
Abstract
Human immunodeficiency virus (HIV) is a chronic disease associated with dyslipidemia and insulin resistance. In addition, the administration of combination antiretroviral therapy is associated with an increase in the incidence of metabolic risk factors (insulin resistance, lipoatrophy, dyslipidemia, and abnormalities of fat distribution in HIV patients). HIV dyslipidemia is a common problem, and associated with an increase in incidence of cardiovascular disease. Further challenges in the management of HIV dyslipidemia are the presence of diabetes and metabolic syndrome, nonalcoholic fatty liver disease, hypothyroidism, chronic kidney disease, the risk of diabetes associated with statin administration, age and ethnicity, and early menopause in females. Dyslipidemia in patients with HIV is different from the normal population, due to the fact that HIV increases insulin resistance and HIV treatment not only may induce dyslipidemia but also may interact with lipid-lowering medication. The use of all statins (apart from simvastatin and lovastatin) is safe and effective in HIV dyslipidemia, and the addition of ezetimibe, fenofibrate, fish oil, and niacin can be used in statin-unresponsive HIV dyslipidemia. The management of dyslipidemia and cardiovascular disease risks associated with HIV is complex, and a certain number of patients may require management in specialist clinics run by specialist physicians in lipid disorders. Future research is needed to address best strategies in the management of hyperlipidemia with HIV infection.
Introduction
Human immunodeficiency virus (HIV) is a chronic disease associated with increased mortality and morbidity from HIV-related conditions.Citation1 Furthermore, HIV is associated with dyslipidemia in the form of high triglycerides and low high-density lipoprotein (HDL).Citation2 The possible mechanisms for HIV-induced dyslipidemia are increased cytokine levels (TNF and IL-6), decreased lipid clearance, and increased hepatic synthesis of very low-density lipoprotein (VLDL).Citation2 Furthermore, Lo and Grinspoon suggested that there is an independent HIV effect on cardiovascular risk.Citation3 Moreover, the administration of combination antiretroviral therapy (cART) is associated with an increase in the incidence of metabolic risk factors (insulin resistance, lipoatrophy, dyslipidemia, and abnormalities of fat distribution) in HIV patients.Citation2,Citation4 In a multicenter cross-sectional study of elderly individuals with HIV, dyslipidemia was found in 54%, cardiovascular disease (CVD) in 23%, and lipodystrophy in 58%.Citation5 Hejazi et al found that dyslipidemia is common in HIV subjects receiving antiretroviral medication: it reaches (82.3%) among 1,583 patients in their Malaysian study.Citation6
It is important to recognize that as patients live longer, they became vulnerable to many complications, prominently CVD. The dyslipidemia associated with cART administration is typically manifested as decreased HDL cholesterol (HDL-C), increased LDL-C (including small, dense LDL), and increased total cholesterol. Such values are associated with increased cardiovascular risk in persons who are not HIV-infected, and obviously place HIV patients at risk for premature cardiovascular events. Common medications used in the treatment of HIV are protease inhibitors (PIs), nucleoside reverse-transcriptase inhibitors (NRTIs), and nonnucleoside reverse-transcriptase inhibitors (NNRTIs).Citation7,Citation8 HIV-related dyslipidemia is increasingly recognized as a problem in patients on cART, particularly those on PI-based regimes.Citation9 PIs are associated with an incidence of dyslipidemia in 70% and 80% in the form of high triglycerides and LDL-C and decreased HDL-C and accumulation of ApoE and ApoC III. PIs are also associated with central obesity, lipoatrophy, and insulin resistance.Citation10 The effect of PIs in lipid profile is due to inhibition of lipogenesis, adipocyte differentiation, decrease in hepatocyte clearance of hepatic chylomicron and VLDL, and stimulation of hepatic synthesis of triglycerides.Citation10,Citation11
NRTIs are also associated with high triglycerides and lipoatrophy, but this effect is less seen with administration of tenofovir. It is recommended to switch to tenofovir in case dyslipidemia becomes an issue, especially in children.Citation12 It is worth mentioning that abacavir and didanosine (NRTIs) were associated with independent risk of myocardial infarction in the DAD study.Citation13 Interestingly, the use of NNRTIs like nevirapine protected against low HDL-C levels, while the use of efavirenz was associated with increase in total cholesterol and triglycerides.Citation14 Penzak et al suggested that an increased percentage of death attributable to cardiac, renal, and hepatic disease among HIV patients treated with highly active antiretroviral therapy (ART).Citation15 The extensive use of cART medication in HIV patients is associated with dyslipidemia, insulin resistance and diabetes.Citation16 The aim of this article is to review the current challenges in treating dyslipidemia with HIV and recommend the solutions from the evidence available so far.
Why is dyslipidemia in HIV patients a challenge to manage?
