
Abstract
Background and Objectives
Chronic obstructive pulmonary disease (COPD) affects over 250 million people globally, carrying a notable economic burden. This systematic literature review aimed to highlight the economic burden associated with moderate-to-very severe COPD and to investigate key drivers of healthcare resource utilization (HRU), direct costs and indirect costs for this patient population.
Materials and Methods
Relevant publications published between January 1, 2006 and November 14, 2016 were captured from the Embase, MEDLINE and MEDLINE In-Process databases. Supplemental searches from relevant 2015–2016 conferences were also performed. Titles and abstracts were reviewed by two independent researchers against pre-defined inclusion and exclusion criteria. Studies were grouped by the type of economic outcome presented (HRU or costs). Where possible, data were also grouped according to COPD severity and/or patient exacerbation history.
Results
In total, 73 primary publications were included in this review: 66 reported HRU, 22 reported direct costs and one reported indirect costs. Most of the studies (94%) reported on data from either Europe or North America. Trends were noted across multiple studies for higher direct costs (including mean costs per patient per year and mean costs per exacerbation) being associated with increasingly severe COPD and/or a history of more frequent or severe exacerbations. Similar trends were noted according to COPD severity and/or exacerbation history for rate of hospitalization and primary care visits. Multivariate analyses were reported by 29 studies and demonstrated the statistical significance of these associations. Several other drivers of increased costs and HRU were highlighted for patients with moderate-to-very severe COPD, including comorbidities, and treatment history.
Conclusion
Moderate-to-very severe COPD represents a considerable economic burden for healthcare providers despite the availability of efficacious treatments and comprehensive guidelines on their use. Further research is warranted to ensure cost-efficient COPD management, to improve treatments and ease budgetary pressures.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by incurable, progressive airflow restriction and has various clinical forms, including emphysema and chronic bronchitis.Citation1 Periods of time in which patients experience an acute deterioration in their respiratory symptoms, known as exacerbations, are a common manifestation of the disease.Citation1 A debilitating yet preventable multifactorial disease, COPD is estimated to affect over 380 million people worldwide.Citation2
The goals of COPD pharmacologic therapy are to provide symptomatic relief, improve health status and exercise tolerance, and prevent and treat exacerbations.Citation1 While therapeutic regimens are adapted according to the needs of each individual patient, most pharmacologic maintenance treatments can be categorized as either inhaled corticosteroids (ICS), long-acting muscarinic antagonists (LAMA) or long-acting β2-agonists (LABA),Citation1 and are often administered as combinations. As an example, triple therapy with an ICS, LAMA and LABA has been shown to improve lung function and patient-reported outcomes, including exacerbation risk, compared with ICS/LABA or LAMA monotherapy.Citation1 Despite recent advances within the field and the availability of guideline-recommended treatments, current management is inadequate for many patients with COPD; this unmet need, coupled with the high prevalence of the condition, suggests a high clinical and economic burden, and this has been demonstrated in a number of studies.
Previous publications have indicated that COPD is associated with a substantial economic burden, both in terms of direct costs to healthcare systems and indirect costs to society.Citation1,Citation3–Citation5 In the United States (US), for example, direct costs of COPD were estimated to be $32 billion in 2010, with indirect costs (incurred by lost working days, for instance) accounting for an additional $20.4 billion.Citation3
While evidence on the economic burden of COPD exists, it generally comprises individual studies that are limited by factors such as population characteristics, geographical location and clinical setting. To better understand the current COPD-related burden in settings where patients are likely to be managed as per globally recognised treatment algorithms, such as from the Global Initiative for Chronic Obstructive Lung Disease (GOLD),Citation1 we performed a comprehensive systematic literature review (SLR) of real-world observational studies in patients with moderate-to-very severe disease and/or those with a history of exacerbations, conducted across a number of industrialized countries during the last decade. This evidence was obtained to address two research questions. Firstly, what is the global economic burden associated with moderate-to-very severe COPD? This was examined with a specific focus on regions with high utilization of healthcare resources, such as Australia, Europe, Japan and North America? Secondly, what are the key drivers of economic burden in moderate-to-very severe COPD?
Materials and Methods
Literature Search
This SLR was conducted using processes similar to those outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelinesCitation6 to identify articles assessing both the economic and/or humanistic burden of COPD. This review summarizes the evidence of COPD’s economic burden only; humanistic outcomes will be reported in another publication. Searches were conducted to capture publications of interest from January 1, 2006 to November 14, 2016 using the electronic literature databases Excerpta Medica Database (Embase), via embase.com, MEDLINE (via embase.com) (Supplementary Table 1) and MEDLINE In-Process (via ncbi.nlm.nih.gov/pubmed) (Supplementary Table 2).
Supplemental grey literature searches of proceedings from the following relevant conferences that took place in 2015 and 2016 were also conducted: European Respiratory Society (ERS), American Academy of Allergy, Asthma, and Immunology (AAAAI), American Thoracic Society (ATS) and International Society for Pharmacoeconomics and Outcomes Research (ISPOR).
Bibliographies of identified SLRs on the economic burden of COPD were examined for any additional relevant publications and to validate the electronic searches.
Study Selection
During the first level of review, titles and abstracts were screened by two investigators independently using pre-defined inclusion and exclusion criteria (Supplementary Table 3). To be included, articles needed to be English-language observational studies published between January 1, 2006 and November 14, 2016 examining adult patients with moderate-to-very severe COPD (defined as post-bronchodilator forced expiratory volume in 1 s/forced vital capacity [FEV1/FVC] of <0.70, plus 50%≤FEV1<80% predicted [moderate], 30%≤FEV1<50% predicted [severe], or FEV1<30% [very severe], or in accordance with GOLD recommendations or other measures employed by investigators), or with a history of frequent exacerbations (≥2 exacerbations in the previous year that required treatment with oral/systemic corticosteroids and/or antibiotics) or exacerbation-related hospitalizations, in the context of healthcare resource utilization (HRU) and costs. Full-text articles for abstracts deemed to be relevant during the first level of review were retrieved and reviewed. Data were restricted to nine countries of interest: Australia, Canada, France, Germany, Italy, Japan, Spain, the United Kingdom (UK), and the United States (US). None of the exclusion criteria and all protocol-specified inclusion criteria needed to be met for inclusion. All rejected records were re-reviewed as a quality-assurance step. At both review stages, any discrepancies were resolved through discussion between the two reviewers and/or by a third, more senior, investigator.
Data Extraction and Synthesis
A standardized data extraction template was used to collect key data elements from the Consolidated Standards of Reporting Trials (CONSORT) checklist (www.consort-statement.org), including study type, study characteristics, population/subpopulations of interest, patient characteristics and categories of outcomes reported. Each entry was validated by a second researcher and a third, more senior, investigator was involved as a quality-assurance step to confirm extractions or resolve disagreements.
Given the nature of the data, it was not appropriate to conduct a quantitative analysis; however, studies were grouped according to the type of economic outcome (direct costs, costs per exacerbation/hospitalization, indirect costs and HRU). Throughout this manuscript, costs are presented as mean (standard deviation [SD]) unless otherwise indicated.
