Abstract
Aim:
To analyze the influence of the duration of habitual physical activity (PA) on the symptoms of climacterium/menopause and on several domains of the health-related quality of life (QOL) in middle-aged women.
Methods:
One hundred and four 45- to 59-year-old women were placed into three groups: group A, subjects who maintained PA less than 30 minutes/day; group B, subjects who maintained or began to perform PA 30–60 minutes/day; and group C, subjects who maintained or increased PA to more than 60 minutes/day. Symptoms of menopause, QOL (physical, psychological, and social), and PA were assessed through the Kupperman Menopausal Index, World Health Organization Quality of Life Brief Version questionnaire, and International Physical Activity Questionnaire, respectively.
Results:
The analysis of covariance (ANCOVA) results, adjusted for age, initial body mass index, schooling years, hormonal replacement therapy, and the number of diseases, indicated that the women who maintained or increased their total habitual PA to more than 60 minutes/day had reduced symptoms of climacterium/menopause (–5.4 ± 0.5; P = 0.001) and improved QOL in the psychological (4.4% ± 0.8%; P = 0.001) and social domains (2.0% ± 0.9%; P = 0.035). ANCOVA revealed a further improvement of approximately 5% in the psychological domain of QOL in group C, who also experienced decreased menopause symptoms (P = 0.001) and lost weight (P = 0.009).
Conclusion:
The habitual practice of at least moderate-intensity PA for 60 minutes/day has a favorable effect on climacterium/menopause symptoms and on QOL, particularly on its psychological and social domains. The influence of habitual PA at the psychological level seems to be at least partially associated with a decrease in menopause symptoms and/or weight loss.
Introduction
Menopause is a biological event rising from ovary failure, for which a diagnosis is retrospectively made after 12 consecutive months of amenorrhea that is not explainable through pathological causes and is associated with plasma values of follicle-stimulating hormone higher than 40 IU/L.Citation1 It is preceded by a transitory shift from the reproductive to the nonreproductive stage, which lasts approximately 2–8 years in 95% of women.Citation2 This transitory phase is usually characterized by specific vasomotor, psychological, and urogenital signs and symptoms, as well as more generalized physical complaints, such as weight gain, changes in the thickness of the skin and hair, and the appearance of fatigue, vertigo, and joint pain.Citation3,Citation4 The intensity of menopause-related complaints ranges from mild to severe in 96% of the women, affecting their quality of life (QOL) not only from the physical and psychological point of view but also at the social level. The QOL scores of middle-aged women are usually lower than those of middle-aged men, young adults, and elderly women.Citation5–Citation7
Despite the general observation of a negative association between menopause and/or the symptoms of menopause and QOL scores,Citation6,Citation8,Citation9 especially at the psychological level,Citation10 some researchers have investigated the influence of lifestyle and, more specifically, physical activity (PA) on menopause symptoms and/or QOL scores in middle-aged women, independent of their menopausal stage.Citation11,Citation12 High levels of PA have been associated with a better QOL, mainly in the physical domain,Citation13 as well as with a decrease in psychologicalCitation14,Citation15 and physicalCitation11 menopause-related complaints. Conversely, low levels of PA seem to correlate with weight gain and obesity during menopause.Citation16
Evidence for the influence of PA on the symptoms of climacterium/menopause and on QOL rises from intervention studies which apply exercise (targeted PA).Citation17–Citation19 Exercise programs with a fundamentally aerobic component, of moderate or higher intensity, an approximate duration of 30 minutes per session, three or four sessions per week, and lasting at least 6 months, have shown positive effects on QOL.Citation18,Citation19 Other studies on the influence of habitual PA (nontargeted PA) performed in different contexts (leisure, household chores, occupation, and transportation) have not yet quantified the exact level of PA necessary to achieve favorable effects on QOL or on the menopause symptoms in middle-aged women;Citation13,Citation14,Citation20 these data would be highly relevant for establishing recommendations regarding habitual PA in the promotion of health. However, these studies indicate a decrease in the overall frequency of symptoms,Citation14 especially psychological symptoms,Citation14,Citation20 in addition to an increase in QOL, mainly in the physical domain.Citation13 Thus, the main aim of this study was to analyze the influence of the duration of habitual PA on the symptoms of climacterium/menopause and on the various domains of health-related QOL scores in middle-aged women.
