
Abstract
Purpose
Many studies have reported the relationship between nonalcoholic fatty liver disease (NAFLD) and bone mineral density (BMD) among adults. However, fewer studies on this topic have been reported in adolescents. We thus conducted a meta-analysis to show the association between NAFLD and BMD in adolescents with obesity.
Materials and methods
Computer retrieval was carried out via PubMed, Embase, Cochrane Library and the Cochrane Central Register of Controlled Trials from inception to September 2018. Six published case–control studies that assessed the relationship between NAFLD and BMD were included.
Results
The six studies included 217 obese adolescents with NAFLD and 236 controls. The meta-analysis indicated that obese children with NAFLD had a lower BMD and Z-score than the control group (weighted mean difference [WMD]–0.03, 95% CI [−0.05, –0.02], P=0.000; [WMD] −0.26, 95% CI [−0.37, −0.14], P=0.000). However, we analyzed the factor of bone mineral content, and there was no correlation between the two groups ([WMD]–55.99, 95% CI [−132.16, 20.18], P=0.150).
Conclusion
Obese children with NAFLD are more susceptible to osteoporosis than children with only obesity. Because of the limitations related to the quantity and quality of the included literature, further studies are still needed.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in the world. Nearly 25.24% of the overall population has NAFLD.Citation1,Citation2 Moreover, NAFLD is the principal cause of chronic liver disease in children, especially among overweight and obese individuals in industrialized countries.Citation3 On a clinical spectrum, NAFLD ranges from nonalcoholic fatty liver (NAFL) to nonalcoholic steatohepatitis (NASH) and liver cirrhosis and fibrosis.Citation4 The serious outcomes of NAFLD are hepatocellular carcinoma and liver failure.Citation5 Unfortunately, in addition to liver destruction, the effects of NAFLD can also occur in extra hepatic organs and cause type 2 diabetes and cardiovascular disease.Citation6,Citation7
It is well established that the affecting mechanisms of NAFLD are insulin resistance (IR) and chronic inflammation.Citation8 Additionally, a high-calorie diet and a sedentary lifestyle contribute to NAFLD development.Citation9 The incidence rate of NAFLD is coincident with the increase in obesity.Citation10 Therefore, NAFLD has attracted worldwide attention.
Osteoporosis is a group of bone diseases with various causes, including general factors related to aging, obesity and sex steroid deficiency, as well as specific risk factors such as the use of glucocorticoids, reduced bone quality, and disruption of microarchitectural integrity.Citation11 In most cases of osteoporosis, the reduction in bone tissue is mainly due to increased bone resorption. Osteoporosis is characterized by low bone mineral density (BMD), bone pain and easy fracture.Citation12 Osteoporosis is a silent disease until fractures occur with increasing frequency, which can cause important problems and even death.Citation13 In industrialized countries, 9%–38% of women and 1%–8% of men >50 years suffer from osteoporosis.Citation14 Therefore, osteoporosis is not only harmful to health but also increases the financial burden of the impacted countries.Citation15
An epidemiological study from Portugal showed that ~3% of adolescents are obese, and 30% are overweight.Citation16,Citation17 In 2017, the Health Behaviour in School-Aged Children from the WHO showed that, among more than half of the European countries, the incidence of adolescent obesity rapidly increased from 2002 to 2014.Citation18 Many studies have demonstrated that NAFLD is associated with low BMD and osteoporosis,Citation19–Citation21 but most studies have focused on adults, and surveys targeting children and adolescents have been limited.Citation22 Here, we investigated the relationship between NAFLD and BMD in adolescents with obesity through a meta-analysis.
Materials and methods
Research strategy
This meta-analysis was conducted and reported following the PRISMA guidelines.Citation23 All the included studies were filtered through PubMed, Embase, and the Cochrane Database from inception to September 2018. We used the following keywords and terms: (“Non-alcoholic Fatty Liver Disease,” “Non alcoholic Fatty Liver Disease,” “NAFLD,” “Nonalcoholic Fatty Liver Disease,” “Fatty Liver, Nonalcoholic,” “Nonalcoholic Fatty Livers,” “Steatohepatitis, Nonalcoholic”) and (“Bone Density,” “Bone Densities,” “Density, Bone,” “Bone Mineral Density,” “Bone Mineral Content”).