Cardiovascular risk and HIV disease
Major cardiovascular-related comorbidities are prevalent in HIV/acquired immunodeficiency syndrome (AIDS), especially older and obese individuals. Chu et al found prevalence rates of 26%, 48%, and 13% for hypertension, dyslipidemia, and diabetes, respectively. They thought that because cardiovascular risk is modifiable, effective treatment of related comorbidities may improve morbidity and mortality in HIV-infected patients.Citation17
Dyslipidemia is also increasingly recognized in HIV-infected children.Citation18 HIV-infected children may be at risk for premature CVD, as they have high levels of cholesterol and triglycerides.Citation19 Even perinatally HIV-infected adolescents may be susceptible to aggregate atherosclerotic CVD risk.Citation20 Interestingly, the prevalence of coronary heart disease (CHD) among a Mediterranean cohort of 3,760 HIV-infected patients was low: 81 patients (prevalence 2.15%).Citation21 has a summary of some studies showing association between HIV and CVD.Citation22–Citation25
Table 1 Summary of some studies showing association between HIV and CVD
Diabetes mellitus, metabolic syndrome, and HIV
Dyslipidemia and increased blood glucose are the most common health threats, with a high incidence among HIV/AIDS patients on ART worldwide. Dyslipidemia, lipodystrophy, and diabetes mellitus can result from long-term ART in HIV patients. In their cohort study, Menezes de Pádua and Moura obtained information on long-term adverse drug reactions to ART from medical charts of treatment-naïve HIV-infected adult patients initiating ART. Of 233 medical charts, 26.1% contained at least one long-term adverse reaction, corresponding to 45 cases of dyslipidemia (19.3%), 16 (6.9%) of lipodystrophy, and five of diabetes mellitus (2.1%).Citation26 Studies from Ghana, Tanzania, Thailand, Ethiopia, and Brazil showed an increase in prevalence of lipoatrophy, insulin resistance, and diabetes in particular with ART.Citation27–Citation31
Dyslipidemia significantly increases with cumulative exposure to ART. Tripathi et al found that there was a significantly higher risk of dyslipidemia in their ART-treated HIV-infected group (adjusted hazard ratio 1.18, 95% confidence interval [CI] 1.07–1.30) and a significantly lower risk in the ART-naïve HIV-infected group (adjusted hazard ratio 0.66, 95% CI 0.53–0.82) compared to the control non-HIV-infected group. They also found that preexisting hypertension, obesity, and diabetes increased the risk of dyslipidemia, whereas hepatitis C virus, lower CD4+ T-cell count, and higher HIV viral load had a protective effect.Citation32 Furthermore, Ledergerber et al suggested that current treatment with PI- and NRTI-containing regimens was associated with the risk of developing type 2 diabetes mellitus.Citation33
HIV represents a chronic inflammatory condition, and this may lead to insulin resistance. Furthermore, changes in body configuration (central obesity, truncal obesity, and lipoatrophy) and associated dyslipidemia all accelerate the process that lead to diabetes mellitus with HIV and ART.
HIV-associated lipodystrophy syndrome consists of lipoatrophy, lipohypertrophy, and metabolic disturbances (dyslipidemia and hyperglycemia). Lipoatrophy involves the face, lower limbs, and buttocks. It is closely related to NRTIs and rarely associated with PIs. Lipohypertrophy is related to the accumulation of adipose tissue (abdomen, breast, and interscapular fat), and this is likely due to PIs. Central fat accumulation is observed more in females, and is associated with increased body fat. Furthermore, PIs are also associated with dyslipidemia due to mitochondrial toxicity and inhibition of glucose transporter type 4, and this leads to inhibition of adipocyte differentiation and an increase in triglyceride levels and insulin resistance. NRTIs can also be associated with dyslipidemia and insulin resistance.Citation34 Other mechanisms were suggested to contribute towards development of HIV-associated lipodystrophy syndrome, some of which are inflammation, inhibition of lipid metabolism (inhibition of lipoprotein lipase and excess triglyceride and risk of insulin resistance), oxidative stress and impaired function of adipokines and transcript factors (adiponectin, leptin, sterol regulatory binding proteins (SREBPs) and peroxisomal proliferatory activator receptors (PPAR) α and γ.Citation35
Nonalcoholic fatty liver disease and HIV
HIV and ART are associated with nonalcoholic fatty liver disease (NAFLD).Citation36–Citation38 The significance of NAFLD lies in the fact that it is associated with insulin resistance in 95% of cases and is also associated with a high risk of CVD and dyslipidemia.Citation39,Citation40 Price et al showed in a multicenter study that computed tomography-defined NAFLD is common among men at risk for HIV infection, is associated with greater visceral adiposity and insulin resistance, and prolonged exposure to dideoxynucleoside analogs is associated with higher prevalence.Citation41 The prevalence of NAFLD in Asian patients with HIV is estimated to be around 31%, and is associated with high BMI, dyslipidemia, and high aspartate transaminase:alanine transaminase ratio, but not with HIV-related factors (treatment with dideoxynucleoside analogs [didanosine, stavudine, and zalcitabine] and cumulative duration of ART).Citation42 Sterling et al showed that NAFLD is around 26%, and the only clinical or laboratory feature associated with biopsy-proven steatosis was γ-glutamyl transpeptidase and insulin resistance.Citation43 NAFLD is also seen in HIV patients who are coinfected with hepatitis C.Citation44,Citation45 The only effective therapy for NAFLD is weight loss, and the use of statins with NAFLD appears to be safe and effective.
