Abstract
A surprising result of the groundbreaking CAPRISA-004 trial, which demonstrated the efficacy of vaginal tenofovir 1% gel in reducing the risk of human immunodeficiency virus (HIV)-1 infection by 39% in heterosexual women, was the added benefit of this microbicide in reducing acquisition of herpes simplex virus type 2 (HSV-2) by 51%. HSV-2 is the most common cause of genital ulcer disease worldwide, and is responsible for considerable morbidity among women and neonates. The virus is further implicated in increasing the risk of both HIV acquisition and transmission, and may have additional adverse consequences in HIV-coinfected persons, making HSV-2 prevention an important clinical and public health objective. While tenofovir had not previously been widely considered to be an anti-herpes drug, in vitro activity against HSV is well documented, raising interest in potential future applications of tenofovir and its prodrugs in HSV-2 control. This article reviews the currently available data for tenofovir as an anti-herpes agent, as well as unanswered questions about delivery systems, drug formulation, rectal administration, drug resistance, and clinical applications.
Introduction
Herpes simplex virus type 2 (HSV-2) is the most common cause of genital ulcer disease worldwide, with an estimated seroprevalence of 20%–80% in different settings around the world and a greater burden of infection in women than in men due to increased susceptibility.Citation1,Citation2 Upon contact with nonintact skin or mucosal surfaces, the virus classically causes recurrent vesicular or pustular ulcerative lesions that may be accompanied by painful, itching, and burning sensations, as well as tender lymphadenopathy.Citation3 HSV-2 is associated with morbidity, social stigma, and increased transmission of human immunodeficiency virus type 1 (herein referred to as HIV) infection, rendering the potential prevention of HSV-2 in both women and men an important clinical and public health objective.
When the groundbreaking results of the CAPRISA-004 trial (conducted by the Centre for the AIDS Programme of Research in South Africa, CAPRISA) were first presented at the XVIII International AIDS Conference in July 2010, showing that vaginal application of tenofovir 1% gel was associated with a 39% decrease in HIV acquisition risk, the additional finding of a 51% reduction in HSV-2 acquisition among susceptible participants was a welcome surprise.Citation4,Citation5 Although this finding regarding HSV-2 has thus far neither been formally published in the scientific literature nor replicated in another clinical trial, it has spawned considerable interest in the potential of this antiretroviral agent to prevent this ubiquitous infection. This paper reviews the characteristics of tenofovir and the results of the CAPRISA-004 trial, provides an explanation for the drug’s anti-herpetic activity, discusses the potential benefits of HSV-2 prevention in women independent of HIV infection status, and raises some unresolved questions about the potential for using this drug for this purpose.
Tenofovir
Tenofovir has been widely used for the treatment of established HIV and hepatitis B infections for several years, and is available as an oral tablet containing 300 mg of the prodrug tenofovir disoproxil fumarate (TDF). Its active metabolite is tenofovir diphosphate, an adenosine analog that acts as an obligate chain terminator of the HIV reverse transcriptase. TDF is available both independently and in fixed-dose coformulated tablets containing another antiretroviral drug, emtricitabine (FTC), and is commonly recommended as part of first-line combination regimens in HIV treatment guidelines worldwide.Citation6–Citation10 Important clinical features of this agent are its potent antiviral activity against both HIV and hepatitis B virus, long intracellular half-life that allows for once-daily dosing, and relatively favorable toxicity profile.
Formulation of tenofovir as a 1% gel represents the first development of an existing antiretroviral drug as a microbicide against HIV. Microbicides are products designed for topical application to the vagina or rectum for the purpose of reducing the risk of acquiring sexually transmitted infections such as HIV and HSV-2. Given the relentless spread of HIV infection worldwide, as well as the biological and social factors which predispose many women to a heightened risk of acquiring sexually transmitted pathogens, there has been considerable interest in developing a female-controlled microbicide against HIV for many years. In particular, difficulties in negotiating condom use by male partners represent a particularly important challenge for many women rooted in gender-based power dynamics, and microbicides could be used without requiring the explicit knowledge or consent of sexual partners. Unfortunately, several earlier HIV microbicide candidates, including the spermicide nonoxynol-9, polyanion products such as Carraguard® and PRO 2000®, the surfactant C31G or SAVVY, and the acid-buffering agent BufferGel® have proven to be ineffective in preventing HIV, and in some cases even enhanced HIV susceptibility, most likely by increasing mucosal ulceration and inflammation.Citation11–Citation15
Tenofovir 1% gel contains 40 mg of 9-[(R)-2-phosphonomethoxy] propyl]adenine monohydrate (PMPA) in a purified water solution with edetate disodium, citric acid, glycerin, methylparaben, propylparaben, and hydroxyethylcellulose. This agent was deemed to be a good candidate for an HIV microbicide given its long half-life and favorable safety profile. Early studies using the gel showed the product to be safe and well tolerated when used twice daily for 2 weeks in a trial of 48 sexually abstinent women in the US,Citation16 and when used in either a once-daily or coitally-dependent fashion in a 6-month trial of 200 sexually active women in India and the US.Citation17 Acceptability was also high, with 94% and 90%–92% of participants in each trial, respectively, agreeing that they would be willing to use the product if it was demonstrated to have anti-HIV efficacy.Citation16,Citation17 Further, data from animal modelsCitation18,Citation19 and ex vivo culture systemsCitation20 provided proof of concept for the efficacy of this microbicide in preventing HIV. However, until the CAPRISA-004 trial, robust human efficacy data were not available.