Inclusion criteria
Inclusion factors were: 1) study types including prospective cohort, retrospective cohort, case–control, and cross-sectional studies evaluating the association between NAFLD and BMD; 2) all the participants were adolescents from puberty stage I to V;Citation24 3) NAFLD patients were diagnosed with an ultrasound examination or pathological examination to make a clear and definite diagnosis, and all the participants were obese according to body mass index (BMI); and 4) BMD was measured by dual energy X-ray absorptiometry.
Exclusion criteria
Exclusion factors were 1) other diseases that could cause NAFLD were excluded, such as viral infections, alcohol intake, and the use of drugs and 2) none of the subjects followed specific diets or therapeutic treatments that could influence BMD or liver function.
Data collection
Two investigators abstracted the data from the suitable studies and conformed them to the same criteria, including research topics, the details of the first author, year of publication, study type, number of patients and number in the control group, basic characteristics of participants, and mean values and SDs of BMD.
Quality assessment
The Newcastle Ottawa Scale (NOS) was used to assess the quality of the involved studies.Citation25 Studies with a score of 7–9 points were considered to be of high quality. The score of each study is represented in .
Table 1 Main characteristics of included studies and quality assessment score
Statistical analysis
Stata Statistical Software (ver. 12.0; StataCorp LP, College Station, TX, USA) was utilized in the meta-analysis, and P<0.05 was regarded as statistically significant. Continuous variables are presented as weighted mean differences (WMDs). If I 2 was more than 50%, heterogeneity was recognized as significant.Citation26 When the heterogeneity was high, a random effects model was used to evaluate the relationship between the two groups. If no obvious heterogeneity existed in the research results, a fixed effects model was used for the meta-analysis.Citation27,Citation28
Results
Literature selection
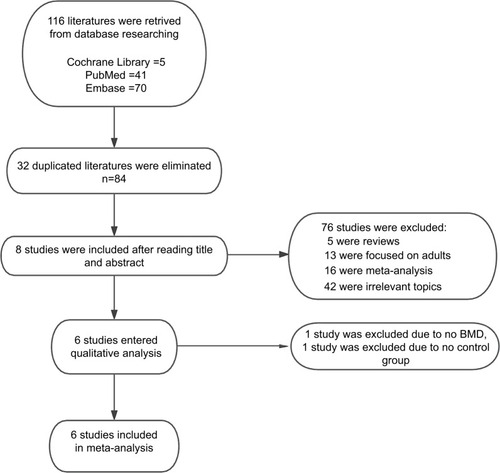
A total of 116 studies were selected from the databases mentioned at the beginning. After eliminating 32 duplicated studies and screening the titles and abstracts for studies that were not relevant because of the topic or research type, 8 studies were included in the full-text review. Finally, there were six studies included in our meta-analysis. A total of 217 obese adolescents with NAFLD and 236 obese adolescents were included, and the retrieved procedures and excluded details can be found in .
Figure 1 Flowchart of the studies’ selecting process and results.
Characteristics of the included studies
The basic characteristics of the six included studies are shown in . Obese adolescents with NAFLD were included in the case group, whereas obese children without NAFLD were included in the control group. The total number of patients in the case group was 217, whereas the control group included 236 individuals. By scanning the full texts of the six studies, we found that the study types were case–control. Among the included studies, five studies were performed in Europe, and one was performed in Asia. Ultrasound, MRI, and liver biopsy were used to diagnose NAFLD. In addition, the study performed in Asia had three groups: the control group, the simple steatosis group, and the NASH group. We integrated the first two groups into one, which was regarded as the control group in this meta-analysis. The NASH group was included in the case group. In addition, five studies had a high quality score, and the one study conducted in Asia had a lower score.
