Abstract
This paper reviews the current situation concerning nutrition-related noncommunicable diseases (N-NCDs) and the risk factors associated with these diseases in the Eastern Mediterranean region (EMR). A systematic literature review of studies and reports published between January 1, 1990 and September 15, 2011 was conducted using the PubMed and Google Scholar databases. Cardiovascular disease, type 2 diabetes, metabolic syndrome, obesity, cancer, and osteoporosis have become the main causes of morbidity and mortality, especially with progressive aging of the population. The estimated mortality rate due to cardiovascular disease and diabetes ranged from 179.8 to 765.2 per 100,000 population, with the highest rates in poor countries. The prevalence of metabolic syndrome was very high, ranging from 19% to 45%. The prevalence of overweight and obesity (body mass index ≥25 kg/m2) has reached an alarming level in most countries of the region, ranging from 25% to 82%, with a higher prevalence among women. The estimated mortality rate for cancer ranged from 61.9 to 151 per 100,000 population. Osteoporosis has become a critical problem, particularly among women. Several risk factors may be contributing to the high prevalence of N-NCDs in EMR, including nutrition transition, low intake of fruit and vegetables, demographic transition, urbanization, physical inactivity, hypertension, tobacco smoking, stunting of growth of preschool children, and lack of nutrition and health awareness. Intervention programs to prevent and control N-NCDs are urgently needed, with special focus on promotion of healthy eating and physical activity.
Introduction
Nutrition-related noncommunicable diseases (N-NCDs) are the most frequent cause of morbidity and mortality in most countries in the Eastern Mediterranean region (EMR), particularly cardiovascular disease, diabetes, and cancer.Citation1 The main risk factors for these noncommunicable diseases include high blood pressure, high concentrations of serum cholesterol, tobacco smoking, unhealthy eating habits, overweight or obesity, and physical inactivity. Demographic and socioeconomic status is another factor linked with N-NCDs in this region.
The EMR countries are also characterized by large numbers of young people. In fact, the majority of the Arab population (54%) is under the age of 25 years.Citation2 Therefore, future projection of N-NCD prevalence rates might reach epidemic levels, with serious consequences for morbidity and mortality.Citation1 N-NCDs can develop even in the younger age groups, because childhood and adolescent obesity elevates the risk of these diseases. Several studies have indicated a high prevalence of overweight and obesity among children and adolescents in the EMR,Citation3–Citation8 as well as prevalence of other risk factors, such as high blood pressure,Citation9–Citation11 physical inactivity,Citation12–Citation15 unhealthy eating,Citation16–Citation18 and hyperlipidemia.Citation19,Citation20 This review highlights the magnitude of N-NCDs in the EMR and discusses possible factors associated with the prevalence of these diseases.
Methods
The search for this review was based on articles and reports on N-NCDs published between January 1, 1990, and September 15, 2011, using the PubMed and Google Scholar databases, in addition to reports published by regional and international organizations. The search covered the EMR countries, including all Arab countries (except Algeria), Afghanistan, Iran, and Pakistan, according to World Health Organization categorization.
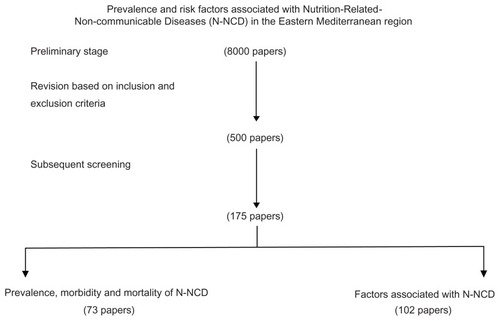
The following key words were used when searching the electronic databases: cardiovascular disease, diabetes, cancer, hypertension, obesity, osteoporosis, dyslipidemia, food consumption, diet, nutrition, physical activity, and smoking, for each country in the region. The titles and abstracts of all articles of potential interest were reviewed for possible inclusion/exclusion in this review. More than 8000 papers were identified at the preliminary stage. The abstracts were then reviewed carefully for final inclusion. The inclusion and exclusion criteria were based on the following:
Only national data on the morbidity and mortality of N-NCDs were included. Therefore, the recent national data provided by the World Health Organization for cardiovascular disease, diabetes, and cancer were considered carefully because these are age-standardized, which make comparison between countries more reliable. For the prevalence of obesity among the various age groups, the search was done on national prevalence published in the literature. When more than one set of national data were available, the most recent one was included.
Morbidity and mortality data from town, rural, urban, and specific ethnic groups, as well as hospital-based data in certain areas, were excluded (most exclusions were in this category)
Studies of an animal or purely biological nature were excluded, because this is an epidemiological review.
For the factors associated with N-NCDs, 1–5 examples were chosen for each disease, as available. The selection of these examples was based on variations between countries, sample size, and year of publication. Consequently, a large number of papers were excluded, especially from countries that had numerous publications on N-NCDs, such as Iran and Saudi Arabia.
Based on the above criteria, we identified 500 papers and reports, and with subsequent screening 175 papers were included in this review ().
Figure 1 Flow chart for processing of the review.
Nutrition-related noncommunicable diseases in EMR
Cardiovascular disease
The EMR is clearly witnessing an increase in cardiovascular disease that is being escalated by the rapidly aging population. Citation2 In a systematic review on stroke in Arab countries, Benamer and GrossetCitation21 found that the annual stroke incidence ranged from 27.5 to 63 per 100,000 population. Ischemic stroke was the commonest subtype in all series. Hypertension, diabetes mellitus, hyperlipidemia, and cardiac disease were the most common risk factors. Another systemic review in Iran, covering publication dates from 1990 to 2008, reported that the annual stroke incidence of various ages in Iran ranged from 23 to 103 per 100,000 population.Citation22
The estimated mortality from cardiovascular disease and diabetes in the EMR reported by the World Health Organization indicated that poor countries such as Djibouti, Somalia, Sudan, and Yemen have one of the highest mortality rates in the region (ranging from 525.6 to 570.7 for men and from 445.7 to 573.4 for women per 100,000 population). Excluding Jordan and Oman (both of which have a high rate), the mortality rate for men ranged from 179.8 in Qatar to 477.3 in Egypt per 100,000 population. For women, the mortality rate ranged from 239.3 in Qatar to 384 in Egypt per 100,000 population. The high mortality rates for cardiovascular disease and diabetes in poor countries may be due to the health systems in these countries, where treatment of chronic diseases is inadequate due to lack of specialized health personnel, inadequate facilities, lack of intensive care, lack of medicines, and lack of awareness among patients.
The prevalence of hypercholesterolemia is considerably high in this region, which may contribute to the high risk of cardiovascular disease. It was estimated that elevated total cholesterol levels ranged from 31% to 58% among adults in the region.Citation23 Data in indicate that increased total cholesterol was more prevalent among female adults in eight countries of the 10 EMR countries included in the World Health Organization database.
Table 1 Prevalence (%) of raised blood pressure, raised blood glucose and raised total cholesterol (aged-standardized adjusted estimates) among adults in the Eastern Mediterranean countries
Hypercholesterolemia was also reported among children and adolescents in the region, with a high prevalence of obesity and inactivity in these age groups,Citation19,Citation20 so the risk of cardiovascular disease in young and middle-aged adults is expected to rise in the future. A study of 1–6-year-old children in Saudi Arabia revealed an overall range for serum cholesterol of 201–507 mmol/L. A total of 6.9% were at borderline risk and 1.6% were at high risk.Citation24 In Tunisia, the prevalence of hypercholesterolemia in 13–19-year-old adolescents was 8.1%.Citation25 A national survey on risk factors for N-NCD in Egyptian adolescents aged 10–18 years reported 10% with borderline and 6% with high levels (≥200 mg/dL) of total cholesterol. This survey also revealed a low high-density lipoprotein cholesterol levels in 9.4% of adolescents, while 7.5% and 10.3% had high and borderline levels, respectively.Citation26 In Kuwait, the prevalence of dyslipidemia was found to be 10.5% in college-aged students.Citation27
Type 2 diabetes
Most of the studies on type 2 diabetes in the EMR are hospital-based, with a focus on clinical factors linked with diabetes, and few of the published studies represent nationally-based diabetic prevalence surveys utilizing World Health Organization criteria. These studies showed that the prevalence of diabetes among adults ranged from 10% to 15%.Citation28 In general, the prevalence of type 2 diabetes in this region has been increasing dramatically during the past two decades. For example, the prevalence of diabetes in Tunisia has doubled over the past 15 years.Citation29 In Jordan, the prevalence has increased by 31.5% from 1994 to 2006.Citation30 Of the 91 countries in which diabetes prevalence has been studied, five of the ten countries with the world’s highest reported rates have been in the EMR, namely the United Arab Emirates, Saudi Arabia, Bahrain, Kuwait, and Oman. It is no coincidence that all of these countries are experiencing nutrition transition. The prevalence of diabetes in these countries is projected to continue to rise during the 2010–2030 period, if the same trend continues.Citation31 Many EMR countries have been reporting the onset of type 2 diabetes in increasingly younger age groups. Such a pattern of diabetes onset extends the potential burden of therapy to an even younger age group for an even longer period of time. It was estimated that, of the total adult population of 220 million in the region, 17 million people have diabetes, with further dramatic increases expected in the future.Citation21
Age-standardized adjusted estimates for raised blood glucose in the EMR countries showed the highest prevalence among Saudi men and women (20 years and older) at 22% and 21.7%, respectively. The prevalence in Egypt was 7% and in Jordan reached 18%. In general, the prevalence rates in men and women were very close (). However, the proportion of underdiagnosed diabetes and prediabetes is considerably high, which means that the burden of diabetes on health care systems in this region is substantially large.Citation32 In Iran, for example, 47% of diabetes cases can be attributed to newly diagnosed disease.Citation33
Cancer
Cancer is an increasing problem in the EMR and ranks as the fourth leading cause of death. It is estimated that cancer kills 270,000 people each year in the EMR. Moreover, the largest increase in cancer incidence among the World Health Organization regions in the next 15 years is likely to be in EMR, in which projection modeling predicts an increase between 100% and 180%.Citation34 Half of the cancer cases in the region occur before the age of 55 years, which is 10–20 years younger than in industrialized countries.Citation34 The mortality rate is 70%, which is higher than in the US (40%) and Europe (55%), indicating significantly lower survival rates after diagnosed cancer.Citation32 Estimated data for mortality due to cancer was found to be the highest in Lebanon (151.2 and 113.2 per 100,000 population for men and women, respectively), whereas the lowest mortality rate for men was observed in United Arab Emirates (63.4) and that for women was in Syria (47.2).Citation23
Breast cancer occupies the number one prevalence position in most countries of the region. El Salim et alCitation35 reported that cases of breast cancer in Arab countries tend to be young and almost half of the patients are younger than 50 years of age, with a median age of 49–52 years as compared with 63 years in industrialized nations. In a review of cancer registrations in the Arab Gulf countries, breast cancer was the most common cancer among women, ranging from 16.1% in Oman to 35.4% in Bahrain. The age-standardized incidence rate (per 100,000 population) was the highest in Bahrain (46.4), followed by Kuwait (44.3), Qatar (35.5), United Arab Emirates (19.2), Oman (14.4), and Saudi Arabia (12.9). However, these rates are still low compared with most developed countries. Citation36 Although the incidence of lung cancer is lower than in Western countries, it is ranked number one in two countries (Bahrain and Tunisia) and number two in four countries (Iraq, Jordan, Kuwait, and Lebanon) in the region. Colon cancer is among the top five cancers in most EMR countries.Citation34 A low intake of fruit and vegetables and low physical activity could be the leading factors associated with this type of cancer. BenerCitation37 suggested that the main risk factors that were positively associated with colon cancer in developing countries are physical inactivity, obesity, abdominal adiposity, alcohol consumption, smoking, and high consumption of red meat and fat. Protective factors included consumption of white meat and fiber-rich foods.