Where possible, data were also grouped according to population characteristics: those with moderate-to-very severe COPD as defined by FEV1% predicted, and/or those with a history of exacerbations and moderate-to-very severe COPD not defined by FEV1% predicted.
Although no formal quality assessment was conducted on these economic studies, aspects related to the quality of the outcomes of these studies were considered in our interpretation of the evidence, including, for example, sample size and study design.
Results
Literature Search
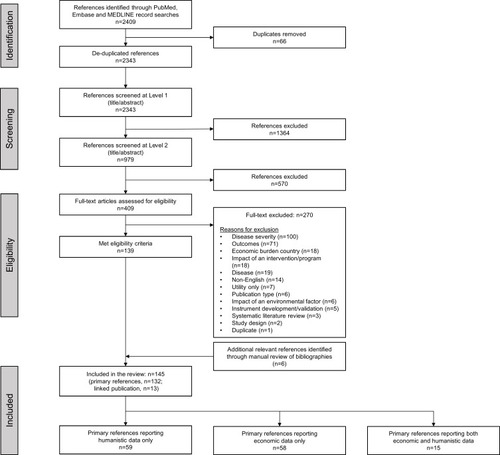
After duplicates were removed, the electronic database searches yielded 2343 unique publications (). Of these, 979 passed the initial title/abstract screening step, and 409 passed the second level of title and abstract screening. A total of 100 publications were excluded at this stage for not reporting on moderate-to-very severe COPD. Overall, 139 publications met the eligibility criteria for inclusion. An additional six publications were identified through manual review of bibliographies, giving a total of 145 publications reporting data on the humanistic and/or economic burden associated with moderate-to-very severe COPD. The 73 primary publications that reported on COPD’s economic burden are included in this manuscript (), while studies reporting on humanistic burden will be summarized in a separate publication.
Table 1 Summary of Included Studies (n=73 Studies)
Figure 1 Identification of studies for inclusion in the systematic literature review (following systematic processes outlined in PRISMA guidelines).
Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
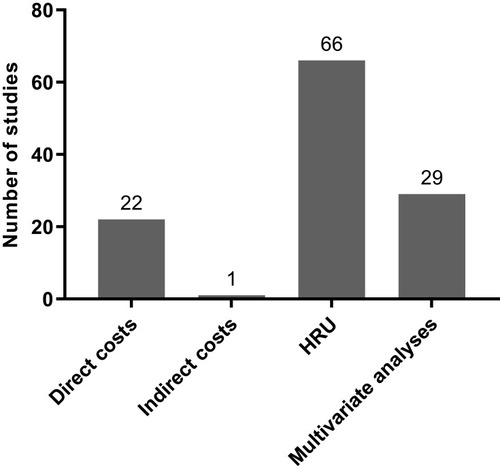
Most of the studies (94%) reported on data from either Europe or North America, with 3% (n=2) reporting on data from Japan and 4% (n=3) from Australia (). Of the 73 studies, most reported on HRU (n=66), followed by direct costs (n=22) and indirect costs (n=1) (). In total, 29 publications reported multivariate data on drivers/predictors of costs and/or HRU ().
Figure 2 Location of included studies.
Abbreviations: UK, United Kingdom; US, United States.
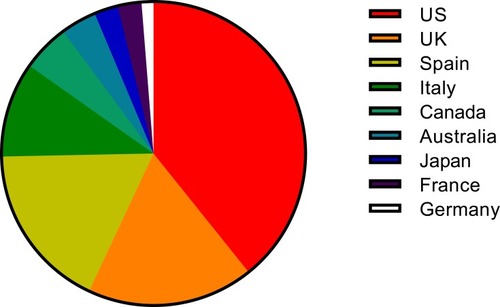
Figure 3 Number of studies reporting on each outcome.
Economic Burden of Moderate-to-Very Severe COPD
HRU
In total, 66 studies reported on HRU, including data regarding hospital admission and length of stay, general practice/primary care visits and intensive care unit (ICU) admission. While more details of HRU in the included studies are included in Supplementary Table 4, in the interests of brevity we have chosen to focus this section on the economic burden of care in the primary, secondary and ICU settings. It must be noted, however, that the studies captured in this review were heterogeneous in nature and are thus challenging to summarize.
In the studies that reported annual hospitalization rates according to COPD severity, COPD-related hospitalizations occurred at a mean annual rate of between 0 and 0.57 in patients with moderate COPD (50%≤FEV1<80% predicted).Citation7–Citation11 Patients with severe COPD (30%≤FEV1<50% predicted) experienced between 0 and 0.44 mean COPD-related hospitalizations per year, while patients with very severe COPD (FEV1<30% predicted) were hospitalized more frequently, from 0 to 0.88 times per year.Citation7–Citation11 In studies where patients’ disease severity was not specified, the highest mean rate of COPD-related annual hospitalizations reported was 1.78 in a population of Spain-based patients who experienced acute exacerbations leading to hospital admission.Citation12 Conversely, the lowest mean rate of COPD-related annual hospitalizations reported was 0.1, in a Spain-based cohort of patients who had experienced <2 exacerbations in the previous year.Citation13
The mean number of annual general practitioner (GP) or primary care visits also varied widely, both within and between COPD severity subgroups. The mean number of visits per patient per year (PPPY) ranged from 2.33 to 12.99 for mild COPD (FEV1≥80% predicted), and from 2.33 to 13.0 for moderate COPD (2.33 visits PPPY was described for patients with “mild-to-moderate COPD” [FEV1≥50% predicted]).Citation8,Citation11,Citation14–Citation17 Patients with severe COPD seemed to visit their GP more frequently, from 2.8 to 15.06 times per year.Citation8,Citation11,Citation14–Citation17 Fewer studies reported the mean number of primary care visits for patients with very severe COPD, but in those that did, the frequency ranged from 3.67 to 12.22 per year.Citation8,Citation11,Citation15 The highest number of GP visits reported was 15.94 per year in a UK-based cohort of patients who experienced ≥2 COPD exacerbations that were moderate-to-severe in severity.Citation18
Only two studies reported length of hospital stay according to COPD severity. One UK-based study reported little variability according to disease severity, with a median stay of 5 days irrespective of whether the patient’s COPD was defined as mild, moderate or severe.Citation11 Length of stay increased to a median of 6 days for patients with very severe disease (FEV1<30% predicted) in this study.Citation11 A study conducted in Spain observed a difference according to COPD severity, with mean length of stay being 8.8 days for patients with mild disease and 16.7 days for patients with severe disease.Citation14 In studies that did not report length of stay according to disease severity, the shortest mean duration reported was 3.24 days (for patients with no diastolic dysfunction) in a US-based studyCitation19 and the longest was 13.2 days in a Canada-based study.Citation20 ICU admission rates were not reported according to disease severity, but ranged from 5% of all hospitalized exacerbations in a study conducted in SpainCitation12 to 19% of all hospitalized exacerbations in a US-based study.Citation21
It is also important to note that the review identified several studies showing increased COPD-associated HRU with exacerbation frequency and the severity of COPD symptoms, particularly breathlessness/dyspnea. Exacerbations are a key driver of HRU by patients with COPD and studies captured in this SLR indicated that patients who experienced more exacerbations had more frequent primary care interactions,Citation11,Citation18,Citation22,Citation23 visits to the emergency department (ED),Citation22,Citation23 hospitalizationsCitation13,Citation18,Citation22–Citation25 and admissions to the ICUCitation13,Citation22 than patients with fewer exacerbations did. Similarly, a retrospective study conducted in the UK primary care setting noted that the rate of hospitalization for a severe exacerbation within a 24-month observation period was 0.12 for patients with moderate breathlessness, increasing to 0.14 and 0.19 for patients with severe and very severe breathlessness, respectively.Citation10 A similar trend was noted for GP home visits, though rates for GP surgery visits were slightly higher for patients with moderate breathlessness (13.00) than those with very severe breathlessness (12.22).Citation10
Direct Costs
Direct costs were reported by a total of 22 studies and a full summary of these results is presented in Supplementary Table 5. In the interests of brevity, we focus here on mean costs PPPY and mean costs per exacerbation, though differences in currencies and cost years mean that comparisons should be interpreted with caution.
