of North Africa and Middle East (for guidance).
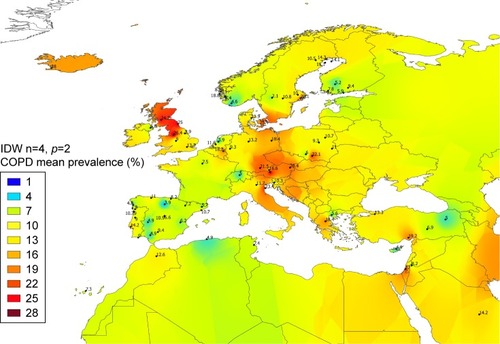
In , the numerical values of the corresponding prevalence rates have been added. The numerical values appear with a decimal and are the same reproduced (rounded) in –.
Figure 2 COPD mean prevalence in Europe.
Abbreviation: IDW, inverse distance weighting.
In the map of , both black spots and numerical figures have been removed to allow a clearer view of the colors with which the different regions were colored.
Figure 3 COPD mean prevalence in Europe.
Abbreviation: IDW, inverse distance weighting.
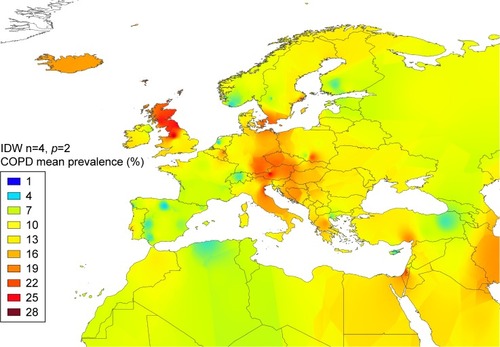
A very high prevalence represented by red tones (≈20%–27%) appears in practically all Great Britain, except in the south of the island that presents brownish colors in the west and yellow in the center and east consistent with an intermediate prevalence. Reddish colors, indicative of a very high prevalence, are also shown in the southeast of the Scandinavian Peninsula, the Island of Amager (Denmark), southeast of Germany, western and southern Poland, Austria, Czech Republic, and Slovakia (these last 2 countries without studies and therefore without real numerical values).
Brown and orange tones (approximately equivalent to a range of numerical values between 15% and 20%) appear in Iceland, Hungary, large areas of Italy (except the regions of Lombardy, Piedmont, Liguria, and Calabria, which appear in yellow color), Croatia, Bosnia and Herzegovina, Serbia, and Greece, as well as in the province of Adana (southern Turkey). Of note, there are no real numerical values for the Balkan countries that were colored by means of the IDW mapping.
Most of the remaining regions of Europe are stained in yellow and green colors, indicative of an intermediate prevalence of ~10%–15%; the Danish peninsula of Jutland, most of Sweden, Norway, and northern Finland, the Baltic seacoast countries and the Baltic islands of Gotland and Aland, Belorussia, most of the lands of Poland, the western half of Germany, the coastal regions of Western Europe and Great Britain bordering the North Sea and the English Channel, Ireland, Portugal, Spain, the Mediterranean major islands, Slovenia, Ukraine, Romania, Bulgaria, European Russia, Montenegro, Albania, Macedonia, and the Anatolian Peninsula are included in this group. Remarkably, many of these regions were stained by IDW interpolation in the absence of real numerical data.
Blue areas (indicative of the prevalence of around or <5%) are scarce and isolated; Switzerland, the island of Cyprus, some cities of Spain, such as Vigo, Burgos, Cáceres, and Seville, scattered areas of the Scandinavian peninsula and Finland, and the Erzurum Province of eastern Turkey are among them.
Discussion
Existing data on COPD prevalence are in general insufficient and irregularly distributed in many regions of Europe, in some of which there is a striking scarcity or even an absolute lack of epidemiological information about this important health issue.