Esophageal cancer is also a matter of concern, given that it is among the top five cancers in seven countries. It is the second most common type of cancer in Iran and Yemen. It is believed that the habit of chewing tobacco in Iran and Khat in Yemen may play a role in the high incidence of esophageal cancer in these two countries.Citation34,Citation35 Although there is a lack of studies on the prevalence of cancer among children, it is increasing in the region. In the Arab Gulf countries, it was reported that the rate of pediatric cancer ranged from 4% in Bahrain to 9.5% in Saudi Arabia and the United Arab Emirates.Citation38
Osteoporosis
Osteoporosis is perceived to be rapidly increasing in the EMR, due to the progressive aging of the population. Osteoporosis is currently known as a systemic skeletal disorder that affects bone density and quality, leading to bone fragility and increased risk of fractures. It is defined as a T-score less than −2.5. The T-score is the number of standard deviations separating an individual’s bone mineral density from the peak bone mineral density of young adults. Bone mineral density is considered normal if it is above −1.0. Bone mineral density appears to be lower on average in the EMR compared with industrialized countries, with the T-score being lower by 0.3–0.6.Citation39
Studies conducted in Iran,Citation40 Lebanon,Citation41 Qatar,Citation42 Saudi Arabia,Citation43,Citation44 Tunisia,Citation45 and MoroccoCitation46 showed that vitamin D levels and bone mineral density were below the standard established in Western countries. The exception to this is Kuwait,Citation47 where the bone mineral density reference level was similar to that in Western countries. Reduced vitamin D and calcium intake by people in the region may be contributing substantially to the high rates of osteoporosis. In Lebanon, for example, it was found that the average daily vitamin D intake by adults 30–50 years was 100.3 ± 67.9 IU, which is much lower than the recommended daily allowance of 200 IU. This intake was significantly higher (P < 0.001) in men than in women (127.5 ± 79.7 IU versus 87.9 ± 57.9 IU). Dietary calcium intake (average 683 ± 275 mg/day) was also lower than the recommended daily intake of 1000 mg, and the difference between men (778 ± 327 mg/day) and women (237 ± 88 mg/day) was statistically significant (P < 0.001).Citation48 In Saudi Arabia, it was found that 81% of school children aged 12–15 years had low serum vitamin D levels, ranging from 2.2 to 24.0 mmol/dL.Citation49
The main risk factors for osteoporosis in the EMR based on the published literature are low vitamin D and calcium intake, inadequate exposure to sunlight, heavy smoking (>20 cigarettes per day), a family history of osteoporosis, being female and postmenopausal for more than two years, low physical activity, thinness, and small body build.Citation50
Overweight and obesity
The prevalence of overweight and obesity among both children and adults in the EMR has increased markedly during the past three decades. In Saudi Arabia, for example, Al-HazzaaCitation51 showed that the prevalence of obesity among schoolboys aged 6–14 years increased seven-fold between 1988 and 2005 (from 3.4% to 24.5%, respectively). The average body fat percentage increased by 49.2% for the same period. In general, all anthropometric measurements increased during this period except for lean body mass. In Iran, the overall prevalence of obesity among adults increased from 13.6% in 1999 to 22.3% in 2007 (odds ratio [OR] 1.08 per year, P < 0.001). Overweight prevalence increased during the same period from 32.2% to 36.3% (OR 1.02 per year, P < 0.001).Citation52
A case-control study in 52 countries showed that adult men in the Middle East have the second highest mean body mass index (27.4) after adults in the US (27.7). Mean body mass index in the rest of the regions ranged from 24.0 in Southeast Asia to 27.0 in Australia and New Zealand. In women, the highest body mass index and waist-to-hip ratio were recorded in the Middle East (body mass index 29.5, and waist-to-hip ratio 0.92).Citation53
Data presented in and indicate that the prevalence of overweight and obesity among adults is considerably high, with the proportion of overweight in men ranging from 19.2% in Libya to 51.7% in Tunisia, while the corresponding proportions in women were 21.1% in Libya and 71% in Tunisia. The prevalence of obesity ranged from 5.7% in Morocco to 39% in Kuwait for men, and from 7.1% in Libya to 53% in Kuwait for women. The prevalence of overweight in EMR among preschool children (0–5 years) ranged from 1.9% in Oman to 21.9% in Syria. Among schoolchildren and adolescents (6–18 years), the prevalence of overweight in males ranged from 5.4% in Iran to 29.3% in Kuwait. Similarly, in females, it ranged from 5.9% in Iran to 32% in Kuwait. With regard to obesity, the prevalence in males ranged from 1.6% in Iran to 24.8% in Kuwait, and a similar pattern was seen in females, with the proportion ranging from 1.3% in Iran to 20% in Kuwait, as shown in and . Unfortunately, the complications of childhood obesity are rarely considered by health authorities in the region, given that they are not clinically apparent until many years after onset of obesity. Clinical studies of obese children indicate development of a vast range of medical consequences, including sleep apnea, asthma, fatty liver disease, menstrual problems and early menarche, type 2 diabetes, hypertension, increased low-density lipoprotein cholesterol, raised serum triglyceride levels, and psychological and social consequences.Citation54
Table 2 National prevalence of overweight and obesity among male preschool children, schoolchildren, adolescents, and adults in Eastern Mediterranean region
Table 3 National prevalence of overweight and obesity among female preschool children, schoolchildren, adolescents, and adults in Eastern Mediterranean region
Metabolic syndrome
The metabolic syndrome is a complex disorder and composed of several metabolic abnormalities, each of which is considered to be a risk factor for cardiovascular disease.Citation53 With the large increase in obesity rates among both adolescents and adults, the metabolic syndrome is also increasing. A high prevalence of metabolic syndrome has been reported in most EMR countries, ranging from 19% to 45%.Citation55–Citation63 For example, the prevalence of metabolic syndrome in the Arab Gulf countries was some 10%–15% higher than in most developing countries, with a higher prevalence among women. The proportion of metabolic syndrome in the Arab Gulf countries ranged from 20.7% to 37.2% using the third Adult Treatment Panel (ATP III) definition, and from 29.6% to 36.2% using the International Diabetes Federation definition.Citation64
There has been a limited number of studies related to pediatric metabolic syndrome in EMR countries. Two studies were carried out in Iran using modified ATP III criteria for metabolic syndrome, and indicated a high prevalence of metabolic syndrome. Esmaillzadeh et alCitation65 found that the prevalence of metabolic syndrome among Iranian adolescents aged 10–19 years was 10.1% (95% confidence interval [CI] 9.0–11.1), whereas Kelishadi et alCitation66 reported a prevalence of 14.1% among Iranian adolescents aged 6–18 years. In Saudi Arabia, Al-DaghriCitation67 found that the overall prevalence of metabolic syndrome among children aged 10–18 years was 9.4% (95% CI 7.8–11.0). A combination of interacting genetic, environmental, and behavioral factors may be responsible for the occurrence of metabolic syndrome in both children and adults.Citation68 Research on the association between dietary habits in children and metabolic syndrome in the EMR is mostly absent. One study has reported a correlation between metabolic syndrome and dietary intake in children and adolescents from this region. It was found that the risk of metabolic syndrome among Iranian children and adolescents (aged 14–19 years) rose with the consumption of solid hydrogenated fat and white bread. The frequent intake of sweets/candies increased the risk of metabolic syndrome in both genders. The frequency of eating fast foods increased this risk in boys but not in girls, and vice versa for carbohydrate-rich foods. In both genders, the intake of fruit, vegetables, and dairy products decreased the risk of metabolic syndrome.Citation69
Factors associated with N-NCDs in EMR
Nutrition transition
Nutrition transition, documented by several studies in the EMR,Citation70–Citation74 is characterized by considerable changes in food intake and dietary behavior in the population. The shift from a traditional diet to a more westernized diet, with a high energy and fat-rich food intake, eating out, and an increase in food portion sizes are apparent in most countries in the EMR. These changes may increase the risk for obesity and other metabolic disorders. Data calculated from the Food Balance SheetCitation75 showed that there has been a decrease in the consumption of red meat by 4.3% and an increase in the consumption of poultry meat by 51.9% in the EMR during the period 1990–2005. However, the daily per capita availability of fruit and vegetables in the region has declined by 7.8% and 0.3%, respectively. It is worth mentioning that there was a great variation between countries in respect to changes in patterns of food consumption.
