
Abstract
Introduction
Fluticasone furoate (FF)/vilanterol (VI) dry powder inhaler (DPI) is the only once-daily maintenance inhaled corticosteroid (ICS)/long-acting β2 adrenergic agonist (LABA) combination for asthma. We aimed to compare the clinical effects of once-daily FF/VI and twice-daily budesonide (BUD)/formoterol (FM) DPI in patients with controlled stable asthma.
Methods
We performed a randomized crossover trial in which stable asthmatic patients controlled on ICS/LABA received 8 weeks of FF/VI (100/25 μg 1 puff once-daily) or BUD/FM (160/4.5 μg 2 puffs twice-daily) DPI treatment. After a 4–8-week washout period, patients received another crossover treatment for 8 weeks. We assessed pulmonary function, the 5-item version asthma control questionnaire (ACQ5), the asthma control test (ACT), and fractional exhaled nitric oxide (FeNO) at baseline and after 8 weeks of treatment (week 8). As the primary outcome was change in force expiratory volume in 1 s (FEV1) between baseline and week 8, we evaluated the incidence of asthma exacerbation and adherence barrier questionnaire (Ask-12) at week 8.
Results
Twenty-three patients were initially enrolled in this study; however, one patient had to be excluded. The FF/VI DPI treatment group showed a similar magnitude of change in FEV1 between baseline and week 8 as the BUD/FM DPI treatment group. In addition, there were no significant differences in pulmonary function tests, ACQ5 scores, ACT scores, and FeNO between baseline and week 8 in both groups. Although the incidence of exacerbation did not differ between groups, the Ask-12 score in the FF/VI DPI group was significantly lower than that in the BUD/FM DPI group.
Conclusions
The present study indicates that once-daily FF/VI DPI is not inferior to twice-daily BUD/FM DPI in clinical effect and more likely to improve inconvenience and forgetfulness in inhalation adherence barriers for stable asthma control therapy. Once-daily FF/VI DPI may be an effective alternative for asthma maintenance treatment.
Introduction
Fluticasone furoate (FF) is an inhaled corticosteroid (ICS) that confers both greater affinity for the glucocorticoid (GC) receptor and longer retention in respiratory tissues than does fluticasone propionate (FP). Once-daily FF has greater anti-inflammatory activity and is more effective than are FP and budesonide (BUD).Citation1 Furthermore, inhaled FF showed longer absorption time from lung into the systemic circulation than inhaled FP.Citation2 In patients with asthma, some randomized clinical studies have demonstrated FF improved pulmonary function, rescue inhaler use, and symptom-free compared to placebo or FP.Citation3–Citation6 Vilanterol (VI) is a once-daily inhaled long-acting β2 adrenergic agonist (LABA) shown to produce prolonged bronchodilation for at least 24 hrs. The fluticasone furoate/vilanterol (FF/VI) dry powder inhaler (DPI) combination device, Ellipta® (GlaxoSmithKline, UK), is an easy-to-use once-daily inhalation device. Most asthma patients made less errors using Ellipta than those using other devices.Citation7,Citation8 Inhaler errors in asthma management are associated with poor adherence and outcomes,Citation9 and as such, the FF/VI Ellipta device may provide improved patient adherence and treatment outcomes. Previous clinical studies of FF/VI DPI delivered from a single inhaler, conducted in patients with asthma, have confirmed efficacy and safety of the treatment.Citation10–Citation15 These randomized control studies have compared the effects of FF/VI DPI combination versus placebo or fluticasone propionate/salmeterol (FP/SLM) DPI on acute exacerbations, pulmonary function, health-related quality of life, and adverse effects, in patients with chronic asthma. In addition, there have been some reports to compare FF/VI DPI therapy with other ICS/LABA combinations, such as budesonide/formoterol (BUD/FM) DPI, and assess patient adherence in asthma inhaler treatment recently.Citation15,Citation16 Therefore, we conducted this randomized crossover study to compare the clinical effects and inhalation adherence barriers of once-daily FF/VI DPI versus twice-daily BUD/FM DPI in patients with controlled stable asthma on ICS/LABA treatment. The primary outcome of this study was changes in force expiratory volume in 1 s (FEV1). Secondary outcomes were to evaluate changes in other pulmonary function tests, the 5-item version asthma control questionnaire (ACQ5), the asthma control test (ACT), and fractional exhaled nitric oxide (FeNO) at baseline and after 8 weeks of treatment. In addition, the incidence of asthma exacerbation and adherence barrier questionnaire (Ask-12 survey) were assessed.
