
Abstract
Leishmaniasis – human immunodeficiency virus (HIV) coinfection can manifest itself as tegumentary or visceral leishmaniasis. Almost 35 countries have reported autochthonous coinfections. Visceral leishmaniasis is more frequently described. However, usual and unusual manifestations of tegumentary leishmaniasis have been reported mainly in the Americas, but the real prevalence of Leishmania infection in HIV-infected patients is not clear. Regarding the clinical manifestations, there are some reports showing unusual manifestations in visceral leishmaniasis and tegumentary leishmaniasis in HIV-infected patients; yet, the usual manifestations are more frequent. Leishmaniasis diagnosis relies on clinical methods, but serological tests are used to diagnose visceral leishmaniasis despite them having a low sensitivity to tegumentary leishmaniasis. The search for the parasite is used to diagnose both visceral leishmaniasis and tegumentary leishmaniasis. Nevertheless, in HIV-infected patients, the sensitivity of serology is very low. Drugs available to treat leishmaniasis are more restricted and cause severe side effects. Furthermore, in HIV-infected patients, these side effects are more prominent and relapses and lethality are more recurrent. In this article, we discuss the current challenges of tegumentary leishmaniasis and visceral leishmaniasis–HIV infection, focusing mainly on the clinical manifestations, diagnosis, and treatment of leishmaniasis.
Introduction
The World Health Organization estimates that from about 900,000 to 1.3 million new cases of leishmaniasis are reported per year; of these, approximately 0.2–0.4 million are of visceral leishmaniasis (VL) and 0.7–1.2 million are of tegumentary leishmaniasis (TL).Citation1,Citation2 Leishmaniasis is endemic in over 98 countries and territories. It affects mainly some of the poorest people on earth, and is associated with malnutrition, population displacement, poor housing, a weak immune system, and lack of financial resources.Citation1,Citation3 The spread of the disease is linked to environmental changes such as deforestation, building of dams, irrigation schemes, and urbanization.Citation1 More than 90% of global VL cases occur in six countries: Bangladesh, Brazil, Ethiopia, India, South Sudan, and Sudan. On the other hand, Afghanistan, Algeria, Brazil, Colombia, Costa Rica, Ethiopia, Iran, Peru, Sudan, and Syria, together account for 70%–75% of the estimated global incidence of TL.Citation1 In Latin America, 96% of VL occurs in Brazil.Citation1,Citation2,Citation4
Human immunodeficiency virus (HIV) infection is a major public health problem globally; there are about 36.9 million people living with HIV and 2.0 million new infections are reported per year.Citation5 HIV is present in practically all countries and territories; however, the major burden of the disease is in sub-Saharan Africa, followed by Southeast Asia, the Americas, Europe, Western Pacific, and the Eastern Mediterranean area.Citation6 Clearly, we can observe an overlap between the transmission areas of HIV and leishmaniasis. As a result, there have been an increasing number of cases of HIV–Leishmania coinfection, which has spread throughout the world. Since the end of the 1980s, Leishmania–HIV coinfection has been reported in 35 countries. Most reports on the coinfection are related to VL and HIV, and little is known about the actual situation of TL–HIV coinfection. In fact, HIV has affected the occurrence of leishmaniasis, mainly VL. Five to six percent of the total cases of VL–HIV around the world occur in the Mediterranean area.Citation7 In some areas of Ethiopia, 35% of all leishmaniasis patients are coinfected with HIV,Citation8 and the trend is spreading to neighboring countries such as Sudan. In India, the prevalence of VL–HIV has increased from 0.88% in 2000 to 2.18% in 2006.Citation9 In Latin America, more precisely, in Brazil, the incidence of this coinfection has increased from 0.7% in 2001 to 8.5% in 2012.Citation10
Some factors related to host and environment can influence the prevalence of VL–HIV coinfection. HIV and Leishmania share an immunopathological mechanism, compromising dendritic cells and macrophages. This fact contributes to replication of both the pathogens, accelerating the progression of VL and HIV.Citation11,Citation12 Notably, immunosuppression is an important factor for the development of VL in patients living with HIV in endemic areas for VL and also for VL reactivation, that is, when a patient infected by HIV presents a decrease in cell immunity, mainly related to CD4+ T-cell count. Factors related to the route of HIV infection also influence the transmission of leishmaniasis. In Spain, 70% of Leishmania–HIV coinfection occurs in intravenous drug users, which is characterized by an anthroponotic transmission cycle of Leishmania, in which Leishmania DNA is found in the shared needles of intravenous drug users.Citation13,Citation14 Another important factor for the occurrence of VL–HIV coinfection is associated with economic migration of people, that is, they become infected in urban areas and then return to rural areas where VL is prevalent. This fact could be observed in Ethiopia’s rural areas where HIV infection is a risk factor for the immigrants to develop VL.Citation15
Demographic data related to Leishmania–HIV coinfection is now available, but abundant data is available for VL rather than TL. Young men are more prevalent in all the cohorts reported. In Spain, between 1997 and 2011, 99.4% of leishmaniasis–HIV coinfection occurred in males (86.4%) aged between 16 and 64 years.Citation16 In other areas, different age groups are affected by VL without HIV. In Brazil, VL is more common in children; however, in the coinfection with HIV, the incidence is more among young males between 29 and 49 years of age, which is the same age group as HIV-infected patients.Citation10 This point is crucial to detect an HIV infection in patients presenting with VL, because in 58% of them, VL is the first clinical manifestation of acquired immunodeficiency syndrome (AIDS).Citation17 Therefore, offering them an HIV test is mandatory. Also, it is important to start the Highly Active Antiretroviral Therapy (HAART) and change the treatment schedule as the drug and the doses used in VL–HIV coinfection are different from those used in VL alone.Citation10 Data related to TL and HIV are poor; there are some reports showing the prevalence in younger males,Citation18,Citation19 similar to that observed in patients not infected with HIV.