In order to test the relationship between change in dietary intake and obesity, Esmaillzadeh and AzadbakhtCitation76 examined the association of obesity with three dietary patterns (healthy, Western, and Iranian) in 486 Iranian women aged 40–60 years. They found that women in the upper category of the healthy pattern scores were less likely to be obese, based on body mass index (OR 0.28, 95% CI 0.14–0.53) or be centrally obese, based on waist circumference (OR 0.30, 95% CI 0.16–0.55). Women in the upper quintile of the Western dietary pattern had greater odds for general obesity (OR 2.73, 95% CI 1.46–5.08) and for central obesity (OR 5.74, 95% CI 2.99–10.99). The association between dietary patterns and general obesity in Iran was not statistically significant. However, subjects in the highest quintile of Iranian dietary patterns had greater odds of being centrally obese either before (OR 2.15, 95% CI 1.18–3.90) or after (OR 2.08, 95% CI 1.09–3.65) control of potential confounders.
High income and urbanization are the main drivers of nutrition transition and emergence of N-NCDs in some countries in the EMR. With the rapid improvement in the economy, people are becoming affluent and are consuming diets high in saturated fat, cholesterol, salt, and refined carbohydrates, and low in polyunsaturated fats and fiber, along with a marked sedentary lifestyle and increased stress.Citation77 High fat consumption has been reported by several studies in this region,Citation78–Citation80 and saturated fats represent a high proportion of the daily energy intake. In Egypt, for instance, MahmoodCitation81 found that total fat was contributing 37% of total energy intake in women.
Unhealthy eating habits and high fat intake have also been reported among school children and adolescents in the region. Unhealthy eating habits among school children aged 6–18 years were studied nationwide in Iran.Citation82 It was found that hydrogenated solid fat was the main type of fat frequently consumed at home (73.8%), about 58% of the children consumed white bread, and 79.3% admitted to adding salt to the food they consumed. The average frequency of deep-fried foods consumed at home was four times per week. Fruit, vegetables, and dairy products were consumed twice a day. Using three categories of a healthy eating index, ie, poor diet, needs improvement, and good diet, it was found that 74%, 23%, and 3%, respectively, of adolescents in Tehran were in these categories. There was a significant negative correlation between healthy eating score and fat intake (r = −0.2, P < 0.001), percentage of saturated fatty acid (r = −0.2, P < 0.05) and cholesterol intake (r = −0.4, P < 0.05), and the ratio of polysaturated/saturated fatty acids in the diet (r = 0.2, P < 0.05).Citation83
Data on the frequency and quantity of food eaten outside the home is another factor which could be associated with obesity.Citation84 The increase in family income and the higher proportion of working women may have contributed substantially to the increase in eating out, the nutritional quality of which is of concern. The increasing frequency of eating out at restaurants and fast food outlets has had a great impact on the dietary habits of people in the region.Citation8 BashourCitation85 showed that 67.4% of male adolescents (13–18 years) in Syria frequently eat outside the home compared with 54.5% of female adolescents (P < 0.001). Food eaten outside the home was more likely to be high in total energy, total fat, saturated fat, cholesterol, and sodium, but be lower in dietary fiber and calcium. In Iran, Hejazi and MazloomCitation86 found a significant difference in mean daily energy intake (P < 0.007) between adolescents (12–16 years) who ate at least one meal away from home (1618 kCal) and those who did not eat outside their homes (1472 kCal).
As a result of nutrition transition, the intake of sugar-sweetened beverages has increased and that of whole grain food has decreased. More and more evidence has been reported on the negative health impact of sugar-sweetened beverages, because regular consumption of these beverages not only contributes to obesity but also to an increased risk of type 2 diabetes and metabolic syndrome.Citation87 The consumption of sugar-sweetened beverages in the EMR is relatively high among both children and adults.Citation88–Citation91 In Kuwait, a high proportion of children (11–13 years) reported consuming sweets (42%), soft drinks (43%), and cakes (31%) several times a day. Further, when all the associated variables were analyzed together using the logistic regression model, lifestyle, school satisfaction, and self-esteem factors appeared to have a stronger association with frequent sugar consumption than did gender, grade, or nationality.Citation88 A cross-sectional study of 9433 Saudi Arabian schoolchildren aged 10–19 years demonstrated that waist circumference and body mass index were positively correlated with sugar-sweetened carbonated beverage intake in boys only (P < 0.0001). However, the intake of these beverages was positively associated with poor dietary choices in both males and females. Correlations between sugar-sweetened drinks and fast foods, savory snacks, iced desserts, and total sugar in boys were 0.39, 0.13, 0.10, and 0.52, respectively (P < 0.001), while the corresponding relationships in girls were 0.45, 0.23, 0.16, and 0.55, respectively (P < 0.001).Citation89
Whole grain cereal intake is associated with many health benefits, including lower body mass index, and lower incidences of type 2 diabetes, cardiovascular disease, and colorectal cancer.Citation92 In general, the contribution of complex carbohydrates (a rich source of dietary fiber and other nutrients) decreased in the 1971–2005 period, and the percentage of this contribution decreased as the per capita income of a country rose. For example, the contribution of complex carbohydrates to daily energy supply was 60%–70% in low-income countries but decreased to 50%–60% and 45%–50% in middle-income and high-income countries, respectively, in the EMR.Citation75 Mean consumption of whole grains and refined grains by Iranian adults (18–74 years) was 93 ± 29 g/day and 201 ± 57 g/day, respectively. Whole grain intake was inversely associated and refined grain was positively associated with the risk of hypertriglyceridemia. Moreover, the proportion of obesity was lower among subjects in the highest quintile of whole grain intake and higher among those in the highest quintile of refined grain intake compared with the corresponding lower quintiles.Citation93
Low intake of fruit and vegetables
Low intake of fruit and vegetables was reported in children and adolescents,Citation94,Citation95 as well as in adults Citation96,Citation97 in many countries in the EMR. Lock et alCitation98 calculated fruit and vegetable intake worldwide, and showed that this was inadequate in EMR countries. In general, the intake was lower than the recommended daily allowance (>400 g) in all age groups and in both genders, except in men aged 45 years and over in poor countries, in addition to Egypt, Iraq, and Morocco. The intake of fruit and vegetables increased with age. For example, the daily consumption of fruit and vegetables ranged from 174 g to 218 g among children aged 0–4 years, increased to 296–348 g among those aged 15–29 years, and to 336–442 g among subjects aged 70–79 years.
There is good evidence that an adequate intake of fruit and vegetables is protective against certain chronic diseases, including obesity, cardiovascular disease, and some types of cancer.Citation99,Citation100 Al-Roomi et alCitation101 conducted a case-control study of lifestyle factors associated with acute myocardial infarction in adults aged 20–79 years in Bahrain. After adjusting for several demographic and health variables, the odds of having a first myocardial infarction in subjects with an infrequent intake of fruit (<3 times/week) was 1.57 (95% CI 0.61–2.53) and in those with an infrequent intake of vegetables (<3 times/week) was 1.40, (95% CI 0.77–2.52), with both rates being higher than in control subjects. After adjusting for several potentially confounding factors, the fruit and vegetable intake in Iranian women aged 18–74 years was found to be significantly and inversely associated with cardiovascular disease.Citation102 In a community-based case-control study in Iran, it was found that a high intake of allium vegetables (OR 0.35) and fruit (OR 0.37) were significantly protective against gastric cancer. However, consumption of red meat (OR 0.34) and dairy products (OR 2.28) was positively associated with risk of gastric cancer. People with a higher reported salt intake (OR 3.10) and drinking strong (OR 2.64) and hot (OR 2.85) tea were at higher risk.Citation103
Kelishadi et alCitation104 found that fruit and vegetable intake had a negative association with obesity among adolescents (11–18 years) in Iran. Adolescents of normal weight (body mass index <85th percentile) were more likely to consume fruit (6.2 ± 1.8 times/week) and vegetables (5.9 ± 1.4 times/week) than overweight/obese adolescents (≥85th percentile), whose intakes were 4.2 ± 1.1 times/week and 3.8 ± 1.2 times/week, respectively. The difference was statistically significant (P < 0.04 and P < 0.03, respectively). A study in university students in Kuwait revealed that regular consumption of fruit and vegetables is protective against obesity (OR 0.55, 95% CI 0.20–1.40 and OR 0.55, 95% CI 0.30–2.24, for fruit and vegetables, respectively).