Statins and associated risk of diabetes in diabetogenic conditions like HIV
Statins are used worldwide in the treatment of hyperlipidemia and CVD in HIV patients. The association between diabetes and statin treatment has been observed in several studies. In a collaborative meta-analysis of randomized clinical trials, statin therapy was associated with a slightly increased risk of development of diabetes, but the risk was low, both in absolute terms and when compared with the reduction in coronary events, and statins can be prescribed for individuals with moderate or high cardiovascular risk or existing CVD.Citation46 Furthermore, intensive-dose statin therapy was associated with an increased risk of new-onset diabetes compared with moderate-dose statin therapy in a meta-analysis of five statin trials.Citation47 Data from the Women’s Health Initiative study (161,808 postmenopausal women aged 50–79 years) showed that statin-medication use in postmenopausal women is associated with an increased risk for diabetes.Citation48 Interesting reviews on the subject have recently been published by Athyros and MikhailidisCitation49 and Athyros et al.Citation50 It is not clear whether the risk of incident diabetes associated with the administration of statins will increase the risk of further insulin resistance associated with HIV and ART. It is worth mentioning that it is recommended clinical practice to continue to monitor plasma glucose in HIV patients taking statin therapy. Further studies are needed to assess whether statin administration in individuals with HIV carries a high risk for diabetes.
High prevalence of chronic kidney disease among HIV patients and associated dyslipidemia
HIV patients are at risk of developing chronic kidney disease (CKD). Several studies suggested that the slight deterioration in renal function is likely due to the HIV more than the ART. In Taiwan, the prevalence of CKD in HIV-infected patients was low (7.03%), and diabetes, hypertension, and hypercholesterolemia were demonstrated to be associated with CKD.Citation51 In a Danish study, tenofovir and indinavir reduced estimated glomerular filtration rate (eGFR), while time with HIV only had a modest effect on renal function.Citation52 The most common causes of acute kidney injury in HIV-infected persons are systemic infections and adverse drug effects. The prevalence of CKD is rising in the HIV-infected population, and CKD is increasingly likely to be caused by comorbid conditions, such as diabetes and hypertension, which frequently cause CKD in the general population.Citation53 In rural northern KwaZulu-Natal, South Africa, Madala et al conducted a cross-sectional study of 302 patients, 290 (96%) of whom were black African, to assess whether diabetes and HIV are associated with CKD. Mean age ± standard deviation was 47.1±17.0 years.Citation54 Approximately 86.4% of females and 54.5% of males were overweight/obese. Dyslipidemia was observed in 47.9% females and 29.2% males (P<0.001). They found that the eGFR was <30 mL/min/1.73 m2 in 50.6% of patients. Using logistic regression analysis, they observed the following CKD risk factors: hypertension (77.8%), diabetes (29.8%), HIV (28.5%), glomerulonephritis (7.0%), and tubulointerstitial diseases (5.6%). Moreover, their study revealed that independent factors associated with eGFR <30 mL/min/1.73 m2 at presentation were: HIV (odds ratio 2.4, 95% CI 1.3–4.2; P=0.004) and hypertension (odds ratio, 95% CI 1.3–4.2; P=0.007). CKD patients have increased risk of CVD, due to increased prevalence of hypertension, dyslipidemia, and diabetes. The key features of dyslipidemia in mild and moderate CKD patients are elevated triglycerides and lipoprotein(a), lower HDL-C, with normal (or low) total cholesterol, and normal (or low) LDL-C.Citation55 Therefore, assessment of renal function constitutes an important part of the management of dyslipidemia with HIV. However, in the future, the clinical impact and hence the requirement for more research in the area of CKD with HIV and retroviral therapy will likely increase, due to aging and continued antiretroviral exposure of the HIV-positive population.
Hypothyroidism and HIV
Patients infected with HIV have a higher prevalence of thyroid dysfunction when compared with the general population. In view of the fact that hypothyroidism is associated with hyperlipidemia, the focus of this section is on the prevalence of hypothyroidism with HIV. Importantly, ART can complicate thyroid function through drug interactions and the immune reconstitution inflammatory syndrome.Citation56 The prevalence of hypothyroidism in HIV patients in France was found to be around 16%, and low CD4 cell counts and administration of stavudine were risk factors.Citation57 While in Thai patients, the prevalence is 13.5%, it is 15.5% in Colombia.Citation58,Citation59 Interestingly, a study from the US showed that the prevalence of abnormal thyroid function was around 12.4%, while the prevalence of hypothyroidism was 7% in Egypt.Citation60,Citation61 Therefore, screening for thyroid function should be part of the management of dyslipidemia with HIV and HIV treatment.
