
Abstract
Background
Randomized trials evaluating electronic Media (eMedia) delivery of interventions are increasingly frequent in mental health. Although a number of reviews have reported efficacy of these interventions, none has reviewed the type of eMedia interventions and quality of their description. We therefore decided to conduct a survey of eMedia-delivered interventions for schizophrenia.
Methods
We surveyed all relevant trials reliably identified in the Cochrane Schizophrenia Group’s comprehensive register of trials by authors working independently. Data were extracted regarding the size of the trial, interventions, outcomes and how well the intervention was described.
Results
eMedia delivery of interventions is increasingly frequent in trials relevant to the care of people with schizophrenia. The trials varied considerably in sample sizes (mean =123, median =87, range =20–507), and interventions were diverse, rarely evaluating the same approaches and were poorly reported. This makes replication impossible. Outcomes in these studies are limited, have not been noted to be chosen by end users and seem unlikely to be easy to apply in routine care. No study reported on potential adverse effects or cost, end users satisfaction or ease of use. None of the papers mentioned the use of CONSORT eHealth guidelines.
Conclusion
There is a need to improve reporting and testing of psychosocial interventions delivered by eMedia. New trials should comply with CONSORT eHealth guidance on design, conduct and reporting, and existing CONSORT should be updated regularly, as the field is constantly evolving.
Background
The use of technology to advance psychological treatment is a developing professional reality.Citation1 The digital revolution has the potential to transform mental health care by connecting patients, services and health data in new ways.Citation2 There has been extensive research on the use of electronic Media (eMedia) technologies for a variety of emotional and mental health problems. A number of literature reviews of interventions delivered through eMedia have been published. These include reviews of interventions for anxiety disorders in adults,Citation3 behavior problems in children,Citation4 treatment of alcohol-related problemsCitation5 and patient education and support for people with schizophrenia.Citation6
Numerous mobile phone-based telemedicine solutions for remote patient monitoring and disease management in schizophrenia have been tested.Citation7 The eMedia-delivered interventions for this population group range from simple telephone reminders to attend follow-up appointmentsCitation8 to complex medication monitoring systems to improve compliance.Citation9 The virtual reality (VR) programs are being used to teach people various skills, most notably vocational and the social competencies,Citation10,Citation11 but novel approaches have been developed to help people with chronic psychotic symptoms.Citation12
eMedia
eMedia can be defined as the media that use electronics or electromechanical energy for end users (audience) to access content (this is in contrast to static media, mainly print). The eMedia sources most familiar to the general public are video recordings, audio recordings, multimedia presentations, slide presentations, CD-ROM and online content. Most new eMedia are now in a digital Media form (dMedia). Numerous terms are used to describe interventions delivered through dMedia, including mobile health and mobile psychosocial interventions (mPSI) ().
Table 1 Overall classification of media to deliver interventions for mental health
Reviews in this area address the effects of specific forms of eMedia,Citation3,Citation13,Citation14 but we know of no definitive overview of how eMedia has been used and described in a defined group of randomized controlled trials (RCTs). In order to replicate the findings, the interventions should be clearly described. This should involve details of their development and initial testing.Citation15 The CONSORT guidelines recommend that in reporting of an RCT, the authors should describe each intervention thoroughly, including control interventions. The description should allow a clinician to know exactly how to administer the intervention that was evaluated in the trial. If the control group is to receive treatment-as-usual (TAU), it is imperative to describe thoroughly what that constitutes. If the control group or intervention group is to receive a combination of interventions, these should be thoroughly described.Citation16,Citation17
Recently, attempts have been made to modify the CONSORT guidelines.Citation18 However, these are not widely used, even though it has been claimed that implementing these might improve the reporting quality of trials in this area.Citation19 The guidelines need to be continuously updated as our understanding of the issues surrounding eMedia interventions is constantly improving.Citation15,Citation20
By taking an overview of the interventions in a specific area it may be possible to highlight areas that need further development in this new and exciting development in mental health care.