Materials and methods
Study participants
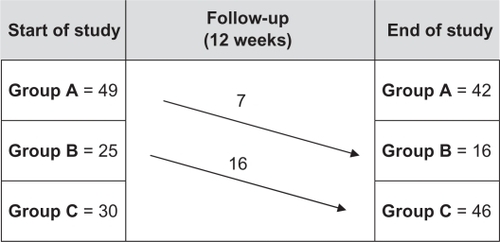
One hundred and twenty 45- to 59-year-old women voluntarily entered the study; participants were recruited through work or institutions associated with educational, health, sport, religious, or insurance services. The study excluded participants who had serious reproductive or hormonal illnesses such as breast, ovarian or endometrial cancer, diabetes, liver disease, current use of psychotropic drugs, or any clinical condition that prevented women from adhering to the PA recommendations for public health – that is the accumulation of at least 30 minutes activity of moderate or greater intensity per day. Only 104 women completed the full 12 weeks of the study. Participants were divided into three groups at the end of the study according to the characteristics of the habitual PA they performed during the period of observation. Group A maintained habitual PA to less than 30 minutes/day (n = 42); group B continued or began to engage in habitual PA for 30–60 minutes/day (n = 16, of which ∼56% maintained the same level of initial habitual PA); and group C continued or began to engage in habitual PA for more than 60 minutes/day (n = 46, of which ∼65% maintained the same level of the initial PA) (). At the beginning of the study, all participants were informed of the health benefits of PA and were advised to be more active in tasks of daily living and to accumulate at least 30 minutes/day PA of moderate or greater intensity (great if ≥60 minutes/day), eg, using stairs instead of elevators or escalators, moving by foot, bicycle, or public transport instead of using the car, and doing active breaks or leisure activities rather than passive activities. Contact was maintained with participants by telephone once a week to encourage them to maintain or increase habitual PA. Three sessions per week of walking was organized during the 12 weeks in one place (park) for participants who wished to do this activity together, but without supervision. It was explained that moderate-intensity physical exertion corresponded to five or six points on a 0–10 scale, where zero represents the absence of exertion and 10 represents maximum exertion.Citation21 A five or six on a 0–10 scale is essentially 45% to 64% of aerobic capacity reserve for moderate intensity. Similarly, a seven or eight on a 0–10 scale means 65% to 84% of reserve is the range for relatively vigorous-intensity activity.
Figure 1 Flow of participants through study.
Data were collected at the beginning and at the end of the study period by the same evaluator. At the beginning of the study, the participants were informed of the aims and procedures of the study and signed an informed consent form according to resolution 196/96 of Conselho Nacional de Saúde, Brazil. This observational study was carried out between September and December 2010, after approval from the Research Ethics Committee of the State University of Santa Catarina, Brazil.
Procedures
PA
Habitual PA was assessed through the short form of the International PA Questionnaire (IPAQ), which was developed by researchers from several countries and has been used by the World Health Organization (WHO) within a multicentric study embracing several countries. This questionnaire was validated by the Studies Center of the Laboratory of Physical Aptitude of São Caetano do Sul, which is an IPAQ coordination center in Brazil.Citation22 The evaluation of habitual PA through IPAQ quantified the number of times each participant walked for at least 10 consecutive minutes (3.3 metabolic equivalents [METs]) and engaged in moderate- (4.0 METs) and vigorous-intensity PA (8.0 METs) during the previous week in various settings: leisure, household chores, occupation, and transportation. Because walking is assigned a level of exertion of 3.3 METs, which is higher than the lower limit for moderate activity (3 METs), the total PA resulting from adding walking, moderate activity, and strong activity corresponds to at least moderate-intensity activity.
Reproductive state (perimenopause vs postmenopause)
The reproductive state of the participants was evaluated through a questionnaire that included age of menarche, regularity of menstrual cycles, and nature of menopause (ie, natural or surgical). Participants who reported 1–11 months of amenorrhea were rated as perimenopausal (45.2% of the women), and those with 12 or more months of amenorrhea were rated as postmenopausal (54.8% of the women).Citation23 The age of menopause was calculated only for the women with natural menopause (79% of the women; 21% reported surgical menopause). The use of hormonal replacement therapy (19.2% of the women) was also included in the questionnaire.