Materials and methods
Subjects
Patients aged 18 years or older, who were treated at Hamamatsu University School of Medicine between April 2014 and April 2015, were enrolled in this study. Patients with asthma whose disease was classified as “controlled,” according to the Global Initiative for Asthma (GINA) criteriaCitation17 of asthma control, had undergone treatment of two actuations of BUD/FM DPI combinations (160/4.5 μg) 2 puffs twice-daily for at least 3 months. All the patients were treated with GINA step 4 therapy at the registration. The exclusion criteria were as follows: (1) treatment with oral or intravenous corticosteroids in the previous 4 weeks, (2) current smoker or having a smoking history of >10 pack-years, or (3) other pulmonary diseases, including chronic obstructive pulmonary disease (COPD), lung cancer, or pulmonary fibrosis. Asthma exacerbation was defined as any of the following events due to asthma symptoms: unexpected or emergency visit to the hospital, hospitalization, and systemic corticosteroid administration for more than 3 days.
Study design
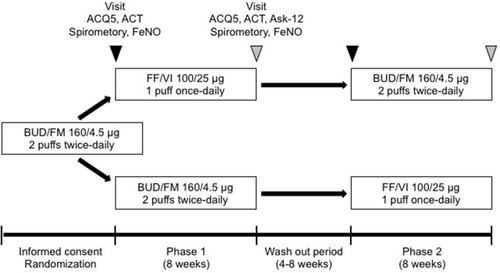
This was a prospective, randomized, open-label, two-period crossover study of the FF/VI DPI versus BUD/FM DPI therapies, conducted in accordance with the Declaration of Helsinki (). The patients who met the entry criteria completed over 2-week run-in period for evaluation of pulmonary function baseline and asthma status. After run-in period, the patients who met eligibility criteria were randomly assigned (1:1) to each of the two groups. The central randomization schedule was generated by using a computer program in our university. They received 8 weeks of FF/VI DPI treatment (100/25 μg) 1 puff once-daily or BUD/FM DPI treatment (160/4.5 μg) 2 puffs twice-daily. After a 4–8-week washout period, these patients received another crossover treatment for 8 weeks. During this study, the additional inhaled ICS other than FF and BUD, LABAs other than VI and FM, long-acting muscarinic antagonist (LAMA), theophylline, mucolytic agents, leukotriene receptor antagonist (LTRA) were withdrawn. A rescue inhaled short-acting β2 adrenergic agonist (SABA) was used on demand to control symptoms throughout the study. We assessed changes in FEV1 as a primary outcome, other pulmonary function tests, ACQ5, ACT, and FeNO at baseline and after 8 weeks of treatment (week 8). The incidence of asthma exacerbation and adherence barrier questionnaire (Ask-12 survey) were also evaluated at week 8. The study protocol was approved by the institutional review board of Hamamatsu University School of Medicine (HUSM 14–146). All patients provided written informed consent. The trial was registered with the University Hospital Medical Information Network (UMIN) Clinical Trial Registry (UMIN ID 000015609).