Demographic transition
The decreasing fertility rate in EMR countries is due to many factors. In poor-income and middle-income countries, economic hardship has introduced a different stimulus for fertility decline. The demographic transition appears to be a product of both development and underdevelopment. For rich countries (such as the Arab Gulf states), more recent changes in the fertility rate are prompted by both the high cost of living and a marked improvement in education for women.Citation105
Excluding Oman, poor countries such as Afghanistan, Djibouti, Pakistan, Palestine, Somalia, Sudan, and Yemen showed the highest decline in fertility during the 2000–2005 period. The average fertility rate for the EMR countries is expected to decrease from 4.2 in 2000–2005 to 2.8 per 1000 population in 2025–2030 (a decrease of 33%), with a further decline to 2.2 is projected for 2045–2050 (a decrease of 21%). Life expectancy is expected to increase sharply in 2000–2050, especially in poor countries, and is already high in the high-income and middle-income countries. The average life expectancy in 2000–2050 will increase from 66.7 to 76.6 years, representing a 15% rise. However, the life expectancy will range from 62.4 years in Afghanistan to 81.1 years in Kuwait during 2045–2050. Consequently, the percentage of the aged population (≥60 years) will increase. The average percentage increase for all the EMR countries will be from 5.8% in 2000–2005 to 15% of the total population in 2045–2050, ranging from 5.8% in Djibouti to 25.7% in Kuwait.Citation106
Urbanization
There is a growing shift in the urban-rural population balance in the EMR. According to recent Arab human development report, the region has been characterized by large movements from rural to urban areas. This rapid urbanization is coupled with increased growth of large cities.Citation2 In fact, in the Arab Gulf states, the vast majority of the population is already living in urban areas, while urbanization is growing fast in middle-income and low-income countries in the region.Citation107 Urbanization means a shift from traditional foods to fast and convenience foods, more female participation in the workforce, more reliance on cars and other types of transportation, higher income, more television viewing, more use of computers and the Internet, a more sedentary lifestyle and less physical activity, and ultimately a more stressful life. Therefore, urbanization will intensify the burden of N-NCDs in the region.Citation108
Urbanization and increased income has led to increasing consumption of white bread, sugar, and excess fat, and decreasing consumption of oils, grains, legumes, and vegetables. This has led to higher consumption of saturated fat, increased total energy and carbohydrate intake, and decreased intake of vitamin C and fiber.Citation109 In Egypt, the ratio of saturated fat to total energy was 11.9 ± 5.2 and 7.4 ± 4.6 (P < 0.0001) among urban and rural men, respectively. The corresponding proportions for women were 10.7 ± 4.3 and 8.5 ± 4.6 (P < 0.013), respectively.Citation110 In Iraq, statistically significant differences between urban and rural populations have been identified in preference for sweetness and sugar consumption. The urban groups consumed a mean of 4.1 teaspoons of sugar per cup of tea versus 1.7 teaspoons per cup for rural groups (P < 0.001). The urban group consumed 62.3 g of sugar in tea per day, compared with 16.6 g for the rural groups. The longer the subjects had been living in the city, the greater was their preference for sweetness (r = 0.43, P < 0.001). Daily consumption of sugar in tea increased from 10 g/day for those living in the city for 2 years or less to 182 g/day for those who had lived for more than 15 years in the city (r = 0.68, P < 0.001).Citation111 A comparison of dietary habits in Pakistani schoolchildren aged 10–12 years from six groups of rural and urban areas showed different patterns. With urbanization, the intake of fat and sugar increased steadily, while that of carbohydrates and fiber decreased.Citation112
Inactivity and sedentary lifestyle
There is growing evidence that inactivity and a sedentary lifestyle are associated with increased risk of N-NCDs.Citation113 Changes to labor-saving occupations, a high dependence on cars and buses for transportation, massive urbanization, propagated satellite television, and increased reliance on computers and telecommunication technology have all led to a more sedentary lifestyle and reduced energy expenditure in most EMR countries. Therefore, leisure activities have changed from outdoor play to indoor entertainment.Citation107 Data on trends in occupational activity in this region are scarce. However, mere observation shows that there has been a great shift from manual work to office work, especially in high-income and middle-income countries. In the Arab Gulf states, for example, people have shifted from farming, pearl diving, and fishing to less physically demanding office work such as banking, selling, accounting, management, teaching, and other administrative work. Manual work in these states has been delegated to migrants, especially from the Indian-subcontinent and the Far East.Citation114
In the majority of countries in the region, there is a paucity of reliable data on physical activity, especially for children and adolescents. Surprisingly, national surveillance data on physical activity are lacking, and most available physical activity/inactivity data are included as one item and as part of wider surveillance of health or noncommunicable diseases. Thus, existing physical activity research in the EMR is hampered by limited reliable data, varying methodology, and different physical activity instruments used by different researchers.Citation115 Some national and local studies have surveyed only leisure-time physical activity and sports,Citation116,Citation117 while a few studies have assessed all domains of physical activity, including occupational, transport, household, yard/garden, and leisure/sports.Citation118 Therefore, it is difficult to make any meaningful comparison between findings from these studies, except for the World Health Organization STEPwise approach to noncommunicable disease surveillance, where similar methodology and instrumentation were used.
Using the stepwise approach of the World Health OrganizationCitation119 to study the risk factors for N-NCDs in eight EMR countries, it was found that the prevalence of low daily physical activity (less than 10 minutes per day) among adults aged 15 years and above was high. Among men, the prevalence was highest in Sudan (75.9%) and lowest in Syria (21.3%), with the comparable percentages in women being 94.8% and 41% in Sudan and Syria, respectively ().
Table 4 National prevalence of risk factors for diet-related chronic noncommunicable diseases in selected Eastern Mediterranean countries in persons aged ≥15 years using the STEPwise approach to surveillance
The Global School Health Survey from 2003–2007Citation120 defined sedentary behavior as the percentage of adolescents spending three or more hours per day sitting, watching television, playing computer games, or talking to friends. In this survey, the proportion of sedentary activity reported for schoolchildren in some EMR countries ranged from 22.4% for boys in Egypt to 44% for adolescents in Jordan. In general, there does not seem to be a large difference between the percentages of sedentary males and females. In addition, the Global School Health Survey findings indicated that schoolchildren from the United Arab Emirates had the lowest prevalence of walking or riding a bicycle to school of all the countries surveyed.
Recently, a multicenter epidemiological survey has been in progress among adolescents in the major Arab cities, ie, the Arab Teens Lifestyle Study, which is using standardized methodology and a valid instrument for the assessment of physical activity, sedentary behavior, and dietary habits among adolescents in the major Arab cities. It is hoped that this project will provide much needed lifestyle information on Arab adolescents.Citation121
Decreased physical activity among schoolchildren and adolescents has been suggested to be a result of increased time spent watching television, playing computer games, and using the Internet, and decreased opportunities for physical activity in schools and communities.Citation82 Several studies in the region have demonstrated that obesity is more prevalent among children watching television for more than 2 hours a day, compared with those who watch television for less than two hours a day.Citation122–Citation124 In Iran, Kelishadi et alCitation82 indicated that the mean length of time per day spent by schoolchildren aged 16–18 years watching television and/or at the computer (playing games or on the Internet) was 4.6 hours and 4.1 hours for boys and girls, respectively, and there was a significant (P < 0.0001) correlation with obesity in both genders (r = 0.61 and 0.48, respectively).
Television occupies much leisure time for both children and adults. Television affects food consumption and lifestyle in three ways, ie, lengthy watching of television has been cited as a contributing factor to higher intake of energy and fat, exposure to television advertising, especially commercials for fast foods and convenience foods, may influence the food choices of viewers towards high intake of fat and energy, and more lengthy watching of television means less physical activity and a more sedentary lifestyle.Citation8,Citation84
Hypertension
Hypertension affects 26% of the total population in the EMR. Prehypertension (blood pressure 120–139/80–89 mmHg) doubles the risk of developing hypertension and should be treated essentially with lifestyle modification. Lowering blood pressure reduces stroke by 35%–40%, myocardial infarction by 20%–25%, and heart failure by more than 50%.Citation125 Hypertension, in general, is underdiagnosed and undertreated in the EMR, meaning the current prevalence of hypertension is likely to be underestimated in these countries. In the United Arab Emirates, it was found that 33% of people aged 40–60 years were underdiagnosed for hypertension and 76% were undertreated.Citation126 In general, the prevalence of elevated blood pressure in EMR countries is considerably high, ranging from 38.8% in Egypt to 51.7% in Libya for male adults. The corresponding range for female adults is 32.5% in the United Arab Emirates and 46.0% in Morocco. With the exception of Morocco, women were less likely to have hypertension than men ().
A sedentary lifestyle, unhealthy eating habits, a high salt intake, and a relatively high prevalence of obesity among adolescents in the EMR may lead to early occurrence of high blood pressure in this age group.Citation127 In a nationwide study which included 16,226 Saudi children and adolescents from birth to 18 years, systolic blood pressure rose steadily with age in both boys and girls. The annual increase in systolic blood pressure was 1.66 mmHg for boys and 1.44 mmHg for girls, while that for diastolic blood pressure was 0.83 mmHg for boys and 0.77 mmHg for girls. Diastolic blood pressure rose sharply in boys at the age of 18 years.Citation128 In Iraq, the prevalence of hypertension was shown to be 1.8-fold higher among obese school children aged 6–12 years (4.7%) than in their nonobese counterparts (2.6%, P < 0.05). The overall prevalence of hypertension was 1.7%, with significantly more high systolic (1.1%) than high diastolic (0.6%, P < 0.05) blood pressure.Citation129 The prevalence of elevated blood pressure among Tunisian adolescents aged 15–19 years was 37.4% ± 1.8% (44.7% ± 2.7% for males versus 30% ± 2.3% for females, P < 0.0001), and that of hypertension was 5.2% ± 1.0% (5% ± 1.4% for males versus 5.3% ± 1.0% for females, P < 0.096).Citation109
Tobacco smoking
Tobacco smoking is a well documented risk factor for many chronic diseases, especially cardiovascular disease, diabetes, and lung cancer.Citation130,Citation131 The prevalence of smoking in EMR countries in males and females aged 15 years and above has been reported by the World Health Organization and the Regional Office for the Eastern Mediterranean.Citation34 For prevalence among males, countries can be divided into three categories, ie, countries with a very high prevalence of tobacco smoking (57%–77%), including Djibouti, Tunisia, and Yemen; countries with a moderate prevalence of tobacco smoking (30%–48%), including Egypt, Iraq, Jordan, Kuwait, Lebanon, Morocco, Pakistan, Palestine, Qatar, and Syria; and countries with a relatively low prevalence of tobacco smoking (<30%), include the rest of the EMR countries. For females, two countries reporting a high prevalence were Lebanon (35%) and Yemen (29%), while the prevalence in other countries ranged from 1.0% to 9%. However, it is worth noting that the prevalence of smoking among women is mostly under-reported, due to cultural factors and, therefore, the actual prevalence may be higher than what is documented.