Symptoms of menopause
The symptoms of menopause were assessed through the Kupperman Menopausal Index, comprising ten symptoms or complaints (vasomotor symptoms, insomnia, paresthesia, nervousness, vertigo, weakness, joint/muscular pain, headache, palpitations, and tinnitus). An addition of six menopause symptoms was included: decreased memory, decreased sexuality (libido, sexual activity, and satisfaction), urinary complaints (exertion-induced urinary incontinence or difficult micturition), vaginal dryness (feeling of dryness and difficulties with sexual intercourse), anxiety, and weight gain.Citation24
The occurrence/frequency of each symptom was assessed on a four-point Likert scale, in which 0 = absence, 1 = mild (occasionally), 2 = moderate (repeatedly), and 3 = intense (constantly). After adding the scores for all of the symptoms, participants were classified either as asymptomatic or as having mild (up to 19 points), moderate (20 to 35 points), or intense (higher than 35 points) symptoms.Citation25,Citation26 This questionnaire was previously validated in Brazil.Citation26
QOL
The QOL was assessed by means of the WHO QOL Brief Version (WHOQOL-BREF) questionnaire, which has been validated for Brazilian Portuguese.Citation27 This questionnaire comprises 26 questions (out of the original 100), 24 questions examining physical (physical pain, energy, locomotion, everyday life activities, medical treatments, and work), psychological (positive feelings, concentration, self-esteem, self-image, negative feelings, and spirituality), social (personal relationships, social support, and sexual activity), and environmental (physical safety, housing, financial resources, health-care facilities, information, leisure, physical environment, and transportation) domains and the remaining two are general questions on QOL.
The questions refer to the previous 2 weeks, and the participants answer them according to a Likert scale for intensity (none/extremely), ability (none/completely), frequency (never/always), or evaluation (very unsatisfied/very satisfied; very bad/very good), in which values are calculated from scores ranging from zero (very bad) to 25 (fair), 50 (good), 75 (very good), and 100% (excellent).
Body composition, health status, and educational level
Body weight and height were reported by the participants themselves. Such values were used to calculate body mass index (weight [kg]/height [m]2). Years of schooling and the number of diseases were calculated from a self-reported questionnaire.
Analysis of data
Data were analyzed using SPSS software (v 16.0; SPSS Inc, Chicago, IL). Descriptive statistics were applied (mean, standard deviation, and amplitude) to characterize the age, age of menarche, age of menopause, body mass index, education, number of diseases, habitual PA variables, QOL domain scores, and symptoms of menopause. Comparisons of the QOL scores and symptoms of menopause in middle-aged women between groups (A vs B vs C) after 12 weeks were performed using analysis of covariance (ANCOVA), adjusted for the baseline values of each dependent variable. The levels of significance were determined through Bonferroni post hoc analyses. Intragroup comparisons between the QOL scores and symptoms of menopause at the beginning and end of the study were made through paired t-tests (in groups A and C) and Wilcoxon signed-rank test (group B). The dose-response relationships between habitual PA and the variations in QOL scores in the physical, psychological, and social domains, the variations in weight, and the variation in the symptoms of menopause were analyzed through ANCOVA adjusted for age, initial body mass index, years of schooling, hormonal replacement therapy, and number of diseases. Significant differences in ANCOVA were tested through simple contrast. The level of statistical significance was established at P < 0.05.
Results
describes the mean characteristics of the participants who were chronologically 50 years of age (45–59 years), age of menarche at 13 years, and age of menopause at 49 years (excluding surgical menopause). Participants had attended school for an average of 11 years, which corresponds to secondary education. Most of the women had a body mass index between 18.5–24.9 kg/m2 (average 21 kg/m2). Most of the participants (56%) did not report any disease. The clinical conditions most often reported were migraine (12%), osteoporosis (11%), high total cholesterol (10%), hypertension (9%), and asthma (2%), with no differences between groups. The duration of total daily habitual PA ranged from 0–200 minutes. The average was 24 minutes/day of moderate- to high-intensity activity (excluding walking) and 23 minutes/day of walking. The best score in the QOL assessment was observed in the social domain (65%), although it also exhibited the widest variation (0%–100%), followed by the psychological (60%) and the physical (57%) domains; the latter exhibited the lowest variation (21%–78%).