Figure 1 Study design. Stable asthmatic patients received 8 weeks of fluticasone furoate/vilanterol (FF/VI) dry powder inhaler (DPI) (100/25 μg 1 puff once-daily) or budesonide/formoterol (BUD/FM) DPI (160/4.5 μg 2 puffs twice-daily) treatment. After a 4–8-week washout period, patients received another crossover treatment for 8 weeks. We assessed pulmonary function, the 5-item version asthma control questionnaire (ACQ5), the asthma control test (ACT), and fractional exhaled nitric oxide (FeNO) at baseline and after 8 weeks of treatment (week 8). The incidence of asthma exacerbation and an adherence barrier questionnaire (Ask-12 survey) were evaluated at week 8.
Measurements
Pulmonary function tests
Spirometry was performed at all visits using CHESTAC-8100 (CHEST M.I. Co., Ltd., Tokyo, Japan) according to the standards of the American Thoracic Society.Citation18 The forced vital capacity (FVC), FEV1, ratio of FEV1/FVC, maximum mid-expiratory flow rate (MMF), maximum expiratory flow rate at 50% FVC (V50), and 25% FVC (V25) were evaluated.
ACQ5 and ACT scores
The ACQ5 consisted of five items assessing nocturnal waking, morning symptoms, activity limitation, shortness of breath, and wheeze during the previous 7 days, excluding frequency of short-acting β2 agonist (SABA) use and FEV1% predicted. Each item was scored on a scale of 0 to 6, where 0 represents good control and 6 represents poor control.Citation19 The overall score of the ACQ5 was the mean of the five responses. The cut-off point for well controlled asthma was ≤0.75 whereas a value of ≥1.50 confirmed uncontrolled asthma.Citation20 A change of 0.5 in each score was considered a clinically meaningful difference, ie, minimum important difference.Citation19 The ACT was a simple questionnaire, recommended by GINA.Citation17 The ACT score consisted of five questions assessing asthma symptoms (daytime and nocturnal), use of rescue medications, and the effect of asthma on daily functioning. The ACT scores for each of the five items were summed to yield a score ranging from 5 to 25 with a higher score indicating better asthma control.Citation21,Citation22
Fractional exhaled nitric oxide (FeNo)
Fractional exhaled nitric oxide was measured using the commercially available analyzer NIOX MINO (Aerocrine AB, Solna, Sweden), according to recommendations from the American Thoracic Society/European Respiratory Society.Citation23
Ask-12 adherence barrier survey
The Ask-12 survey is a 12-item, self-administered questionnaire designed to assess behavior and barriers associated with medication adherence (Table S1).Citation24 The Ask-12 survey consisted of 12 items in three subscales, including inconvenient/forgetfulness, health beliefs, and behavior items, for adherence barriers assessment. Items 1 to 7, which assess barriers to treatment adherence, were rated with the following five response options: strongly agree, agree, neutral, disagree, and strongly disagree. Items 8 to 12 assessed adherence behavior. For all items, except items 4 to 7, higher scores suggested greater problems with adherence. Items 4 to 7 were reverse scored so that their final recoded scores were in the same direction, with higher scores representing stronger barriers to adherence. The Ask-12 total score range was 12 to 60 points, with higher scores representing greater barriers to adherence. In this study, patients with good adherence were defined as 1 point (strongly disagree) or 2 points (disagree), while patients with poor adherence were done as 4 points (agree) or 5 points (strongly agree) on item 1, “I just forget to take my medicines some of the time.” at week 8. We assessed all outcomes in the patients with good adherence between FF/VI DPI and BUD/FM DPI groups.