Early menopause
Menopause in the general population is associated with a threefold increase of risk of ischemic heart disease. Menopause is also associated with a high risk of atherosclerosis, dyslipidemia, insulin resistance, and thrombotic tendency. In a multicenter Italian surveillance study based on an anonymous questionnaire completed by 585 HIV-positive women aged 18 years or older, 352 women 45 years or younger were included in the analysis. Among the 352 patients 45 years or younger, 27 reported menopause for a prevalence of 7.7%. Among the 173 women 40 years or younger, nine reported amenorrhea in the previous 12 months for a 5.2% prevalence. This last proportion was more than twofold greater than the one observed in the HIV-negative Italian population. The HIV-infected cohort was about equivalent to that in the general Italian population (7.7% versus 7.1%). However, HIV-infected women had a greater prevalence of menopause at 40 years or younger than women in the population at large (5.2% versus 1.8%).Citation62 A review by Kojic et al suggested that the mean age of menopause for menopausal women living with HIV is likely to be 47–48 years, while for non-HIV women the mean age of menopause is around 51 years.Citation63 Women living with HIV have multiple, potentially additive factors that predispose them to metabolic complications, including osteoporosis, lipid and glucose disturbances, and cardiovascular risk.Citation63,Citation64 These factors include the consequences of HIV itself, impact of ART, loss of the protective effects of estrogen in menopausal women, and adverse effects of highly active antiretroviral therapy (HAART).Citation65,Citation66
Statin therapy is useful in hyperlipidemic postmenopausal women. Statins can help maintain or increase bone mass of hypercholesterolemic menopausal women through promoting bone synthesis.Citation67 In their population-based case–control study, Fournier et al found that statins could potentially attenuate the increased risk of venous thromboembolism associated with hormonal therapy combinations of oral estrogens and progestogens.Citation68 Studies are needed to confirm whether these factors are clinically significant and for better understanding of the possible interactions between HIV and hormones and how these influence disease progression and treatment. Therefore, screening for early menopause in women with HIV should be part of the management of dyslipidemia with HIV and HIV treatment.
Aging with HIV
One important feature of the success of ART is that individuals with HIV live longer. In several studies, comorbidities like diabetes, dyslipidemia, CKD, hypertension, and CVD in HIV patients increased with age.Citation69 This will lead to a significant burden in health resources in the near future unless extensive research is carried in order to develop the best health strategies to tackle such an epidemic.
Solutions for hyperlipidemia in HIV patients
The management of hyperlipidemia in HIV patients can be difficult. However, it is always recommended that lifestyle modifications in terms of weight reduction and calorie restriction are important part in the management of this type of difficult hyperlipidemia. Therefore, the majority of patients with HIV dyslipidemia may require lipid-lowering therapy. Controlled clinical trials and clinical experience have shown the benefit of statins as treatment for CVD, familial hypercholesterolemia, and dyslipidemia with diabetes.Citation70 In addition, recent large clinical trials have further demonstrated the clinical benefits and safety of statins in patients with a wide range of high risks for CVD and safety of statins as monotherapy or in combination with other lipid-lowering medications. Interestingly, statins are safe and effective, and can improve liver tests and reduce cardiovascular morbidity in patients with NAFLD.Citation71–Citation73 Different types of statins are available to lower plasma lipids to guideline levels in patients with HIV, but all differ in their pharmacokinetic properties, drug-interaction profiles, and risk of myotoxicity. provides a summary of the effects of different statins and other lipid-lowering medication.Citation15,Citation17,Citation74–Citation110
Table 2 Summary of the effect of different statins and other lipid-lowering medications
Conclusion
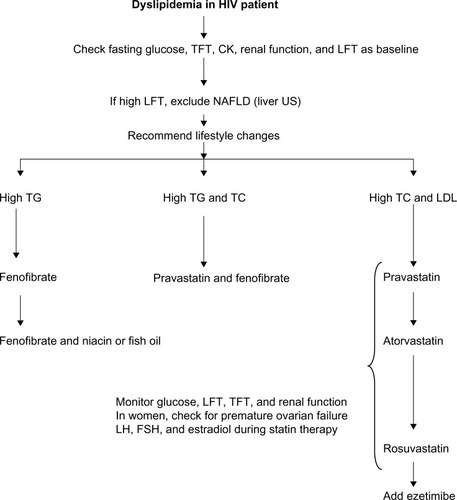
The dyslipidemia in patients with HIV is unique, due to 1) the fact that HIV per se and treatment of HIV may induce it, 2) the interaction between HIV treatment and statins, and 3) HIV dyslipidemia may be related to HIV or HIV treatment-induced conditions like NAFLD, hypothyroidism, early menopause, diabetes, and CKD (). The aging population of HIV patients will represent a serious challenge in terms of the management of dyslipidemia. Most guidelines recommend the use of rosuvastatin, atorvastatin, and pravastatin. Statin-unresponsive HIV dyslipidemia can be treated with the addition of ezetimibe, fenofibrate, fish oil, and niacin. illustrates the need to monitor glucose, liver, renal, and thyroid function. In women, it is important to manage issues related to premature menopause. We recommend that hyperlipidemia needs be managed in specialized clinics, and future research about the aging HIV population is needed.
Figure 1 Illustration of different potential factors that lead hyperlipidemia with HIV and associated increase in risk of CVD.

Figure 2 Illustration showing possible summary of current guidelines for the management of HIV dyslipidemia. Aging populations will need special consideration with regard to adjustment for lipid-lowering medication.
Disclosure
The authors report no conflicts of interest in this work.