Table 1 Characteristics of the study participants (n = 104)
Only 11% of participants did not report any symptoms of menopause. Among those who did report symptoms, 41% rated them as moderate in intensity ().
Table 2 Characteristics of the sample according to the symptoms of menopause (n = 104)
and describe the initial and final scores of QOL and of the symptoms of menopause, set into the three groups according to the amount of habitual PA practiced during the 12 weeks of the study. ANCOVA adjusted for baseline values indicated that the participants who engaged in habitual PA for more than 60 minutes/day had improved physical domain QOL scores compared with participants who engaged in habitual PA for less than 30 minutes/day. The most active participants also showed increased QOL scores in the psychological and social domains and a decrease in almost all of the symptoms of menopause compared with the participants who engaged in habitual PA for 60 minutes/day or less.
Table 3 Comparison of quality of life scores among middle-aged women who maintained their total habitual physical activity less than 30 minutes/day (group A), continued or began to engage in physical activity 30–60 minutes/day (group B), or continued or began to engage in physical activity for more than 60 minutes/day (group C), as assessed retrospectively after 12 weeks
Table 4 Comparison of menopause symptoms among middle-aged women who maintained their total habitual physical activity less than 30 minutes/day (group A), continued or began to engage in physical activity 30–60 minutes/day (group B), or continued or began to engage in physical activity for more than 60 minutes/day (group C), as assessed retrospectively after 12 weeks
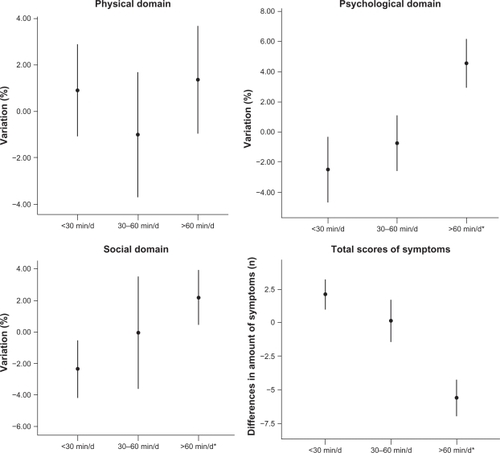
presents the variations in the QOL scores and in the symptoms of menopause according to total habitual PA adjusted for age, initial body mass index, years of schooling, hormonal replacement therapy, and number of diseases. Improvements in the psychological and social domains and in the symptoms of menopause were observed in women who engaged in habitual PA for more than 60 minutes/day.
Figure 2 Average variation in quality of life and symptoms of menopause according to the habitual practice of total physical activity (<30 minutes/day; between 30 and 60 minutes/day; >60 minutes/day) over 12 weeks. Dose-response relationship between the amount of physical activity and variations in the quality of life in the physical, psychological, and social domains and the variation in the symptoms of menopause evaluated by analysis of covariance (ANCOVA) adjusted for age, baseline body mass index, years of schooling, hormonal replacement therapy, and number of diseases, with 95% confidence intervals (physical domain P = 0.062; psychological domain P = 0.001; social domain P = 0.035; and total score of symptoms P = 0.001). Significant differences in ANCOVA tested through simple contrast.
Abbreviation: min/d, minutes per day.
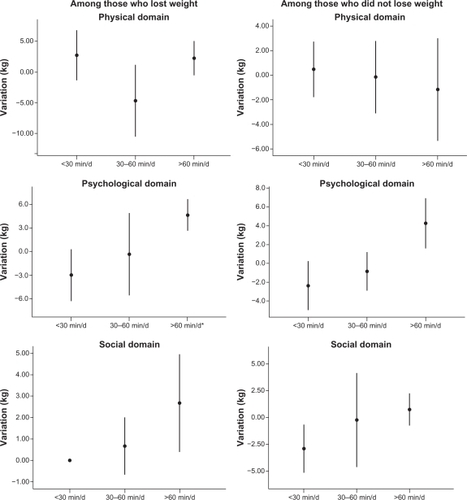
The effects of reducing menopause symptoms and body weight on the QOL scores in each habitual PA group are shown in and . The results indicate improvement in the psychological domain in participants who engaged in habitual PA for more than 60 minutes/day and had a decrease in menopause symptoms or in body weight.