Aims
The aim of this survey was to provide a broad overview of the type of eMedia interventions for all randomized trials relevant to people with schizophrenia. We also wanted to examine whether these interventions are described in details using a criterion (for example, existing CONSORT eHealth checklist). We did not aim to review the effects of these interventions.
Methods
Search methods
Searched source
On January 6, 2015, we searched the Cochrane Schizophrenia Group’s Study-Based Register of Trials and updated this search on October 5, 2015. The Cochrane Schizophrenia Group’s Register of Trials is kept on Microsoft access-based computer program called MeerKat (version 1.6) and is compiled by systematic searches of major national and international resources (including monthly updates of AMED, BIOSIS, CINAHL, EMBASE, MEDLINE, PsycINFO, PubMed and registries of clinical trials) and their monthly updates, hand-searches, gray literature and conference proceedings (for detailed description of the register see Group’s Module). There is no language, date, document type or publication status limitations for the inclusion of records into this register.
Search strategy
We used the following search strategy, which has been developed based on literature review and consulting with the authors of the review:
(*Computer* OR *Internet* OR *Electronic* OR *Media* OR *Phone*) in Intervention Field of STUDY (418 results).
In such a study-based register, searching the major concept retrieves all the synonym keywords and relevant studies because all the studies have already been organized based on their interventions and linked to the relevant topics ( describes detailed keywords).
Inclusion criteria
We included published randomized or quasi-RCTs using any eMedia relevant to people with schizophrenia or schizophrenia-like illnesses with at least one outcome relevant to that same group of people. We also included studies that used social media or the Internet for patient or caregiver education. There was no requirement for papers to report any particular outcome measure or length of follow-up.
By eMedia, we meant media that use electronics or electromechanical energy for end users (audience) to access content (for example, interventions delivered through [but not limited to] mobile phones, tablets, computers, TV or radio). Initially, we wanted to classify interventions according to the type of media and type of e-platform being used, based on information technology (IT) system. IT experts advised that the interventions could be classified based on the extension and file type. However, it might be too complicated for health professionals (). On detailed examination of studies, however, we found that only limited information was available in the majority of studies on these aspects of intervention, and it was impossible to classify on this basis. In any event, this was also not clinically relevant and we, therefore, decided to classify studies according to the type of intervention.
Table 2 Types of digital media
Initial search returned 296 abstracts. Of these, 96 were considered irrelevant. All the abstracts were carefully inspected. Full paper was obtained for clarification if warranted. Given the lack of consensus criteria for eMedia, we adopted a broad definition whereby a paper was included if the intervention was deemed to be delivered by an electronic medium by the trialist. We also included papers in which the trialists did not explicitly mention the intervention, but there was evidence that some electronic medium was employed. Multiple reports of single trials were grouped to avoid double counting. Two authors (FN and SX) held numerous discussions to clarify selection, issues around media categories, suitability and classification of studies into groups. The selected trials were then grouped by type of intervention, and the data on the description of the intervention and size of the trial were independently extracted (FN, SX and TM). SF was consulted when there was a disagreement and to clarify issues. We worked with a team of IT specialists to clarify issues around the classification of eMedia types. One author (SX) has qualifications in IT and medicine. Data were entered into an electronic database. In addition, we also inspected published meta-analyses and relevant Cochrane reviews. After excluding duplicates, and studies not concerning a therapeutic intervention or assessment, we finally selected 61 studies.
Results
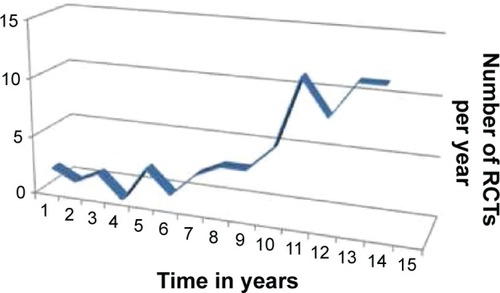
The 61 studies involved 5,352 people with schizophrenia (mean =123, median =87, range =20–507). Studies of this type are of increasing in frequency ().