In total, nine studies presented mean costs PPPY and demonstrated that costs can vary widely across and within countries, and according to patient or disease characteristics.Citation7,Citation15,Citation18,Citation23,Citation24,Citation26–Citation29 The lowest mean costs PPPY were reported for a population of patients with mild COPD in Italy: €1047 PPPY (cost year, 2004).Citation7 The highest costs reported were also found in Italy, not unexpectedly for patients with very severe COPD, whose mean costs PPPY amounted to €38,820 (cost year, not reported [NR]).Citation26
Three studies specifically reported costs according to disease severity, demonstrating clear trends. In two studies based in the UK, costs PPPY increased from £2012–£2087 in patients with moderate disease, to £2092–£2290 in patients with severe disease and to £2258–£2639 in patients with very severe disease (cost year, 2011).Citation10,Citation18 A similar trend was observed in Italy: costs PPPY increased from €2319 in patients with moderate disease to €3752 in patients with severe disease and to €5033 in patients with very severe disease (cost year, 2004).Citation7
Three studies presented mean costs PPPY according to patient or disease characteristics. A study based in Japan observed a large discrepancy in costs according to presence and severity of dyspnea: patients with moderate-to-severe dyspnea (Medical Research Council [MRC] score ≥2) had mean costs PPPY of €6348, compared with only €2797 for patients with mild or no dyspnea (MRC score <2; cost year, 2015).Citation27 A retrospective study based in the UK healthcare setting also noted higher costs PPPY for patients with more severe breathlessness, but the differences according to severity were smaller: £2258 for very severe breathlessness, £2151 for severe breathlessness and £2012 for moderate breathlessness.Citation10 A trend according to increased costs with comorbidities was also noted; as an example, patients with heart disease had higher costs PPPY compared with patients without heart disease in a study conducted in Spain: €2898.66 vs €1672.64, respectively (cost year, NR).Citation28
This SLR also found that annual costs per patient generally increased according to exacerbation frequency. A study conducted in the UK (cost year, 2011), for example, noted that annual per patient costs related to COPD increased from £1523 in patients with no exacerbations, to £2405 in patients with one exacerbation, and to £3396 in patients with ≥2 exacerbations, in the 12 months following study entry.Citation18 The impact of exacerbation history as a driver of direct costs will be explored in greater detail in a later section of this review.
Exacerbations account for a substantial proportion of the direct costs associated with COPD, and this SLR captured seven studies that reported mean costs per exacerbation,Citation20,Citation21,Citation24,Citation29–Citation32 but few studies reported this outcome according to exacerbation severity. Two studies reported mean costs per moderate exacerbation (characterized by the need for management with COPD-specific antibiotics or oral corticosteroids, or a medical diagnosis), which ranged from $269 in the US (US dollars [USD]; cost year, 2011)Citation29 to $641 in Canada (Canadian dollars [CAD]; cost year, 2006).Citation20 Where mean costs were reported for severe exacerbations (defined by the need for hospitalization),Citation20,Citation21,Citation24,Citation29–Citation32 costs were higher than those reported for moderate exacerbations. The lowest reported mean cost for a hospitalized exacerbation was $3164 in Italy (USD; cost year, 2013),Citation30 while the highest was substantially greater: $18,120 in the US (USD; cost year, 2011).Citation29 The wide range of costs across countries is notable, even when being mindful of differences in currencies and cost years.
Although cross-trial comparisons are challenging due to differences in currencies and cost years, this SLR indicates that, consistent with the higher rates of HRU noted with increasingly severe disease and COPD symptoms, and more frequent exacerbations, direct costs generally increase alongside COPD and symptom severity, and exacerbation frequency. Specific independent drivers of direct costs will be explored by examining multivariate analyses in a later section of this review.
Indirect Costs
Only one study on indirect costs, conducted in Spain, was identified.Citation28 This study reported on outpatients with moderate-to-very severe COPD (FEV1 <80% predicted) and found a statistically significant difference in the cost of sick leave days PPPY in those without heart disease (€76.61) compared with those with heart disease (€38.33 [cost year, NR]; p<0.05). This SLR did not identify any studies that explored potential predictors of indirect costs in patients with moderate-to-very severe COPD.
Key Drivers of Economic Burden
This SLR identified 29 studies in which multivariate analyses were performed to explore potential drivers of economic burden in patients with moderate-to-very severe COPD. Of these studies, 24 reported multivariate analyses of HRU outcomes (; Supplementary Table 6) and seven reported direct costs (; Supplementary Table 7).