References
- BittarRGiralPAslangulEDeterminants of low-density lipoprotein particle diameter during antiretroviral therapy including protease inhibitors in HIV-1-infected patientsAntivir Ther201217585586022318219
- GrinspoonSCarrACardiovascular risk and body-fat abnormalities in HIV-infected adultsN Engl J Med20053521486215635112
- LoJGrinspoonSCardiovascular disease in HIV-infected patients: does HIV infection in and of itself increase cardiovascular risk?Curr Opin HIV AIDS20083320721319372968
- DubéMPParkerRATebasPGlucose metabolism, lipid, and body fat changes in antiretroviral-naive subjects randomized to nelfinavir or efavirenz plus dual nucleosidesAIDS200519161807181816227788
- MotheBPerezIDomingoPHIV-1 infection in subjects older than 70: a multicenter cross-sectional assessment in Catalonia, SpainCurr HIV Res20097659760019929794
- HejaziNRajikanRChoongCLSaharSMetabolic abnormalities in adult HIV infected population on antiretroviral medication in Malaysia: a cross-sectional surveyBMC Public Health20131375823947428
- ZouWBerglundLHIV and highly active antiretroviral therapy: dyslipidemia, metabolic aberrations, and cardiovascular riskPrev Cardiol20071029610317392622
- MallewaJEHigginsSPGarbettSSaxenaNVilarFJCardiovascular disease risk management in HIV patients, experiences from Greater ManchesterInt J STD AIDS200920642542619451331
- CalzaLManfrediRChiodoFDyslipidaemia associated with anti-retroviral therapy in HIV-infected patientsJ Antimicrob Chemother2004531101414645323
- HruzPWMurataHMuecklerMAdverse metabolic consequences of HIV protease inhibitor therapy: the search for a central mechanismAm J Physiol Endocrinol Metab20012804E549E55311254460
- FauvelJBonnetERuidavetsJBAn interaction between Apo C-III variants and protease inhibitors contributes to high triglyceride/low HDL levels in treated HIV patientsAIDS200115182397240611740190
- ViganòAAldrovandiGMGiacometVImprovement in dyslipidaemia after switching stavudine to tenofovir and replacing protease inhibitors with efavirenz in HIV-infected childrenAntivir Ther200510891792416430197
- D:A:D Study GroupSabinCAWormSWUse of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaborationLancet200837196221417142618387667
- BernalEMasiáMPadillaSGutiérrezFHigh-density lipoprotein cholesterol in HIV-infected patients: evidence for an association with HIV-1 viral load, antiretroviral therapy status, and regimen compositionAIDS Patient Care STDS200822756957518479224
- PenzakSRChuckSKStajichGVSafety and efficacy of HMG-CoA reductase inhibitors for treatment of hyperlipidemia in patients with HIV infectionPharmacotherapy20002091066107110999499
- GrinspoonSKGrunfeldCKotlerDPState of the science conference: Initiative to decrease cardiovascular risk and increase quality of care for patients living with HIV/AIDS: executive summaryCirculation2008118219821018566320
- ChuCUmanskiGBlankAMeissnerPGrossbergRSelwynPAComorbidity-related treatment outcomes among HIV-infected adults in the Bronx, NYJ Urban Health201188350751621302140
- KaminDHadiganCHyperlipidemia in children with HIV infection: an emerging problemExpert Rev Cardiovasc Ther20031114315015030304
- MillerTIBorkowskyWDiMeglioLAMetabolic abnormalities and viral replication are associated with biomarkers of vascular dysfunction in HIV-infected childrenHIV Med201213526427522136114
- PatelKWangJJacobsonDLAggregate risk of cardiovascular disease among adolescents perinatally infected with the human immunodeficiency virusCirculation2014129111204121224366631
- EcheverríaPDomingoPLlibreJMPrevalence of ischemic heart disease and management of coronary risk in daily clinical practice: results from a Mediterranean cohort of HIV-infected patientsBiomed Res Int2014201482305825170515
- WormSWDe WitSWeberRDiabetes mellitus, preexisting coronary heart disease, and the risk of subsequent coronary heart disease events in patients infected with human immunodeficiency virus: the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D Study)Circulation2009119680581119188509
- WormSWFriis-MøllerNBruyandMHigh prevalence of the metabolic syndrome in HIV-infected patients: impact of different definitions of the metabolic syndromeAIDS201024342743519910787
- TriantVALeeHHadiganCGrinspoonSKIncreased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus diseaseJ Clin Endocrinol Metab20079272506251217456578
- DAD Study GroupFriis-MøllerNReissPClass of antiretroviral drugs and the risk of myocardial infarctionN Engl J Med2007356171723173517460226
- Menezes de PáduaCAMouraCSAvailability of data on adverse reactions to antiretroviral drugs in medical charts according to the Naranjo algorithm: an example of a Brazilian historical cohortClin Drug Investig2014346395402
- KagarukiGBMayigeMTNgadayaESMagnitude and risk factors of non-communicable diseases among people living with HIV in Tanzania: a cross sectional study from Mbeya and Dar es Salaam regionsBMC Public Health20141490425183300