Especially in VL–HIV coinfection, a worrying situation is the increased relapse and lethality. Predictive factors of these outcomes are poorly known. Low CD4+ T-lymphocyte count, no increase in this cell count, and absence of secondary prophylaxis against VL in HIV-infected patients contribute to increased relapse and lethality.Citation20 However, none of these factors are related to the parasite. It is necessary to know TCD4+ count to start HAART as soon as possible, preferably with the use of protease inhibitors.Citation21 HAART can reduce not only relapse and lethality, but also the prevalence of VL–HIV coinfection. Clearly, a decrease of VL–HIV coinfection in Spain has been observed after the introduction of HAART.Citation22–Citation24 To date, there are no data about the impact of HAART on TL.
Different species of Leishmania can cause leishmaniasis, and they are involved in the development of TL () or VL. The genus Leishmania is divided into the subgenera Leishmania and Viannia. Around the world, 21 species of Leishmania can cause tegumentary or visceral lesions; however, Leishmania from the subgenus Viannia causes mainly tegumentary lesions and is autochthonous in the Americas.Citation25 Regarding the subgenus Leishmania, some species cause TL in Europe, Africa, and Asia, whereas some other species (Leishmania (Leishmania) infantum or Leishmania (Leishmania) infantum chagasi) cause VL in America and Europe and Leishmania (Leishmania) donovani causes VL in India and other Asian and African countries.Citation26 The occurrence of HIV infection can disrupt this scenario because the species causing VL can also cause tegumentary lesions in HIV-infected patients and the species causing TL can affect the internal organs such as the spleen and liver.
Table 1 Leishmania species related to clinical manifestation of tegumentary leishmaniasis.
We assume that most cases of VL or TL occur in HIV-infected patients because some clinical manifestations could be mistaken as those of other opportunistic infections in immunosuppressed patients presenting with visceral or tegumentary lesions. In AIDS, TL can be mistaken with the cutaneous lesions caused by histoplasmosis, cryptococcosis or tuberculosis. Visceral involvement can be easily confused with diseases affecting the spleen, liver, or bone marrow, mainly disseminated mycobacteriosis or tuberculosis and histoplasmosis.
Clinical manifestations
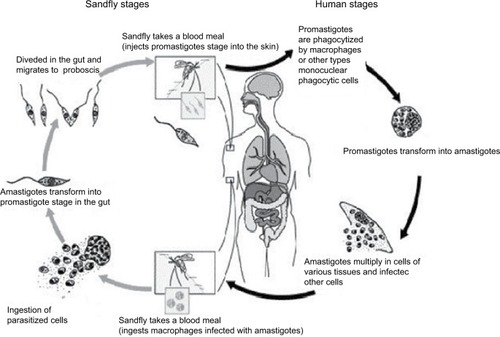
After transmission of Leishmania by sandfly or contaminated needles, the parasite enters into the macrophages or other types of cells. After multiplication of amastigotes, there is disruption of these cells and the parasites infect the other cells. Depending on the Leishmania species involved in the infection, TL or VL may be caused. After the sandfly takes a blood meal, ingesting the infected macrophages, transformation will occur into promastigotes within the digestive tract of the insect vector. When it takes a new blood meal, the infected females can transmit the promastigotes to the vertebrate host ().
Figure 1 Life cycle of Leishmania into the vertebrate and invertebrate host.
The wide spectrum of clinical presentations depends on the complex interplay between the infecting species, vector, immune and nutritional status of the host, age, genetic background of the host, inoculation site, and parasite load.Citation27–Citation29 Cutaneous, mucocutaneous, and visceral forms are the main clinical forms ( and ).Citation30
Figure 2 Lesions of tegumentary leishmaniasis.
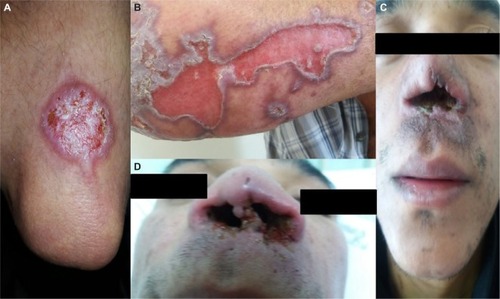
Figure 3 Clinical manifestation of visceral leishmaniasis in HIV-infected patient, showing hepatomegaly and splenomegaly.