CAPRISA-004 trial
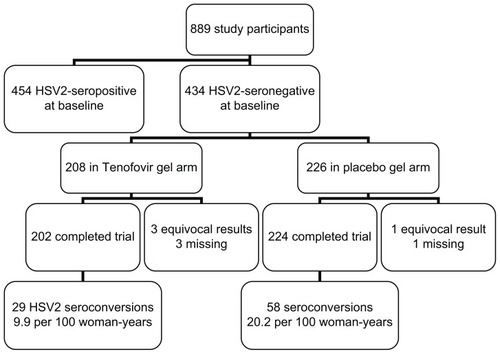
CAPRISA-004 was a randomized, double-blind, placebocontrolled clinical trial of tenofovir 1% vaginal gel as a strategy for preventing incident HIV infections among women aged 18–40 years not infected with HIV.Citation5 Participants were instructed to apply one dose of the gel within 12 hours Before coitus, followed by a second dose as soon as possible within 12 hours Afterwards, to a maximum of Two doses per 24-hour period (ie. the so-called “BAT24” dosing strategy). All participants also received comprehensive HIV prevention services, including pretest and post-test counseling, sexually transmitted infection monitoring and treatment, and condoms, as well as an adherence support program involving motivational interviewing. In the primary efficacy analysis, the incidence of HIV (95% confidence interval [CI]) was 5.6 (4.0–7.7) per 100 woman-years in the active arm versus 9.1 (6.9–11.7) in the placebo arm, giving an incidence rate ratio of 0.61 (95% CI 0.40–0.94). Acceptability of the gel was high at 97.4%.
Unexpectedly, the trial also found tenofovir 1% gel to be associated with a decreased incidence of serologically confirmed HSV-2 infection, with an incidence (95% CI) of 9.9 (6.6–14.2) per 100 woman-years in the active arm versus 20.2 (15.3–26.1) in the placebo arm, giving an incidence rate ratio of 0.49 (0.30–0.78) or 51% (22%–70%) efficacy ().Citation4 Sensitivity analyses that variously assigned equivocal HSV-2 serology results as HSV-2 seronegative or seropositive did not significantly change the conclusions, and adjustment for potential confounders including study site, age, condom use, sexually transmitted infections, contraceptive use,
Figure 1 Herpes simplex virus type 2 prevention with tenofovir 1% vaginal gel in the CAPRISA-004 trial. number of sexual partners, and parity gave a similar efficacy estimate of 47% (33%–83%).
Tenofovir: an antiherpes drug?
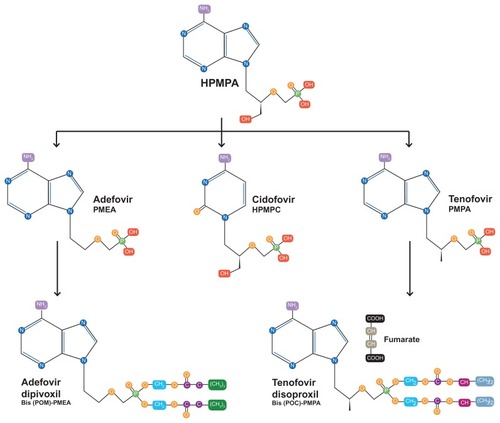
While previous microbicides such as PRO-2000, Carraguard, Buffergel, and others had in part been conceived of as HSV-2 prevention tools based on data from in vitro systems,Citation21 animal models,Citation22–Citation24 and early human data,Citation25 the CAPRISA result was surprising because tenofovir had not previously been widely conceived of as an anti-herpetic agent. Indeed, early studies during the development of tenofovir showed the compound to have little if any anti-HSV activity.Citation26 However, more detailed examination of the molecular chemistry of tenofovir reveals close similarity with the anti-cytomegalovirus agent, cidofovir (). Both compounds, along with adefovir, are classified as acyclic nucleoside phosphonates, and are derivatives of (S)-9-(3-hydroxy-2-phosphonylmethoxypropyl) adenine (HPMPA), itself originally developed as a broad-spectrum anti-DNA virus agent.Citation27
Figure 2 Chemical structure of tenofovir showing similarities to other anti-DNA virus compounds.
More recently, in an effort to explain the CAPRISA-004 findings, the direct activity of tenofovir against both laboratory and clinical strains of HSV-2 and HSV-1 has been confirmed in vitro using cell cultures of human embryonic lung fibroblasts and primary human keratinocytes, where the EC50 for HSV-2 was found to range from 85,000 to 193,000 ng/mL, as well as ex vivo human tonsillar and cervicovaginal tissues, and a mouse model.Citation28 Although the concentrations required were 1–2 orders of magnitude greater than for traditional anti-herpetic drugs like acyclovir and cidofovir, replication of clinical HSV isolates was inhibited in a dose-dependent manner. The cell culture findings are similar to original reports showing an EC50 of 244 μM or 70,000 ng/mL for (R)-PMPA against HSV-2.Citation26
However, importantly, standard doses of oral TDF do not appear to exhibit similarly meaningful anti-HSV activity in the genital tract. In a study of 40 HIV-1 seropositive persons coinfected with HSV-1 and/or HSV-2 who were taking daily oral TDF as part of suppressive combination antiretroviral therapy, for instance, we observed no decreases in HSV shedding from the oral, genital, or anal mucosa during a 28-day sampling period using polymerase chain reaction for detection of HSV.Citation29 Further, a subanalysis of the iPrEx (Preexposure Prophylaxis Initiative) trial, the primary analysis of which demonstrated 44% efficacy of oral TDF compared with placebo in preventing HIV among men who have sex with men,Citation30 found no difference in the rate of HSV-2 acquisition between the study arms in the 1416 participants who were HSV-2 seronegative at baseline.Citation31
The most likely explanation for these discrepant results is that, in contrast with topical application, standard dose oral TDF produces inadequate genital tract concentrations to block HSV-2 replication and acquisition ().Citation32–Citation36 When used as part of a suppressive antiretroviral treatment regimen, TDF achieves excellent penetration of both the female and male genital tract, and the demonstrated efficacy of daily oral TDF in preventing sexually transmitted HIV infection in several recent clinical trials shows the adequacy of achievable genital tract concentrations (roughly 70–80 ng/mL in cervicovaginal fluid) for inhibiting HIV.Citation30 However, these concentrations are low in comparison with the in vitro EC50 of tenofovir for HSV-2, cited above at 70,000–193,000 ng/mL in various studies.Citation26,Citation28 In contrast, the median cervicovaginal fluid tenofovir concentration achieved among tenofovir gel users who remained HIV-negative throughout the CAPRISA trial was 520 (range 0–1.3 million) ng/mL,Citation32 and among healthy volunteers using a single dose of the gel was roughly 100,000 ng/mL.Citation36 Still higher cervicovaginal fluid concentrations are achievable in healthy volunteers using multiple doses of the vaginal gel.Citation36 Further supporting this pharmacokinetic hypothesis, a relationship was observed between cervicovaginal fluid tenofovir concentrations in the CAPRISA trial and HSV-2 acquisition risk, with 24% versus 6% of women acquiring HSV-2 if concentrations were < or > 100,000 ng/mL. Although higher doses of oral TDF might theoretically be able to overcome these pharmacokinetic challenges, the risk of treatment-limiting drug toxicities at such doses may preclude their use.