Results of the meta-analysis
Contrast indicator of BMD (g/cm2)
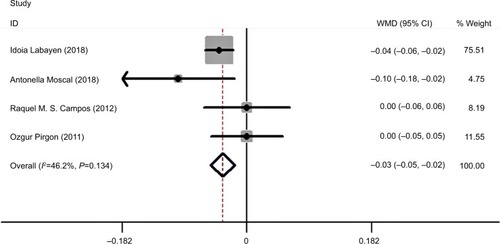
A total of 173 cases and 192 controls were included. A meta-analysis was conducted using a fixed effects model to evaluate the correlation between the case group and the control group with respect to BMD. The results showed that I 2=60.2%, P=0.039 (). Because of significant heterogeneity, we used a random effects model; however, the outcome was the same as that of the above-mentioned model (). After eliminating the study with a low quality score, we performed the analysis using the fixed effects model again, and the result was I 2=46.2%, P=0.000 (). The meta-analysis indicated that obese adolescents with NAFLD had a higher BMD than those without the illness.
Figure 2 (A) Meta-analysis of the correlation between obese adolescents with NAFLD and obese adolescents without NAFLD in BMD (fixed effects model). (B) Meta-analysis of the correlation between obese adolescents with NAFLD and obese adolescents without NAFLD in BMD (random effects model).
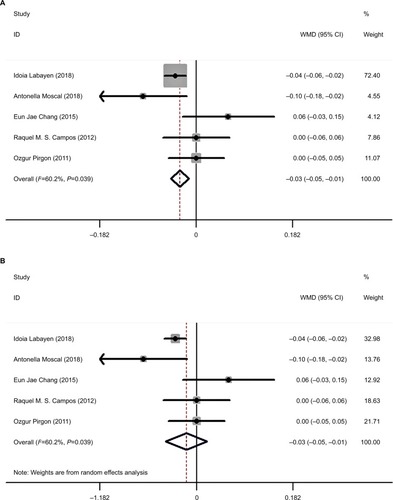
Figure 3 After eliminating the low score study the graph shows the meta-analysis of the correlation between obese adolescents without NAFLD in BMD (Fixed effects model).
Assessing differences using Z-scores
In this section, six studies were included in the meta-analysis. There were 217 patients in the case group and 236 individuals in the control group. A fixed effects model was used to assess the Z-score relationship between the two groups. The results demonstrated that I 2=26.9%, P=0.000 ().
Figure 4 Meta-analysis of the correlation between obese adolescents with NAFLD and obese adolescents without NAFLD in Z-score (Fixed effects model).
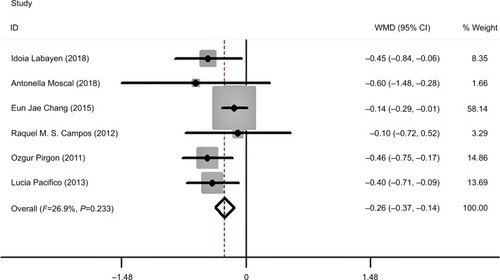
The meta-analysis showed that obese adolescents had a positive Z-score; therefore, the Z-scores revealed that obese adolescents with NAFLD were more likely to develop osteoporosis.
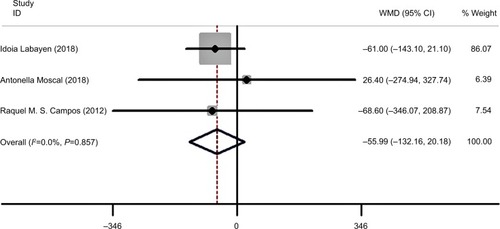
Assessing differences using BMC (g)
Three studies contained indicators of BMC. The total number in the case group was 84, whereas in the control group the number was 105. Through a meta-analysis, a fixed effects model showed that there was no significant difference between the NAFLD group and non-NAFLD group (I 2=0.0%, P=0.150). The outcome is shown in .