To assess the COPD prevalence throughout the European continent and its surrounding islands, an efficient method of proven utility, known as IDW multivariate interpolation (or spatial analysis), which is usually applied to various disciplines concerned with the earth’s surface, such as cartography, geography, hydrology, climatology, and agriculture, was used in the present study in order to generate a continuous map of COPD prevalence.
Basically, IDW interpolation uses data points with known values to estimate other values at unknown locations, in order to create a raster surface consisting of an array of cells (pixels) arranged in rows and columns (or a grid) in which each cell contains a value representing some prevalence information, finally covering a whole area. The IDW method is based on the assumption that the attribute value of an unsampled point is the weighted average of known values within the 4 nearest data points. IDW assumes that each measured point has a local influence that diminishes with distance, weighting the points closer to the prediction location greater than those located farther away, which means that weights are inversely related to the distances between the sampled locations and the predicted ones.Citation7
The IDW interpolation is a simple and intuitive method, easy to handle and interpret, relatively fast for calculations, and easy to compute, which also has the advantage of allowing to easily renewing the database, with a flexibility of the inclusion of studies newly identified, that are more recent, or with a better study design. Similar flexibility applies to the exclusion of others of less scientific quality to automatically reconstructing new, updated maps. In addition, IDW has a mathematical precision that makes it always exact, but this advantage can be a disadvantage if the actual data were erroneous or inaccurate. Since it works automatically creating new points from others supposedly accurate, it is crucial to introduce reliable data; otherwise the final results will also be inaccurate or erroneous.
For the present study, the numerical data of prevalence rates were obtained with the best available evidence in publicly accessible scientific databases, and only surveys constituted by patients of at least ≥40 years of age and a confirmed diagnosis of COPD with spirometry were selected for the analysis.
Limitations
However, the authors of the present study are aware that the analysis may have some limitations due to a number of confounding factors frequently associated with cross-sectional studies, and sometimes these confounding variables could have led to spurious associations. For example, the sampling approach varied from study to study or even among sites in the same study. In addition, the size of the samples was highly variable, with significant differences between regions, and some of them were not proportional to the general population of the studied region. Remarkably, the lack or scarcity of data in extensive regions of Europe makes the scientific hypotheses from which some conclusions were drawn less reliable.
There are also some (though not statistically significant) differences in the age distribution between regions of Europe and even within the same region of the same country, and since in spirometry-based studies the prevalence of COPD increases with age, the lack of homogeneity in this variable may be the reason for some of the erratic values.
On the other hand, when modeling relative risks or ORs from data obtained from a given population, results may not be applicable to populations with different levels of exposure, as the relations may not be linear across all exposure levels. Regrettably, in our study, there was no proportionality between the number of urban and rural cohorts, and thus, studies performed in populations with high levels of smoking or occupational air pollutants exposure may not be generalizable to those of populations with lower levels of exposure.
Another limitation may be related to the differences in case definitions. The definition based on post-BD FEV1/FVC <0.70 was used in the large majority (80%) of studies, but this still does not address all possible sources of variation in case definition, since this fixed ratio criterion may potentially overdiagnose COPD in the elderly and it may underdiagnose COPD in younger patients. Besides, a number of technical issues could have affected the estimates, such as the quality of the commercial models of the spirometers used, the level of training of the operators, and the process of collection and storage of spirometry measurements.Citation2–Citation5
Finally, an intrinsic limitation of GIS is that geographic proximity does not take into account borders, which often within Europe mirror a different language or dialect. Common language is a well-established factor for unevenly distributing genes, related to or not to health, and many other social determinants.Citation78
Nevertheless, in spite of all these criticisms, it should be emphasized that GIS unquestionably offers a useful new tool in epidemiology, which makes it ever easier to connect spatially referenced physical and social phenomena to population patterns of health, disease, and well-being.