Figure 1 Number of RCTs over the years (2001–2014).
These trials used a variety of eMedia (eg, mobile/static telephone – calls/messaging/applications [apps], computer software, web pages) and reported outcomes such as adherence, assessment of symptoms, patient education, symptom improvements and compliance ().
Table 3 Summary of randomised trials of eMedia interventions for schizophrenia
We classified the interventions according to the target areas into the following types:
Education and information
Assessment, screening and monitoring
Improved communications
Relapse management/engagement
Specialized interventions
Eleven trials reported testing of eMedia-delivered education/information or training (mean =124, median =91, range =25–311): four on assessment, screening or symptom monitoring (mean =100, median =90, range =24–225), another four on communication improvement (mean =221, median =165, range =50–507) and six on relapse management and engagement (mean =135, median =124, range =47–254). However, the largest number of trials (37) focused on testing of provision of specialized interventions. These included cognitive remediation (CR) (34 RCTs, N=1,833), problem solving (one RCT, N=20) and a novel cognitive behaviour therapy [CBT]-based Avatar therapy (one RCT, N=26).
TAU was the most common control group. Only a small number of studies compared the intervention with an active control (eg, an educational training video compared with a non-educational control video) or with a real-life intervention (eg, VR job skills training compared with the therapist-delivered group). Only two studies compared the same intervention delivered through a different eMedia (eg, SMS-delivered problem solving compared with telephone-delivered problem solving). None of the trials surveyed in this study mentioned the use of CONSORT-eHEALTH checklist. These papers did not describe the interventions in details using an existing criterion. Although a significant minority of studies reported feasibility of the interventions (n=12), none reported end user experience. None of the trials reported participants’ level of digital literacy.Citation20
Discussion
Nearly half (n=35) of the studies reported the use of computer programs for CR. Trials of eMedia-delivered interventions are increasing in frequency. Studies that may have seemed unusual a decade ago are now much more common.
Most studies are small (please note the lower end of the range of numbers in “Results” section). We recognize that many were undertaken by researchers working on very low budgets, and power calculations may have been uninformative when there is little to base them on. Now this does not apply. There are studies albeit small. More informative power calculations are possible, and we suggest that these should be for outcomes that end users designate as important. Even if studies of the exact eMedia do not exist, those proposing to undertake such trials should be able to extrapolate from other good evidence – even if the original intervention was not delivered by eMedia.
To our knowledge, this is the first literature survey reporting an overview of eMedia-delivered interventions for schizophrenia. Previous literature reviews have focused mainly on the outcome of interventions.Citation3–Citation6,Citation13,Citation21 The eMedia interventions, like any other health care intervention, should be clearly described so that results can be replicated.Citation15
Types of eMedia
There was a wide variation in the eMedia used. It varied from television (TV), radio, telephone and desktop computer to game console, smartphones and handheld device. It is not possible to classify eMedia due to the variety of file formats. On the basis of this survey, currently there are two types of media used:
Interactive media (eg, mobile phone apps or websites)
Didactic media (TV, video, etc.)
The survey also highlighted the following types of interventions that are delivered by eMedia;
Type 1: Intervention delivered by a human therapist through a mobile app or a computer program (eg, telephone-delivered problem solving by a therapist, Avatar therapy).
Type 2: Intervention based on a manualized, well-established therapy delivered through eMedia (eg, MoodGym).
Type 3: Intervention that did not exist before and is not underpinned by an existing theoretical framework.