Statistical analysis
The target sample size was 22 patients in each group, which provided 80% power at a two-sided α level of 5% to detect a difference of 90 mL or over in FEV1, assuming a standard deviation (SD) of 40 mL in both groups, and the non-inferiority margin was 0.2 L. Data are shown as the mean ± SD. The treatment difference of change in FEV1 as a primary endpoint between FF/VI DPI and BUD/FM DPI groups was analyzed by Welch’s t-test. We analyzed the incidence of asthma exacerbation, ACT scores, and Ask-12 scores and compared these between the FF/VI DPI and BUD/FM DPI groups with Pearson’s chi-squared test or Wilcoxon rank sum test. We compared between the baseline and post-treatment values in each inhalation device by paired T-test, and assessed the difference between both treatment groups by multivariate analysis of variance (MANOVA). All statistical analyses were performed with JMP® 13.2.0 (SAS Institute Inc., Cary, NC, USA). A p-value of <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 23 patients were initially enrolled in this study; however, one patient who dislocated her temporomandibular joint during the study had to be excluded. Patient characteristics are described in . Briefly, the mean age was 62.0 years and 63.6% of patients were female. The mean body mass index (BMI) was 23.9 kg/m2. Fifteen patients had never smoked and seven were former smokers. The mean duration of treatment with BUD/FM DPI for asthma was 17.5 months. Eight patients had already been treated with LTRA. No patient received tiotropium or theophylline as a controller, while five patients had undergone antihistamines therapy (). Three patients experienced asthma exacerbation during this study (). All of the asthma exacerbation cases were unexpected visit to the hospital and systemic corticosteroid administration for more than 3 days. The incidence of exacerbation was not significantly different between both groups (FF/VI 9.1% vs BUD/FM 4.6%; p=0.5498).
Table 1 Patient characteristics
Table 2 Patient treatment at the registration
Table 3 Incidence of asthma exacerbation
Changes in pulmonary function, asthma control, and fractional exhaled nitric oxide (FeNO)
There were no significant differences in pulmonary function parameters, ACQ5 scores, ACT scores, and FeNO between baseline and after week 8 of treatment in each treatment group (). In comparison between FF/VI DPI and BUD/FM DPI treatment groups, the FF/VI DPI treatment group showed a similar magnitude of change in FEV1 between baseline and week 8 as the BUD/FM DPI treatment group (FF/VI 2.15±0.54 to 2.08±0.54 L vs BUD/FM 2.07±0.53 to 2.10±0.51 L; p=0.203). The treatment difference of change volume in FEV1 in FF/VI DPI treatment was −53 mL (95% CI, 29 mL to −136 mL, p=0.200) within non-inferiority margin of BUD/FM DPI group. In addition, we evaluated changes in other pulmonary function parameters in the FF/VI DPI treatment group and noted that they were not different to those in the BUD/FM DPI treatment group. There were no significant changes in ACQ5 scores (FF/VI 0.29±0.41 to 0.39±0.54 vs BUD/FM 0.35±0.42 to 0.39±0.51; p=0.4024), ACT scores (FF/VI 23.8±1.83 to 23.5±1.96 vs BUD/FM 23.3±2.10 to 23.6±2.21; p=0.2185), and FeNO (FF/VI 26.1±19.5 to 24.3±19.6 ppb vs BUD/FM 23.5±17.4 to 25.7±17.7 ppb; p=0.2530) between both treatment groups.
Table 4 Change in parameters from baseline to after 8 weeks of treatment
Adherence assessment using the Ask-12 survey
We assessed behavior and barriers related to inhaler device adherence for asthma maintenance treatment using the Ask-12 survey (). The Ask-12 total score in the FF/VI DPI group was significantly lower than that in the BUD/FM DPI group (FF/VI 19.3±5.71 vs BUD/FM 24.1±8.60; p=0.0366). In subscale analysis, health beliefs and behavior scores were not significantly different between both groups; on the other hand, the inconvenience and forgetfulness score in the FF/VI DPI group was significantly lower than that in the BUD/FM DPI group (FF/VI 5.40±2.93 vs BUD/FM 7.05±2.69; p=0.0425). The results indicate that FF/VI DPI treatment had significantly less inconvenience and forgetfulness associated with the therapy as well as better adherence barriers compared to BUD/FM DPI treatment.