Therefore, in our opinion, the easy-to-interpret and eye-catching impacting results of this technique may contribute to enhancing public health surveillance as well as delineating the prevalence of COPD in Europe and in other countries; to increase the number of doctors who treat this type of patients and the health authorities and national governments’ interest in strengthening regulations to address occupational and environmental risk factors, regulate tobacco use, and improve public awareness; to all together increase the rate of diagnoses and to implement the application of preventive and therapeutic measures to avoid potential side effects and unnecessary costs; and to reduce the high global COPD burden in coming years.
Disclosure
The authors report no conflicts of interest in this work.
References
- GBD 2015 Chronic Respiratory Disease CollaboratorsGlobal, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015Lancet Respir Med2017569170628822787
- BerndLJoanBSMichaelSDeterminants of underdiagnosis of COPD in national and international surveysChest201514897198525950276
- Fernández-VillarASorianoJBLópez-CamposJLOverdiagnosis of COPD: precise definitions and proposals for improvementBr J Gen Pract20176718318428360069
- SorianoJBRodriguez-RoisinRChronic obstructive pulmonary disease overview: epidemiology, risk factors and clinical presentationProc Am Thorac Soc2011836336721816993
- AdeloyeDChuaSLeeCGlobal and regional estimates of COPD prevalence: systematic review and meta-analysisJ Glob Health2015502041526755942
- MitasLMitasovaHSpatial interpolationLongleyPAGoodchildMFMaguireDJRhindDWGeographical Information Systems (GIS): Principles, Techniques, Management and ApplicationsNew YorkJohn Wiley1999481492
- ShepardDA two-dimensional interpolation function for irregularly-spaced dataProceedings of the 1968 23rd ACM National Conference. ACM’681968ACMNew York, NY517524
- BlancoIde SerresFJCárcabaVLaraBFernández-BustilloEAlpha-1 antitrypsin deficiency PI*Z and PI*S gene frequency distribution using on maps of the world by an inverse distance weighting (IDW) multivariate interpolation methodHepat Mon20121210 HCCe743423166537
- BlancoIBuenoPDiegoIAlpha-1 antitrypsin Pi*Z gene frequency and Pi*ZZ genotype numbers worldwide: an updateInt J Chron Obstruct Pulmon Dis20171256156928243076
- BlancoIBuenoPDiegoIAlpha-1 antitrypsin Pi*SZ genotype: estimated prevalence and number of SZ subjects worldwideInt J Chron Obstruct Pulmon Dis2017121683169428652721
- FabriciusPLokkeAMarottJLVestboJLangePPrevalence of COPD in CopenhagenRespir Med201110541041720952174
- MaioSSherrillDLMacNeeWThe European Respiratory Society spirometry tent: a unique form of screening for airway obstructionEur Respir J2012391458146722267757
- HansenJGPedersenLOvervadKOmlandOJensenHKSorensenHTThe prevalence of chronic obstructive pulmonary disease among Danes aged 45–84 years: population–based studyCOPD2008534735219353348
- KainuARouhosASovijärviALindqvistASarnaSLundbäckBCOPD in Helsinki, Finland: socioeconomic status based on occupation has an important impact on prevalenceScand J Public Health20134157057823599377
- Jyrki-TapaniKSovijarviALundbackBChronic obstructive pulmonary disease in Finland: prevalence and risk factorsCOPD2005233133917146998
- IsoahoRPuolijokiHHuhtiEKiveläSLLaippalaPTalaEPrevalence of chronic obstructive pulmonary disease in elderly FinnsRespir Med1994885715807991881
- KanervistoMVasankariTLaitinenTHeliövaaraMJousilahtiPSaarelainenSLow socioeconomic status is associated with chronic obstructive airway diseasesRespir Med20111051140114621459567