Asymptomatic infections
The role of asymptomatic infection remains poorly recognized. Its proportion is five to ten times higher among immunocompetent hosts than the number of apparent VL cases infected as shown by serological evidence of anti-Leishmania antibodies, by detection of parasite DNA in blood samples, or by a positive reaction to the leishmanin skin test.Citation31–Citation34 Epidemiology of this asymptomatic infection in the parasite cycle is still unknown. Regarding the HIV-infected patients, the number of asymptomatic carriers also seems to be larger than the clinically evident VL patients.Citation35,Citation36 Association of a higher parasite load has already been demonstrated in those with higher HIV viral loads and appears to be related to a higher risk to develop the clinical disease. It has been shown that HIV infection may increase the risk of developing VL by 100 up to 2,300 times in endemic areas.Citation36–Citation38
Visceral leishmaniasis
The clinical presentation of VL in HIV-infected patients is equivalent to that observed in non-coinfected individuals. Typical forms comprise initially intermittent fever followed by a continuous pattern; nontender hepatosplenomegaly due to involvement of the reticuloendothelial system; pancytopenia, mainly due to parasites directly invading the bone marrow, causing signs and symptoms related to each cytopenia and leading to anemia, hemorrhages, and concurrent infections. Weight loss and anorexia may be misdiagnosed with other opportunistic infections or AIDS wasting syndrome itself.Citation31,Citation39 Furthermore, atypical VL remains undiagnosed in clinical settings, or is diagnosed with substantial delay, when early recognition and treatment are utmostly necessary. Most of the unusual clinical manifestations occur in patients with HIV with very low CD4+ T-cell counts. These patients might also be affected with other opportunistic infections, making timely etiologic diagnosis challenging.Citation40
In a trial regarding secondary prophylaxis for VL relapses, eight (15%) of 54 patients with VL coinfected with HIV, screened during 14 months, presented with atypical clinical presentation of leishmaniasis. Three of them had skin lesions (one patient with scattered nodular lesions and two with post–kala-azar dermal leishmaniasis-like lesions), two had oral lesions, two had lymph node involvement (one with intra-abdominal lymph node involvement), and one patient had rectal lesions.Citation40
Nevertheless, the main clinical differences between HIV-infected and non-coinfected individuals seem to be a wide variety of atypical and overlapping clinical presentations, with Leishmania parasites isolated from unusual sites (gastrointestinal and oral mucosa, skin, pleura, pericardium, lymph nodes, Kaposi’s sarcoma lesions, and respiratory tract).Citation41–Citation53 Moreover, it is noteworthy that the lower response rate to the treatment and the higher rate of relapse may be reduced by HAART, but not avoided entirely.Citation54
Tegumentary leishmaniasis
After the insect bite and an incubation period from 2 weeks to 3 months, a small erythematous, itchy papule or nodule appears, sometimes preceded or followed by draining lymph node enlargement. Its initial lesion may cure spontaneously or evolve into clinical disease after months.Citation29
Regarding the clinical forms of TL, they can be divided as follows:Citation55
Localized cutaneous leishmaniasis (LCL): It is the most frequent form that is commonly caused by dermotropic species. Often, lesions appear on an exposed area of the body surface (one to ten). The typical lesion is a round, well-delimited, painless ulcer with a central crust, which may be sometimes hemorrhagic. It may cure spontaneously, leading to a hypopigmented, smooth, thin scar.Citation56 L. major, L. aethiopica, L. tropica, L. mexicana, L. amazonensis, L. (V.) braziliensis, L. (V.) guyanensis, L. (V.) shawi, L. (V.) lainsoni, and L. (V.) naiffi can cause localized cutaneous leishmaniasis.
Leishmaniasis recidiva cutis: It is more common in the Old World.Citation57 It may produce papule and vesicular lesions after clinical cure in or around the scar of the already healed lesion, with a time frame that may vary from months to years. It is caused mainly by L. (L.) aethiopica and L. (V.) braziliensis.
Disseminated leishmaniasis: This causes multiple pleomorphic lesions (10–300), often acneiform and papular, in two or more noncontiguous areas of the body surface.Citation58 In this form, L. (V.) braziliensis seems to be the only species encountered.Citation59,Citation60
Diffuse cutaneous leishmaniasis: It is a rare condition with nodular lesions that do not evolve into ulcerations, and thus act as an anergic pattern. Typically, the lesions are rich in parasites and the species involved are: L. (L.) mexicana and L. (L.) amazonensis in the Americas and L. (L.) aethiopica in the Old World.Citation61
Mucocutaneous leishmaniasis: This occurs years after the onset of TL and is characterized by the destruction of oral–nasal and pharyngeal cavities that may evolve into disfiguring lesions. The clinical manifestations may start as a mild nasal inflammation and stuffiness, followed by ulcerations and perforations of the septum, extending to soft palate, pharynx, or larynx. It is caused mainly by L. (V.) braziliensis and L. (V.) guyanensis.
Regarding the HIV-infected patients, these manifestations seem to be similar to the non-coinfected ones, but they may be present in unusual forms. A wide variety of lesions have already been described in case series, such as papules, nodules, plaques, and diverse ulcerations forms. In addition, different forms of mucosal lesions have also been reported, such as widespread, diffuse infiltration of the mucosal surface of the palate and genital lesions, which were present in 27% of the patients in a series.Citation18,Citation62
IRIS and leishmaniasis
Generally, HAART has led to a significant decline in AIDS-associated morbidity and mortality due, in part, to the partial recovery of the immune system. Nevertheless, some individuals under HAART may experience clinical deterioration, despite concomitant increases in CD4+ T-lymphocyte counts and decreases in plasma HIV-1 viral loads. This fact is a result of an inflammatory response or “deregulation” of the immune system to both intact subclinical pathogens and residual antigens. As a result, clinical manifestations of this syndrome are diverse and depend on the infectious or noninfectious agents involved.Citation63–Citation66
In the case of Leishmania sp. infection, this restoration may be translated as a new disease or a progression of a latent one.Citation55 Three clinical variations of leishmaniasis with dermatological involvement have been reported: diffuse mucocutaneous, post– or para–kala-azar dermal leishmaniasis, and sporotrichoid dermal and subcutaneous nodules.Citation67 Few cases of TL as a manifestation of immune reconstitution inflammatory syndrome (IRIS) in patients with AIDS have been reported to date.Citation68–Citation70 In general, disseminated skin lesions (on the arms, lower limbs, and feet) and lesions in the nasal, oropharyngeal, as well as genital mucosa have been reported.Citation68
Although VL seems to be rare in the context of IRIS, it must be considered as a cause of sudden fever of unknown origin following the initiation of antiretroviral treatment in HIV patients from (or with travel history to) endemic areas.Citation71
Diagnosis of leishmaniasis in HIV-infected patient
Laboratory diagnosis of VL