- NgalaRAFiankoKDyslipidaemia and dysglycaemia in HIV-infected patients on highly active anti-retroviral therapy in Kumasi MetropolisAfr Health Sci20131341107111624940339
- JantarapakdeJPhanuphakNChaturawitCPrevalence of metabolic syndrome among antiretroviral-naive and antiretroviral-experienced HIV-1 infected Thai adultsAIDS Patient Care STDS201428733134024914459
- TesfayeDYKindeSMedhinGBurden of metabolic syndrome among HIV-infected patients in Southern EthiopiaDiabetes Metab Syndr20148210210724907175
- PaulaAASchechterMTuboiSHContinuous increase of cardiovascular diseases, diabetes, and non-HIV related cancers as causes of death in HIV-infected individuals in Brazil: an analysis of nationwide dataPLoS One201494e9463624728320
- TripathiAJerrellJMLieseADAssociation of clinical and therapeutic factors with incident dyslipidemia in a cohort of human immunodeficiency virus-infected and non-infected adults: 1994–2011Metab Syndr Relat Disord201311641742623909647
- LedergerberBFurrerHRickenbachMFactors associated with the incidence of type 2 diabetes mellitus in HIV-infected participants in the Swiss HIV Cohort StudyClin Infect Dis200745111111917554711
- de WaalRCohenKMaartensGSystematic review of antiretroviral-associated lipodystrophy: lipoatrophy, but not central fat gain, is an antiretroviral adverse drug reactionPLoS One201385e6362323723990
- KotlerDPHIV lipodystrophy etiology and pathogenesis. Body composition and metabolic alterations: etiology and pathogenesisAIDS Read200313Suppl 4S5S912762287
- LemoineMSerfatyLCapeauJFrom nonalcoholic fatty liver to nonalcoholic steatohepatitis and cirrhosis in HIV-infected patients: diagnosis and managementCurr Opin Infect Dis2012251101622183113
- ArendtBMMohammedSSMaDWNon-alcoholic fatty liver disease in HIV infection associated with altered hepatic fatty acid compositionCurr HIV Res20119212813521434863
- Crum-CianfloneNKrauseDWessmanDFatty liver disease is associated with underlying cardiovascular disease in HIV-infected personsHIV Med201112846347121251186
- AhmedMHByrneCDModulation of sterol regulatory element binding proteins (SREBPs) as potential treatments for non-alcoholic fatty liver disease (NAFLD)Drug Discov Today20071217–1874074717826687
- AhmedMHByrneCDCurrent treatment of non-alcoholic fatty liver diseaseDiabetes Obes Metab200911318819518564173
- PriceJCSeabergECLatanichRRisk factors for fatty liver in the Multicenter AIDS Cohort StudyAm J Gastroenterol2014109569570424642579
- NishijimaTGatanagaHShimboTTraditional but not HIV-related factors are associated with nonalcoholic fatty liver disease in Asian patients with HIV-1 infectionPLoS One201491e8759624498148
- SterlingRKSmithPGBruntEMHepatic steatosis in human immunodeficiency virus: a prospective study in patients without viral hepatitis, diabetes, or alcohol abuseJ Clin Gastroenterol201347218218723059409
- MachadoMVOliveiraAGCortez-PintoHHepatic steatosis in patients coinfected with human immunodeficiency virus/hepatitis C virus: a meta-analysis of the risk factorsHepatology2010521717820578130
- Bani-SadrFBarangeKDaoudFPersistently normal alanine aminotransferase levels in HIV/HCV-coinfected patients: the role of steatosisHIV Med200910741742119490173
- SattarNPreissDMurrayHMStatins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trialsLancet2010375971673574220167359
- PreissDSeshasaiSRWelshPRisk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysisJAMA2011305242556256421693744
- CulverALOckeneISBalasubramanianRStatin use and risk of diabetes mellitus in postmenopausal women in the Women’s Health InitiativeArch Intern Med2012172214415222231607
- AthyrosVGMikhailidisDPPharmacotherapy: statins and new-onset diabetes mellitus – a matter for debateNat Rev Endocrinol20128313313422310848
- AthyrosVGTziomalosKKaragiannisAMikhailidisDPLipid-lowering agents and new onset diabetes mellitusExpert Opin Pharmacother201011121965197020486831
- HsiehMHLuPLKuoMCPrevalence of and associated factors with chronic kidney disease in human immunodeficiency virus-infected patients in TaiwanJ Microbiol Immunol Infect Epub1072013
- RaschMGEngsigFNFeldt-RasmussenBRenal function and incidence of chronic kidney disease in HIV patients: a Danish cohort studyScand J Infect Dis201244968969622680981
- WyattCMThe kidney in HIV infection: beyond HIV-associated nephropathyTop Antivir Med201220310611022954611
- MadalaNDThusiGPAssoungaAGNaickerSCharacteristics of South African patients presenting with kidney disease in rural KwaZulu-Natal: a cross sectional studyBMC Nephrol2014156124731300
- AhmedMHKhalilAAEzetimibe as a potential treatment for dyslipidemia associated with chronic renal failure and renal transplantSaudi J Kidney Dis Transpl20102161021102921060168
- ParsaAABhangooAHIV and thyroid dysfunctionRev Endocr Metab Disord201314212713123743889