Figure 3 Average variation in the quality of life according to habitual practice of total physical activity (<30 minutes/day; between 30 and 60 minutes/day; >60 minutes/day) over 12 weeks, analyzed separately for two groups of participants: (A) those who had a decrease in menopause symptoms and (B) those whose symptoms remained constant or increased. Dose-response relationship between the amount of physical activity and variations in the quality of life in the physical, psychological, and social domains and the variation in the symptoms of menopause evaluated by analysis of covariance (ANCOVA) adjusted for age, baseline body mass index, years of schooling, hormonal replacement therapy, and number of diseases, with 95% confidence intervals. Among the women with decreased symptoms: physical domain P = 0.623; psychological domain P = 0.001; and social domain P = 0.073. Among the women without decreased symptoms: physical domain P = 0.545; psychological domain P = 0.761; and social domain P = 0.584. Significant differences in ANCOVA tested through simple contrast.
Abbreviation: min/d, minutes per day.
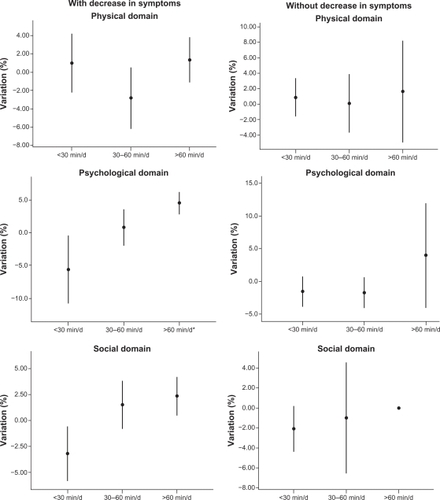
Figure 4 Average variation in quality of life according to habitual practice of total physical activity (<30 minutes/day; between 30 and 60 minutes/day; >60 minutes/day) over 12 weeks, analyzed separately for two groups of participants: (A) those who lost weight and (B) those who maintained or gained weight. Dose-response relationships between the amount of physical activity and variations in the quality of life in the physical, psychological, and social domains and variations in the symptoms of menopause evaluated by analysis of covariance (ANCOVA) adjusted for age, baseline body mass index, years of schooling, hormonal replacement therapy, and number of diseases, with 95% confidence intervals. Among those who lost weight: physical domain P = 0.698 and psychological domain P = 0.009; (B) <30 minutes/day = −3 ± 1; 30–60 minutes/day = 0.7 ± 2; >60 minutes/day = 0.1 ± 2; P = 0.082; social domain P = 0.051. Among those who did not lose weight: physical domain P = 0.960; psychological domain P = 0.082; and social domain P = 0.212. Significant differences in ANCOVA tested through simple contrast.
Abbreviation: min/d, minutes per day.
Discussion
The main aim of this study was to analyze the influence of the duration of habitual PA on the symptoms of climacterium/menopause and on different domains of health-related QOL in middle-aged women. The results indicate a positive dose-response relationship between the amount of total habitual PA assessed through IPAC (ie, the addition of walking, and moderate or vigorous activity lasting at least 10 minutes per session) and improvement in the symptoms of menopause and in QOL scores. At the end of 12 weeks, there were improvements in the psychological (approximately 5%) and social (approximately 2.5%) domains of QOL in middle-aged women who engaged in PA for at least 60 minutes/day. Engaging in habitual PA for at least 60 minutes/day showed more favorable effects on the psychological QOL (as well as a positive trend in the social domain, as the levels of significance were borderline) of the women who lost weight and/or had eased symptoms of menopause.