Figure 5 Meta-analysis of the correlation between obese adolescents with NAFLD and obese adolescents without NAFLD in BMC (Fixed effects model).
Discussion
According to this meta-analysis, we can conclude that obese adolescents with NAFLD have a higher BMD and Z-score than obese adolescents without NAFLD. However, when comparing the BMCs of the two groups, there was no difference. This is the only study to our knowledge to investigate the relationship between BMD and NAFLD in adolescents.
A recent study from Handzlik-Orlik et alCitation29 showed a relationship between NAFLD and osteoporosis. In addition, a retrospective study from People’s Republic of China that involved more than 7,000 men demonstrated that men with NAFLD had a high risk of suffering from an osteoporotic fracture.Citation30 A reduced BMD may be attributed to liver disorder.Citation31,Citation32 Although some clinical studies provided evidence that NAFLD is related to low BMD,Citation19–Citation34 the pathogenesis underlying the correlation between NAFLD and decreased BMD is not clear.
According to current studies, several hypotheses have been proposed, including mechanisms involving tumor necrosis factor (TNF)-α, osteopontin (OPN), osteoprotegerin (OPG), osteocalcin and fetuin-A.Citation35–Citation42 The main factor out of these is TNF-α. A previous study demonstrated that TNF-α could enhance osteoclast activity, inhibit osteoblast differentiation, and increase osteoblastapoptosis.Citation43–Citation45 Additionally, vitamin D plays a significant role in liver pathophysiology and NAFLD.Citation46 These cytokines and regulatory pathways have been associated with the presence of NAFLD.Citation47 Therefore, it has been proposed that the presence of systematic and constant inflammation in NAFLD patients contributes to the correlation between NAFLD and low BMD.Citation45 When focusing on children and adolescents, apart from the mechanisms mentioned above, a study of Hispanic children indicated that NAFLD was associated with obesity and the PNPLA3 gene.Citation48 NAFLD is strongly associated with obesity.Citation49 Childhood obesity can develop into adult obesity.Citation50,Citation51 Simmonds et alCitation52 conducted a meta-analysis, and the results showed that obese children had a 5-fold higher risk of adult obesity than normal-weight children. Therefore, children and adolescents who are overweight and obese are susceptible to NAFLD and problems related to bone metabolism.
Boys had notably higher BMC values than girls older than 14 years old; however, before this age cutoff, there were no sex differences in total body, femoral neck or lumbar spine BMD in a study conducted by Baxter-Jones et al.Citation53 Other experts also demonstrated that within the age range of 9–11, no differences in total BMD were observed between boys and girls.Citation54,Citation55 As for adolescents with NAFLD, research on the prevalence of osteoporosis in different genders is limited. Yu et alCitation56 performed a study on the relationship between bone marrow fat content and hepatic fat content in children with NAFLD. In their study, they found that in boys, bone marrow fat content and hepatic fat content had a significant positive relationship with known or suspected NAFLD, whereas in girls, no such relationship was observed. However, until now, there has been no direct evidence to explain this difference. Genetic factors, biological differences, sample sizes, and other elements may contribute to this phenomenon. As a result, further studies need to explore this relationship between different genders.
However, there are several limitations of this meta-analysis. First, some confounders were not eliminated, and some included studies were missing essential data, such as the number of boys and girls, age, BMI, BMC, and BMD; thus, we did not conduct subgroup analyses. Second, we did not evaluate the severity of NAFLD, and the results we obtained included the range of this disease. Third, because few studies have been performed on this subject, after filtering the studies, only six studies were included in this meta-analysis. If more studies are conducted in the future, we will further study the subgroups. Finally, most studies were from western countries, only one was from Asia, so the results may not be generalizable to some regions; further research needs to be done.
Conclusion
This meta-analysis explored the concept of obese adolescents with NAFLD exhibiting a lower BMD. However, due to the quality and quantity of the included studies, further studies are needed to reveal the relationship between NAFLD and BMD in obese children.