- BeltranSLescureFXDesailloudRIncreased prevalence of hypothyroidism among human immunodeficiency virus-infected patients: a need for screeningClin Infect Dis200337457958312905143
- GómezQCVesgaGJLowenstein DeMEMass screening for hypothyroidism in a cohort of HIV infected patients in a Bogotá hospital, ColombiaRev Chilena Infectol20112815963 Spanish21526288
- KetsamathiCJongjaroenprasertWChailurkitLOUdomsubpayakulUKiertiburanakulSPrevalence of thyroid dysfunction in Thai HIV-infected patientsCurr HIV Res20064446346717073621
- WienerMLoYKleinRSAbnormal thyroid function in older men with or at risk for HIV infectionHIV Med20089754454918554308
- NoureldeenAQustiSYKhojaGMThyroid function in newly diagnosed HIV-infected patientsToxicol Ind Health2014301091992523188649
- de PommerolMHessamfarMLawson-AyayiSMenopause and HIV infection: age at onset and associated factors, ANRS CO3 Aquitaine cohortInt J STD AIDS2011222677221427426
- KojicEMWangCCCu-UvinSHIV and menopause: a reviewJ Womens Health (Larchmt)200716101402141118062755
- YinMTShuAZhangCATrabecular and cortical microarchitecture in postmenopausal HIV-infected womenCalcif Tissue Int201392655756523460340
- FerreiraCEPinto-NetoAMCondeDMCosta-PaivaLMoraisSSMagalhãesJMenopause symptoms in women infected with HIV: prevalence and associated factorsGynecol Endocrinol200723419820517505939
- LoutfyMRSonnenberg-SchwanUMargoleseSSherrLA review of reproductive health research, guidelines and related gaps for women living with HIVAIDS Care201325665766623088551
- IbrahimN’MohamedNShuidANUpdate on statins: hope for osteoporotic fracture healing treatmentCurr Drug Targets201314131524153223876090
- FournierJPDuijnhovenRGRenouxCDell’AnielloSKlungelOHSuissaSConcurrent use of statins and hormone therapy and risk of venous thromboembolism in postmenopausal women: a population-based case-control studyMenopause20142191023102624937027
- CardosoSWTorresTSSantini-OliveiraMMarinsLMVelosoVGGrinsztejnBAging with HIV: a practical reviewBraz J Infect Dis201317446447923711587
- AhmedMHHamadMARouthCConnollyVStatins as potential treatment for cholesterol gallstones: an attempt to understand the underlying mechanism of actionsExpert Opin Pharmacother201112172673268122043827
- AthyrosVGTziomalosKGossiosTDSafety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post-hoc analysisLancet201037697561916192221109302
- AthyrosVGTziomalosKDaskalopoulosGNKaragiannisAMikhailidisDPStatin-based treatment for cardiovascular risk and non-alcoholic fatty liver disease. Killing two birds with one stone?Ann Med201143316717121476786
- AthyrosVGMikhailidisDPDidangelosTPEffect of multifactorial treatment on non-alcoholic fatty liver disease in metabolic syndrome: a randomised studyCurr Med Res Opin200622587388316709309
- WilliamsDFeelyJPharmacokinetic-pharmacodynamic drug interactions with HMG-CoA reductase inhibitorsClin Pharmacokinet200241534337012036392
- PenzakSRChuckSKManagement of protease inhibitor-associated hyperlipidemiaAm J Cardiovasc Drugs2002229110614727985
- GerberJGRosenkranzSLFichtenbaumCJEffect of efavirenz on the pharmacokinetics of simvastatin, atorvastatin, and pravastatin: results of AIDS Clinical Trials Group 5108 StudyJ Acquir Immune Defic Syndr200539330731215980690
- MelroeNHKopaczewskiJHenryKHuebschJIntervention for hyperlipidemia associated with protease inhibitorsJ Assoc Nurses AIDS Care1999104556910394560
- DubeMPSteinJHAbergJAGuidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)-infected adults receiving antiretroviral therapy: recommendations of the HIV Medical Association of the Infectious Disease Society of America and the Adult AIDS Clinical Trials GroupClin Infect Dis200337561362712942391
- SchambelanMBensonCACarrAManagement of metabolic complications associated with antiretroviral therapy for HIV-1 infection: recommendations of an International AIDS Society-USA panelJ Acquir Immune Defic Syndr200231325727512439201
- LoJDyslipidemia and lipid management in HIV-infected patientsCurr Opin Endocrinol Diabetes Obes201118214414721297466
- SolerADeigEGuilJRodríguez-MartinMGuelarAPedrolEEffectiveness and tolerance of atorvastatin for antiretroviral therapy-secondary dyslipemiaMed Clin (Barc)20061277250252 Spanish16942727
- JacobsonTAComparative pharmacokinetic interaction profiles of pravastatin, simvastatin, and atorvastatin when coadministered with cytochrome P450 inhibitorsAm J Cardiol20049491140114615518608
- BonnetFAurillac-LavignolleVBreilhDPravastatin in HIV-infected patients treated with protease inhibitors: a placebo-controlled randomized studyHIV Clin Trials200781536017434849
- SteinJHMerwoodMABellehumeurJLEffects of pravastatin on lipoproteins and endothelial function in patients receiving human immunodeficiency virus protease inhibitorsAm Heart J20041474E1815077088
- AbergJAZackinRABrobstSWA randomized trial of the efficacy and safety of fenofibrate versus pravastatin in HIV-infected subjects with lipid abnormalities: AIDS Clinical Trials Group Study 5087AIDS Res Hum Retroviruses200521975776716218799