Standardizing, regulating, guiding regarding the intervention
There is an interest in standardizing interventions in this area and have been attempts to establish criteria to self-certify mobile app development.Citation22 This followed concerns about the lack of standardization and risk assessment of medical apps.Citation23,Citation24
The health regulatory agencies have not paid sufficient attention to eMedia-delivered interventions, and therefore limited information and guidance are available for clinicians or end users. The US Food and Drug Administration (FDA) released guidance recently, focusing primarily on apps that transform the mobile platform into a regulated medical device.Citation25 The remaining eMedia will be subject to “enforcement discretion”, that is, no regulation.Citation26 The Therapeutic Goods Administration for health care practitioners in Australia provides limited guidance.Citation27 Similarly, the British Medicines and Healthcare Products Regulatory Agency does not offer concrete advice for clinicians or end users. However, the Business Standards Institution has developed “PAS 277 Health and wellness apps – Quality criteria across the life cycle – Code of practice”Citation28 in conjunction with Innovate UK (www.innovateuk.gov.uk). The purpose of these guidelines is to develop a set of principles that health app developers should follow to ensure that their products and services can be trusted by health care professionals and the public. This is an important starting point. However, with the slow recognition, acceptance and standardization of health apps and the fast pace of development, it seems unlikely that standards and regulation will keep up with technological advancement.Citation29 No trial reported ease (or difficulty) of access and use of the eMedia under test.
None of the studies in this survey followed a set of guidelines for quality control.Citation27 Having read these studies in detail, we remain unclear about the fidelity of most interventions. A small number of studies describe the evidence relating to the manualized intervention, which is, in their trial, delivered through an eMedia (for example, CR trials). A few studies gave details of the eMedia developers, and an even smaller number gave details of the intervention in the public arena (for example, https://www.itareps.com). While some of these interventions might be ready to be used in clinical practice (eg, ClinTouch), others may well be impractical (eg, Avatar therapy) due to cost, training or ease/difficulty of use.
These relatively new interventions present trialists with a dilemma of what to use as a comparison. TAU can be problematic,Citation30 and most studies using a TAU comparison failed to describe adequately what exactly was “usual”. A small number of trials employed innovative control groups such as an active control using a similar eMedia, a real-life intervention or a different eMedia used to deliver the same intervention.
Reporting and outcomes
Use of technical (IT) jargon may not make sense to many health professionals. This could easily be overcome by providing details of the intervention in an online supplement or website. Some guidance is available in reporting mPSI.Citation15
Outcomes were not clearly of importance to end users. Scale-derived measures (for example, scores on Positive and Negative Syndrome Scale) are important mostly to researchers and are not usual in routine care. While researchers are an important constituency for the trial to serve, they are not the only one. End users might be more interested in an outcome like user experience. It is important that eMedia trials do not lose the opportunity to undertake trials that are likely to make any effective procedure applicable to wide use.Citation29
None of the studies reported on direct or indirect adverse effects or on the cost-effectiveness of these interventions (or just the cost of the intervention). Effective encouragement of taking medications may lead to adverse events. There is evidence that psychosocial interventions also cause adverse outcomes.Citation31 Delivery through eMedia complicates and possibly increases risks. Furthermore, there may be risks particular to eMedia such as reduction in social activities or even addiction to eMedia.Citation23
There seems to be an underlying assumption in developing eMedia-delivered interventions that they are cost-effective compared with human media-delivered treatments. No study reported cost per unit of intervention or cost-effectiveness. The assumption of eMedia being more cost-effective remains an assumption.
Criteria
There is an urgent need to set criteria for standardization of development, evaluation and reporting of eMedia interventions. It is imperative that uniform processes are followed and that criteria for trial reporting are developed in consultation with experts in care, evaluation and IT. Recognizing that such suggestions must evolve with technology, we suggest that the CONSORT statement needs to be constantly updated.
Conclusion
This survey reports numerous areas of weakness in current description of eMedia-delivered interventions for schizophrenia. Most notable issues are descriptions of development and initial testing and reporting of interventions, their theoretical underpinning and their side effects. There is also a need to improve reporting end user experience and adapting interventions to their digital or e-literacy skills. None of the trials reported use of CONSORT eHealth. Updating these guidelines, especially for psychosocial interventions, might be the way forward.
Acknowledgments
We are grateful to the Cochrane Schizophrenia Group for their support.
Supplementary material
Table S1 Detailed keywords
Disclosure
The authors report no conflicts of interest in this work.