Irrespective of the HIV status, parasitological diagnosis remains the confirmatory tool because of its high specificity.Citation9,Citation72 Lymph nodes, bone marrow, and spleen are the main tissues used for the demonstration of amastigote forms in preparations stained with Giemsa or Leishman stain.Citation72 In HIV-infected as well as in non-HIV-infected individuals, samples for microscopy from the spleen tissues have the best sensitivity, followed by those from bone marrow and lymph nodes.Citation73 Nevertheless, bone marrow aspiration is the most utilized exam due to its good sensitivity (67%–94%) and lower risk of complications compared to spleen aspiration.Citation74,Citation75 Culture can add sensitivity, but it needs a special medium (Novy–MacNeal–Nicolle medium), and it is usually not available in most endemic regions.Citation26
Regarding serological diagnosis in HIV-infected patients, there is limited evidence of the performance of the tests with a large variety of studies.Citation76 Serological tests are clearly less reliable in these patients,Citation73 and there are doubts about which technique is superior to others in this context.Citation10 For antibody demonstration, indirect immunofluorescence assay,Citation32 direct agglutination test (DAT), enzyme immunoassays, and immunoblotting can be utilized with variable sensitivity.Citation9,Citation76 Cota et al conducted a review including 33 studies and 1,489 patients, and showed an overall limited sensitivity of serological tests and observed that DAT and immunoblotting had a better performance compared to enzyme-linked immunosorbent assay and IFA.Citation76 In an original paper including 113 HIV-infected symptomatic patients, DAT exhibited good overall performance (positivity of 89%), with no statistical differences in comparison with molecular diagnosis. IFA and recombinant K39 antigen-based immunochromatographic test (rk39 dipstick test) presented the lowest sensitivity (45.6% and 60.9%, respectively).Citation77
In theory, methods to detect antigens would work better on the diagnosis of active leishmaniasis in HIV-infected patients, because they could be related to the parasite burden.Citation9 Despite this concept, a latex agglutination test kit (Katex) that detects antigen in urine samples showed satisfactory sensitivity and specificity in immunocompetent VL patients, but poorer sensitivity in HIV-coinfected individuals.Citation9,Citation78 In a study including a small sample of 13 individuals with HIV–Leishmania coinfection in Latin America, only five were Katex positive, while DAT positivity was 100%.Citation79
Molecular diagnosis of VL using various Leishmania gene target sequences is becoming increasingly relevant both in non–HIV- and HIV-infected patients.Citation9 Advantages include high sensitivity and specificity, possibility to use samples from peripheral blood or bone marrow, and possibility of laboratory follow-up in treated patients.Citation10 Thus, besides the diagnosis, it would be possible to monitor the efficacy of therapy, avoiding invasive procedures.Citation73 The positivity of polymerase chain reaction (PCR) varies considering the use of whole blood (less invasive) or bone marrow (83%–98% and 93%–100%, respectively).Citation76 It is important to note that PCR is not a unique method and that it is very difficult to compare different studies due to the different PCR targets utilized. Probably, PCR assay based on amplification of kinetoplast is the most sensible method to detect DNA from Leishmania.Citation77,Citation80 Real-time qPCR is an alternative for diagnosis and follow-up of infection, with a positivity of 85.7% in HIV-infected patients in Latin America.Citation77,Citation81 Although this method is considered a useful tool for the diagnosis of coinfected patients, it is noteworthy that asymptomatic individuals could show positive results,Citation77 which limits its use to the active disease diagnosis in areas of high transmission of VL.
Diagnosis of TL
Although there are case reports describing several clinical presentations of cutaneous leishmaniasis associated with HIV infection, there are no studies regarding laboratory diagnosis of cutaneous leishmaniasis exclusively in HIV-infected patients.Citation57,Citation82–Citation84 Theoretically, HIV-infected patients should show greater positivity in direct exams and lower accuracy in serological methods because of the host cell-mediated immune deficiency. However, there are no studies comparing the positivity of diagnostic methods in HIV-infected patients; therefore, all information available comes from reports and case series.Citation18
In VL, parasitological diagnosis remains the main test for diagnosis of cutaneous and mucocutaneous leishmaniasis due to its high specificity.Citation58 Direct exam of biopsy specimens, scrapings, or impression smears for amastigote search can be performed by Giemsa staining. This is the most common diagnostic approach because of its availability and easy execution. The sensitivity of the direct examination is low, especially in the Americas chronic and mucosal cases, which could also compromise the diagnosis of HIV-infected patients.Citation55,Citation58 Nevertheless, in a case series including 15 individuals, positivity of direct examination was 80%, probably due to severe immunosuppression of the patients involved.Citation18 Culture (Novy–MacNeal–Nicolle medium) of samples obtained through biopsy and aspirate samples can complement the diagnosis.Citation55
Molecular diagnosis is a promising field that has seen major growth in the last decades. Studies with immunocompetent patients have shown PCR-based methods to be useful, especially in cases of expected low parasite load, like in mucosal forms. Other advantages include the possibility of using different biological materials and easy identification of Leishmania species, which is also possible by culture, but it is more time consuming and expensive. Specificity and sensitivity of PCR-based methods can reach values near 100%. Real-time PCR is another approach with promising results. This technique can also detect the Leishmania genus and species, and gives more rapid results and causes less contamination.Citation55,Citation58 Regarding the diagnosis based on immunological test, leishmanin skin test (Montenegro test) can be used, but it can refer to past or present infections. This method can be associated with other tests to improve diagnosis.Citation25 Predominance of cellular immune response is related to positivity of leishmanin skin test. Therefore, it would be expected that patients with immunosuppression due to HIV infection could have negative Montenegro test as a result of predominance of T helper 2 (Th2) cell response in advanced disease. However, case reports showed high positivity of Montenegro test in HIV patients, opposing this concept and indicating that this test can help diagnosis, even in HIV-infected patients.Citation19,Citation84 Indirect immunofluorescence assay and enzyme-linked immunosorbent assay are the methods commonly used for the diagnosis of cutaneous leishmaniasis, but their sensitivity is considered low. This is a challenge in HIV-infected patients, because sometimes this is the only diagnostic tool available.Citation25 In the Mediterranean region, as expected, serological tests showed low sensitivity in HIV–Leishmania-infected individuals. However, in Brazil, the sensitivity was higher, reaching 77% in a small case series.Citation18 This discrepancy reveals the need for studies including more patients in order to establish the real importance of serological methods on leishmaniasis diagnosis in HIV-infected patients.