Table 1 Tenofovir and tenofovir diphosphate C24h concentrations achieved in pharmacokinetic studies of oral TDF and tenofovir 1% vaginal gel
Further clinical trial data in different populations and study settings are needed to confirm that tenofovir 1% gel is an effective microbicide not only against HIV but HSV-2 as well. An unfortunate setback in this regard was the announcement in November 2011 that the VOICE (Vaginal and Oral Interventions to Control the Epidemic) trial was discontinuing the tenofovir and placebo gel arms of the trial early, upon recommendation from the trial’s independent data safety and monitoring board, due to lack of efficacy in preventing HIV. VOICE (also known as the Microbicide Trials Network or MTN-003 trial) was designed as a five-arm randomized trial comparing oral TDF, oral TDF-FTC, oral placebo, tenofovir 1% vaginal gel, and placebo gel as alternative strategies for HIV prevention among sexually active women in Uganda, Zimbabwe, and South Africa. The oral TDF arm of this trial was similarly discontinued prematurely for lack of efficacy in September 2011; the TDF-FTC and oral placebo arms of the trial continue. Data regarding HSV-2 acquisition in VOICE are not yet available, but follow-up of all trial participants is expected by August 2012, with final results by 2013. Importantly, unlike the CAPRISA-004 trial, the VOICE trial used a once-daily tenofovir gel dosing strategy, and detailed information on adherence and pericoital genital tract drug concentrations are not yet available.
Further data are also expected from MTN-021, a placebocontrolled trial of daily tenofovir 1% gel in sexually experienced adolescent females not infected with HIV, and from FACTS-001, a randomized trial of tenofovir 1% gel using the BAT24 dosing strategy being conducted among 18–30-year-old women at seven sites in South Africa. Data on pregnancy and lactation are also needed and will be obtained in the ongoing MTN-008 trial of 7-day courses of daily tenofovir 1% gel in 18–40-year-old American women. Although no differences in pregnancy outcomes or congenital anomalies were noted between the two CAPRISA-004 trial arms, participants in that trial were instructed to discontinue gel use if they became pregnant. Data on HIV-exposed uninfected infants of women who took oral TDF as part of antiretroviral therapy in pregnancy suggest no excess of small for gestational age or low birth weight, but slightly lower length and head circumference for age at one year.Citation37 However, the overall clinical relevance of these findings and their applicability to topical tenofovir use are unknown.
Benefits of HSV-2 prevention in women not infected with HIV
If confirmed to be effective in these and other studies, important benefits could derive from the use of tenofovir-based HSV-2 prophylaxis in HIV-uninfected women, including the prevention of HSV-2 related morbidity and indirect benefits in preventing HIV acquisition.
In addition to causing morbidity in the form of recurrent genital ulceration, systemic symptoms such as fever, malaise, headache, and myalgia also occur during primary HSV-2 infection in 70% of women, and other manifestations may include dysuria, cervicitis, and central nervous system complications, including urinary retention and aseptic meningitis. HSV can also be transported via the lymphatics to cause disseminated infection, and HSV viremia can be detected using polymerase chain reaction in 24% of uncomplicated primary genital infections, although the clinical consequences of this viremia are unknown.Citation38 These manifestations are further associated with considerable psychological distress and utilization of health care resources. Of still greater concern is the potential in pregnancy for neonatal HSV infection, a devastating and potentially fatal vertically transmitted condition, with skin, mucosal, neurological, and/or disseminated visceral manifestations. The risk of neonatal HSV is greatest if primary HSV infection (ie, infection in the absence of either HSV-1 or 2 antibodies) occurs during pregnancy,Citation39 making the prevention of HSV-2 in pregnancy an important priority.