Weight loss in overweight women has been associated with a better QOL,Citation28,Citation29 and weight gain has been associated with both a worse QOLCitation30–Citation33 and an increase in menopause-related physical complaints (vertigo, joint pain, abdominal pain, fatigue, and alterations of the skin), particularly when weight gain is over 5 kg.Citation32 In this study, the average weight loss associated with improvement in the psychological domain scores of middle-aged women who engaged in habitual PA for more than 60 minutes/day was close to 5% (approximately 3 kg). This level of habitual PA is usually recommended to lose weight or to prevent weight gain.Citation34
Other studies conducted with shorter durations/amounts of PA/exercise (30 minutes/day) but over a longer period of time (6 months) also indicated positive effects on QOL; these effects were mainly in the psychological domainCitation18,Citation19 but were also observed in the physical domain.Citation12,Citation18,Citation19 The physical domain, as assessed by WHOQOL-BREF, includes physical pain, energy, locomotion, performance of everyday activities, medical treatments, and work. In this study, no influence of duration or intensity of habitual PA on physical domain scores was observed. Approximately 41% of women report/exhibit a moderate frequency of physical complaints that can cause limitations or reductions in their physical health.Citation8 However, the decrease in symptoms of the women who engaged in moderate- or high-intensity habitual PA for at least 60 minutes/day in this study did not favorably influence their physical domain scores.
Overall, almost all of the symptoms of menopause decreased in the women who engaged in habitual PA for 60 minutes/day or more. This result agrees with previous findings that PA contributes to a decreased occurrence of several symptoms of menopause.Citation11,Citation35,Citation36 However, these results also indicate that engaging in at least moderate-intensity habitual PA for 30 minutes/day in sessions of 10 or more successive minutes can be insufficient for the purposes of promoting QOL and decreasing the frequency of menopause symptoms in middle-aged women.Citation37
This was not a randomized controlled trial. At baseline, it was not possible to recruit a significant number of women with insufficient habitual PA (accumulation <30 minutes/day activity of moderate or greater intensity) and consequently habitual PA of participants was not similar. On the other hand, about 85% of participants who were not sufficiently active at the start remained insufficiently active during the study. Since typically less active people are generally those who benefit most from habitual PA, it is likely that the size of the effects on symptoms and QOL could have been larger if a greater number of insufficiently active women had increased their habitual PA.
Conclusion
The habitual practice of at least moderate-intensity PA for 60 minutes/day has a favorable influence on the prevention of symptoms of climacterium/menopause and on QOL, particularly in the psychological and social domains in middle-aged women. The influence of habitual PA at the psychological level seems partially associated with a decrease in the symptoms of menopause and/or with weight loss.
Disclosure
The authors report no conflicts of interest in this work.
References
- Board of the International Menopause SocietyPinesASturdeeDWBirkhäuserMHIMS updated recommendations on postmenopausal hormone therapyClimacteric200710318119417487645
- SperoffLFritzMAClinical gynecologic endocrinology and infertility7th edPhiladelphia, PALippincott Williams and Wilkins2005
- PerezKSGarberCEExercise prescription for the menopausal years: promoting and enhancing well-beingACSMS Health Fit J2011153814
- DaleyAMacArthurCMcManausRFactors associated with the use of complementary medicine and non-pharmacological interventions in symptomatic menopausal womenClimateric200695336346
- FeldmanDEDucharmeAGiannettiNSeverity at entry to specialized heart failure clinics: discrepancies between health-related quality of life and function in men and womenCan J Cardiol201127338238721514784
- WaidyasekeraHWijewardenaKLindmarkGNaessenTMenopausal symptoms and quality of life during the menopausal transition in Sri Lankan womenMenopause200916116417018703984
- NappiRELachowskyMMenopause and sexuality: prevalence of symptoms and impact on quality of lifeMaturitas200963213814119464129
- MatthewsKABrombergerJTDoes the menopausal transition affect health-related quality of life?Am J Med2005118Suppl 12B253616414324