Treatment of Leishmania–HIV coinfection
As shown previously, leishmaniasis–HIV coinfection poses some difficulties for diagnosis, as well as in identifying the atypical clinical manifestations, either in visceral or tegumentary forms.Citation85 Patients with severe immunosuppression, presenting with opportunistic diseases, and using the highly effective HAART may have drug interaction problems. Briefly, drug interaction is widespread during the treatment of opportunistic infections and AIDS. Additional toxicity in the treatment for Leishmania–HIV coinfection should be avoided, and minimal side effects have to be sought. Coinfection is associated with high initial failures, relapses, drug toxicity, and mortality.Citation73
VL–HIV comorbidity has some particularities depending on the area studied, and drug combinations have been used. Liposomal amphotericin is the major drug used with better outcomes in coinfected individuals.Citation85 However, dosing is still a great problem, as there is no consensus on which is the best choice for different populations worldwide. A study conducted in South Asia showed that a single dose of 10 mg/kg of liposomal amphotericin B (LAmB) is sufficient to treat VL–HIV coinfected individuals; on the other hand, higher doses are necessary for the treatment of the same VL–HIV coinfection in Ethiopia.Citation86 In Brazil (where almost 90% of all VL cases from the Americas are reported), LAmB is recommended in a total dose of 20–40 mg/kg, although not based on clinical trials but only based on observational studies conducted in Latin America.Citation10 Few studies about miltefosine are available worldwide, showing limited efficacy and acceptable toxicity.Citation73 Although a combination therapy remains to be explored, a combination of LAmB (30 mg/kg) and miltefosine (100 mg/day for 14 days) has also been used for the treatment of coinfections in India with great results, as reported by Mahajan et al.Citation87 Antimonials still continue to be used to treat VL patients in East Africa and Latin America; however, for VL–HIV coinfection, they pose some difficulties. They are not only unsafe because of life-threatening toxicity, but also have low effectiveness and should be avoided in this population.Citation73,Citation88 Nevertheless, secondary prophylaxis with LAmB (3–4 mg/kg) every 2–4 weeks is recommended for preventing relapses of VL in HIV-coinfected individuals, since they have a high rate of annual recurrence. Other alternatives include the use of pentamidine isethionate monthly at a dose of 4 mg/kg.Citation89 HAART also has to be initiated to prevent VL relapses, as patients with lower CD4+ T-cell counts are at increased risk despite the use of secondary prophylaxis and effective initial treatment for VL.Citation89 Also, HIV-1 protease inhibitors have shown some inhibitory effect on Leishmania in vitro, even though in doses that would be unacceptable for human beings in vivo. Anyway, HAART with protease inhibitors, as a backbone combination therapy, would be preferable in this coinfected population, as it acts as a primary prophylaxis in asymptomatic Leishmania infection, as an adjunctive therapy in those with clinical manifestations, or as a maintenance therapy in those who are treatment unresponsive.Citation21
Studies regarding the treatment of TL–HIV coinfection are scarce and therapy must follow the guidelines established for immunocompetent individuals, based on epidemiology and the species of Leishmania involved. Instead of local therapy, systemic therapy is more frequently indicated for the treatment of TL–HIV coinfection. Moreover, the management of cutaneous or mucosal leishmaniasis can be challenging for the clinicians dealing with severe immunosuppression of HIV because there are higher risks of treatment failure and dissemination of Leishmania. Clinical healing of lesions and prevention of parasite dissemination by destroying them or improving the host’s immunity is the treatment goal of TL. As indicated by the Centers for Disease Control from the USA, antimonials (20 mg/kg Sb5+) intravenous/intramuscular for 28 days or LAmB as for VL (20–40 mg/kg) has shown great results in the treatment of cutaneous or mucocutaneous leishmaniasis in HIV-coinfected patients.Citation25,Citation55,Citation73 However, as in VL treatment, use of antimonials for TL therapy implicates some side effects, mainly cardiotoxicity and renal failure. Another study conducted in Sao Paulo, Brazil showed a good response to LAmB when used for the treatment of mucosal leishmaniasis.Citation90 Ultimately, no secondary prophylaxis is indicated for TL–HIV coinfection.Citation25
An important point to be explored in leishmaniasis treatment, both visceral and tegumentary, is the search for new active drugs against all species of Leishmania, focusing on the mechanism of action to eliminate the parasite. We support this point because after clinical cure is obtained, parasites continue to be present in some organs or lesions, and if immunosuppression is still present, reactivations or relapses of leishmaniasis may occur.
Current contents
Leishmania–HIV coinfection has spread around the world due to several factors related to the environment, host, or parasite. Different species of Leishmania can cause visceral or tegumentary lesions. Two species can cause VL (L. (L.) donovani and L. (L.) infantum [or L. (L.) infantum chagasi in the Americas]). Other species from the Leishmania genus can cause TL in the New or Old World, and Leishmania from Viannia genus causes only TL in the Americas. In HIV-infected patients, there are anecdotal cases such as cutaneous lesions caused by L. (L.) infantum or visceral lesions caused by dermotropic species. Most patients with visceral or cutaneous leishmaniasis and HIV infection have clinical manifestations similar to those of patients not infected with HIV; but unusual manifestations of cutaneous leishmaniasis and VL and usual manifestations of these clinical forms, such as IRIS, are described in patients with HIV/AIDS. Regarding treatment response, we observed an increase in relapse and lethality in VL–HIV coinfected patients despite having the same clinical manifestations as those occurring in VL alone. Diagnosis based on serology or skin test has failed, with the sensitivity being under 50% for VL due to immunosuppression. Parasitological methods have presented high positivity both for TL and VL. Nowadays, it is of paramount importance that the physicians working in nonendemic areas for leishmaniasis watch out for the possible diagnosis of leishmaniasis in HIV-infected patients and the physicians working in endemic areas for leishmaniasis watch out for unusual manifestations of leishmaniasis or relapses, which could be associated with HIV infection.