Preventing HSV-2 would have further indirect benefits to personal and public health because HSV-2 significantly increases the risk of HIV acquisition by a factor of approximately 2.1 (95% CI 1.4–3.2).Citation40 This is particularly true because incident HSV-2 infection has a greater impact on increasing HIV acquisition risk than prevalent HSV-2.Citation41 Further, in meta-analyses that considered the relative risk of HIV associated with HSV-2 infection separately by gender, the summary adjusted relative risk was higher in women at 3.1 (95% CI 1.7–5.6), than in men (relative risk 2.7, 95% CI 1.9–3.9) and in men who have sex with men (relative risk 1.7, 95% CI 1.2–2.4).Citation42
Several biological mechanisms may underlie this negative synergy. Microscopic or macroscopic physical disruptions of the epithelial barrier of genital mucosal surfaces by HSV-2 may provide portals of entry and exit for HIV during sexual contact. Studies involving intensive daily sampling of HSV-2 infected adults have shown that roughly 40%–50% of shedding episodes in immunocompetent adults are asymptomatic and brief, at only 12 hours or less,Citation43,Citation44 and mathematical modeling further suggests that neuronal release of small numbers of HSV virions into the genital tract is nearly constant.Citation45 This frequent, low-level viral shedding is difficult to suppress even with high doses of anti-HSV medication.Citation46 In addition, the host immune response to HSV-2 reactivation involves an influx of CD4-positive T cells, thereby increasing the pool of locally susceptible target cells in persons sexually exposed to HIV.Citation47–Citation49
Of note, detailed analyses from the CAPRISA-004 trial show that tenofovir gel reduced the risk of HIV acquisition to a similar degree in participants with and without HSV-2 infection; further, after adjustment for prevalent HSV-2 infection, the effect of tenofovir on HIV prevention was not significantly changed. In contrast, mathematical modeling suggests a partial role of HSV-2 prevention in preventing HIV.Citation50 Taken together, these findings suggest that tenofovir-related HSV-2 prevention at best contributed modestly to its HIV prevention effect in this trial, although long-term benefits of HSV-2 prevention in reducing HIV risk likely exist.
Benefits of HSV-2 prevention in HIV-infected women
Among HIV-infected populations, the estimated HSV-2 seroprevalence is 60%–95%.Citation51 Preventing HSV-2 in the remaining 5%–40% of HIV-infected women is also important for several reasons. First, the usual manifestations of HSV-2 are exacerbated in the context of HIV. Mucocutaneous shedding of HSV is greater in frequency and quantity in the context of HIV. A study among 176 women showed the prevalence of asymptomatic genital HSV-2 culture positivity to be roughly four times higher in HIV-infected than in uninfected participants (13.2% versus 3.6%, P = 0.04; odds ratio 4.1, 95% CI 1.0–27.4).Citation52 Symptomatic reactivations of HSV-2 are also more frequent and severe with increasing HIV-related immunosuppression,Citation53 and can cause extensive lesions featuring deep ulceration and necrosis, and chronic mucocutaneous HSV infection is considered an acquired immune deficiency syndrome (AIDS)-defining illness.Citation54,Citation55 As in other immunocompromised populations, HSV-2 can also produce atypical hypertrophic, verrucous, and nodular lesions in HIV-infected hosts regardless of CD4 count that can be challenging to treat.Citation56,Citation57 Further complicating the management of HIV and HSV-2 coinfection is the risk of acyclovir resistance which may necessitate second-line therapies; resistant strains of HSV-2 are largely confined to patients with advanced AIDS and chronic herpetic ulcerations.Citation58 These exacerbations and perturbations of the usual clinical manifestations of HSV-2 in the setting of HIV are felt to be attributable to HIV-related impairment of T cell immunity against the virus. Both the breadth and the magnitude of T cell responses to HSV-2 are downregulated in HIV, and HSV-2 coinfected individuals compared with HSV-2 monoinfected individuals.Citation59,Citation60
Second, because HSV-2 reactivations are associated with increases in plasma HIV viral load,Citation61 preventing HSV-2 in HIV-infected women could theoretically avoid an adverse impact of HSV-2 on HIV disease progression. Importantly, however, definitive evidence from longitudinal studies that HSV-2 accelerates HIV disease progression is lacking.Citation62 Although two clinical trials from Sub-Saharan Africa demonstrated modest attenuation in HIV disease progression among HSV-2 coinfected adults randomized to receive acyclovir 400 mg twice daily,Citation63,Citation64 it is likely that these benefits derive at least in part from the direct anti-HIV effects of acyclovir rather than from the reversal of HSV-2-related effects.Citation65,Citation66
Finally, HSV-2 prevention among HIV-infected persons could have downstream benefits in decreasing onward HIV transmission, given that coinfection is thought to increase HIV transmissibility.Citation67 A study in Uganda showed that genital ulcer disease, the bulk of which was caused by HSV-2, increased the risk of transmitting HIV to sexual partners by roughly four-fold.Citation68
Unanswered questions
Although the CAPRISA-004 trial provided proof-of-concept that topical tenofovir can prevent HIV and HSV-2 infections in women, several important questions remain regarding delivery systems, drug formulation, rectal administration, drug resistance, and usage in the management of established HSV infection, among other issues.