The proportion of tobacco smoking in the region was also found to be high among schoolchildren and adolescents,Citation132–Citation136 medical students,Citation137,Citation138 and physicians.Citation139 For example, 25% of Iraqi male adolescents in Kurdistan were reported to be currently smokers, compared with 2.7% in females.Citation132 In Tunisia, the prevalence of current smoking was higher (33%) among adolescent males aged 13–15 years compared with 4.8% among females.Citation133 Similar patterns were noticed among secondary school students in Lebanon,Citation134 Saudi Arabia,Citation135 and Iran.Citation136 Among medical students, Almerie et alCitation137 showed that 15.8% of male medical students in Syria were current smokers compared with 3.3% of females. The prevalence of smoking in the western region of Saudi Arabia was 24.8% in male medical students compared with 9.1% in females.Citation138 Behbehani et alCitation139 reported a study of smoking among physicians in Bahrain and Kuwait, finding that 14.6% and 13.4% of physicians, respectively, in these two countries were current smokers.
The high prevalence of smoking among secondary schoolchildren and women in this region could be attributed to high use of water-pipe tobacco smoking. Water-pipe smoking in the EMR countries is traditionally the domain of men; however, this type of smoking has increased dramatically among both men and women in the past 15 years. A recent systematic review on the prevalence of tobacco smoking reported a concerning high use of water-pipe smoking among school and university students in the Middle Eastern countries as well as among Middle Eastern immigrants living in Western countries.Citation140 A multinational study carried out among school students (13–15 years) in Gulf Cooperative Council countries showed that the prevalence of water-pipe smoking was 15% in Bahrain, 16% in Kuwait, 9% in Oman, 14% in Qatar, 15% in the United Arab Emirates, and 15% in Yemen. The study found that boys were significantly more likely to smoke a water-pipe than girls, except in Qatar, and water-pipe smoking among these groups was more common than cigarette smoking in most of the countries studied.Citation141 Similar patterns of water-pipe smoking were observed in university students in the region, with a prevalence rate for ever use ranging from 8% to 64% in males and 3% to 37% in females.Citation142–Citation146 About 6.4% of physicians in Bahrain were current water-pipe smokers, while the prevalence was 12% in their Kuwaiti counterparts.Citation139
Several factors may explain the steady increase in water-pipe smoking in the region: first, the social acceptance of water-pipe smoking, especially in women; second, the misperception that water-pipe smoking is less harmful than cigarette smoking; third, the widespread emergence of coffee shops which provide water-pipes for both men and women; and fourth, the lack of legislation to control water-pipe smoking in public.
The very high smoking rate (77%) reported for Yemen could be linked with khat chewing. Khat is a leafy green plant containing cathinone and cathine as active ingredients. The khat-chewing habit is widespread in Yemen and Somalia. The erroneous belief that khat chewing does not have any negative effects on health has played an important role in the high khat chewing rates in these countries. Ali et alCitation147 showed that khat chewing carries a significantly higher risk of cardiogenic shock, stroke, and mortality. After adjustment of baseline variables, khat chewing was an independent risk factor for inhospital mortality (OR 1.9, 95% CI 1.3–2.7, P < 0.001) and stroke (OR 2.7, 95% CI 1.3–5.9, P < 0.01).
Stunting
Recent findings showed that stunting (short height for age) is comorbid with overweight or obesity in the same child and other members of the same household. Research has shown that stunted children are more likely to be overweight in countries undergoing a rapid nutrition transition.Citation8 Stunting is the most common type of undernutrition prevalent among preschool children (0–5 years) in the EMR. It has been estimated that the prevalence of stunting among children under five years ranged from 8% in Qatar to 53% in Yemen.Citation148 In a study of overweight and stunting from large national surveys conducted between 2001 and 2004 in five countries in the EMR (Djibouti, Libya, Morocco, Syria, and Yemen), El-Taguri et alCitation149 showed that the risk ratio for overweight in stunted children ranged from 2.14 in Djibouti to 3.85 in Libya.
Lack of nutrition and health awareness
The lack of knowledge and the negative attitudes of the public regarding risk factors for N-NCDs may be important barriers to the prevention and control of these diseases. In a study conducted to assess knowledge about stroke among the general public in the Arab Gulf countries, it was found that the majority (71%) of subjects had not even heard the term stroke. About 29% considered the age group 30–50 years to be at highest risk for stroke. The commonest risk factors identified were hypertension (23%) and smoking (27%). People who did not know the term stroke had a higher incidence of diabetes, hypertension, and had more than one risk factor (P < 0.05). In a univariate comparison, younger age (P < 0.001), higher education (P < 0.001), and female gender (P < 0.008) were the best predictors of knowledge about stroke. However, when a multivariate logistic regression model was used, educational level, monthly income, and smoking independently predicted knowledge about stroke.Citation150
In Bahrain, Musaiger et alCitation151 found that there was a large deficit in knowledge among adults about risk factors for osteoporosis. For example, 45% of men and 42% of women did not know that exposure to sunlight can help to reduce the risk. About 38% of men and 32% of women believed that green leafy vegetables are the best source of calcium rather than milk and dairy products. Only 40% of men and 53% of women believed that only women are at risk of osteoporosis, while the rest either disagreed or did not know. Misconceptions and inadequate knowledge regarding obesity were studied among Arab women,Citation152 and it was found that 43% of women believed that drinking a lot of water led to obesity. About 54% of the women believed that wrapping the abdomen with clothes after delivery helps to decrease abdominal fat. Also, 31% of the women believed that skipping breakfast helps in reducing weight. Similar findings were reported among adolescents in BahrainCitation153 and university students in the United Arab Emirates.Citation154
Physicians and medical students in the EMR were also shown to be deficient regarding important nutritional information. Citation155,Citation156 It was found that 52% and 77% of physicians and medical students, respectively, in Iran did not know the amount of energy intake needed per kilogram per day for the average person. About 42% and 81% of physicians and medical students, respectively, did not know the correct percentage of energy needed from fat, carbohydrates, and protein in a healthy diet.Citation155 Al-NumairCitation156 reported that primary care physicians in Saudi Arabia had poor knowledge about hydrogenated fat, sources of vitamin BCitation12, substances raising blood high-density lipoprotein cholesterol levels, type of dietary fiber contributing to lowering blood cholesterol, and nutrients associated with prevention of hypertension.
Conclusion
N-NCDs have reached critical levels in most EMR countries, representing more than 50%–60% of total deaths, and creating a health and economic burden on government health services.Citation157 Intervention programs to prevent and control N-NCDs in these countries are lacking. Most of the current programs are focusing on education through mass media, especially television, the press, and booklets.Citation28 There is a need to establish a comprehensive strategy to include all the N-NCDs rather than separate strategies for each disease, which is happening in many EMR countries. It is well documented that the risk factors for these diseases are related to each other, and that each disease may be a risk factor for another N-NCD. In order to combat N-NCDs, we need to focus on practical solutions that can be applied to prevent and control these diseases and make better use of the most reliable research data. Programs used in such a strategy should be long-term and sustainable, and the proposed activities should include all segments of the community. Private sectors as well as governmental sectors should be involved in the preparation and implementation of such programs. Three main components should be promoted in this strategy, ie, healthy eating, physical activity, and a healthy lifestyle, and avoidance of tobacco smoking.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health Organization, Regional Office of East MediterraneanRegional data on noncommunicable diseases risk factors Available from: http://www.emro.who.int.ncdAccessed February 25, 2009
- MirkinBPopulation levels, trends and policies in the Arab region: Challenges and opportunitiesArab Human Development ReportUnited Nations Developing Programme2010 Available from: http://www.arab-hdr.org/publications/other/ahdrps/paper01-en.pdfAccessed January 25, 2012
- WangYLobsteinTWorldwide trends in childhood overweight and obesityInt J Pediatr Obes20061112517902211
- KostiRIPanagiotakosDBThe epidemic of obesity in children and adolescents in the worldCent Eur J Public Health20061415115917243492
- MirmiranPSherafat-KazemzadehRJalali-FarahaniSAziziFChildhood obesity in the Middle East: a reviewEast Mediterr Health J2010161009111721218730
- PapandreouCAbuMou’adTJildehCAbdeenZPhilalithisATzanakisNObesity in Mediterranean region (1997–2007): a systematic reviewObes Rev2008938939918248588
- SibaiAMNasreddineLMokdadAHAdraNTabetMHwallaNNutrition transition and cardiovascular disease risk factors in Middle East and North Africa Countries: reviewing the evidenceAnn Nutr Metab20105719320321088386
- MusaigerAOOverweight and obesity in the Eastern Mediterranean: prevalence and possible causesJ Obes2011201140723721941635
- Al-HazzaaHMPhysical activity, fitness and fatness among Saudi children and adolescents: implications for cardiovascular healthSaudi Med J20022314415011938387
- Al-SendiAMShettyPMusaigerAOMyattMRelationship between body composition and blood pressure in Bahraini adolescentsBr J Nutr20039083784414552329
- Bin-ZaalAAMusaigerAOD’SouzaRThe association between obesity and blood pressure among adolescents in Dubai, UAEPak J Med Sci201026271276
- Al-SabbahHVereeckenCKolsterenPAbdeenZMaesLFood habits and physical activity patterns among Palestinian adolescents: findings from national study of Palestinian school children (HBSC-WBG 2004)Public Health Nutr20071073974617381946
- MusharrafiehUTamimHMRahiACDeterminants of university students physical execises: a study from LebanonInt J Public Health20085320821318716725
- HenryCJKLightowlerHJAl-HouraniHMPhysical activity and levels of inactivity in adolescent females aged 11–16 years in the United Arab EmiratesAm J Hum Biol20041634635315101059
- FazahAJacobCMoussaEEl-HageRYoussefHDelamarchePActivity, inactivity and quality of life among Lebanese adolescentsPediatr Int20105257357820030747
- Bin ZaalAAMusaigerAOD’SouzaRDietary habits associated with obesity among adolescents in Dubai, United Arab EmiratesNutr Hosp20092443744419721923
- SayeghADiniELHoltRDBediRFood and drink consumption, sociodemographic factors and dental caries in 4–5-year-old children in Amman, JordanBr Dent J2002193374212171204
- MusaigerAOBaderZAl-RoomiKD’SouzaRDietary and lifestyle habits among adolescents in BahrainFood Nutr ResSeptember 92011 [Epub ahead of print.]