Table 2 Multivariate Analyses of HRU (n=24 Studies)
Table 3 Multivariate Analyses of Direct Costs (n=7 Studies)
HRU
Independent drivers of more frequent hospitalization for a COPD- or respiratory-related cause included increasing disease severity,Citation33 restricted lung functionCitation33 and higher baseline C-reactive protein concentrations.Citation34 Increasingly severe disease was also an independent driver of more frequent non-COPD-related hospitalizations,Citation35 as were the number of previous exacerbations, use of short-acting β2-agonists (SABA) and use of long-term oxygen therapy (LTOT) among other variables.Citation25
Factors independently associated with longer hospital stays for a COPD exacerbation were numerous and were reported in six studies.Citation31,Citation32,Citation36–Citation39 Drivers included the presence of comorbidities such as strokeCitation31 and some cardiac abnormalities,Citation31,Citation32 advancing age and being female.Citation36 Furthermore, specific care-related factors such as a hospital’s size, location or type were also found to be independent drivers of length of stay. Increased hospital size, for example, was associated with longer stays but admission to a teaching hospital was associated with shorter stays compared with a non-teaching hospital.Citation36
Some cardiac abnormalities, such as congestive heart failure and dysrhythmia,Citation32 alongside pneumonia, anemia and anxiety or depression among other comorbidities, were identified as independent drivers of ICU admission.Citation32 Severe COPD (indicated by the use of home oxygen, oral/intravenous steroids, vasopressors or ventilation) and higher B-type natriuretic peptide levels were both found to be drivers of longer ICU stays.Citation38
Eight studies analyzed potential drivers of COPD-related readmission to hospital for patients admitted with an exacerbation of COPD.Citation39–Citation46 Among those that explored readmission for another exacerbation in the shorter term (within 30 days or within 2 months), history of coronary heart disease,Citation46 hospitalizations in the previous yearCitation44 and baseline FEV1<30% predicted (vs ≥50% predicted)Citation43 were identified as independent drivers of increased readmission risk, but this is not an exhaustive summary. Interestingly, though perhaps not surprisingly, taking 150 mins of moderate-to-strenuous exercise each week was independently associated with a lower risk of readmission for an exacerbation within 30 days.Citation44 Regular physical activity was also independently associated with lower readmission risk in another study.Citation39 Studies that assessed risks of readmission for another exacerbation in the longer term (with follow-ups ranging from 1 to 6 years) identified congestive heart disease and pulmonary heart disease as independent drivers of increased risk.Citation41 Notably, ischemic heart disease and cardiac arrhythmia were also identified as drivers of increased readmission risk, but only in female patients.Citation41 Being maleCitation40,Citation42 and having a history of previous hospital staysCitation40 were similarly associated with an increased risk of readmission. Factors identified as drivers of lower readmission risk for a COPD-related cause in the long term included Hispanic ethnicity and diabetes.Citation40
The majority of factors found to be independently associated with an increased risk of readmission for any cause were comorbidities, ranging from liver disease, paraplegia and substance abuse,Citation47 to neurologic conditions and heart disease.Citation31 Having an increased number of comorbid conditions was also associated with an increased risk of readmission.Citation31
For drivers of primary care utilization, associations between more frequent GP visits and being female, suffering with obesity, depression, anxiety or other comorbidities were noted in one retrospective cohort study.Citation10 Emergency department visits of any cause were found to be independently associated with COPD severity,Citation35 age, comorbidity, exacerbation frequencyCitation10 and emotional intelligence,Citation48 among other factors. One study reported on potential drivers of LTOT and found that female gender, white race (vs black or other races), low socioeconomic status and a higher Elixhauser Comorbidity score (among other variables) were independently associated with an increased likelihood of receiving such therapy.Citation49
A cross-sectional study among patients with COPD in Spain identified drivers of high HRU, defined as having had one hospital admission for a COPD exacerbation, ≥2 ED visits for COPD exacerbations or ≥2 unscheduled outpatient visits related to COPD in the previous year. Independent drivers included London Chest Activity of Daily Living (LCADL) scale score, leukocyte count and fibrinogen level.Citation50
Direct Costs
Increasingly severe dyspnea was identified as an independent driver of higher annual COPD management costs per patient,Citation27 while older age, receipt of appropriate bronchodilator therapy and higher pre-index COPD-related costsCitation51 were found to be independent predictors of higher COPD-related costs per patient at 6 months after discharge. In two retrospective cohort studies that assessed potential drivers of annual exacerbation costs for patients with chronic bronchitis, numerous independent drivers were identified. Regarding increased annual exacerbation costs per patient, these included being of black race, high income, comorbid cardiovascular disease and comorbid diabetes, among other factors.Citation23 Independent drivers of higher costs per individual exacerbation (of any severity) in patients with chronic bronchitis included Deyo-Charlson’s Comorbidity Index score, the number of exacerbations during the previous year and the number of prescription fills for short-acting muscarinic antagonist (SAMA) therapy, among other factors.Citation29
Potential drivers of costs per hospitalized exacerbation were assessed in three studies conducted in the US.Citation31,Citation32,Citation36 Independent predictors of higher costs included cardiac comorbidities, such as congestive heart failure and ischemic heart disease,Citation32 the nature of the patient’s COPD (emphysema vs chronic bronchitis), as well as advancing age,Citation36 Hispanic race (vs white race), and ICU treatment,Citation31,Citation36 among other factors. Severity score was also described as a predictor of costs, but the nature of this association was unclear in the source publication.Citation31
Discussion
It is important to understand the economic burden associated with moderate-to-very severe COPD and its treatment, particularly given that COPD presents major challenges for patients, healthcare providers and society. Optimal management of patients, their symptoms and exacerbations is one such challenge. This SLR investigated the current impact of COPD on HRU needs and both direct and indirect costs, based on a broad definition of patients whose COPD severity was typically confirmed by FEV1% predicted or assumed (from exacerbation history) to be at least moderate. The analysis was intentionally limited to nine industrialized countries of interest (and to a 10-year time frame) to ensure inclusion of evidence from settings where patients were likely to be receiving guideline-recommended therapeutic management; the US was the most well-represented country.
Fewer studies reported costs compared with those that provided HRU evidence and, considering the inherent variation in geographical location, timing and methodology between the available studies, cross-study comparisons should be interpreted with caution. Overall, however, direct costs were found to generally increase with COPD severity, exacerbation frequency and severity of COPD symptoms. The SLR also found higher rates of HRU, in terms of hospitalization, length of hospital stay and primary care interactions, for patients with more severe COPD, more frequent COPD exacerbations and more severe COPD symptoms.
As shown by the numerous studies that performed multivariate analyses, independent drivers of HRU and costs are diverse. Factors related to disease severity, the frequency and severity of COPD exacerbations, comorbidities and treatment history (among others) were significantly associated with elements of HRU, ranging from hospitalization to LTOT. More severe COPD and a history of frequent exacerbations, for example, were each positively associated with an increased likelihood of hospitalization.Citation25,Citation33,Citation35 Disease severity was also identified as a driver of ED visits,Citation35 and longer hospital or ICU stays.Citation38 These multivariate data support trends reported in other studies, captured both in this SLR and others in the broader literature. As an example, a cross-sectional survey conducted across France, Germany, Italy, Spain and the UK found that moderate-to-severe dyspnea was associated with a significant disease burden in patients with COPD, and was associated with significantly more frequent hospitalizations, specialist and physician consultations, LTOT use and pulmonary rehabilitation (all p<0.0001).Citation52
Examining multivariate analyses of direct costs per patient for COPD also identified dyspnea severity,Citation27 and exacerbation frequencyCitation29 and severityCitation23 as significant drivers. This was perhaps to be expected: a more intensive treatment regimen may be required to manage symptoms and/or exacerbations and thus is likely to carry a burden of increased costs. These results are in keeping with the SLR of economic burden in COPD by Srivastava et al (2015), which found that direct and indirect costs per patient increased with symptoms, dyspnea severity and disease duration.Citation53 The data are also supported by results reported by other studies captured in this SLR that did not employ multivariate analyses: trends for higher costs according to more severe disease were noted in both ItalyCitation7,Citation26 and the UK.Citation10,Citation18
Other key drivers identified through multivariate analysis as predictors of economic burden in moderate-to-very severe COPD included the number of previous exacerbations, as well as the presence and types of comorbidities. Comorbidities have frequently been associated with significantly higher costs for patients with COPD in the wider literature.Citation53–Citation56 An SLR of 12 studies from the US and across Europe/Asia that analyzed the excess costs of comorbidities in COPD found that pneumonia, cardiovascular disease and diabetes were associated with the highest excess costs.Citation55 This SLR supports these findings: comorbid diabetes and comorbid cardiovascular disease were found to be potential predictors of annual exacerbation-related costsCitation23 and pneumonia was found to be an independent predictor of the cost of exacerbation-related hospitalization.Citation32 These findings highlight the importance of careful management of comorbidities alongside optimal COPD-specific therapy, to minimize HRU and associated costs.