Delivery systems
The optimal delivery system for achieving relevant genital tract concentrations using topical tenofovir remains to be determined. Limitations of the vaginal gel formulation are that it is relatively short-acting (hence requiring repeated applications), requires use of an applicator, and can be associated with leakage. Extended-release systems that require reapplication only every 1–3 months, such as intravaginal rings, may thus be an attractive alternative, offering advantages including coital independence, improved adherence, and greater acceptability.Citation69 Such systems further offer the potential for coadministration with more than one active ingredient, such as a contraceptive or additional microbicide, although not without their own challenges. Given the water solubility of tenofovir, for instance, coformulation with hydrophobic drugs such as levonorgestrel and the investigational antiretroviral, dapivirine, may require a segmented design,Citation70 and technical challenges may preclude inclusion of more than two agents.Citation71 Also, there remain unanswered questions about whether hormonal contraception potentiates HIV acquisition.Citation72
At present, a tenofovir-loaded polyurethane ring capable of releasing 10 mg tenofovir daily for 90 days is under evaluation, as is a combination ring containing levonorgestrel. The combination of tenofovir with acyclovir has also been studied in animal models as a strategy for improving efficacy in preventing HSV-2, and shown to produce constant drug release rates.Citation73,Citation74 Other novel delivery systems under investigation for delivering tenofovir to the vagina include a pH-responsive nanoparticle system,Citation75,Citation76 and could include bioadhesive films and vaginal tablets, although none of these methods would offer extended-release possibilities. Combination of tenofovir with novel HIV non-nucleoside reverse transcriptase inhibitors has also been explored, although retaining the gel formulation.Citation77,Citation78
Formulation
Whether tenofovir or a prodrug offers a better formulation for HSV-2 preventive applications is another important question. Although TDF cannot be formulated into a gel because of its hydrolytic instability,Citation79 TDF is suitable for formulation in an intravaginal ring, and confers the advantage over tenofovir of increased hydrophobicity, potentially resulting in improved uptake into cells.Citation80,Citation81 GS-7340 is another prodrug of tenofovir, which, when taken orally, has a longer half-life in the bloodstream than TDF, and more intracellular rather than bloodstream metabolism compared with tenofovir.Citation82 These properties of GS-7340 are being exploited in clinical trials for the treatment of established HIV infection, where it is hoped that greater antiviral efficacy and lower systemic toxicity can be achieved with a lower drug dose. Whether the formulation will achieve clinically relevant concentrations in the vaginal tract for preventing HSV-2 remains to be determined.
Rectal application
Because receptive anal intercourse is another important potential route for transmission of both HIV and HSV-2, tenofovir 1% gel has been studied for its safety and tolerability as a rectal microbicide. In a Phase I trial of 18 participants, including four women, the original vaginal formulation was associated with a suboptimal gastrointestinal side effect profile when applied rectally.Citation83 A reduced glycerin formulation was thus developed specifically for rectal application, the decreased osmolality of which (836 mOsmol/kg compared with 3111 mOsmol/kg for the vaginal gel) was associated with acceptable systemic and mucosal safety, acceptability, and adherence in a trial of 65 participants (including 20 women);Citation84 further testing in MTN-017, an 8-week Phase II trial, is planned.
Drug resistance
An important consideration with prophylactic tenofovir is the potential for the development of antiviral drug resistance, particularly in HIV, but whether clinically relevant tenofovir resistance mutations exist in HSV-2 is unknown. One scenario in which such resistance could theoretically arise is in women not infected with HIV who develop breakthrough infection but continue to use topical tenofovir before the diagnosis is made, even though systemic absorption of the gel is known to be low. Another scenario in which such resistance could arise is if topical tenofovir is used for HSV-2 prevention by women already known to have HIV infection. Such use could be restricted to patients already receiving highly active antiretroviral therapy to minimize the risk of systemic drug resistance, although resistance in the genital compartment could theoretically emerge, with public health implications.
Importantly, of the 35 CAPRISA-004 participants who acquired HIV in the tenofovir arm and whose plasma samples could be tested for resistance, no tenofovir-related resistance mutations (K65R or K70E) were observed on bulk sequencing,Citation5 nor were there clinically relevant mutation frequencies by deep pyrosequencing.Citation85 Among the 21 women whose cervicovaginal swab specimens could be tested for resistance, only one had detectable K65R at a frequency of 0.8% from proviral DNA only; this level is in the range observed for drug-naïve HIV patients.Citation86 These encouraging results must be interpreted in light of the limited exposure of the virus to the drug in these women; resistance assays in plasma were conducted an estimated 3–4 weeks after HIV acquisition in these women, and only three of the 21 cervicovaginal specimens contained detectable drug at all.Citation5,Citation86
Role in clinical management of HSV infection
If tenofovir is an anti-herpes medication, it is reasonable to envisage potential roles for the drug in the management of established HSV infection and reduction of onward HSV transmission, in addition to primary prevention of HSV. Such roles could involve chronic suppressive therapy for individuals with frequent outbreaks or for prevention purposes, as well as short-course treatment of herpes flares, akin to current therapeutic indications for acyclovir and related compounds. Topical formulations would be best suited to this role, give that oral TDF appears unlikely to have a clinically meaningful impact on HSV shedding or symptoms,Citation29 and could offer the additional advantage of decreased systemic absorption and related toxicities. A Phase IV trial of oral and topical tenofovir for reducing HSV shedding in HSV-2 seropositive, HIV-uninfected persons (NCT01448616) is currently underway. The documented activity of tenofovir against HSV-1 in addition to HSV-2 is also relevant in this regard,Citation26,Citation28 given the increasingly important role of HSV-1 in genital herpes infection in many settings and its potential relevance to HIV infection.Citation87
Conclusion
Although not previously considered to be an anti-herpes medication, tenofovir has recently been demonstrated to have in vitro activity against HSV-2 and in vivo protective efficacy against HSV-2 acquisition as a vaginal microbicide. Further study is needed to confirm these clinical findings, assess its potential use in other populations, and optimize formulation and delivery systems. These efforts may eventually identify HSV-2 prevention as a new use for this existing drug, with unique advantages over existing strategies, including potential for use without requiring the consent of sexual partners. Nevertheless, the available data suggest an incomplete protective effect of tenofovir 1% gel against HSV-2 acquisition at only 51%, cautioning that this strategy must be complemented by ongoing efforts to develop other novel anti-herpetic drugs and a protective HSV-2 vaccine.
Acknowledgment
The author receives postdoctoral fellowship funding from the Ontario HIV Treatment Network.
Disclosure
The author reports no relevant conflicts of interest in this work.