- Al-ShehriANSalehZASalamaMMHassanYMPrevalence of hyperlipidemia among Saudi school children in RiyadhAnn Saudi Med2004246815310005
- AziziARahmaniMMadjidMAllahverdianAGhanbarianJHajipourRSerum lipid levels in an Iranian population of children and adolescents: Tehran Lipid and Glucose StudyEur J Epidemiol20011728128811680549
- BenamerHTGrossetDStroke in Arab countries: systematic literature reviewJ Neurol Sci200915182319428027
- HosseiniAASobhania-RadDGhandehariKBenamerHTSFrequency and clinical patterns of stroke in Iran – systematic and critical reviewBMC Neurol2010107220731823
- World Health OrganizationGlobal Status Report on Non-Communicable Diseases, 2010Geneva, SwitzerlandWorld Health Organization2011
- El-HazmiMAIWarsyASEvaluation of serum cholesterol and triglyceride levels in 1–6-year-old Saudi childrenJ Trop Pediatr20014718118511419685
- HarrabiIGhannemHGahaRHochlafMLimamKEssoussiASEpidemiology of dyslipidemia among schoolchildren in Sousse, TunisiaDiabetes Metab20053128528916142019
- National Nutrition InstituteDiet, Nutrition and Prevention of Chronic Non-Communicable Diseases among Egyptian AdolescentsCairo, EgyptMinistry of Health2008
- Al MajedHTAlAttarATSadekAAPrevalence of dyslipidemia and obesity among college students in KuwaitAlexandria J Med2011476771
- MusaigerAOHassanASObeidOThe paradox of nutrition-related diseases in the Arab countries: the need for actionInt J Environ Res Public Health201183637367122016708
- BouguerraRAlbertiHSalemLBThe global diabetes pandemic: the Tunisian experiencesEur J Clin Nutr20076116016516900086
- AjlouniKKhaderYSBatiehaAAjlouniHEl-KhateebMAn increase in prevalence of diabetes mellitus in Jordan over 10 yearsJ Diabetes Complications20082231732418413210
- ShawJESicreeRAZimmetPZGlobal estimates of the prevalence of diabetes for 2010 and 2030Diabetes Res Clin Pract20108741419896746
- KhatibONon-communicable diseases. Risk factors and regional strategies for prevention and careEast Mediterr Health J20041077878816335764
- EsteghamatiAMeysamieAKhaizadehOThird national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemiaBMC Public Health2009916717619480675
- World Health Organization, Regional Office for the Eastern MediterraneanTowards a strategy for cancer control in the Eastern Mediterranean regionCairo2009 Available from: www.emro.who.int/dsaf/dsa1002.pdfAccessed January 25, 2012
- El SalimMooreMAAl-LawatiJACancer epidemiology and control in the Arab World – past, present and futureAsian Pac J Cancer Prev20091031619469617
- RavichandranKAl-ZahraniASAssociation of reproductive factors with the incidence of breast cancer in Gulf Corporation Council countriesEast Mediterr Health J20091561262119731777
- BenerAColon cancer in rapidly developing countries: a review of the lifestyle, dietary, consanguinity and hereditary risk factorsOncol Rev20115511
- Al-HamdanNRavichandranKAl-SayyedJIncidence of cancer in Gulf Corporation Council countries, 1998–2001East Mediterr Health J20091560061119731776
- World Health Organization, Regional Office for the Eastern MediterraneanReport on the consultation on establishing regional guidelines on osteoporosisCairo2005 Available from: www.emro.who.int/ncd/pdf/who_em_ncd_044_e_en.pdfAccessed January 25, 2012
- HashemipourSLarijaniBAdibiHVitamin D deficiency and causative factors in the population of TehranBMC Public Health200443815327695
- El-Hajj FuleihanGBaddouraRAwadaHSalamNSalamounMRizkPLow peak bone mineral density in healthy Lebanese subjectsBone20023152052812398950
- BenerARizkDEShaheenHMicallefROsmanNDunnEVMeasurement-specific quality of life satisfaction during menopause in an Arabian Gulf countryClimacteric20003434911910609
- ArdawiMSMaimanyAABahkshTMNasratHAMilaatWAAl-RaddadiRMBone mineral density of the spine and femur in healthy SaudisOsteoporos Int200516435515167986
- El-DessoukiMIOsteoporosis in post menopausal Saudi women using x-ray bone densitometrySaudi Med J20032495395612973476
- MeddebNSahliHChahedMVitamin D deficiency in TunisiaOsteoporos Int20051618018315197539
- AllaliFEl AichaouiSKhazaniHHigh prevalence of hypovitaminosis D in Morocco: relation to lifestyle, physical performance, bone makers, and bone mineral densitySemin Arthritis Rheum200938441451
- DoughertyGAl-MazroukNBone density measured by dual-energy x-ray absorptiometry in healthy Kuwaiti womenCalcif Tissue Int20016822522911353949
- Gannage-YaredMHChemaliRYaacoubNHalabyGHypovitaminosis D in a sunny country: relation to lifestyle and bone markersJ Bone Miner Res2000151856186210977006
- SiddiquiAMKamfarHZPrevalence of vitamin D deficiency rickets in adolescent school girls in Western region, Saudi ArabiaSaudi Med J20072844144417334476
- MaaloufGGannage-YaredMHEzzedineJMiddle East and North Africa consensus on osteoporosisJ Musculoskelet Neuronal Interact2007713114317627082
- Al-HazzaaHMPrevalence and trends in obesity among school boys in Central Saudi Arabia between 1988 and 2005Saudi Med J2007281569157417914521
- EsteghamatiAKhalilzadehOMohammadKSecular trends of obesity in Iran between 1999–2007: national surveys of risk factors of non-communicable diseasesMetab Syndr Relat Disord2010820921320085488
- YusufSHawkenSOunpuuSObesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control studyLancet20053661640164916271645
- LobsteinTBaurLUauyRObesity in children and young people: a crisis in public healthObes Rev20045410415096099
- ThanopoulouAKaramanosBAngelicoFEpidemiological evidence for the non-random clustering of the components of the metabolic syndrome: multicenter study of the Mediterranean Group for the Study of DiabetesEur J Clin Nutr2006601376138316823407
- AL-LawatiJAMohammedAJAl-HinaiHQJousilahtiPPrevalence of the metabolic syndrome among Omani adultsDiabetes Care2003261781178512766109
- Al-RashanIAl-NesefYPrevalence of overweight, obesity, and metabolic syndrome among Kuwaitis: result from community-based national surveyAngiology201061424919398424
- BenerAZirieMMusallamMKhaderYSAl-HamaqAOPrevalence of metabolic syndrome according to Adult International Panell III and International Diabetes Federation Criteria: a population-based studyMetab Syndr Relat Disord2009722123019320557
- SibaiAMObeidOBatalMAfraNElkhouryDHwallaNPrevalence and correlates of metabolic syndrome in an adult Lebanese populationCVD Prev Control200838390
- HarzallahFAlbertiHBen-KhalifaFThe metabolic syndrome in an Arab population. a first look at the next International Diabetes Federation criteriaDiabet Med20062344144416620275
- Abdul-RahimHFHusseiniABjertnessEGicamanRGordonNHJervellJThe metabolic syndrome in the West Bank population, an urban-rural comparisonDiabetes Care20012427527911213878
- DelavariAForouzanfarMHAlikhaniSSharifianAKelishadiRFirst national study of the prevalence of the metabolic syndrome and optimal cutoff points of waist circumference in the Middle East: the national survey of risk factors for noncommunicable diseases of IranDiabetes Care2009321092109719279302
- MalikMAbdel-RazigSThe prevalence of metabolic syndrome among the multiethnic population of the United Arab Emirates: a report of a national surveyMetab Syndr Relat Disord2008617718618699721
- MabryRMReevesMMEakinEGOwenNGender differences in the prevalence of the metabolic syndrome in Gulf Corporation Council countries: a systematic reviewDiabet Med20102759359720536958
- EsmaillzadehAMirmiranPAzedbakhtLEtemadiAAziziFHigh prevalence of the metabolic syndrome in Iranian adolescentsObesity20061437738216648607
- KelishadiRArdalanGGheiratmandRAdeliKDelavariAMajdzadehetRPediatric metabolic syndrome and associated anthropometric indices: CASPIAN studyActa Pediatr20069516251634
- Al-DaghriNMExtremely high prevalence of metabolic syndrome manifestations among Arab youth: a call for early interventionEur J Clin Invest2010401063106620624169
- KelishadiRChildhood overweight, obesity and metabolic syndrome in developing countriesEpidemiol Rev200729627617478440
- KelishadiRGouyaMMAdeliKFactors associated with metabolic syndrome in a national sample of youths: CASPIAN studyNutr Metab Cardiovasc Dis20081846147017935959
- GhassemiHHarrisonGMohammadKAn accelerated nutrition transition in IranPublic Health Nutr2002514915512027278
- GalalOMThe nutrition transition in Egypt: obesity, undernutrition and the food consumption contextPublic Health Nutr2002514114812027277
- BenjellounSNutrition transition in MoroccoPublic Health Nutr2002513514012027276
- MadanatHNTroutmanKPAl-MadiBThe nutrition transition in Jordan: the political, economic and food consumption contextPromot Educ20081561018430689