Table 5 Scoring of Ask-12 adherence barrier survey
Discussion
This study showed that in patients with stable asthma controlled with ICS/LABA, the clinical effect of once-daily FF/VI DPI treatment was not inferior to that of twice-daily BUD/FM DPI therapy. In addition, FF/VI DPI significantly reduced inconvenience and forgetfulness scores in Ask-12 survey and may improve inhaler device adherence barriers compared with BUD/FM DPI. Recent studies have reported that FF/VI DPI had better clinical efficacy in improving asthma symptoms, pulmonary function, and health-related quality of life, and in reducing asthma exacerbation compared to placebo or other optimized usual care.Citation10–Citation15 However, the patients analyzed in these studies had uncontrolled asthma. Additionally, there are few studies that assess inhaler device adherence barriers for maintenance treatment in controlled asthma patients. Consequently, we investigated the clinical effects and inhalation adherence barriers of once-daily FF/VI DPI compared with twice-daily BUD/FM DPI in patients with controlled stable asthma on ICS/LABA therapy in a randomized crossover study.
Fluticasone furoate/Vilanterol is an ICS/LABA combination therapy with inherent 24 hrs activity, currently used as a once-daily treatment device. Fluticasone furoate has been shown to have stronger affinity for the GC receptor and longer activation in respiratory cells compared with other GCs.Citation1 In particular, the drug was several times more potent than BUD in inhibiting inflammatory cytokine production in respiratory.Citation1 Furthermore, inhaled FF demonstrated prolonged absorption from lung into the systemic circulation compared to inhaled FP.Citation2 Actually, some clinical studies have reported that FF DPI improved peak expiratory flow, pre-dose evening FEV1, and treatment effect on rescue/symptom-free compared to placebo or other ICS in patients with asthma.Citation3–Citation6 Additionally, Vilanterol is a once-daily inhaled LABA shown to induce prolonged bronchodilation for at least 24 hrs. VI has a stronger affinity for β2 adrenergic receptor than FM, and is faster and longer acting than SLM.Citation25 Accordingly, FF/VI DPI (100/25 μg) 1 puff once-daily has been expected to have a clinical effect comparable to BUD/FM DPI (160/4.5 μg) 2 puffs twice-daily for inhaled asthma treatment. In this study, we found that there were no differences in incidence of asthma exacerbation, pulmonary function parameters, and symptom scores between FF/VI DPI (100/25 μg) 1 puff once-daily and BUD/FM DPI (160/4.5 μg) 2 puffs twice-daily. We suggest FF/VI DPI once-daily therapy as an alternative control in patients with stable asthma controlled on BUD/FM DPI twice-daily.
The effectiveness of inhaled therapy for asthma is strongly influenced by the adherence and inhaler technique of these inhalations, as poor inhaler adherence and technique error have led to poor asthma control.Citation9,Citation26,Citation27 Recently, comparative clinical studies have reported on errors in handling and wrong technique use for various inhaler devices.Citation7–Citation9 On the other hand, patient adherence has been recently assessed using some different subjective scales, such as the Morisky medication adherence scale (MMAS),Citation28 the medication adherence rating scale (MARS),Citation29 and the “Adherence starts with knowledge 20” (Ask-20) questionnaire.Citation30,Citation31 Clinical studies using the Ask-20 questionnaire have recently reported correlations between adherence and adherence barriers to inhaled treatment in patients with asthma.Citation32,Citation33 The Ask-20 total score discriminated between those patients with good and poor medication adherence as patients with poor adherence to inhaled medicines had significantly higher total Ask-20 scores.Citation32,Citation33 However, the questionnaire is comprised of twenty items and a specific part of the questionnaire does not address inhalation technique or education.Citation33 Therefore, the Ask-20 questionnaire as adherence barriers assessment tool is not widely used in the inhaled medication clinical field.Citation30 In this study, we performed the Ask-12 survey, which is modified from the Ask-20 survey, and can be used in daily medical practice.Citation24,Citation34 Previous studies reported that the Ask-12 total score correlated with pharmacy-refill ratesCitation24,Citation34 and that the optimal cut-off value of the total score was 23 points to discriminate poor adherence with inhalation treatment.Citation34 We found that the Ask-12 total score associated with the once-daily FF/VI DPI device was significantly lower than that of the twice-daily BUD/FM DPI, and that the asthma patients who used the once-daily inhaler had a reduced adherence barrier related to inconvenience and forgetfulness than those using the twice-daily device. An additional reason for this improvement is likely that the FF/VI DPI device (Ellipta) was easy to use, had fewer steps, shorter instructions, and a more intuitive design.Citation7 Recent studies have shown that the Ellipta device caused less errors in inhaler treatment compared to other inhaler devices,Citation7 and asthma patients were able to learn the correct use of the device after being instructed only three times.Citation8 In this assessment of the Ask-12 survey, we showed that the inconvenience and forgetfulness scores of the Ellipta, a simple and once-daily device with low error rates, were significantly decreased when compared to that of another twice-daily device.