References
- Paz-BaileyGRamaswamyMHawkesSJGerettiAMHerpes simplex virus type 2: epidemiology and management options in developing countriesSex Transm Infect200783162217098770
- MertzGJBenedettiJAshleyRSelkeSACoreyLRisk factors for the sexual transmission of genital herpesAnn Intern Med19921161972021309413
- CoreyLAdamsHGBrownZAHolmesKKGenital herpes simplex virus infections: clinical manifestations, course, and complicationsAnn Intern Med1983989589726344712
- KarimSSKarimQEffectiveness and safety of vaginal microbicide 1% tenofovir gel for prevention of HIV infection in womenAbstract TUSS0204 presented at the XVIII International AIDS ConferenceJuly 18–23, 2010Vienna, Austria
- Abdool KarimQAbdool KarimSSFrohlichJAEffectiveness and safety of tenofovir gel, an antiretroviral microbicide, for the prevention of HIV infection in womenScience20103291168117420643915
- Panel on Antiretroviral Guidelines for Adults and Adolescents Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescentsDepartment of Health and Human Services Available at: http://www.aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdfAccessed April 10, 2012
- ThompsonMAAbergJACahnPAntiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panelJAMA201030432133320639566
- European AIDS Clinical SocietyGuidelines: clinical management and treatment of HIV infected adults in Europe Available at: http://www.europeanaidsclinicalsociety.org/index.php?option=com_content&view=article&id=59&Itemid=41Accessed June 2, 2012
- GazzardBGAndersonJBabikerABritish HIV Association guidelines for the treatment of HIV-1-infected adults with antiretroviral therapy 2008HIV Med2008956360818826546
- World Health OrganisationRapid advice: antiretroviral therapy for HIV infection in adults and adolescents Available at: http://www.who.int/hiv/pub/arv/advice/en/index.htmlAccessed July 2, 2012
- Van DammeLRamjeeGAlaryMEffectiveness of COL-1492, a nonoxynol-9 vaginal gel, on HIV-1 transmission in female sex workers: a randomised controlled trialLancet200236097197712383665
- PetersonLNandaKOpokuBKSAVVY (C31G) gel for prevention of HIV infection in women: a Phase 3, double-blind, randomized, placebo-controlled trial in GhanaPLoS One20072e131218091987
- Skoler-KarpoffSRamjeeGAhmedKEfficacy of Carraguard for prevention of HIV infection in women in South Africa: a randomised, double-blind, placebo-controlled trialLancet20083721977198719059048
- McCormackSRamjeeGKamaliAPRO2000 vaginal gel for prevention of HIV-1 infection (Microbicides Development Programme 301): a phase 3, randomised, double-blind, parallel-group trialLancet20103761329133720851460
- Abdool KarimSSRichardsonBARamjeeGSafety and effectiveness of BufferGel and 0.5% PRO2000 gel for the prevention of HIV infection in womenAIDS20112595796621330907
- MayerKHMaslankowskiLAGaiFSafety and tolerability of tenofovir vaginal gel in abstinent and sexually active HIV-infected and uninfected womenAIDS20062054355116470118
- HillierSLJoshiSCyrus-CameronESafety and acceptability of coitally dependent use of 1% tenofovir gel over six months of useAbstract 655 presented at the Microbicides ConferenceFebruary 24–27, 2008New Delhi, India
- CranageMSharpeSHerreraCPrevention of SIV rectal transmission and priming of T cell responses in macaques after local pre-exposure application of tenofovir gelPLoS Med20085e15718684007
- ParikhUMDobardCSharmaSComplete protection from repeated vaginal simian-human immunodeficiency virus exposures in macaques by a topical gel containing tenofovir alone or with emtricitabineJ Virol200983103581036519656878
- RohanLCMonclaBJKunjara Na AyudhyaRPIn vitro and ex vivo testing of tenofovir shows it is effective as an HIV-1 microbicidePLoS One20105e931020174579
- CheshenkoNKellerMJMasCasulloVCandidate topical microbicides bind herpes simplex virus glycoprotein B and prevent viral entry and cell-to-cell spreadAntimicrob Agents Chemother2004482025203615155195
- ZacharopoulosVRPhillipsDMVaginal formulations of carrageenan protect mice from herpes simplex virus infectionClin Diagn Lab Immunol199744654689220165
- MaguireRABergmanNPhillipsDMComparison of microbicides for efficacy in protecting mice against vaginal challenge with herpes simplex virus type 2, cytotoxicity, antibacterial properties, and sperm immobilizationSex Transm Dis20012825926511354263
- ZeitlinLHoenTEAchillesSLTests of Buffergel for contraception and prevention of sexually transmitted diseases in animal modelsSex Transm Dis20012841742311460027
- KellerMJZerhouni-LayachiBCheshenkoNPRO 2000 gel inhibits HIV and herpes simplex virus infection following vaginal application: a double-blind placebo-controlled trialJ Infect Dis2006193273516323128
- BalzariniJHolyAJindrichJDifferential antiherpesvirus and antiretrovirus effects of the (S) and (R) enantiomers of acyclic nucleoside phosphonates: potent and selective in vitro and in vivo antiretrovirus activities of (R)-9-(2-phosphonomethoxypropyl)-2,6-diaminopurineAntimicrob Agents Chemother1993373323388452366
- De ClercqEThe acyclic nucleoside phosphonates from inception to clinical use: historical perspectiveAntiviral Res20077511317116336
- AndreiGLiscoAVanpouilleCTopical tenofovir, a microbicide effective against HIV, inhibits herpes simplex virus-2 replicationCell Host Microbe20111037938922018238