- SibaiAMNasreddineLMokdadAHAdraNTabetMHwallaNNutrition transition and cardiovascular disease risk factors in Middle East and North Africa Countries: reviewing the evidenceAnn Nutr Metab20105719320321088386
- Food and Agriculture Organization of the United NationsFood Balance Sheet Available from: http://faostat.fao.org/Accessed January 25, 2012
- EsmaillzadehAAzadbakhtLMajor dietary patterns in relation to general obesity and central adiposity among Iranian womenJ Nutr200813835836318203904
- GalalONutrition-related health patterns in the Middle EastAsia Pac J Clin Nutr20031233734314505998
- MusaigerAODiet and prevention of coronary heart disease in the Arab Middle East countriesMed Princ Pract20021191612444306
- KimigarSMGhaffarpourMHoushiar-RedAHomozdyariHZellipourLFood consumption pattern in the Islamic Republic of Iran and its relation to coronary heart diseaseEast Mediterr Health J19984539547
- NasreddineLHwallaNSibaiAHamzeMParent-MassinDFood consumption patterns in an adult urban population in Beirut, LebanonPublic Health Nutr2006919420316571173
- MahmoodAHNutritional status and anthropometric measurements among women in Egypt, National Survey 2001–2002Arab J Food Nutr20041198107
- KelishadiRArdalanGGheiratmandRAssociation of physical activity and dietary behaviours in relation to the body mass index in a national sample of Iranian children and adolescents: CASPIAN studyBull World Health Organ200785192617242754
- MirmiranPAzadbakhtLAziziLDietary quality-adherence to the dietary guidelines in Tehranian adolescents: Tehran Lipid and Glucose StudyInt J Vitam Nutr Res20057519520016028635
- FrenchSAStoryMJefferyRWEnvironmental influences on eating and physical activityAnnu Rev Public Health20012230933511274524
- BashourHNSurvey of dietary habits of in-school adolescents in Damascus, Syria Arab RepublicEast Mediterr Health J20041085386216335773
- HejaziNMazloomZSocioeconomic status, youth’s eating patterns and meal consumed away from homePak J Biol Sci20091273073319634480
- BrayGASoft drinks and obesity: the evidenceCMR J200921014
- HonkalaSHonkalaEAl-SahliNConsumption of sugar products and associated-life and school-satisfaction and self-esteem factors among schoolchildren in KuwaitActa Odontol Scand200664798816546849
- CollisonKSZaidiMZSubhaniSMAl-RubeaanKShoukriMAl-MohannaFASugar sweetened carbonated beverage consumption correlates with waist circumference and poor dietary choices in school childrenBMC Public Health20101023420459689
- NgSWZaghloalSAliHHarrisonGEl-SadigMPopkinBMNutrition transition in the United Arab EmiratesEur J Clin Nutr2011651328133721772317
- IsmailAITanzerJMDingleJLCurrent trends of sugar consumption in developing countriesCommunity Dent Oral Epidemiol1997254384439429817
- HigginsJWhole gain, and the subsequence meal effect: Implications for glucose control and the role of fermentationJ Nutr MetabOctober 302011 [Epub ahead of print.]
- EsmaillzadehAMirmiranPAziziFWhole-grain intake and prevalence of hypertriglyceridemic waist phenotype in Tehranian adultsAm J Clin Nutr200581556315640460
- NasreddineLMehio-SibaiAMrayatiMAdraNHwallaNAdolescent obesity in Syria: prevalence and associated factorsChild Care Health Dev20103640441319961497
- KelishadiRArdalanGGheiratmandRAssociation of physical activity and dietary behaviours in relation to the bodymass index in a national sample of Iranian children and adolescents: CASPIAN StudyBull World Health Organ200785192617242754
- El-GhazaliSIbrahimJMKanariBMIsmailNAThe relationship between lifestyle and body mass index among university students in KuwaitEgyptian J Com Med2010286976
- DastgiriSMahdaviRTuTunchiHFaramarziEPrevalence of obesity, food choices and socio-economic status: a cross-sectional study in the north-west of IranPublic Health Nutr20069996100017125562
- LockKPomerleauJCauserLAltmannDRMcKeeMThe global burden of disease attributable to low consumption of fruit and vegetables: implications for the global strategy on dietBull World Health Organ20058310010815744402
- HungHCJoshipuraKJJiangRFruit and vegetable intake and risk of major chronic diseaseJ Natl Cancer Inst2004961577158415523086
- NessARPowlesJWFruit and vegetables, and cardiovascular disease: a reviewInt J Epidemiol1997261139126498
- Al-RoomiKMusigerAOAl-AwadiHLifestyle and risk of acute myocardial infarction in a Gulf Arab populationInt J Epidemiol1994239319397860173
- MirmiranPNooriNZavarehMBAziziFFruit and vegetable consumption and risk factors for cardiovascular diseaseMetabolism20095846046819303965
- PourfarziFWhelanAKaldorJMalikzadehRThe role of diet and other environmental factors in the causation of gastric cancer in Iran – a population based studyInt J Cancer20091251953196019569234
- KelishadiRPourMHSarraf-ZadeganNSadryObesity and associated modifiable environmental factors in Iranian adolescents: Isfahan Healthy Heart Programme-Heart Health Promotion from ChildhoodPediatr Int20034543544212911481
- RashadHDemographic transition in Arab countries: a new perspectiveJ Popul Res20001783101
- World Health Organization/Regional Off ice for the Eastern MediterraneanActive Aging and Promotion of the Health of the Older PeopleCairo, EgyptRegional Off ice of the Eastern Mediterranean2006
- MisraAKhuranaLObesity and the metabolic syndrome in developing countriesJ Clin Endocrinol Metab200893S9S3018987276
- MonteiroCAMouraECCondeWLPopkinBMSocioeconomic status and obesity in adult populations of developing countries: a reviewBull World Health Organ20048294094615654409
- Aounallah-SkhiriHTraissalPEl-AliJNutrition transition among adolescents of a South-Mediterranean country: dietary patterns association with socio-economic factors, overweight and blood pressure; a cross-sectional study in TunisiaNutr J2011103821513570
- SolimanASKhorshidAIbrahimNDorghamLMcPhersonRSDiet and cooking practices in Egypt: exploration of potential relationship to early-chest colorectal cancerNutr Res199818785797
- JamalHASheihamACowellCRWaltRGTaste preference for sweetness in urban and rural population in IraqJ Dent Res19967618791889
- HakeemRThomasJBadruddinSHFood habits and nutrient density of diet of Pakistani children living in different urban and rural settingsJ Health Popul Nutr20022025526312430763
- WarburtonDERNicolCWBredinSSDHealth benefits of physical activity: the evidenceCMAJ200617480180916534088
- KopiszewstiAArab versus Asian migrant workers in the GCC countries Population Division, United Nations Secretariat2006 Available from: http://www.un.org/esa/population/meetings/EGM_Ittmig_Arab/P02_Kapiszewski.pdfAccessed January 26, 2012
- Al-HazzaaHMThe public health burden of physical inactivity in Saudi ArabiaJ Fam Community Med2004114551
- Al-NozhaMAl-HazzaaHArafahMRPhysical activity and inactivity among Saudi aged 30–70 years: A population-based cross-sectional studySaudi Med J20072855956817457478
- Al-RefaeeSAAl-HazzaaHMPhysical activity profile of Saudi males: implications for healthSaudi Med J20012278478911590453
- Al-HazzaaHMHealth-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ)Public Health Nutr200710596417212844
- World Health OrganizationSTEPwise approach to surveillance (STEPS) Available from: http://www.who.int/chp/steps/en/Accessed September 17, 2011
- GutholdRCowanMJAutenriethCSKannLRileyLMPhysical activity and sedentary behavior among schoolchildren: a 34-country comparisonJ Pediatr20101574349e120304415
- Al-HazzaaHMMusaigerAOPhysical activity patterns and eating habits of adolescents living in major Arab cities: The Arab Teens Lifestyle StudySaudi Med J20103121021120174744
- FarahatTMMechaelAAAbu-SalemMPrevalence of obesity among preschool children in Menofia, EgyptArab J Food Nutr20038107118
- Al-HazzaaHMAl-RasheediAAAdiposity and physical activity levels among preschool children in Jeddah, Saudi ArabiaSaudi Med J20072876677317457449
- LaftaRKKadhimMJChildhood obesity in Iraq: prevalence and possible risk factorsAnn Saudi Med20052538939316270761
- World Health Organization/Regional Off ice for the Eastern MediterraneanReport on the Regional Consultation on Hypertension, Prevention and ControlCairo, EgyptWorld Health Organization/Regional Office for the Eastern Mediterranean2004
- AbdullaAMNagelkerkeNJAbouchacraSPathanJYAdemAObinecheENUnder-treatment and under diagnosis of hypertension: a serious problem in the United Arab EmiratesBMC Cardiovasc Disord200662416753071
- BenerAAl-SuwaidiJAl-JaberKAl-MarriSElbagiIEEpidemiology of hypertension and its associated risk factors in the Qatari populationJ Hum Hypertens20041852953014973519