The present study had some limitations. The study involved open-label administration, had a short duration of treatment, and had a relatively small sample size. In particular, open-label prospective study has potential biases and could influence results in some clinical endpoints. Furthermore, we used the subjective measurement of self-reported adherence barriers without the objective measures of adherence such as dose counter or monitoring devices in this study. We think that a much larger and longer study would be required to confirm comparable clinical effectiveness including asthma exacerbation and improving adherence barriers in different inhaled devices for controlled asthma maintenance therapy. However, this study is important in terms of being one of the randomized crossover trials to compare the pulmonary functions and adherence barriers between once-daily and twice-daily inhaled therapies for stable asthma.
Conclusion
This study indicated that the clinical effect of once-daily FF/VI DPI was not inferior to that of twice-daily BUD/FM DPI for asthma maintenance therapy. FF/VI DPI treatment is more likely to improve inconvenience and forgetfulness in inhalation adherence barriers compared with BUD/FM DPI. As such, FF/VI DPI is a useful option for asthma maintenance treatment.
Abbreviations
ACQ5, 5-item version asthma control questionnaire; ACT, asthma control test; Ask-12, adherence barrier questionnaire; BUD, budesonide; COPD, chronic obstructive pulmonary disease; DPI, dry powder inhaler; FeNO, fractional exhaled nitric oxide; FEV1, force expiratory volume in 1 s; FF, fluticasone furoate; FM, formoterol; FP, fluticasone propionate; FVC, forced vital capacity; GC, glucocorticoid; ICS, inhaled corticosteroid; LABA, long-acting β2 adrenergic agonist; LAMA, long-acting muscarinic antagonist; LTRA, leukotriene receptor antagonist; MMF, maximum mid-expiratory flow rate; SABA, short-acting β2 adrenergic agonist; SLM, salmeterol; V25, maximum expiratory flow rate at 25%; V50, maximum expiratory flow rate at 50%; VI, vilanterol.
Consent for publication
All patients provided written informed consent.
Ethics approval and consent to participate
The study protocol was approved by the institutional review board of Hamamatsu University School of Medicine (HUSM 14-146). The trial was registered with the University Hospital Medical Information Network (UMIN) Clinical Trial Registry (UMIN ID 000015609).