- TanDHKaulRRaboudJMWalmsleySLNo impact of oral tenofovir disoproxil fumarate on herpes simplex virus shedding in HIV-infected adultsAIDS20112520721021150556
- GrantRMLamaJRAndersonPLPreexposure chemoprophylaxis for HIV prevention in men who have sex with menN Engl J Med20103632587259921091279
- LamaJMayerKSchechterMOral TDF and its impact in HSV-2 acquisition and clinical expressionAbstract 1003 presented at the 18th Conference on Retroviruses and Opportunistic InfectionsFebruary 27–March 2, 2011Boston, MA
- KashubaADAbdool KarimSSKraftEDo systemic and genital tract tenofovir concentrations predict HIV seroconversion in the CAPRISA 004 tenofovir gel trialAbstract TUSS0503 presented at the XVIII International AIDS ConferenceJuly 18–23, 2010Vienna, Austria
- PattersonKBPrinceHAKraftEPenetration of tenofovir and emtricitabine in mucosal tissues: implications for prevention of HIV-1 transmissionSci Transl Med20113112114
- DumondJBYehRFPattersonKBAntiretroviral drug exposure in the female genital tract: implications for oral pre- and post-exposure prophylaxisAIDS2007211899190717721097
- KwaraADelongARezkNAntiretroviral drug concentrations and HIV RNA in the genital tract of HIV-infected women receiving long-term highly active antiretroviral therapyClin Infect Dis20084671972518220480
- SchwartzJLRountreeWKashubaADA multi-compartment, single and multiple dose pharmacokinetic study of the vaginal candidate microbicide 1% tenofovir gelPLoS One20116e2597422039430
- SiberryGKWilliamsPLMendezHSafety of tenofovir use during pregnancy: early growth outcomes in HIV-exposed uninfected infantsAIDS2012261151115922382151
- JohnstonCMagaretASelkeSRemingtonMCoreyLWaldAHerpes simplex virus viremia during primary genital infectionJ Infect Dis2008198313418471083
- BrownZASelkeSZehJThe acquisition of herpes simplex virus during pregnancyN Engl J Med19973375095159262493
- WaldALinkKRisk of human immunodeficiency virus infection in herpes simplex virus type 2-seropositive persons: a meta-analysisJ Infect Dis2002185455211756980
- ReynoldsSJRisbudARShepherdMERecent herpes simplex virus type 2 infection and the risk of human immunodeficiency virus type 1 acquisition in IndiaJ Infect Dis20031871513152112721931
- FreemanEEWeissHAGlynnJRCrossPLWhitworthJAHayesRJHerpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studiesAIDS200620738316327322
- MarkKEWaldAMagaretASRapidly cleared episodes of herpes simplex virus reactivation in immunocompetent adultsJ Infect Dis20081981141114918783315
- MarkKEWaldAMagaretASRapidly cleared episodes of oral and anogenital herpes simplex virus shedding in HIV-infected adultsJ Acquir Immune Defic Syndr20105448248820616743
- SchifferJTAbu-RaddadLMarkKEFrequent release of low amounts of herpes simplex virus from neurons: results of a mathematical modelSci Transl Med200917ra16
- JohnstonCSaracinoMKuntzSStandard-dose and highdose daily antiviral therapy for short episodes of genital HSV-2 reactivation: three randomised, open-label, cross-over trialsLancet201237964164722225814
- CunninghamALTurnerRRMillerACParaMFMeriganTCEvolution of recurrent herpes simplex lesions. An immunohistologic studyJ Clin Invest1985752262333880773
- KoelleDMAbboHPeckAZiegweidKCoreyLDirect recovery of herpes simplex virus (HSV)-specific T lymphocyte clones from recurrent genital HSV-2 lesionsJ Infect Dis19941699569618169426
- KoelleDMCoreyLBurkeRLAntigenic specificities of human CD4+ T-cell clones recovered from recurrent genital herpes simplex virus type 2 lesionsJ Virol199468280328107512152
- BoilyMCDimitrovDMâsseBHow much of the overall microbicide effectiveness against HIV is due to the protection of TFV gel against HSV-2 The CAPRISA-004 trialAbstract 999 presented at the 18th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2011Boston, MA
- GuptaRWarrenTWaldAGenital herpesLancet20083702127213718156035
- AugenbraunMFeldmanJChirgwinKIncreased genital shedding of herpes simplex virus type 2 in HIV-seropositive womenAnn Intern Med19951238458477486467
- BagdadesEKPillayDSquireSBO’NeilCJohnsonMAGriffithsPDRelationship between herpes simplex virus ulceration and CD4+ cell counts in patients with HIV infectionAIDS19926131713201361745
- SafrinSAshleyRHoulihanCCusickPSMillsJClinical and serologic features of herpes simplex virus infection in patients with AIDSAIDS19915110711101657040
- SiegalFPLopezCHammerGSSevere acquired immunodeficiency in male homosexuals, manifested by chronic perianal ulcerative herpes simplex lesionsN Engl J Med1981305143914446272110
- YudinMHKaulRProgressive hypertrophic genital herpes in an HIVinfected woman despite immune recovery on antiretroviral therapyInfect Dis Obstet Gynecol2008200859253218784844
- HolmesAMcMenaminMMulcahyFBerginCThalidomide therapy for the treatment of hypertrophic herpes simplex virus-related genitalis in HIV-infected individualsClin Infect Dis200744e96e9917479932
- BaconTHLevinMJLearyJJSariskyRTSuttonDHerpes simplex virus resistance to acyclovir and penciclovir after two decades of antiviral therapyClin Microbiol Rev20031611412812525428
- ShethPMSunderjiSShinLYCoinfection with herpes simplex virus type 2 is associated with reduced HIV-specific T cell responses and systemic immune activationJ Infect Dis20081971394140118444797
- KaulRPettengellCShethPMThe genital tract immune milieu: an important determinant of HIV susceptibility and secondary transmissionJ Reprod Immunol200877324017395270