A limitation of this study was perhaps the paucity of data available on indirect costs. However, among the studies identified by the SLR was a 2016 population-based survey across 12 countries (including the US, the UK, Germany, Italy and Spain), which described how indirect costs were several times greater than direct costs in many countries.Citation30 This highlights the extreme, and often hidden, economic burden carried by loss of productivity and absenteeism. A US-based survey focusing on all COPD severities (not just moderate-to-very severe) observed that COPD-attributable absenteeism accounted for costs of approximately $3.9 billion dollars in 2010, with an estimated 16.4 million work days lost due to COPD; these costs are expected to rise in coming years.Citation57 With their clear impact on economic burden, the indirect costs of COPD certainly warrant further investigation across regions and healthcare systems.
This study employed a pragmatic approach and allowed a flexible definition of moderate-to-very-severe COPD, though this automatically introduced a degree of between-study heterogeneity in the SLR, which made comparing data between studies more challenging. Nonetheless, many of the key outcomes were consistently demonstrated across studies, and, where possible, we qualitatively compared HRU and costs according to disease severity. The trends observed and inferences made through qualitative analysis were supported by multivariate analysis studies captured by this SLR, which were specifically designed to identify independent predictors of COPD’s economic burden.
This study focused on moderate-to-very severe COPD: studies examining only mild COPD were excluded. Although widening the search parameters may have delivered a more comprehensive dataset, COPD is underdiagnosed in its early stages. As many patients do not become known to healthcare systems until their disease has advanced to moderate-to-severe stages,Citation58 it is likely that the parameters employed by this SLR captured the majority of patients with a confirmed COPD diagnosis.
This SLR provides detailed evidence of the considerable real-world economic burden carried by moderate-to-very severe COPD, especially for patients with a history of exacerbations and/or more severe COPD, despite the availability of efficacious treatments and well-defined guidance on their use.
With worldwide healthcare budgets facing increasing financial pressures, understanding the economic burden of diseases such as COPD is essential to ensure that the disease is managed efficiently and that emerging therapies are made available to the patients who need them. Further progress in the management of COPD exacerbations and HRU is required to improve patient care and to reduce the associated strain on healthcare budgets around the world.
Abbreviations
AAAAI, American Academy of Allergy, Asthma, and Immunology; ATS, American Thoracic Society; CAD, Canadian dollar; CONSORT, Consolidated Standards of Reporting Trials; COPD, chronic obstructive pulmonary disease; ED, emergency department; ERS, European Respiratory Society; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GP, general practitioner; HRU, healthcare resource utilization; ICS, inhaled corticosteroid; ICU, intensive care unit; ISPOR, International Society for Pharmacoeconomics and Outcomes Research; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LCADL, London Chest Activity of Daily Living; LTOT, long-term oxygen therapy; MRC, Medical Research Council; NR, not reported; PPPY, per patient per year; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; SLR, systematic literature review; UK, United Kingdom; US, United States.
Author Contributions
All authors contributed to the study conceptualization, data sourcing, data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare the following conflicts of interest during the last 3 years in relation to this article: SZ and ASI are employees of, and hold shares in, GlaxoSmithKline plc.; ASI is also a part-time unpaid professor at McMaster University, Canada. Evidera (II) was contracted by GlaxoSmithKline plc. to conduct the systematic literature review but was not paid for the development of this manuscript. MR is an employee of Xcenda UK and was previously employed by Evidera and contracted by GlaxoSmithKline plc. to conduct the systematic literature review but was not paid for the development of this publication. DK is a former GlaxoSmithKline plc. employee and is currently employed by Forest Systematic Reviews Ltd, contracted by GlaxoSmithKline plc. The authors report no other conflicts of interest in this work.
Acknowledgments
This study was funded by GlaxoSmithKline plc. (study HO-16-16282). The authors thank Juliet Kenny for her assistance in the conception of the study and interpretation of the data. Editorial support (in the form of writing assistance, collating author comments, assembling tables/figures, grammatical editing and referencing) was provided by Fiona Scott, PhD, and Molly Macpherson, BSc, of Gardiner-Caldwell Communications (Macclesfield, UK), and was funded by GlaxoSmithKline plc.
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2019 Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf. Accessed 311, 2019.
- AdeloyeD, ChuaS, LeeC, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. doi:10.7189/jogh.05.02041526755942
- GuarascioAJ, RaySM, FinchCK, SelfTH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. doi:10.2147/CEOR.S3432123818799
- LøkkeA, HilbergO, TønnesenP, IbsenR, KjellbergJ, JennumP. Direct and indirect economic and health consequences of COPD in Denmark: a national register-based study: 1998–2010. BMJ Open. 2014;4(1):e004069. doi:10.1136/bmjopen-2013-004069
- WackerME, JörresRA, KarchA, et al. Assessing health-related quality of life in COPD: comparing generic and disease-specific instruments with focus on comorbidities. BMC Pulm Med. 2016;16(1):70.27160582
- MoherD, LiberatiA, TetzlaffJ, AltmanDG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.100009719621072
- KolevaD, MotterliniN, BanfiP, GarattiniL. Healthcare costs of COPD in Italian referral centres: a prospective study. Respir Med. 2007;101(11):2312–2320. doi:10.1016/j.rmed.2007.06.02017681461
- MerinopoulouE, Raluy-CalladoM, RamagopalanS, MacLachlanS, KhalidJM. COPD exacerbations by disease severity in England. Int J Chron Obstruct Pulmon Dis. 2016;11:697–709. doi:10.2147/COPD.S10025027099486
- MullerovaH, HanMK, BaxterR, GOLDDK. 2013 COPD classification: a comparison with GOLD 2011 and COPD outcomes in the UK Clinical Practice Research Datalink (CPRD) COPD cohort. Am J Respir Crit Care Med. 2014;189:A5965. doi:10.1164/rccm.201306-1150OC