Acknowledgments
This study was supported by the First Affiliated Hospital of Guangxi Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
- Chalasani N Younossi Z Lavine JE The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology Gastroenterology 2012 142 7 1592 1609 22656328
- Rinella M Charlton M Mary R The globalization of nonalcoholic fatty liver disease: prevalence and impact on world health Hepatology 2016 64 1 19 22 26926530
- Welsh JA Karpen S Vos MB Saul K Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010 J Pediatr 2013 162 3 496 500 23084707
- Burt AD Lackner C Tiniakos DG Burt Alastair D Carolin L Diagnosis and assessment of NAFLD: definitions and histopathological classification Semin Liver Dis 2015 35 3 207 220 26378639
- Nobili V Svegliati-Baroni G Alisi A Miele L Valenti L Vajro P A 360-degree overview of paediatric NAFLD: recent insights J Hepatol 2013 58 6 1218 1229 23238106
- Korean Association for the Study of the Liver (KASL) KASL clinical practice guidelines: management of nonalcoholic fatty liver disease Clin Mol Hepatol 2013 19 4 325 348 24459637
- Alkhater SA Paediatric non-alcoholic fatty liver disease: an overview Obes Rev 2015 16 5 393 405 25753407
- Méndez-Sánchez N Arrese M Zamora-Valdés D Uribe M Nahum M-S Daniel Z-V Current concepts in the pathogenesis of nonalcoholic fatty liver disease Liver Int 2007 27 4 423 433 17403181
- Italian Association for the Study of the Liver (AISF) AISF position paper on nonalcoholic fatty liver disease (NAFLD): updates and future directions Dig Liver Dis 2017 49 5 471 483 28215516
- Umehara T Toshihiro U Nonalcoholic fatty liver disease with elevated alanine aminotransferase levels is negatively associated with bone mineral density: cross-sectional study in U.S. adults PLoS One 2018 13 6 e0197900 29897928
- Sözen T Özışık L BaşaranBaşaran NÇ Tümay S Lale Özışık Çalık BN An overview and management of osteoporosis Eur J Rheumatol 2017 4 1 46 56 28293453
- Yamamoto K Definition and diagnostic criteria of osteoporosis in Japan Clin Calcium 2001 11 1 19 24 15775485
- Cosman F de Beur SJ Leboff MS Clinician’s guide to prevention and treatment of osteoporosis Osteoporos Int 2014 25 10 2359 2381 25182228
- Wade SW Strader C Fitzpatrick LA Anthony MS O’Malley CD Estimating prevalence of osteoporosis: examples from industrialized countries Arch Osteoporos 2014 9 1 182 24847682
- Cummings SR Melton LJ Joseph ML Epidemiology and outcomes of osteoporotic fractures Lancet 2002 359 9319 1761 1767 12049882
- Videira-Silva A Sardinha L Fonseca H Antonio V-S Effect of a physical activity consultation in the management of adolescent overweight (the PAC-MAnO project): study rationale, design and methods BMJ Paediatr Open 2018 2 1 e000214
- Sardinha LB Santos R Vale S Prevalence of overweight and obesity among Portuguese youth: a study in a representative sample of 10-18-year-old children and adolescents Int J Pediatr Obes 2011 6 2–2 e124 e128 20919807
- Inchley J Currie D Jewell J Adolescent Obesity and Related Behaviours: Trends and Inequalities in the WHO European Region; 2002–2014 Geneva World Health Organization 2017
- Pardee PE Dunn W Schwimmer JB Non-alcoholic fatty liver disease is associated with low bone mineral density in obese children Aliment Pharmacol Ther 2012 35 2 248 254 22111971
- Purnak T Beyazit Y Ozaslan E Efe C Hayretci M The evaluation of bone mineral density in patients with nonalcoholic fatty liver disease Wien Klin Wochenschr 2012 124 15–16 526 531 22850810