- BenediktsdóttirBGudmundssonGJorundsdottirKBVollmerWGíslasonTPrevalence of COPD in Iceland – the BOLD studyLaeknabladid200793471477 Icelandic17541146
- WaatevikMSkorgeTDOmenaasEBakkePGulsvikAJohannessenAIncreased prevalence of chronic obstructive pulmonary disease in a general populationRespir Med20131071037104523680166
- HvidstenSCStoresundLWentzel-LarsenTGulsvikALehmannSPrevalence and predictors of undiagnosed chronic obstructive pulmonary disease in a Norwegian adult general populationClin Respir J20104132120298413
- BuistASMcBurnieMAVollmerWMInternational variation in the prevalence of COPD (The BOLD Study): a population-based prevalence studyLancet200737074175017765523
- BakkePSBasteVHanoaRGulsvikAPrevalence of obstructive lung disease in a general population: relation to occupational title and exposure to some airborne agentsThorax1991468638701792631
- JohannessenAOmenaasEBakkePGulsvikAIncidence of GOLD – defined chronic obstructive pulmonary disease in a general adult populationInt J Tuberc Lung Dis2005992693216104642
- DanielssonPOlafsdottirISBenediktsdottirBGislasonTJansonCThe prevalence of chronic obstructive pulmonary disease in Uppsala, Sweden – the Burden of Obstructive Lung Disease (BOLD) study: cross-sectional population-based studyClin Respir J2012612012721651748
- LindbergABjergARonmarkELarssonLGLundbackBPrevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking: report from the Obstructive Lung Disease in Northern Sweden StudiesRespir Med200610026427215975774
- LindbergAJonssonACRonmarkELundgrenRLarssonLGLundbackBPrevalence of chronic obstructive pulmonary disease according to BTS, ERS, GOLD and ATS criteria in relation to doctor’s diagnosis, symptoms, age, gender, and smoking habitsRespiration20057247147916210885
- LindströmMJönssonELarssonKLundbäckBUnderdiagnosis of chronic obstructive pulmonary disease in Northern SwedenInt J Tuberc Lung Dis20026768411931405
- HasselgrenMArneMLindahlAJansonSLundbäckBEstimated prevalences of respiratory symptoms, asthma and chronic obstructive pulmonary disease related to detection rate in primary health careScand J Prim Health Care200119545711303549
- LarssonMWhere is the borderline between asthma and “COPD”? Reflections on a diagnostic questionnaireLakartidningen19959210891092 Swedish7700110
- RocheNDalmayFPerezTImpact of chronic airflow obstruction in a working populationEur Respir J2008311227123318216058
- VanfleterenLEFranssenFMWesselingGWoutersEFThe prevalence of chronic obstructive pulmonary disease in Maastricht, the NetherlandsRespir Med201210687187422349067
- van DurmeYMTAVerhammeKMCStijnenTPrevalence, incidence, and lifetime risk for the development of COPD in the elderly: the Rotterdam studyChest200913536837719201711
- AfonsoASVerhammeKMSturkenboomMCBrusselleGGCOPD in the general population: prevalence, incidence and survivalRespir Med20111051872188421852081
- JordanREMillerMRLamKBChengKKMarshJAdabPSex, susceptibility to smoking and chronic obstructive pulmonary disease: the effect of different diagnostic criteria. Analysis of the Health Survey for EnglandThorax20126760060522382600
- MelvilleAMPless-MulloliTAfolabiOAStentonSCCOPD prevalence and its association with occupational exposures in a general populationEur Respir J20103648849320110401
- MurtaghEHeaneyLGinglesJPrevalence of obstructive lung disease in a general population sample: the NICECOPD studyEur J Epidemiol20052044345316080593
- DickinsonJAMeakerMSearleMRatcliffeGScreening older patients for obstructive airways disease in a semi-rural practiceThorax19995450150510335003