- PunekarYS, WurstK, ShuklaA. Resource use and costs up to two years post diagnosis among newly diagnosed COPD patients in the UK primary care setting: a retrospective cohort study. COPD. 2015;12(3):267–275. doi:10.3109/15412555.2014.93395325093809
- ThomasM, RadwanA, StonhamC, MarshallS. COPD exacerbation frequency, pharmacotherapy and resource use: an observational study in UK primary care. COPD. 2014;11(3):300–309. doi:10.3109/15412555.2013.84167124152210
- Bustamante-FermoselA, De Miguel-yanesJM, Duffort-FalcóM, MunozJ. Mortality-related factors after hospitalization for acute exacerbation of chronic obstructive pulmonary disease: the burden of clinical features. Am J Emerg Med. 2007;25(5):515–522. doi:10.1016/j.ajem.2006.09.01417543654
- ValidoA, Gomez-BasteroA, AlmadanaV, LuqueE, MontemayorT. Clinical and functional differences, exercise capacity and physical activity among frequent and not frequent exacerbators in COPD patients. Eur Respir J. 2014;44(Suppl 58):P4883. doi:10.1183/09031936.00003814
- MartínA, Rodríguez-González MoroJM, IzquierdoJL, GobarttE, de LucasP. Health-related quality of life in outpatients with COPD in daily practice: the VICE Spanish Study. Int J Chron Obstruct Pulmon Dis. 2008;3(4):683–692. doi:10.2147/COPD.S479119283915
- PunekarYS, LandisSH, BonarK, LeH. Health care utilisation and costs among COPD patients newly prescribed maintenance therapy in the United Kingdom (UK). Thorax. 2015b;70:A142–A143. doi:10.1136/thoraxjnl-2015-207770.269
- YeoJ, KarimovaG, BansalS. Co-morbidity in older patients with COPD–its impact on health service utilisation and quality of life, a community study. Age Ageing. 2006;35(1):33–37. doi:10.1093/ageing/afj00216364931
- MapelDW, DutroMP, MartonJP, WoodruffK, MakeB. Identifying and characterizing COPD patients in US managed care. A retrospective, cross-sectional analysis of administrative claims data. BMC Health Serv Res. 2011;11:43. doi:10.1186/1472-6963-11-4321345188
- PunekarYS, ShuklaA, MüllerovaH. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int J Chron Obstruct Pulmon Dis. 2014;9:65–73. doi:10.2147/COPD24426781
- AbusaidGH, BarbagelataA, TueroE, MahmoodA, SharmaG. Diastolic dysfunction and COPD exacerbation. Postgrad Med. 2009;121(4):76–81. doi:10.3810/pgm.2009.07.203319641273
- MittmannN, KuramotoL, SeungSJ, HaddonJM, Bradley-KennedyC, FitzgeraldJM. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med. 2008;102(3):413–421. doi:10.1016/j.rmed.2007.10.01018086519
- XuX, KnightT, BaikR, TuX, ParkerJM. Patient characteristics, health resource utilization (HRU) and treatment costs of chronic obstructive pulmonary disease (COPD) patients treated in hospital facilities for exacerbations. Am J Respir Crit Care Med. 2012;185:A3047.
- DalalAA, PatelJ, D’SouzaA, FarrellyE, NagarS, ShahM. Impact of COPD exacerbation frequency on costs for a managed care population. J Manag Care Spec Pharm. 2015;21(7):575–583. doi:10.18553/jmcp.2015.21.7.57526108382
- PasqualeMK, SunSX, SongF, HartnettHJ, StemkowskiSA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. doi:10.2147/COPD.S3699723152680
- BlasiF, CesanaG, ContiS, et al. The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patients. PLoS One. 2014;9(6):e101228. doi:10.1371/journal.pone.010122824971791
- MiravitllesM, CalleM, Alvarez-GutierrezF, GobarttE, LópezF, MartinA. Exacerbations, hospital admissions and impaired health status in chronic obstructive pulmonary disease. Qual Life Res. 2006;15(3):471–480. doi:10.1007/s11136-005-3215-y16547786
- VitaccaM, BianchiL, BazzaA, CliniEM. Advanced COPD patients under home mechanical ventilation and/or long term oxygen therapy: italian healthcare costs. Monaldi Arch Chest Dis. 2011;75(4):207–214. doi:10.4081/monaldi.2011.20822462308
- SmallM, HolbrookT, WoodR, MullerovaH, NayaI, PunekarYS. Prevalence and burden of dyspnoea among COPD patients in Japan. Int J Clin Pract. 2016;70(8):676–681. doi:10.1111/ijcp.2016.70.issue-827396989
- de Miguel-díezJ, Carrasco-GarridoP, Rejas-GutierrezJ, et al. The influence of heart disease on characteristics, quality of life, use of health resources, and costs of COPD in primary care settings. BMC Cardiovasc Disord. 2010;10:8. doi:10.1186/1471-2261-10-820167091
- AbudaggaA, SunSX, TanH, SolemCT. Exacerbations among chronic bronchitis patients treated with maintenance medications from a US managed care population: an administrative claims data analysis. Int J Chron Obstruct Pulmon Dis. 2013;8:175–185. doi:10.2147/COPD.S4043723589684
- FooJ, LandisSH, MaskellJ, et al. Continuing to Confront COPD International Patient Survey: economic impact of COPD in 12 countries. PLoS One. 2016;11(4):e0152618. doi:10.1371/journal.pone.015261827092775
- RobertsMH, BorregoM, PetersenH, KharatA, BlanchetteC. Estimating the burden and course of severe COPD exacerbations in the U.S. Hispanic population. Am J Respir Crit Care Med. 2011a;183:A1496.
- SilverH, BlanchetteCM, RobertsM, PetersenH, StCharlesME. Prevalence of comorbidities in patients hospitalized for COPD exacerbations and impact on impatient mortality and hospital expenditures. Am J Respir Crit Care Med. 2010;181:A5943. doi:10.1164/rccm.200904-0493OC
- Garcia-AymerichJ, Serra PonsI, ManninoDM, MaasAK, MillerDP, DavisKJ. Lung function impairment, COPD hospitalisations and subsequent mortality. Thorax. 2011;66(7):585–590. doi:10.1136/thx.2010.15287621515553
- GallegoM, PomaresX, CapillaS, et al. C-reactive protein in outpatients with acute exacerbation of COPD: its relationship with microbial etiology and severity. Int J Chron Obstruct Pulmon Dis. 2016;11:2633–2640. doi:10.2147/COPD27799762
- DhamaneAD, WittEA, SuJ. Associations between COPD severity and work productivity, health-related quality of life, and health care resource use: a cross-sectional analysis of national survey data. J Occup Environ Med. 2016;58(6):e191–e197. doi:10.1097/JOM.000000000000073527206123
- StanfordRH, ShenY, McLaughlinT. Cost of chronic obstructive pulmonary disease in the emergency department and hospital: an analysis of administrative data from 218 US hospitals. Treat Respir Med. 2006;5(5):343–349. doi:10.2165/00151829-200605050-0000516928147
- MahmudN, McNabb-BalterJ, ChanWW. The impact of gastroesophageal reflux on the length of hospital stay for COPD exacerbations: a report of the nationwide inpatient sample. Gastroenterology. 2015;148(4Suppl. 1):S606. doi:10.1016/S0016-5085(15)32044-8
- VallabhajosyulaS, HaddadTM, SundaragiriPR, et al. Role of B-type natriuretic peptide in predicting in-hospital outcomes in acute exacerbation of chronic obstructive pulmonary disease: a five-year retrospective analysis. Am J Respir Crit Care Med. 2015;191:A2938.