Disclosure
The authors report no conflicts of interest in this work.
References
- Organization WHControl of the LeishmaniasesGenevaWHO2010
- AlvarJVelezIDBernCLeishmaniasis worldwide and global estimates of its incidencePloS One201275e3567122693548
- AlvarJYactayoSBernCLeishmaniasis and povertyTrends Parasitol2006221255255717023215
- Pan American Health Organization WHOLeishmaniases: Epidemiological Report of the AmericasPan American Health Organization, World Health OrganizationWashington2013
- UNAIDSWorld AIDS Day Report 2012 [cited 2013 22 july 2013]; Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/JC2434_WorldAIDSday_results_en.pdf
- UNAIDSGlobal report: UNAIDS report on the global AIDS epidemicGenevaWorld Health Organization2012
- Monge-MailloBNormanFFCruzIAlvarJLopez-VelezRVisceral leishmaniasis and HIV coinfection in the Mediterranean regionPLoS Negl Trop Dis201488e302125144380
- DiroELynenLRitmeijerKBoelaertMHailuAvan GriensvenJVisceral Leishmaniasis and HIV coinfection in East AfricaPLoS Negl Trop Dis201486e286924968313
- SinghSChanging trends in the epidemiology, clinical presentation, and diagnosis of Leishmania-HIV co-infection in IndiaIJID20142910311225449244
- LindosoJACotaGFda CruzAMVisceral leishmaniasis and HIV coinfection in Latin AmericaPLoS Negl Trop Dis201489e313625233461
- GargRBaratCOuelletMLodgeRTremblayMJLeishmania infantum amastigotes enhance HIV-1 production in cocultures of human dendritic cells and CD4 T cells by inducing secretion of IL-6 and TNF-alphaPLoS Negl Trop Dis200935e44119468304
- BernierRTurcoSJOlivierMTremblayMActivation of human immunodeficiency virus type 1 in monocytoid cells by the protozoan parasite Leishmania donovaniJ Virol19956911728272857474154
- AlvarJCanavateCGutierrez-SolarBLeishmania and human immunodeficiency virus coinfection: the first 10 yearsClin Microbiol Rev19971022983199105756
- MolinaRGradoniLAlvarJHIV and the transmission of leishmaniaAnn Trop Med Parasit200397Suppl 1294514678631
- ArgawDMulugetaAHerreroMRisk factors for visceral Leishmaniasis among residents and migrants in Kafta-Humera, EthiopiaPLoS Negl Trop Dis2013711e254324244778
- HerradorZGherasimAJimenezBCGranadosMSan MartinJVAparicioPEpidemiological changes in leishmaniasis in Spain according to hospitalization-based records, 1997–2011: raising awareness towards leishmaniasis in non-HIV patientsPLoS Negl Trop Dis201593e000359425756785
- CotaGFde SousaMRde MendoncaALPatrocinioAAssunçãoLSde FariaSRRabelloALeishmania-HIV co-infection: clinical presentation and outcomes in an urban area in BrazilPLoS Negl Trop Dis201484e281624743472
- LindosoJABarbosaRNPosada-VergaraMPDuarteMIOyafusoLKAmatoVSGotoHUnusual manifestations of tegumentary leishmaniasis in AIDS patients from the new worldBr J Dermatol2009160231131819187345
- GuerraJACoelhoLIPereiraFRAmerican tegumentary leishmaniasis and HIV-AIDS association in a tertiary care center in the Brazilian AmazonAm J Trop Med Hyg201185352452721896816
- CotaGFde SousaMRRabelloAPredictors of visceral leishmaniasis relapse in HIV-infected patients: a systematic reviewPLoS Negl Trop Dis201156e115321666786
- van GriensvenJDiroELopez-VelezRHIV-1 protease inhibitors for treatment of visceral leishmaniasis in HIV-co-infected individualsLancet Infect Dis201313325125923427890
- Lopez-VelezRCasadoJLPintadoVDecline of a visceral leishmaniasis epidemic in HIV-infected patients after the introduction of highly active antiretroviral therapy (HAART)Clin Microbiol Infect20017739439511531992
- RussoRNigroLPanarelloGMontineriAClinical survey of Leishmania/HIV co-infection in Catania, Italy: the impact of highly active antiretroviral therapy (HAART)Ann Trop Med Parasitol200397Suppl 1149155
- del GiudicePMary-KrauseMPradierCImpact of highly active antiretroviral therapy on the incidence of visceral leishmaniasis in a French cohort of patients infected with human immunodeficiency virusJ Infect Dis200218691366137012402211
- GotoHLauletta LindosoJACutaneous and mucocutaneous leishmaniasisInfect Dis Clin North Am201226229330722632640
- van GriensvenJDiroEVisceral leishmaniasisInfect Dis Clin North Am201226230932222632641
- AkilovOEKhachemouneAHasanTClinical manifestations and classification of Old World cutaneous leishmaniasisInt J Dermatol200746213214217269962
- SchwartzEHatzCBlumJNew world cutaneous leishmaniasis in travellersLancet Infect Dis20066634234916728320
- BogdanCLeishmaniasis in rheumatology, haematology and oncology: epidemiological, immunological and clinical aspects and caveatsAnn Rheum Dis201271Suppl 2i60i6622460140
- SaporitoLGiammancoGMDe GraziaSColombaCVisceral leishmaniasis: host-parasite interactions and clinical presentation in the immunocompetent and in the immunocompromised hostIJID2013178e572e57623380419
- Organization WHControl of the leishmaniasesWorld Health Organ Tech Rep Ser2010949xiixiii1186 back cover21485694
- AntinoriSSchifanellaLCorbellinoMLeishmaniasis: new insights from an old and neglected diseaseEur J Clin Microbiol Infect Dis201231210911821533874