References
- BarakAHenLBoniel-NissimMShapiraNA comprehensive review and a meta-analysis of the effectiveness of Internet-based psychotherapeutic interventionsNational Library of Medicine. PubMed Health2008 [cited 2015 Sep 26]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0026877/Accessed May 20, 2016
- HollisCMorrissRMartinJTechnological innovations in mental healthcare: harnessing the digital revolutionBr J Psychiatry2015206426326525833865
- Mayo-WilsonEMontgomeryPMedia-delivered cognitive behavioural therapy and behavioural therapy (self-help) for anxiety disorders in adultsCochrane Database Syst Rev20139CD00533024018460
- MontgomeryPMedia-based behavioural treatments for behavioural problems in childrenCochrane Database Syst Rev20061CD00220616437442
- StallmanHKavanaghDWhiteAInternet interventions for treatment of alcohol-related problemsThe Cochrane Library. Stallman. Wiley Online Library [cited 2015 Sep 26]. Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010228/abstractAccessed May 20, 2016
- VälimäkiMHätönenHLahtiMKuosmanenLAdamsCEInformation and communication technology in patient education and support for people with schizophreniaCochrane Database Syst Rev201210CD00719823076932
- ŠpanielFVohlídkaPKoženýJThe Information Technology Aided Relapse Prevention Programme in Schizophrenia: an extension of a mirror-design follow-upInt J Clin Pract200862121943194618795967
- BurgoyneRWAcostaFXYamamotoJTelephone prompting to increase attendance at a Psychiatric Outpatient ClinicAm J Psychiatry198314033453476829808
- FrangouSSachpazidisIStassinakisASakasGTelemonitoring of medication adherence in patients with schizophreniaTelemed J E Health200511667568316430387
- ParkKMKuJChoiSHA virtual reality application in role-plays of social skills training for schizophrenia: a randomized, controlled trialPsychiatry Res2011189216617221529970
- SmithMJFlemingMFWrightMAVirtual reality job interview training and 6-month employment outcomes for individuals with schizophrenia seeking employmentSchizophr Res20151661–3869126032567
- LeffJWilliamsGHuckvaleMAArbuthnotMLeffAPComputer-assisted therapy for medication-resistant auditory hallucinations: proof-of-concept studyBr J Psychiatry2013202642843323429202
- ClementSLassmanFBarleyEMass media interventions for reducing mental health-related stigmaCochrane Database Syst Rev20137CD00945323881731
- OlthuisJVWattMCStewartSHTherapist-delivered distance cognitive behavioural therapy for anxiety disorders in adultsCochrane Database Syst RevJohn Wiley & Sons, Ltd2011 [cited 2015 Sep 27]. Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009028/abstractAccessed May 20, 2016
- NaeemFSyedYXiangSDevelopment, testing and reporting of mobile apps for psycho-social interventions: lessons from the pharmaceuticalsJ Med Diagn Methods2015 [cited 2016 Jan 18];4(1000191). Available from: http://www.omicsgroup.org/journals/development-testing-and-reporting-of-mobile-apps-for-psychosocialinterventions-lessons-from-the-pharmaceuticals-2168-9784-1000191.php?aid=65355Accessed May 20, 2016
- BoutronIMoherDAltmanDGSchulzKFRavaudPCONSORT GroupExtending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaborationAnn Intern Med2008148429530918283207
- SchulzKFAltmanDGMoherDCONSORT GroupCONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trialsBMC Med2010811820334633
- EysenbachGCONSORT-EHEALTH GroupCONSORT-EHEALTH: improving and standardizing evaluation reports of Web-based and mobile health interventionsJ Med Internet Res2011134e12622209829
- EysenbachGCONSORT-EHEALTH: implementation of a checklist for authors and editors to improve reporting of web-based and mobile randomized controlled trialsStud Health Technol Inform201319265766123920638