- Al-SalloumAAEl-MouzanMIAl-HerbishASAl-OmarAAQurashiMMBlood pressure standards for Saudi children and adolescentsAnn Saudi Med20092917317819448364
- SubahiMDBlood pressure profile and hypertension in Iraqi primary school childrenSaudi Med J20062748248616598324
- VillablancaACMcDonaldJMRutledgeJCSmoking and cardiovascular diseaseClin Chest Med20002115917210763097
- National Cancer InstituteHealth effects of exposure to environmental tobacco smoke: a report of the California Environmental Protection AgencySmoking and Tobacco Control Monograph No. 10Bethesda, MDUS Department of Health and Human Service, National Institutes of Health, National Cancer Institute NIH Pub No 99-46451999
- SiziyaSMuulaASRudatsikiraECorrelates of current smoking in-school adolescents in the Kurdistan region of IraqConfl Health20071131918053219
- HarrabiIChahedHMaatougJGahaJEssoussiSGhannemHPredictors of smoking initiation among schoolchildren in Tunisia: a 4 years cohort studyAfr Health Sci2009914715220589142
- El-RoueihebZTamimHKanjMJabbourSAlayanIMusharrafiehUCigarette and waterpipe smoking among Lebanese adolescents, a cross-sectional study, 2003–2004Nicotine Tob Res20081030931418236295
- AminTTAmarMAZazaBOSulemanWHarm perception, attitudes and predicators of waterpipe (shisha) smoking among secondary school adolescent in Al-Hassa, Saudi ArabiaAsian Pac J Cancer Prev20101129330120843104
- KelishadiRMokhtariMRTavasoliAADeterminants of tobacco smoking among youths in Isfahan, IranInt J Public Health20075217317917958284
- AlmerieMQMatarHESalamMCigarettes of waterpipe smoking among medical students in Syria: a cross-sectional studyInt J Tuberc Lung Dis2008121085109118713509
- WaliSOSmoking habits among medical students in Western Saudi ArabiaSaudi Med J20113284344821858395
- BehbehaniNNHamadehRRMacklaiNSKnowledge of and attitudes towards tobacco control among smoking and non-smoking physicians in 2 Gulf Arab statesSaudi Med J20042558559115138525
- AklEAGunukulaSKAleenSObeidRAbou-JaoudePHoneineRThe prevalence of waterpipe tobacco smoking among the general and specific population: a systematic reviewBMC Public Health20111124425521504559
- Moh’d Al-MullaAAbdou HelmySAl-LawatiJPrevalence of tobacco use among students aged 13–15 years in Health Ministers’ Council/Gulf Corporation Council Member Status, 2001–2004J Sch Health20087833734318489467
- ChaayaMEl-RoueihebZChemaitellyHAzarGNasrJAl-SahabBArgileh smoking among university students: a new tobacco epidemicNicotine Tob Res2004645746315203779
- Al-TurkiYASmoking habits among medical students in Central Saudi ArabiaSaudi Med J20062770070316680263
- MandilAHusseinAOmerHCharacteristics and risk factors of tobacco consumption among University of Sharjah students, 2005East Mediterr Health J2007131449145818341194
- MaziakWEissenbergTRastamSBeliefs and attitudes related to narghile (waterpipe) smoking among university students in SyriaAnn Epidemiol20041464665415380795
- MaziakWFouadFMAsfarTPrevalence and characteristics of narghile smoking among university students in SyriaInt J Tuber Lung Dis20048882889
- AliVVMZabaidMAl-MotarrebAAssociation of khat chewing with increased risk of stroke and death in patients presenting with acute coronary syndromeMayo Clin Proc20108597498020926835
- United Nations Children’s FundThe State of World’s Children2008Child SurvivalNew York, NYUnited Nations Children’s Fund2007
- El TaguriABesmarFAbdel MonemABetilmalIRicourCRolland-CacheraMFStunting is a major risk factor for overweight: results from national surveys in 5 Arab countriesEast Mediterr Health J20091554956219731771
- KamranSBenerABDeleuDThe level of awareness of stroke risk factors and symptoms in the Gulf Cooperation Council Countries: Gulf Cooperation Council Stroke Awareness StudyNeuroepidemiology20092923524218176080
- MusaigerAOAl-MaskariAAlawatiHFactors associated with the risk of osteoporosis among adults in BahrainArab J Food Nutr2008194962
- MusaigerAOShahbeekNEThe effect of education and obesity on attitudes toward fads related to weight reduction among Arab women in QatarJ Nutr Food Sci200131201204
- MusaigerAOMatterAMAlekriSAMahdiAEKnowledge and attitudes of Bahraini adolescents toward obesityJ Consumer Studies Home Economics199115321325
- MusaigerAOKnowledge and attitudes of university female students towards obesityInt Q Community Health Educ19931433734420841234
- HosseiniSNayebiNAmirkalaliBSeyedkhoeiNHeshmatRAre physicians good candidates for recommending dietIran J Public Health2008374853
- Al-NumairKNutrition knowledge of primary health care physicians in Saudi ArabiaPak J Nutr20043344347
- HabibSSahaSBurden of non-communicable disease: global overview. Diabetes and Metabolic SyndClinical Research and Reviews200844147
- de OnisMBlossnerMPrevalence and trends of overweight among preschool children in developing countriesAm J Clin Nutr2000721032103911010948
- Al-RaeesGYAl-AmerMShehabMNutritional Status of Bahraini Children Aged 2–6 Years oldJuffair, Kingdom of BahrainMinistry of Health2003
- Administration of Food and NutritionKuwait Nutritional Surveillance SystemMurgab, KuwaitMinistry of Health2005
- AlasfoorDMohammedAJImplications of the use of the new WHO growth charts on the interpretation of malnutrition and obesity in infants and young children in OmanEast Mediterr Health J20091589089820187540
- KamalAABenerAKareem Al-MullaAMGrowth pattern of Qatari preschool childrenCroat Med J20044546146515311420
- Food and Agriculture Organization of the United NationsNutrition Country Profile – SudanRome, ItalyFood and Nutrition Division, Food and Agriculture Organization of the United Nations2005
- United Nations Environment Programme, United Nations Children’s FundMICS 111 Survey in 2006TunisiaNational Office of Population and Family, Ministry of Public Health2007
- BaderZMusaigerAOAl-RoomiKD’SouzaROverweight and obesity among adolescents in BahrainAnthropol Anz20086640140819216180
- National Nutrition InstituteDiet, Nutrition and Prevention of Chronic Non-Communicable Diseases among Egyptian AdolescentsCairo, EgyptMinistry of Health2008
- KelishadiRArdalanGGheiratmandRThinness, overweight and obesity in a national sample of Iranian children and adolescents: CASPIAN StudyChild Care Health Dev200834445418171443
- El-BayoumyIShadyILotfyHPrevalence of obesity among adolescents (10 to 14 years) in KuwaitAsia Pac J Public Health20092115315919190003
- SibaiAMHwallaNAdraNRahalBPrevalence and covariates of obesity in Lebanon: findings from the first epidemiological studyObes Res2003111353136114627756
- BenerAKamalAAGrowth patterns of Qatari school children and adolescent aged 6–18 yearsJ Health Popul Nutr20052325025816262022
- El MouzanMIFosterPJAl HerbishASPrevalence of overweight and obesity in Saudi children and adolescentsAnn Saudi Med20103020320820427936
- Aounallah-SkhiriHRomdhaneHBTraissacPNutritional status of Tunisian adolescents: associated gender, environmental and socio-economic factorsPublic Health Nutr2008111306131718561866
- United Arab Emirates Global School-based Student SurveyAbu Dhabi, United Arab Emirates2005 Available from: http://www.who.int/chp/gshs/2005_United_Arab_Emirates_GSHS_Country_Report.pdfAccessed January 26, 2012
- Ministry of HealthNational Non-Communicable Diseases Risk Factor Survey, 2007Juffair, Kingdom of BahrainMinistry of Health2010
- JanghorbaniMAminiMWillettWCFirst nationwide survey of prevalence of overweight, underweight, and abdominal obesity in Iranian adultsObesity2007152797280818070771
- Ministry of HealthRisk Factors for Non-Communicable Diseases in KuwaitMurgab, KuwaitMinistry of Health2007
- Food and Agriculture Organization of the United NationsNutrition Country Profile – Libyan Arab JamahiriyaFood and Nutrition Division2005 Available from: ftp://ftp.fao.org/es/esn/nutrition/ncp/lby.pdfAccessed January 26, 2012
- MokhtarNElatiJChabirRDiet culture and obesity in northern AfricaJ Nutr2001131887S892S11238780
- Ministry of HealthNational Health Survey 2000, Study of Lifestyle Risk FactorsSultanate of OmanMinistry of Health2000
- Ministry of HealthCountry-Specific Standard ReportRiyadh, Saudi ArabiaMinistry of Health2010
- El-AtiJTraissacPChirazBChange in nutritional status of adult women in Tunisia from 1996 to 2005: effect of living environment and socio-economic factorsInt J Obes200832Suppl 1S215
- Food and Agriculture Organization of the United NationsNutrition Country Profile – PalestineRome, ItalyFood and Nutrition Division, Food and Agriculture Organization of the United Nations2005