- RenwickDSConnollyMJPrevalence and treatment of chronic airways obstruction in adults over the age of 45Thorax1996511641688711649
- ShahabLJarvisMJBrittonJWestRPrevalence, diagnosis and relation to tobacco dependence of chronic obstructive pulmonary disease in a nationally representative population sampleThorax2006611043104717040932
- WeissGSteinacherILamprechtBDetection of chronic obstructive pulmonary disease in primary care in Salzburg, Austria: findings from the real worldRespiration20148713614324296512
- SchirnhoferLLamprechtBVollmerWMCOPD prevalence in Salzburg, Austria: results from the Burden of Obstructive Lung Disease (BOLD) studyChest2007131293617218553
- GeldmacherHBillerHHerbstADie Prävalenz der chronisch obstruktiven Lungenerkrankung (COPD) in Deutschland [The prevalence of chronic obstructive pulmonary disease (COPD) in Germany. Results of the BOLD study]Dtsch Med Wochenschr200813326092614 German19052996
- GingterCWilmSAbholzHHIs COPD a rare disease? Prevalence and identification rates in smokers aged 40 years and over within general practice in GermanyFam Pract2009263919033180
- BednarekMMaciejewskiJWozniakMKucaPZielinskiJPrevalence, severity and underdiagnosis of COPD in the primary care settingThorax20086340240718234906
- Nizankowska-MogilnickaEMejzaFBuistASPrevalence of COPD and tobacco smoking in Malopolska region – results from the BOLD study in PolandPol Arch Med Wewn200711740241018062562
- PlywaczewskiRBednarekMJonczakLZielinskiJPrevalence of COPD in Warsaw populationPneumonol Alergol Pol200371329335 Polish15052966
- PaprzyckiPPanasiukLSodolskiWPrevalence of obstructive respiratory disorders in the rural population of the Lublin regionAnn Univ Mariae Curie Sklodowska Med200358727815314962
- SiatkowskaHKozielskiJZioraDChronic obstructive pulmonary disease patients in the general practicePneumonol Alergol Pol20107811212020306422
- Grzetic-RomcevicTDevcicBSoncSSpirometric testing on World COPD DayInt J Chron Obstruct Pulmon Dis2011614114621468166
- BridevauxPOProbst-HenschNMSchindlerCPrevalence of airflow obstruction in smokers and never-smokers in SwitzerlandEur Respir J2010361259126920413537
- BárbaraCRodriguesFDiasHChronic obstructive pulmonary disease prevalence in Lisbon, Portugal: the burden of obstructive lung disease studyRev Port Pneumol2013199610523664024
- CardosoJFerreiraJRAlmeidaJDoença Pulmonar Obstrutiva Crónica em Portugal: estudo Pneumobil (1995) e estudo de prevalência de 2002 revisitados [Chronic obstructive pulmonary disease in Portugal: Pneumobil (1995) and 2002 prevalence studies revisited]Rev Port Pneumol2013198895 Portuguese23639349
- MascarenhasJFalcãoHLourençoPPopulation-based study on the prevalence of spirometric obstructive pattern in Porto, PortugalRespir Care20115661962521276282
- MiravitllesMSorianoJBGarcía-RíoFPrevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activitiesThorax20096486386819553233
- PeñaVSMiravitllesMGabrielRGeographic variations in prevalence and underdiagnosis of COPD: results of the IBERPOC multicentre epidemiological studyChest200011898198911035667
- Cabrera LópezCJuliá SerdáGCabrera LacalzadaCPrevalencia de la enfermedad pulmonar obstructiva crónica en las Islas Canarias [Prevalence of chronic obstructive pulmonary disease in the Canary Islands]Arch Bronconeumol201450272277 Spanish24507558
- ViegiGPedreschiMPistelliFPrevalence of airways obstruction in a general population: European Respiratory Society vs American Thoracic Society definitionChest20001175 Suppl 2339S345S10843974
- SichletidisLTsiotsiosIGavriilidisAPrevalence of chronic obstructive pulmonary disease and rhinitis in northern GreeceRespiration20057227027715942296