- DesjeuxPHuman leishmaniases: epidemiology and public health aspectsWorld Health Stat Q1992452–32672751462660
- SakthianandeswarenAFooteSJHandmanEThe role of host genetics in leishmaniasisTrends Parasitol200925838339119617002
- ColombaCSaporitoLVitaleFCryptic Leishmania infantum infection in Italian HIV infected patientsBMC Infect Dis2009919920003257
- EzraNOchoaMTCraftNHuman immunodeficiency virus and leishmaniasisJ Glob Infect Dis20102324825720927287
- KallelKAmmariLKaouechEBelhadjSAnaneSKilaniBChakerEAsymptomatic bearing of Leishmania infantum among Tunisian HIV infected patientsPathol Biol (Paris)2007551052152417888586
- García-GarcíaJAMartín-SánchezJGállegoMUse of noninvasive markers to detect leishmania infection in asymptomatic human immunodeficiency virus-infected patientsJ Clin Microbiol200644124455445817050814
- PearsonRDLareauSMJeronimoSMLeishmaniasis at the end of the millenniumCurr Infect Dis Rep19991544845211095822
- DiroEvan GriensvenJMohammedRAtypical manifestations of visceral leishmaniasis in patients with HIV in north Ethiopia: a gap in guidelines for the management of opportunistic infections in resource poor settingsLancet Infect Dis201515112212925300862
- EjaraEDLynenLBoelaertMVan GriensvenJChallenges in HIV and visceral Leishmania co-infection: future research directionsTrop Med Int Health201015101266126720723183
- AraMMailloCPeónGClavelACuestaJGrasaMPCarapetoFJVisceral leishmaniasis with cutaneous lesions in a patient infected with human immunodeficiency virusBr J Dermatol199813911141179764161
- BoschRJRodrigoABSánchezPde GálvezMVHerreraEPresence of Leishmania organisms in specific and non-specific skin lesions in HIV-infected individuals with visceral leishmaniasisInt J Dermatol2002411067067512390190
- González-BeatoMJMoyanoBSánchezCGonzález-BeatoMTPérez-MolinaJAMirallesPLázaroPKaposi’s sarcoma-like lesions and other nodules as cutaneous involvement in AIDS-related visceral leishmaniasisBr J Dermatol200014361316131811122042
- DereureJDuong ThanhHLavabre-BertrandTVisceral leishmaniasis. Persistence of parasites in lymph nodes after clinical cureJ Infect2003471778112850167
- AliagaLCoboFMediavillaJDLocalized mucosal leishmaniasis due to Leishmania (Leishmania) infantum: clinical and microbiologic findings in 31 patientsMedicine (Baltimore)200382314715812792301
- AlbrechtHStellbrinkHJGrossGBergBHelmchenUMensingHTreatment of atypical leishmaniasis with interferon gamma resulting in progression of Kaposi’s sarcoma in an AIDS patientClin Investig1994721210411047
- AlonsoMJMuñozEPicazoADuodenal leishmaniasis diagnosed by biopsy in two HIV-positive patientsPathol Res Pract199719314347 discussion 49–509112272
- AngaranoGMaggiPRolloMALaroccaAMQuartoMScaloneAGradoniLDiffuse necrotic hepatic lesions due to visceral leishmaniasis in AIDSJ Infect19983621671699570648
- BalkhairABen AbidFGastric and cutaneous dissemination of visceral leishmaniasis in a patient with advanced HIVIJID200812111111317643333
- BetzPElsingCPurrmannJFrenzelHLeishmaniasis of the upper gastrointestinal tract in an HIV positive patientPathologe199011297100 German2330354
- CánovasDLCarbonellJTorresJAltésJBuadesJLaryngeal leishmaniasis as initial opportunistic disease in HIV infectionJ Laryngol Otol199410812108910927861090
- HeudierPTaillanBGarnierGMartyPFuzibetJGDujardinPPulmonary site of visceral leishmaniasis in HIV infectionPresse Med199322221060
- López-VélezRThe impact of highly active antiretroviral therapy (HAART) on visceral leishmaniasis in Spanish patients who are co-infected with HIVAnn Trop Med Parasitol200397Suppl 114314714678641
- GotoHLindosoJACurrent diagnosis and treatment of cutaneous and mucocutaneous leishmaniasisExpert Rev Anti Infect Ther20108441943320377337
- ScarisbrickJJChiodiniPLWatsonJClinical features and diagnosis of 42 travellers with cutaneous leishmaniasisTravel Med Infect Dis200641142116887720
- MachadoESBraga MdaPDa CruzAMDisseminated American muco-cutaneous leishmaniasis caused by Leishmania braziliensis braziliensis in a patient with AIDS: a case reportMem Inst Oswaldo Cruz19928744874921343662
- ReithingerRDujardinJCLouzirHPirmezCAlexanderBBrookerSCutaneous leishmaniasisLancet Infect Dis20077958159617714672
- TuretzMLMachadoPRKoAIDisseminated leishmaniasis: a new and emerging form of leishmaniasis observed in northeastern BrazilJ Infect Dis2002186121829183412447770
- CostaJMMarsdenPDLlanos-CuentasEADisseminated cutaneous leishmaniasis in a field clinic in Bahia, Brazil: a report of eight casesJ Trop Med Hyg19868963193233806749
- BarralACostaJMBittencourtALBarral-NettoMCarvalhoEMPolar and subpolar diffuse cutaneous leishmaniasis in Brazil: clinical and immunopathologic aspectsInt J Dermatol19953474744797591410
- PuigLPradinaudRLeishmania and HIV co-infection: dermatological manifestationsAnn Trop Med Parasitol200397Suppl 110711414678638