- EscarrabillJ, TorrenteE, EsquinasC, et al. Clinical audit of patients hospitalized due to COPD exacerbation. MAG-1 Study. Arch Bronconeumol. 2015;51(10):483–489. doi:10.1016/j.arbres.2014.06.02325447590
- McGhanR, RadcliffT, FishR, SutherlandER, WelshC, MakeB. Predictors of rehospitalization and death after a severe exacerbation of COPD. Chest. 2007;132(6):1748–1755. doi:10.1378/chest.06-301817890477
- ChenY, LiQ, JohansenH. Age and sex variations in hospital readmissions for COPD associated with overall and cardiac comorbidity. Int J Tuberc Lung Dis. 2009;13(3):394–399.19275803
- SuissaS, Dell’AnielloS, ErnstP. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-20151822684094
- QuintanaJM, EstebanC, Garcia-GutierrezS, et al. Predictors of hospital admission two months after emergency department evaluation of COPD exacerbation. Respiration. 2014;88(4):298–306. doi:10.1159/00036599625228470
- NguyenHQ, ChuL, Liu I-LA, et al. Higher level of regular physical activity is associated with lower risk of 30-day readmissions in patients with COPD. Am J Respir Crit Care Med. 2014;189:A2452. doi:10.1164/rccm.201306-1150OC
- GatheralT, KumarN, SansomB, et al. COPD-related bronchiectasis; independent impact on disease course and outcomes. COPD. 2014;11(6):605–614. doi:10.3109/15412555.2014.92217424983298
- NantsupawatT, LimsuwatC, NugentK. Factors affecting chronic obstructive pulmonary disease early rehospitalization. Chron Respir Dis. 2012;9(2):93–98. doi:10.1177/147997231243870322399574
- DuVallS, BrownK, NiciL, et al. Incidence and predictors of hospital readmission among patients with chronic obstructive pulmonary disease in the Department of Veterans Affairs. Chest. 2015;148(4 Suppl):684A. doi:10.1378/chest.2223166
- BenzoRP, KirschJL, DuloheryMM, Abascal-BoladoB. Emotional intelligence: a novel outcome associated with wellbeing and self-management in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2016;13(1):10–16. doi:10.1513/AnnalsATS.201508-490OC26501370
- NishiSP, ZhangW, KuoYF, SharmaG. Oxygen therapy use in older adults with chronic obstructive pulmonary disease. PLoS One. 2015;10(3):e0120684. doi:10.1371/journal.pone.012068425785586
- Garciía-PoloC, Alcázar-NavarreteB, Ruiz-IturriagaLA, et al. Factors associated with high healthcare resource utilisation among COPD patients. Respir Med. 2012;106(12):1734–1742. doi:10.1016/j.rmed.2012.09.00923058483
- TranM, XiangP, RascatiKL, et al. HEDIS quality measure performance and other factors predictive of health care costs following COPD-related admission. Value Health. 2016;19:A122.
- PunekarYS, MullerovaH, SmallM, et al. Prevalence and burden of dyspnoea among patients with chronic obstructive pulmonary disease in five European countries. Pulmonary Ther 2016;2(1):59–72.
- SrivastavaK, ThakurD, SharmaS, PunekarYS. Systematic review of humanistic and economic burden of symptomatic chronic obstructive pulmonary disease. Pharmacoeconomics. 2015;33(5):467–488. doi:10.1007/s40273-015-0252-425663178
- DalalAA, ShahM, LunacsekO, HananiaNA. Clinical and economic burden of patients diagnosed with COPD with comorbid cardiovascular disease. Respir Med. 2011;105(10):1516–1522. doi:10.1016/j.rmed.2011.04.00521684731
- HuberMB, WackerME, VogelmeierCF, LeidlR, WatzH. Excess costs of comorbidities in chronic obstructive pulmonary disease: a systematic review. PLoS One. 2015;10(4):e0123292. doi:10.1371/journal.pone.012329225875204
- ManninoDM, HiguchiK, YuTC, et al. Economic burden of COPD in the presence of comorbidities. Chest. 2015;148(1):138–150. doi:10.1378/chest.14-243425675282
- FordES, MurphyLB, KhavjouO, GilesWH, HoltJB, CroftJB. Total and state-specific medical and absenteeism costs of COPD among adults aged >/= 18 years in the United States for 2010 and projections through 2020. Chest. 2015;147(1):31–45. doi:10.1378/chest.14-097225058738
- LøkkeA, UlrikCS, DahlR, et al. Detection of previously undiagnosed cases of COPD in a high-risk population identified in general practice. COPD. 2012;9(5):458–465. doi:10.3109/15412555.2012.68511822643016
- BuXN, YangT, ThompsonMA, HutchinsonAF, IrvingLB. Changes in the BODE index, exacerbation duration and hospitalisation in a cohort of COPD patients. Singapore Med J. 2011;52(12):894–900.22159933
- Carrasco GarridoP, de Miguel DíezJ, Rejas GutiérrezJ, et al. Negative impact of chronic obstructive pulmonary disease on the health-related quality of life of patients. Results of the EPIDEPOC study. Health Qual Life Outcomes. 2006;4:31. doi:10.1186/1477-7525-4-3116719899
- CollinsEG, HalabiS, LangstonM, SchnellT, TobinMJ, LaghiF. Sexual dysfunction in men with COPD: impact on quality of life and survival. Lung. 2012;190(5):545–556. doi:10.1007/s00408-012-9398-422752718
- DalalAA, ShahM, D’SouzaAO, RaneP. Costs of inpatient and emergency department care for chronic obstructive pulmonary disease in an elderly Medicare population. J Med Econ. 2010a;13(4):591–598. doi:10.3111/13696998.2010.52173420854113
- LindenauerPK, PekowP, GaoS, CrawfordAS, GutierrezB, BenjaminEM. Quality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2006;144(12):894–903. doi:10.7326/0003-4819-144-12-200606200-0000616785478
- DalalAA, ShahM, D’SouzaAO. Economic burden of health care admissions related to chronic obstructive pulmonary disease exacerbations: data from inpatient administrative database. Am J Respir Crit Care Med. 2010b;181:A1492.
- PatelJ, DalalAA, NagarS, D’SouzaAO, ShahM, FarrellyE. Economic burden of frequently and infrequently exacerbating patients with a diagnosis of COPD. Am J Respir Crit Care Med. 2013;187:A1437.
- DhamaneA, WittEA, HernandezG, SuJ. Association between COPD severity and work productivity, quality of life and healthcare resource use. Am J Respir Crit Care Med. 2015;191:A4447.