- MinasMHatzoglouCKaretsiECOPD prevalence and the differences between newly and previously diagnosed COPD patients in a spirometry programPrim Care Respir J20101936337020532466
- ZachariadesAGZachariadouTAdamideTAnagnostopoulouUGeorgiouAGourgoulianisKIPrevalence of chronic obstructive pulmonary disease in Cyprus: a population-based studyCOPD2012925926722432899
- ArslanZIlgazlıAEtilerNHamzaoğluOPrevalence of chronic obstructive pulmonary disease in Kocaeli: an industrialised city in TurkeyBalkan Med J20133038739325207146
- ErdoganAYimazel-UcarEArazOSaglamLMiriciNAContribution of spirometry to early diagnosis of chronic obstructive pulmonary disease in primary health care centersTurk J Med Sci201443690694
- GunenHHacievliyagilSSYetkinOGulbasGMutluLCPehlivanEPrevalence of COPD: first epidemiological study of a large region in TurkeyEur J Intern Med20081949950419013377
- GuerrieroMCaminatiMViegiGSennaGCesanaGPomariCCOPD prevalence in a north-eastern Italian general populationRespir Med20151091040104726052037
- de MarcoRAccordiniSCerveriIAn international survey of chronic obstructive pulmonary disease in young adults according to GOLD stagesThorax20045912012514760151
- ChuchalinAGKhaltaevNAntonovNSChronic respiratory diseases and risk factors in 12 regions of the Russian FederationInt J Chron Obstruct Pulmon Dis2014996397425246783
- ArtyukhovIPArshukovaILDobretsovaEADuginaTAShulminAVDemkoIVEpidemiology of chronic obstructive pulmonary disease: a population-based study in Krasnoyarsk region, RussiaInt J Chron Obstruct Pulmon Dis2015101781178626366070
- DeveciFDeveciSETürkoğluSThe prevalence of chronic obstructive pulmonary disease in Elazig, Eastern TurkeyEur J Intern Med20112217217621402248
- AmraBGolshanMFietzeIPenzelTWelteTCorrelation between chronic obstructive pulmonary disease and obstructive sleep apnea syndrome in a general population in IranJ Res Med Sci20111688588922279455
- GolshanMAmraBWelteTSample survey of chronic obstructive pulmonary disease and associated risk factors in Isfahan, IranTanaffos2011103236
- Al ZaabiAAsadFAbdouJPrevalence of COPD in Abu Dhabi, United Arab EmiratesRespir Med201110556657021216136
- Al GhobainMAlhamadEHAlorainyHSAl KassimiFLababidiHAl-HajjajMSThe prevalence of chronic obstructive pulmonary disease in Riyadh, Saudi Arabia: a BOLD studyInt J Tuberc Lung Dis2015191252125726459542
- WakedMKhayatGSalamehPChronic obstructive pulmonary disease prevalence in Lebanon: a cross-sectional descriptive studyClin Epidemiol2011331532322253549
- Al OmariMKhassawnehBYKhaderYDauodASBergusGPrevalence of chronic obstructive pulmonary disease among adult male cigarettes smokers: a community-based study in JordanInt J Chron Obstruct Pulmon Dis2014975375825092972
- StavDRazMPrevalence of chronic obstructive pulmonary disease among smokers aged 45 and up in IsraelIsr Med Assoc J2007980080218085037
- El RhaziKNejjariCBenJellounMCEl BiazeMAttassiMGarcia-LarsenVPrevalence of chronic obstructive pulmonary disease in Fez, Morocco: results from the BOLD studyInt J Tuberc Lung Dis20162013614126688540
- AdeloyeDBasquillCPapanaAChanKYRudanICampbellHAn estimate of the prevalence of COPD in Africa: a systematic analysisCOPD201512718124946179
- Cavalli-SforzaLMenozziPPiazzaAThe History and Geography of Human GenesPrincetonPrinceton University Press1996
- EuroVoc [webpage on the Internet]Multilingual Thesaurus of the European Union Available from: http://eurovoc.europa.eu/drupal/?q=request&uri=http://eurovoc.europa.eu/100277Accessed November 24, 2017