- NaeemFGireNXiangSReporting and understanding the safety and adverse effect profile of mobile apps for psychosocial interventions: an updateWorld J Psychiatry20166218719127354959
- KlecunELichtnerVCornfordTe-Literacy in health careStud Health Technol Inform201420584384725160306
- WhiteAKavanaghDStallmanHOnline alcohol interventions: a systematic reviewJ Med Internet Res2010125e6221169175
- LewisTA systematic self-certification model for mobile medical appsJ Med Internet Res2013154e8923615332
- LewisTLWyattJCmHealth and mobile medical apps: a framework to assess risk and promote safer useJ Med Internet Res2014169e21025223398
- FDAMobile medical applications [Internet]2014 [cited 2015 Oct 15]. Available from: http://www.fda.gov/MedicalDevices/DigitalHealth/MobileMedicalApplications/default.htmAccessed May 20, 2016
- McCarthyMFDA will not regulate most mobile medical appsBMJ2013347f584124072875
- TGARegulation of medical software and mobile medical “apps” [Internet]Therapeutic Goods Administration (TGA)2013 [cited 2015 Oct 15]. Available from: https://www.tga.gov.au/regulation-medical-software-and-mobile-medical-appsAccessed May 20, 2016
- BSIPAS 277:2015 Health and wellness apps. Quality criteria across the life cycleCode of practice [Internet]2015 [cited 2015 Oct 15]. Available from: http://shop.bsigroup.com/forms/PASs/PAS-2772015/Accessed May 20, 2016
- VincentCJNiezenGO’KaneAAStawarzKCan standards and regulations keep up with health technology?JMIR MHealth UHealth201532e6426041730
- ThorpeKEZwarensteinMOxmanADA pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial designersJ Clin Epidemiol200962546447519348971
- BerkMParkerGThe elephant on the couch: side effects of psychotherapyAust N Z J Psychiatry200943978779419670051
- RotondiAJHaasGLAndersonCMA Clinical Trial to Test the Feasibility of a Telehealth Psychoeducational Intervention for Persons With Schizophrenia and Their Families: Intervention and 3-Month FindingsRehabil Psychol200550432533626321774
- RotondiAJAndersonCMHaasGLWeb-based Home Delivery of Multi-Family Psychoeducational Therapy to Persons with Schizophrenia and their Family Members: 1-year Outcomes and Cognitive DesignSchizophrenia BulletinOxford Univ PressGreat Clarendon St, Oxford Ox2 6dp, England2011319319
- WirshingDASergiMJMintzJA Videotape Intervention to Enhance the Informed Consent Process for Medical and Psychiatric Treatment ResearchAm J Psychiatry2005162118618815625221
- JonesRBAtkinsonJMCoiaDARandomised trial of personalised computer based information for patients with schizophreniaBMJ2001322729083584011290639
- PitkänenAVälimäkiMKuosmanenLPatient education methods to support quality of life and functional ability among patients with schizophrenia: a randomised clinical trialQual Life Res Int J Qual Life Asp Treat Care Rehabil2012212247256
- KaplanKSolomonPSalzerMSBrusilovskiyEAssessing an Internet-based parenting intervention for mothers with a serious mental illness: A randomized controlled trialPsychiatr Rehabil J201437322223124978623
- ParkK-MKuJChoiS-HA virtual reality application in role-plays of social skills training for schizophrenia: a randomized, controlled trialPsychiatry Res2011189216617221529970
- SmithMJFlemingMFWrightMAVirtual reality job interview training and 6-month employment outcomes for individuals with schizophrenia seeking employmentSchizophr Res20151661–3869126032567
- TsangMMYManDWKA virtual reality-based vocational training system (VRVTS) for people with schizophrenia in vocational rehabilitationSchizophr Res20131441–3516223356951
- TorresAMendezLPMerinoHMoranEAImproving social functioning in schizophrenia by playing the train gamePsychiatr Serv Wash DC2002537799801
- KaplanKSalzerMSSolomonPBrusilovskiyECousounisPInternet peer support for individuals with psychiatric disabilities: A randomized controlled trialSoc Sci Med2011721546221112682