- DushianthanA, TemblettP, BhattaA. Outcome of a cohort of older population with COPD, admitted with hypercapnaeic respiratory failure and acidosis. Am J Respir Crit Care Med. 2010;181:A1506. doi:10.1164/rccm.200904-0493OC
- EstebanC, ArosteguiI, AburtoM, et al. Chronic obstructive pulmonary disease subtypes. Transitions over time. PLoS One. 2016;11(9):e0161710. doi:10.1371/journal.pone.016171027611911
- GadreS, DuggalA, GuzmanJ. Epidemiological characteristics and outcomes of patients with severe COPD requiring mechanical ventilation. Chest. 2014;146(4 Suppl 2):58A. doi:10.1378/chest.199191124652410
- Garcia-AymerichJ, FélezMA, EscarrabillJ, et al. Physical activity and its determinants in severe chronic obstructive pulmonary disease. Med Sci Sports Exerc. 2004;36(10):1667–1673. doi:10.1249/01.MSS.0000142378.98039.5815595285
- GavazziA, De MariaR, ManzoliL, et al. Palliative needs for heart failure or chronic obstructive pulmonary disease: results of a multicenter observational registry. Int J Cardiol. 2015;184:552–558. doi:10.1016/j.ijcard.2015.03.05625767016
- HuangH, LinI, GoldsteinB, RosielloR, MenzinJ. Rehospitalization rates and mortality among patients with severe chronic obstructive pulmonary disease receiving long-term oxygen therapy in a managed-care setting. Am J Respir Crit Care Med. 2014;189:A3058. doi:10.1164/rccm.201306-1150OC
- KeiltyS, MurphyP, HartN. 1 year UK survival readmission rate in chronic obstructive pulmonary disease (COPD) survivors following acute non-invasive ventilation (NIV). Thorax. 2013;68(Suppl. 3):A47–A48. doi:10.1136/thoraxjnl-2013-204457.95
- LusuardiM, LucioniC, De BenedettoF, MazziS, SanguinettiCM, DonnerCF. GOLD severity stratification and risk of hospitalisation for COPD exacerbations. Monaldi Arch Chest Dis. 2008;69(4):164–169. doi:10.4081/monaldi.2008.37819350838
- MatkovicZ, HuertaA, SolerN, et al. Predictors of adverse outcome in patients hospitalised for exacerbation of chronic obstructive pulmonary disease. Respiration. 2012;84(1):17–26. doi:10.1159/00033546722327370
- PunekarYS, ShuklaA, MuellerovaH. Comparing COPD costs by exacerbation frequency and dyspnoea level in a primary care setting in the United Kingdom. Value Health. 2013;16(7):A723. doi:10.1016/j.jval.2013.08.2259
- PunekarYS, WurstK, ShuklaA. COPD management costs among newly diagnosed COPD patients in the UK primary care setting. Am J Respir Crit Care Med. 2013;187:A4373.
- PunekarYS, ShuklaA, MuellerovaH. Disease management costs associated with COPD patients with infrequent exacerbations in the UK primary care setting. Am J Respir Crit Care Med. 2013;187:A4374.
- MerinopoulouE, Raluy-CalladoM, RamagopalanS, MacLachlanS, KhalidJM. Resource use and exacerbations of chronic obstructive pulmonary disease (COPD) by GOLD categories. Value Health. 2015;18(7):A506–A507. doi:10.1016/j.jval.2015.09.1449
- FitzGeraldJM, HaddonJM, Bradley-KennedyC, KuramotoL, FordGT, RUSIC Study GroupT. The RUSIC Study Group. Resource Use Study in COPD (RUSIC): a prospective study to quantify the effects of COPD exacerbations on health care resource use among COPD patients. Can Respir J. 2007;14(3):145–152. doi:10.1155/2007/92191417464378
- MolinariN, BriandC, VachierI, et al. Hospitalizations for COPD exacerbations: trends and determinants of death. COPD. 2015;12(6):621–627. doi:10.3109/15412555.2015.100793126263032
- PhilipJ, LoweA, GoldM, et al. Using administrative datasets to assist prognostication in chronic obstructive pulmonary disease (COPD). Palliat Med. 2010;24:S25.
- PitassiM, VitaleC, D’AmatoM, StanziolaA, MormileM, MolinoA. Impact of bronchiectasis on duration of hospitalization in patients with exacerbations of COPD. Eur Respir J. 2015;46:PA4701.
- PrettoJJ, McDonaldVM, WarkPA, HensleyMJ. Multicentre audit of inpatient management of acute exacerbations of chronic obstructive pulmonary disease: comparison with clinical guidelines. Intern Med J. 2012;42(4):380–387. doi:10.1111/j.1445-5994.2011.02475.x21395962
- ShortPM, WilliamsonPA, SinganayagamA, AkramA, ChalmersJD, SchembriS. Guideline adherent therapy and reduced mortality and length of stay in adults hospitalised with exacerbations of COPD. Thorax. 2013;68(Suppl. 3):A136. doi:10.1136/thoraxjnl-2013-204457.283
- RobertsCM, StoneRA, LoweD, PurseyNA, BuckinghamRJ. Co-morbidities and 90-day outcomes in hospitalized COPD exacerbations. COPD. 2011b;8(5):354–361. doi:10.3109/15412555.2011.60036221864116
- SharafkhanehA, AltanAE, ColiceGL, et al. A simple rule to identify patients with chronic obstructive pulmonary disease who may need treatment reevaluation. Respir Med. 2014;108(9):1310–1320. doi:10.1016/j.rmed.2014.07.00225130680
- SteerJ, GibsonGJ, BourkeSC. Longitudinal change in quality of life following hospitalisation for acute exacerbations of COPD. BMJ Open Respir Res. 2015;2(1):e000069. doi:10.1136/bmjresp-2014-000069
- StefanMS, NathansonB, LindenauerP, HigginsT, SteingrubJ. Characteristics, ventilation strategies, and outcomes of patients hospitalized in intensive care units with an acute exacerbation of COPD. Am J Respir Crit Care Med. 2014;189:A1632. doi:10.1164/rccm.201306-1150OC
- StefanMS, ShiehMS, PekowPS, HillN, RothbergMB, LindenauerPK. Trends in mechanical ventilation among patients hospitalized with acute exacerbations of COPD in the United States, 2001 to 2011. Chest. 2015;147(4):959–968. doi:10.1378/chest.14-121625375230
- ThomasM, RadwanA, StonhamC, MarshallS. Exacerbation frequency and maintenance treatment of COPD in UK clinical practice. Thorax. 2011;66(Suppl 4):A153. doi:10.1136/thoraxjnl-2011-201054c.211
- VitaccaM, EscarrabillJ, GalavottiG, et al. Home mechanical ventilation patients: a retrospective survey to identify level of burden in real life. Monaldi Arch Chest Dis. 2007;67(3):142–147. doi:10.4081/monaldi.2007.48518018753
- WangQ, BourbeauJ. Outcomes and health-related quality of life following hospitalization for an acute exacerbation of COPD. Respirology. 2005;10(3):334–340. doi:10.1111/res.2005.10.issue-315955146
- YuAP, YangH, WuEQ, SetyawanJ, MocarskiM, BlumS. Incremental third-party costs associated with COPD exacerbations: a retrospective claims analysis. J Med Econ. 2011;14(3):315–323. doi:10.3111/13696998.2011.57629521500975