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
- Rossios C, To Y, To M, et al. Long-acting fluticasone furoate has a superior pharmacological profile to fluticasone propionate in human respiratory cells. Eur J Pharmacol. 2011;670:244–251. doi:10.1016/j.ejphar.2011.08.02221920359
- Allen A, Bareille PJ, Rousell VM. Fluticasone furoate, a novel inhaled corticosteroid, demonstrates prolonged lung absorption kinetics in man compared with inhaled fluticasone propionate. Clin Pharmacokinet. 2013;52:37–42. doi:10.1007/s40262-012-0021-x23184737
- Busse WW, Bleecker ER, Bateman ED, et al. Fluticasone furoate demonstrates efficacy in patients with asthma symptomatic on medium doses of inhaled corticosteroid therapy: an 8-week, randomised, placebo-controlled trial. Thorax. 2012;67:35–41. doi:10.1136/thoraxjnl-2011-20030821828231
- Bateman ED, Bleecker ER, Lötvall J, et al. Dose effect of once-daily fluticasone furoate in persistent asthma: a randomized trial. Respir Med. 2012;106:642–650. doi:10.1016/j.rmed.2012.01.00422342538
- Lötvall J, Bleecker ER, Busse WW, et al. Efficacy and safety of fluticasone furoate 100 μg once-daily in patients with persistent asthma: a 24-week placebo and active-controlled randomised trial. Respir Med. 2014;108:41–49. doi:10.1016/j.rmed.2013.11.00924295556
- Woodcock A, Bleecker ER, Busse WW, et al. Fluticasone furoate: once-daily evening treatment versus twice-daily treatment in moderate asthma. Resir Res. 2011;12:160. doi:10.1186/1465-9921-12-160
- van der Palen J, Thomas M, Chrystyn H, et al. A randomised open-label cross-over study of inhaler errors, preference and time to achieve correct inhaler use in patients with COPD or asthma: comparison of ELLIPTA with other inhaler devices. NPJ Prim Care Respir Med. 2016;26:16079. doi:10.1038/npjpcrm.2016.7927883002
- Takaku Y, Kurashima K, Ohta C, et al. How many instructions are required to correct inhalation errors in patients with asthma and chronic obstructive pulmonary disease? Respir Med. 2017;123:110–115. doi:10.1016/j.rmed.2016.12.01228137486
- Price DB, Román-Rodríguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5:1071–1081. doi:10.1016/j.jaip.2017.01.00428286157
- Busse WW, O’Byrne PM, Bleecker ER, et al. Safety and tolerability of the novel inhaled corticosteroid fluticasone furoate in combination with the β2 agonist vilanterol administered once daily for 52 weeks in patients ≥12 years old with asthma: a randomised trial. Thorax. 2013;68:513–520. doi:10.1136/thoraxjnl-2012-20260623440247
- Woodcock A, Bleecker ER, Lötvall J, et al. Efficacy and safety of fluticasone furoate/vilanterol compared with fluticasone propionate/salmeterol combination in adult and adolescent patients with persistent asthma: a randomized trial. Chest. 2013;144:1222–1229. doi:10.1378/chest.13-017823846316
- O’Byrne PM, Bleecker ER, Bateman ED, et al. Once-daily fluticasone furoate alone or combined with vilanterol in persistent asthma. Eur Respir J. 2014;43:773–782. doi:10.1183/09031936.0006451324136330
- Bateman ED, O’Byrne PM, Busse WW, et al. Once-daily fluticasone furoate (FF)/vilanterol reduces risk of severe exacerbations in asthma versus FF alone. Thorax. 2014;69:312–319. doi:10.1136/thoraxjnl-2013-20360024253831
- Dwan K, Milan SJ, Bax L, Walters N, Powell C. Vilanterol and fluticasone furoate for asthma. Cochrane Database Syst Rev. 2016;9:CD010758.27582089
- Woodcock A, Vestbo J, Bakerly ND, et al. Salford Lung Study Investigators, effectiveness of fluticasone furoate plus vilanterol on asthma control in clinical practice: an open-label, parallel group, randomised controlled trial. Lancet. 2017;390:2247–2255. doi:10.1016/S0140-6736(17)32397-828903864
- Devillier P, Humbert M, Boye A, et al. Efficacy and safety of once-daily fluticasone furoate/vilanterol (FF/VI) versus twice-daily inhaled corticosteroids/long-acting β2-agonists (ICS/LABA) in patients with uncontrolled asthma: an open-label, randomized, controlled trial. Respir Med. 2018;141:111–120. doi:10.1016/j.rmed.2018.06.00930053956
- Global Initiative for Asthma. Global strategy for asthma management and prevention. [updated 2018]. Available from: https://ginasthma.org. Accessed 329, 2018.