- NaritaMAshkinDHollenderESPitchenikAEParadoxical worsening of tuberculosis following antiretroviral therapy in patients with AIDSAm J Respir Crit Care Med199815811571619655723
- Gea-BanaclocheJCClifford LaneHImmune reconstitution in HIV infectionAIDS (London, England)199913Suppl AS25S38
- StoneSFPricePKeaneNMMurrayRJFrenchMALevels of IL-6 and soluble IL-6 receptor are increased in HIV patients with a history of immune restoration disease after HAARTHIV Med200231212712059947
- KovalCEGigliottiFNevinsDDemeterLMImmune reconstitution syndrome after successful treatment of Pneumocystis carinii pneumonia in a man with human immunodeficiency virus type 1 infectionClin Infect Dis200235449149312145736
- AmersonEHMaurerTAImmune reconstitution inflammatory syndrome and tropical dermatosesDermatol Clin2011291394321095526
- Posada-VergaraMPLindosoJATolezanoJEPereira-ChioccolaVLSilvaMVGotoHTegumentary leishmaniasis as a manifestation of immune reconstitution inflammatory syndrome in 2 patients with AIDSJ Infect Dis2005192101819182216235183
- SinhaSFernándezGKapilaRLambertWCSchwartzRADiffuse cutaneous leishmaniasis associated with the immune reconstitution inflammatory syndromeInt J Dermatol200847121263127019126013
- Chrusciak-TalhariARibeiro-RodriguesRTalhariCTegumentary leishmaniasis as the cause of immune reconstitution inflammatory syndrome in a patient co-infected with human immunodeficiency virus and Leishmania guyanensisAnn Trop Med Parasitol2009814559564
- SchleenvoigtBTIgnatiusRBaierMDevelopment of visceral leishmaniasis in an HIV(+) patient upon immune reconstitution following the initiation of antiretroviral therapyInfection201644111511926123228
- SrivastavaPDayamaAMehrotraSSundarSDiagnosis of visceral leishmaniasisTrans R Soc Trop Med Hyg201110511621074233
- van GriensvenJCarrilloELopez-VelezRLynenLMorenoJLeishmaniasis in immunosuppressed individualsClin Microbiol Infect201420428629924450618
- AlvarJAparicioPAseffaAThe relationship between leishmaniasis and AIDS: the second 10 yearsClin Microb Rev2008212334359 table of contents
- LimaIPMullerMCHolandaTAHarhayMCostaCHCostaDLHuman immunodeficiency virus/Leishmania infantum in the first foci of urban American visceral leishmaniasis: clinical presentation from 1994 to 2010Rev Soc Bras Med Trop201346215616023666663
- CotaGFde SousaMRDemarquiFNRabelloAThe diagnostic accuracy of serologic and molecular methods for detecting visceral leishmaniasis in HIV infected patients: meta-analysisPLoS Negl Trop Dis201265e166522666514
- CotaGFde SousaMRde Freitas NogueiraBMComparison of parasitological, serological, and molecular tests for visceral leishmaniasis in HIV-infected patients: a cross-sectional delayed-type studyAm J Trop Med Hyg201389357057723836568
- AttarZJChanceMLel-SafiSLatex agglutination test for the detection of urinary antigens in visceral leishmaniasisActa Trop2001781111611164745
- Barbosa JuniorWLRamos de AraujoPSDias de AndradeLRapid tests and the diagnosis of visceral leishmaniasis and human immunodeficiency virus/acquired immunodeficiency syndrome coinfectionAm J Trop Med Hyg201593596796926416105
- NuzumEWhiteF3rdThakurCDietzeRWagesJGroglMBermanJDiagnosis of symptomatic visceral leishmaniasis by use of the polymerase chain reaction on patient bloodJ Infect Dis199517137517547876635
- BossolascoSGaieraGOlchiniDReal-time PCR assay for clinical management of human immunodeficiency virus-infected patients with visceral leishmaniasisJ Clin Microbiol200341115080508414605142
- HozannahASantosMChrusciak-TalhariATalhariCLeishmaniasis and AIDS coinfectionAn Bras Dermatol201388699299324474115
- SampaioRNSalaroCPResendePde PaulaCDAmerican cutaneous leishmaniasis associated with HIV/AIDS: report of four clinical casesRev Soc Bras Med Trop2002356651654 Portuguese12612749
- MattosMCaizaAFernandesOGonçalvesAJPirmezCSouzaCSOliveira-NetoMPAmerican cutaneous leishmaniasis associated with HIV infection: report of four casesJ Eur Acad Dermatol Venereol19981032182259643324
- ZijlstraEEVisceral leishmaniasis: a forgotten epidemicArch Dis Child2016101656156726895806
- BalasegaramMRitmeijerKLimaMALiposomal amphotericin B as a treatment for human leishmaniasisExpert Opin Emerg Drugs201217449351023167833
- MahajanRDasPIsaakidisPCombination treatment for visceral leishmaniasis patients coinfected with human immunodeficiency virus in IndiaClin Infect Dis20156181255126226129756
- DiroELynenLMohammedRBoelaertMHailuAvan GriensvenJHigh parasitological failure rate of visceral leishmaniasis to sodium stibogluconate among HIV co-infected adults in EthiopiaPLoS Negl Trop Dis201485e287524854196
- DiroERitmeijerKBoelaertMUse of pentamidine as secondary prophylaxis to prevent visceral leishmaniasis relapse in HIV infected patients, the first twelve months of a prospective cohort studyPLoS Negl Trop Dis2015910e000408726431253
- CunhaMALeaoACde Cassia SolerRLindosoJAEfficacy and safety of liposomal amphotericin B for the treatment of mucosal leishmaniasis from the new world: a retrospective studyAm J Trop Med Hyg20159361214121826483120