- AvisNEColvinABrombergerJTChange in health-related quality of life over the menopausal transition in a multiethnic cohort of middle-aged women: Study of Women’s Health Across the Nation (SWAN)Menopause200916586086919436224
- UtianWHPsychosocial and socioeconomic burden of vasomotor symptoms in menopause: a comprehensive reviewHealth Qual Life Outcomes200534716083502
- MoilanenJAaltoAMHemminkiEAroARRaitanenJLuotoRPrevalence of menopause symptoms and their association with lifestyle among Finnish middle-aged womenMaturitas201067436837420869181
- FreemanEWSammelMDLinHSymptoms associated with menopausal transition and reproductive hormones in midlife womenObstet Gynecol20071102 Pt 123024017666595
- Wendel-VosGCSchuitAJTijhuisMAKromhoutDLeisure time physical activity and health-related quality of life: cross-sectional and longitudinal associationsQual Life Res200413366767715130029
- NelsonDBSammelMDFreemanEWLinHGraciaCRSchmitzKHEffect of physical activity on menopausal symptoms among urban womenMed Sci Sports Exerc2008401505818091021
- ElavskySMcauleyEPhysical activity, symptoms, esteem, and life satisfaction during menopauseMaturitas2005523–437438516198515
- LovejoyJCChampagneCMde JongeLXieHSmithSRIncreased visceral fat and decreased energy expenditure during the menopausal transitionInt J Obes (Lond)200832694995818332882
- MirzaiinjmabadiKMAndersonDBarnesMThe relationship between exercise, body mass index and menopausal symptoms in midlife Australian womenInt J Nurs Pract2006121283416403194
- MartinCKChurchTSThompsonAMEarnestCPBlairSNExercise dose and quality of life: results of a randomized controlled trialArch Intern Med2009169326927819204218
- AgilAAbikeFDaskapanAAlacaRTüzünAShort-term exercise approaches on menopausal symptoms, psychological health, and quality of life in postmenopausal womenObstet Gynecol Int2010 [Epub ahead of print.]10.1155/2010/274261
- WolinKYGlynnRJColditzGALeeIMKawachiILong-term physical activity patterns and health-related quality of life in US womenAm J Prev Med200732649049917533064
- NelsonMERejeskiWJBlairSNPhysical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart AssociationMed Sci Sports Exerc20073981435144517762378
- PardiniRMatsudoSMatsudoVValidation of the international physical activity questionnaire (IPAQ): pilot study in Brazilian young adultsMed Sci Sports Exerc1997296S5S9
- BurgerHGThe menopausal transitionBaillieres Clin Obstet Gynaecol19961033473598931899
- FreemanEWSammelMDLiuLMartinPPsychometric properties of a menopausal symptom listMenopause200310325826512792299
- KuppermanHSBlattMHGWiesbaderHFillerWComparative clinical evaluation of estrogenic preparations by the menopausal and amenorrheal indicesJ Clin Endocrinol Metab195313668870313061588
- De SousaRLSousaESSSilvaJCBFilizolaRGTest-retest reliability in application of the Blatt and Kupperman menopausal indexRev Bras Ginecol Obstet2000228481487 Portuguese.
- FleckMPALouzadaSXavierMApplication of the Portuguese version of the abbreviated instrument of quality life WHOQOL-brefRev Saúde Pública2000342178183 Portuguese.
- FineJTColditzGACoakleyEHA prospective study of weight change and health-related quality of life in womenJAMA1999282222136214210591335
- FontaineKRBarofskyIAndersenREImpact of weight loss on health-related quality of lifeQual Life Res19998327527710472159
- DaleyAMacArthurCStokes-LampardHMcManusRWilsonSMutrieNExercise participation, body mass index, and health-related quality of life in women of menopausal ageBr J Gen Pract20075753513013517266830
- GoldEBSternfeldBKelseyJLRelation of demographic and lifestyle factors to symptoms in a multiracial/ethnic population of women 40–55 years of ageAm J Epidemiol2000152546347310981461
- LiCBorgfeldtCSamsioeGLidfeldtJNerbrandCBackground factors influencing somatic and psychological symptoms in middle-age women with different hormonal status. A population-based study of Swedish womenMaturitas2005523–430631815967603
- GallicchioLVisvanathanKMillerSRBody mass, estrogen levels, and hot flashes in midlife womenAm J Obstet Gynecol200519341353136016202725
- United States Department of Health and Human ServicesDietary guidelines for Americans, 20051112005 Available from: http://www.health.gov/dietaryguidelines/dga2005/document/default.htm. Accessed July 10, 2011.
- MoriyamaCKOnedaBBernardoFRA randomized, placebo-controlled trial of the effects of physical exercises and estrogen therapy on health-related quality of life in postmenopausal womenMenopause2008154 Pt 161361818551087
- DaleyAJStokes-LampardHJMacArthurCExercise to reduce vaso-motor and other menopausal symptoms: a reviewMaturitas200963317618019285813
- GuimarãesACABaptistaFRelationship between physical activity and menopausal symptomsJ Phys Act Health2011In press.