- Standardization of spirometry. American Thoracic Society, 1994 update. Am J Respir Crit Care Med. 1995;152:1107–1136. doi:10.1164/ajrccm.152.3.76637927663792
- Juniper EF, Svensson K, Mörk AC, Ståhl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99:553–558. doi:10.1016/j.rmed.2004.10.00815823451
- Juniper E, Bousquet J, Abetz L, Bateman ED, Committee TGOAL. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the asthma control questionnaire. Respir Med. 2006;100:616–621. doi:10.1016/j.rmed.2005.08.01216226443
- Shirai T, Furuhashi K, Suda T, Chida K. Relationship of the asthma control test with pulmonary function and exhaled nitric oxide. Ann Allergy Asthma Immunol. 2008;101:608–613. doi:10.1016/S1081-1206(10)60223-219119704
- Schatz M, Sorkness CA, Li JT, et al. Asthma control test: reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J Allergy Clin Immunol. 2006;117:549–556. doi:10.1016/j.jaci.2006.01.01116522452
- American Thoracic Society, European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005;171:912–930. doi:10.1164/rccm.200406-710ST15817806
- Matza LS, Park J, Coyne KS, Skinner EP, Malley KG, Wolever RQ. Derivation and validation of the ASK-12 adherence barrier survey. Ann Pharmacother. 2009;43:1621–1630. doi:10.1345/aph.1M17419776298
- Slack RJ, Barrett VJ, Morrison VS, et al. In vitro pharmacological characterization of vilanterol, a novel long-acting β2-adrenoceptor agonist with 24 hr duration of action. J Pharmacol Exp Ther. 2013;344:218–230. doi:10.1124/jpet.112.19848123131596
- Giraud V, Allaert FA, Roche N. Inhaler technique and asthma: feasability and acceptability of training by pharmacists. Respir Med. 2011;105:1815–1822. doi:10.1016/j.rmed.2011.07.00421802271
- Al-Jahdali H, Ahmed A, Al-Harbi A, et al. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin. Immunol. 2013;9:8. doi:10.1186/1710-1492-9-823510684
- Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74. doi:10.1097/00005650-198601000-000073945130
- Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr Res. 2000;42:241–247. doi:10.1016/S0920-9964(99)00130-910785582
- Matza LS, Yu-Isenberg KS, Coyne KS, et al. Further testing of the reliability and validity of the ASK-20 adherence barrier questionnaire in a medical center outpatient population. Curr Med Res Opin. 2008;24:3197–3206. doi:10.1185/0300799080246364218922213
- Hahn SR, Park J, Skinner EP, et al. Development of the ASK-20 adherence barrier survey. Curr Med Res Opin. 2008;24:2127–2138. doi:10.1185/0300799080217476918554431
- Atsuta R, To Y, Sakamoto S, et al. Assessing usability of the “Adherence Starts with Knowledge 20” (ASK-20) questionnaire for Japanese adults with bronchial asthma receiving inhaled corticosteroids long term. Allergol Int. 2017;66:411–417. doi:10.1016/j.alit.2016.09.00127712949
- Toyama T, Kawayama T, Kinoshita T, et al. Differences in adherence barriers to inhaled medicines between Japanese patients with chronic obstructive pulmonary disease and asthma evaluated using the “Adherence Starts with Knowledge 20” (ASK-20) questionnaire. Intern Med. 2019;58:175–185. doi:10.2169/internalmedicine.0488-1730210101
- Takemura M, Nishio M, Fukumitsu K, et al. Optimal cut-off value and clinical usefulness of the Adherence Starts with Knowledge-12 in patients with asthma taking inhaled corticosteroids. J Thorac Dis. 2017;9:2350–2359. doi:10.21037/jtd28932539