- Cui R Sheng H Rui XF Low bone mineral density in Chinese adults with nonalcoholic fatty liver disease Int J Endocrinol 2013 2013 396545 23983685
- Poggiogalle E Donini LM Lenzi A Chiesa C Pacifico L Non-alcoholic fatty liver disease connections with fat-free tissues: a focus on bone and skeletal muscle World J Gastroenterol 2017 23 10 1747 1757 28348479
- Liberati A Altman DG Tetzlaff J The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration J Clin Epidemiol 2009 62 10 e1 34 19631507
- Tanner JM Whitehouse RH Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty Arch Dis Child 1976 51 3 170 179 952550
- Stang A Andreas S Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses Eur J Epidemiol 2010 25 9 603 605 20652370
- Cochran WG The combination of estimates from different experiments Biometrics 1954 10 1 101 129
- Shachar M Meta-analysis: the preferred method of choice for the assessment of distance learning quality factors IRRODL 2008 9 3 1 15
- Dersimonian R Laird N Meta-analysis in clinical trials Control Clin Trials 1986 7 3 177 188 3802833
- Handzlik-Orlik G Holecki M Wilczyński K Duława J Osteoporosis in liver disease: pathogenesis and management Ther Adv Endocrinol Metab 2016 7 3 128 135 27293541
- Li M Xu Y Xu M Association between nonalcoholic fatty liver disease (NAFLD) and osteoporotic fracture in middle-aged and elderly Chinese J Clin Endocrinol Metab 2012 97 6 2033 2038 22466338
- Moon SS Lee YS Kim SW Seong-Su M Association of nonalcoholic fatty liver disease with low bone mass in postmenopausal women Endocrine 2012 42 2 423 429 22407492
- Guañabens N Parés A Núria G Albert P Osteoporosis in chronic liver disease Liver Int 2018 38 5 776 785 29479832
- Ozgur P Huseyin B Ismet T Correlation of insulin sensitivity with bone mineral status in obese adolescents with nonalcoholic fatty liver disease Clin Endocrinol 2011 75 189 195
- Campos RMS de Piano A da Silva PL The role of pro/anti-inflammatory adipokines on bone metabolism in NAFLD obese adolescents: effects of long-term interdisciplinary therapy Endocrine 2012 42 1 146 156 22315014
- Aigner E Theurl I Theurl M Pathways underlying iron accumulation in human nonalcoholic fatty liver disease Am J Clin Nutr 2008 87 5 1374 1383 18469261
- Manco M Marcellini M Giannone G Nobili V Correlation of serum TNF-alpha levels and histologic liver injury scores in pediatric nonalcoholic fatty liver disease Am J Clin Pathol 2007 127 6 954 960 17509993
- Morimoto J Kon S Matsui Y Uede T Junko M Shigeyuki K Osteopontin; as a target molecule for the treatment of inflammatory diseases Curr Drug Targets 2010 11 4 494 505 20196720
- Yilmaz Y Yonal O Kurt R Serum levels of osteoprotegerin in the spectrum of nonalcoholic fatty liver disease Scand J Clin Lab Invest 2010 70 8 541 546 20942739
- Yilmaz Y Kurt R Eren F Imeryuz N Serum osteocalcin levels in patients with nonalcoholic fatty liver disease: association with ballooning degeneration Scand J Clin Lab Invest 2011 71 8 631 636 21859358
- Haukeland JW Dahl TB Yndestad A Fetuin A in nonalcoholic fatty liver disease: in vivo and in vitro studies Eur J Endocrinol 2012 166 3 503 510 22170794
- Yilmaz Y Yonal O Kurt R Serum fetuin A/α2HS-glycoprotein levels in patients with non-alcoholic fatty liver disease: relation with liver fibrosis Ann Clin Biochem 2010 47 Pt 6 549 553 20926473
- Reinehr T Roth CL Thomas R Fetuin-A and its relation to metabolic syndrome and fatty liver disease in obese children before and after weight loss J Clin Endocrinol Metab 2008 93 11 4479 4485 18728159