- GrayRHLiXWawerMJDeterminants of HIV-1 load in subjects with early and later HIV infections, in a general-population cohort of Rakai, UgandaJ Infect Dis2004181209121515031789
- TanDHSMurphyKShahPSWalmsleySLSystematic review of the impact of herpes simplex virus type 2 on HIV disease progressionAbstract 305 presented at the Ontario HIV Treatment Network Research ConferenceNovember 14–15, 2011Toronto, Canada
- LingappaJRBaetenJMWaldADaily aciclovir for HIV-1 disease progression in people dually infected with HIV-1 and herpes simplex virus type 2: a randomised placebo-controlled trialLancet201037582483320153888
- ReynoldsSJMakumbiFNewellKEffect of daily aciclovir on HIV disease progression in individuals in Rakai, Uganda, co-infected with HIV-1 and herpes simplex virus type 2: a randomised, double-blind placebo-controlled trialLancet Infect Dis20121244144822433279
- McMahonMASilicianoJDLaiJThe antiherpetic drug acyclovir inhibits HIV replication and selects the V75I reverse transcriptase multidrug resistance mutationJ Biol Chem2008283312893129318818198
- LiscoAVanpouilleCTchesnokovEPAcyclovir is activated into a HIV-1 reverse transcriptase inhibitor in herpesvirus-infected human tissuesCell Host Microbe2008426027018779052
- CoreyLWaldACelumCLQuinnTCThe effects of herpes simplex virus-2 on HIV-1 acquisition and transmission: a review of two overlapping epidemicsJ Acquir Immune Defic Syndr20043543544515021308
- GrayRHWawerMJBrookmeyerRProbability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1-discordant couples in Rakai, UgandaLancet20013571149115311323041
- MalcolmRKEdwardsKLKiserPRomanoJSmithTJAdvances in microbicide vaginal ringsAntiviral Res201088Suppl 1S30S3921109066
- JohnsonTJGuptaKMFabianJAlbrightTHKiserPFSegmented polyurethane intravaginal rings for the sustained combined delivery of antiretroviral agents dapivirine and tenofovirEur J Pharm Sci20103920321219958831
- FriendDRDrug delivery in multiple indication (multipurpose) prevention technologies: systems to prevent HIV-1 transmission and unintended pregnancies or HSV-2 transmissionExpert Opin Drug Deliv2012941742722385316
- BlishCABaetenJMHormonal contraception and HIV-1 transmissionAm J Reprod Immunol20116530230721087338
- KellyLCarrDClarkMRIn vivo release in sheep of a dual loaded microbicide polyurethane vaginal ringPaper presented at the American Association of Pharmaceutical Scientists Annual Meeting and ExpositionOctober 23–27, 2011Washington, DC
- MossJAMaloneAMSmithTJSimultaneous delivery of tenofovir and acyclovir via an intravaginal ringAntimicrob Agents Chemother20125687588222123689
- ZhangTSturgisTFYouanBBpH-responsive nanoparticles releasing tenofovir intended for the prevention of HIV transmissionEur J Pharm Biopharm20117952653621736940
- AlukdaDSturgisTYouanBBFormulation of tenofovir-loaded functionalized solid lipid nanoparticles intended for HIV preventionJ Pharm Sci20111003345335621437910
- HamASUgaonkarSRShiLDevelopment of a combination microbicide gel formulation containing IQP-0528 and tenofovir for the prevention of HIV infectionJ Pharm Sci20121011423143522227864
- KiserPFMahalingamAFabianJDesign of tenofovir-UC781 combination microbicide vaginal gelsJ Pharm Sci20121011852186422359356
- AndersonPLKiserJJGardnerEMRowerJEMeditzAGrantRMPharmacological considerations for tenofovir and emtricitabine to prevent HIV infectionJ Antimicrob Chemother20116624025021118913
- MossJABaumMMMaloneAMTenofovir and tenofovir disoproxil fumarate pharmacokinetics from intravaginal ringsAIDS20122670771022210639
- MesquitaPMRastogiRSegarraTJIntravaginal ring delivery of tenofovir disoproxil fumarate for prevention of HIV and herpes simplex virus infectionJ Antimicrob Chemother20126771730173822467632
- RuanePDeJesusEBergerDGS-7340 25 mg and 40 mg demonstrate superior efficacy to tenofovir disoproxil fumarate 300 mg in a 10-day monotherapy study of HIV-1+ patientsAbstract 103 presented at the 19th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2012Seattle, WA
- AntonPCranstonRCarballo-DieguezARMP-02/MTN-006: A phase 1 placebo-controlled trial of rectally applied 1% vaginal TFV gel with comparison to oral TDFAbstract 34 LB presented at the 18th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2011Boston, MA
- McGowanIHoesleyCAndrewPMTN-007: a Phase 1 randomized, double-blind, placebo-controlled rectal safety and acceptability study of tenofovir 1% gelAbstract 34LB presented at the19th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2012Seattle, WA
- FischerWHuntGSibekoSTenofovir resistance mutation frequencies assessed by deep pyrosequencing of plasma virus from breakthrough HIV infections: CAPRISA 004 microbicide trialAbstract 1063 presented at the 19th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2012Seattle, WA
- WeiXMorrisLNaranbhaiVSensitive tenofovir resistance screening of HIV-1 from the genital tract of women with breakthrough infections: CAPRISA 004 tenofovir gel trialAbstract 33 presented at the 19th Conference on Retroviruses and Opportunistic InfectionsMarch 5–8, 2012Seattle, WA
- TanDHKaulRWalsmleySLeft out but not forgotten: should closer attention be paid to coinfection with herpes simplex virus type 1 and HIV?Can J Infect Dis Med Microbiol200920e1e720190881