- CalzaLColangeliVManfrediRRosuvastatin for the treatment of hyperlipidaemia in HIV-infected patients receiving protease inhibitors: a pilot studyAIDS200519101103110515958843
- AhmedMHRosuvastatin as treatment for non alcoholic steatohepatitis (NASH) and highly active antiretroviral therapy (HAART)-dyslipidaemia: new treatment for global dangersMed Hypotheses200666244044116223568
- CalzaLManfrediRColangeliVPocaterraDPavoniMChiodoFRosuvastatin, pravastatin, and atorvastatin for the treatment of hypercholesterolaemia in HIV-infected patients receiving protease inhibitorsCurr HIV Res20086657257818991624
- AslangulEAssoumouLBittarRRosuvastatin versus pravastatin in dyslipidemic HIV-1-infected patients receiving protease inhibitors: a randomized trialAIDS2010241778319838098
- BottaroEGCaravelloOScapellatoPGRosuvastatin for the treatment of dyslipidemia in HIV-infected patients receiving highly active antiretroviral therapy. Preliminary experienceEnferm Infecc Microbiol Clin2008266325329 Spanish18588813
- SinghSWilligJHMugaveroMJComparative effectiveness and toxicity of statins among HIV-infected patientsClin Infect Dis201152338739521189273
- BenesicAZillyMKlugeFLipid lowering therapy with fluvastatin and pravastatin in patients with HIV infection and antiretroviral therapy: comparison of efficacy and interaction with indinavirInfection200432422923315293079
- CalzaLManfrediRChiodoFStatins and fibrates for the treatment of hyperlipidaemia in HIV-infected patients receiving HAARTAIDS200317685185912660532
- WohlDAWatersDSimpsonRJJrEzetimibe alone reduces low-density lipoprotein cholesterol in HIV-infected patients receiving combination antiretroviral therapyClin Infect Dis20084781105110818781882
- NegredoEMoltoJPuigJEzetimibe, a promising lipid-lowering agent for the treatment of dyslipidaemia in HIV-infected patients with poor response to statinsAIDS200620172159216417086055
- ChowDChenHGlesbyMJShort-term ezetimibe is well tolerated and effective in combination with statin therapy to treat elevated LDL cholesterol in HIV-infected patientsAIDS200923162133214119770624
- Berg-WolfMVKlibanovOMGaughanJPTedaldiEMEzetimibe combined with low-dose statin effectively lowers LDL in protease inhibitor treated patientsAIDS Patient Care STDS Epub572008
- ChastainLMBainAMEdwardsKLBedimoRBustiAJA retrospective study of the lipid-lowering efficacy and safety of ezetimibe added to hydroxy methylglutaryl coenzyme A reductase therapy in HIV-infected patients with hyperlipidemiaJ Clin Lipidol20071663463921291706
- BennettMTJohnsKWBondyGPEzetimibe is effective when added to maximally tolerated lipid lowering therapy in patients with HIVLipids Health Dis200761517565701
- SamineniDFichtenbaumCJFenofibrate in the treatment of dyslipidemia associated with HIV infectionExpert Opin Drug Metab Toxicol201068995100420604734
- BadiouSMerle De BoeverCDupuyAMBaillatVCristolJPReynesJFenofibrate improves the atherogenic lipid profile and enhances LDL resistance to oxidation in HIV-positive adultsAtherosclerosis2004172227327915019537
- ThomasJCLopes-VirellaMFDel BeneVEUse of fenofibrate in the management of protease inhibitor-associated lipid abnormalitiesPharmacotherapy200020672773410853629
- RaoAD’AmicoSBalasubramanyamAMaldonadoMFenofibrate is effective in treating hypertriglyceridemia associated with HIV lipodystrophyAm J Med Sci2004327631531815201643
- FichtenbaumCJYehTMEvansSRAbergJATreatment with pravastatin and fenofibrate improves atherogenic lipid profiles but not inflammatory markers in ACTG 5087J Clin Lipidol20104427928720824151
- BalasubramanyamACorazaISmithEOCombination of niacin and fenofibrate with lifestyle changes improves dyslipidemia and hypoadiponectinemia in HIV patients on antiretroviral therapy: results of “Heart Positive,” a randomized, controlled trialJ Clin Endocrinol Metab20119672236224721565796
- GerberJGKitchDWFichtenbaumCJFish oil and fenofibrate for the treatment of hypertriglyceridemia in HIV-infected subjects on antiretroviral therapy: results of ACTG A5186J Acquir Immune Defic Syndr200847445946617971707
- SamsonSLPownallHJScottLWHeart Positive: design of a randomized controlled clinical trial of intensive lifestyle intervention, niacin and fenofibrate for HIV lipodystrophy/dyslipidemiaContemp Clin Trials200627651853016914390
- SouzaSAChowDCWalshEJFordS3rdShikumaCPilot study on the safety and tolerability of extended release niacin for HIV-infected patients with hypertriglyceridemiaHawaii Med J201069512212520533755
- GerberMTMondyKEYarasheskiKENiacin in HIV-infected individuals with hyperlipidemia receiving potent antiretroviral therapyClin Infect Dis200439341942515307011
- DubéMPWuJWAbergJASafety and efficacy of extended-release niacin for the treatment of dyslipidaemia in patients with HIV infection: AIDS Clinical Trials Group Study A5148Antivir Ther20061181081108917302378