- Kudo O Fujikawa Y Itonaga I Sabokbar A Torisu T Athanasou NA Proinflammatory cytokine (TNFalpha/IL-1alpha) induction of human osteoclast formation J Pathol 2002 198 2 220 227 12237882
- Gilbert L He X Farmer P Expression of the osteoblast differentiation factor RUNX2 (Cbfa1/AML3/Pebp2alpha A) is inhibited by tumor necrosis factor-alpha J Biol Chem 2002 277 4 2695 2701 11723115
- Haley B Pegah G Younossi Zobair M Pediatric non-alcoholic fatty liver disease Children 2017 4 6
- Yilmaz Y Review article: non-alcoholic fatty liver disease and osteoporosis – clinical and molecular crosstalk Aliment Pharmacol Ther 2012 36 4 345 352 22730920
- Cai D Yuan M Frantz DF Local and systemic insulin resistance resulting from hepatic activation of IKK-beta and NF-kappaB Nat Med 2005 11 2 183 190 15685173
- Betancourt-Garcia MM Arguelles A Montes J Hernandez A Singh M Forse RA Pediatric nonalcoholic fatty liver disease: the rise of a lethal disease among Mexican American Hispanic children Obes Surg 2017 27 1 236 244 27822768
- Schwimmer JB Deutsch R Kahen T Lavine JE Stanley C Behling C Prevalence of fatty liver in children and adolescents Pediatrics 2006 118 4 1388 1393 17015527
- Venn AJ Thomson RJ Schmidt MD Overweight and obesity from childhood to adulthood: a follow-up of participants in the 1985 Australian Schools Health and Fitness Survey Med J Aust 2007 186 9 458 460 17484707
- Ogden CL Carroll MD Kit BK Flegal KM Prevalence of childhood and adult obesity in the United States, 2011-2012 JAMA 2014 311 8 806 814 24570244
- Simmonds M Burch J Llewellyn A The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis Health Technol Assess 2015 19 1 336
- Baxter-Jones AD Mirwald RL McKay HA Bailey DA A longitudinal analysis of sex differences in bone mineral accrual in healthy 8-19-year-old boys and girls Ann Hum Biol 2003 30 2 160 175 12637192
- Ferretti JL Capozza RF Cointry GR Gender-related differences in the relationship between densitometric values of whole-body bone mineral content and lean body mass in humans between 2 and 87 years of age Bone 1998 22 6 683 690 9626409
- Maynard LM Guo SS Chumlea WC Total-body and regional bone mineral content and areal bone mineral density in children aged 8-18 Y: the Fels longitudinal study Am J Clin Nutr 1998 68 5 1111 1117 9808230
- Yu NY Wolfson T Middleton MS Bone marrow fat content is correlated with hepatic fat content in paediatric non-alcoholic fatter liver disease Clin Radiol 2017 72 5 e9 425
- Pacifico L Bezzi M Lombardo C V Adipokines and C-reactive protein in relation to bone mineralization in pediatric nonalcoholic fatty liver disease[J World Journal of Gastroenterology 2013 19 25 4007 4014 23840146
- Labayen I Ruiz J R Arenaza L Hepatic fat content and bone mineral density in children with overweight/obesity [J]. Pediatr. Res 2018 84 684 688
- Antonella M Danilo F Elenora S Relationship between nonalcoholic steatohepatitis, PNPLA3 I148M genotype and bone mineral density in adolescents [J]. Liver International 2018 38 2301 2308
- Campos RMS de Piano A da Silva PL The role of pro/antiinflammatory adipokines on bone metabolism in NAFLD obese adolescents: effects of long-term interdisciplinary therapy Endocrine 2012 42 1 146 156 22315014
- Pirgon O Bilgin H Tolu I Correlation of insulin sensitivity with bone mineral status in obese adolescents with nonalcoholic fatty liver disease[J] Clinical Endocrinology 2011 75 2 189 195 21521307
- Jae C E Yong Y D Ran Y H Vitamin D Status and Bone Mineral Density in Obese Children with Nonalcoholic Fatty Liver Disease[J] Journal of Korean Medical Science 2015 30 12 1821 1827 26713058