- ChinmanMYoungASSchellTHassellJMintzJComputer-assisted self-assessment in persons with severe mental illnessJ Clin Psychiatry200465101343135115491237
- AnzaiNRehab Rounds: Training Persons With Schizophrenia in Illness Self-Management: A Randomized Controlled Trial in JapanPsychiatr Serv200253554554711986501
- KasckowJZickmundSGurklisJUsing telehealth to augment an intensive case monitoring program in veterans with schizophrenia and suicidal ideation: A pilot trialPsychiatry Res201623911111627137970
- Palmier-ClausJEAinsworthJMachinMThe feasibility and validity of ambulatory self-report of psychotic symptoms using a smartphone software applicationBMC Psychiatry20121217223075387
- van der KriekeLEmerenciaACBoonstraNWunderinkLde JongePSytemaSA Web-Based Tool to Support Shared Decision Making for People With a Psychotic Disorder: Randomized Controlled Trial and Process EvaluationJ Med Internet Res20131510e21624100091
- SteinwachsDMRoterDLSkinnerEAA web-based program to empower patients who have schizophrenia to discuss quality of care with mental health providersPsychiatr Serv Wash DC2011621112961302
- PriebeSMcCabeRBullenkampJStructured patient-clinician communication and 1-year outcome in community mental healthcare: cluster randomised controlled trialBr J Psychiatry J Ment Sci2007191420426
- WoltmannEMWilknissSMTeachoutAMcHugoGJDrakeRETrial of an Electronic Decision Support System to Facilitate Shared Decision Making in Community Mental HealthPsychiatr Serv2011621546021209300
- ZanjaniFMillerBTurianoNRossJOslinDEffectiveness of Telephone-Based Referral Care Management, a Brief Intervention to Improve Psychiatric Treatment EngagementPsychiatr Serv200859777678118586995
- KomatsuHSekineYOkamuraNEffectiveness of Information Technology Aided Relapse Prevention Programme in Schizophrenia excluding the effect of user adherence: a randomized controlled trialSchizophr Res2013150124024423998952
- StipEMVincentPDPGuevremontCMSA randomized controlled trial with a Canadian electronic pill dispenser used to measure and improve medication adherence in patients with schizophreniaPharm Med Outcomes Res20134100
- FrangouSSachpazidisIStassinakisASakasGTelemonitoring of medication adherence in patients with schizophreniaTelemed J E-Health Off J Am Telemed Assoc2005116675683
- VelliganDMintzJMaplesNA randomized trial comparing in person and electronic interventions for improving adherence to oral medications in schizophreniaSchizophr Bull2013395999100723086987
- KauppiKKannistoKAHätönenHMobile phone text message reminders: Measuring preferences of people with antipsychotic medicationSchizophr Res20151681–251452226293215
- BrysonGBellMDInitial and final work performance in schizophrenia: cognitive and symptom predictorsJ Nerv Ment Dis20031912879212586961
- CavallaroRAnselmettiSPolettiSComputer-aided neurocognitive remediation as an enhancing strategy for schizophrenia rehabilitationPsychiatry Res2009169319119619740550
- d’AmatoTBationRCochetAA randomized, controlled trial of computer-assisted cognitive remediation for schizophreniaSchizophr Res20111252–328429021094025
- DangJZhangJGuoZA pilot study of iPad-assisted cognitive training for schizophreniaArch Psychiatr Nurs201428319719924856273
- DickinsonDTenhulaWMorrisSA Randomized, Controlled Trial of Computer-Assisted Cognitive Remediation for SchizophreniaAm J Psychiatry2010167217018020008941
- DrakeRJDayCJPicucciRA naturalistic, randomized, controlled trial combining cognitive remediation with cognitive-behavioural therapy after first-episode non-affective psychosisPsychol Med20144491889189924172842
- GarridoGBarriosMPenadésRComputer-assisted cognitive remediation therapy: Cognition, self-esteem and quality of life in schizophreniaSchizophr Res20131502–356356924035402
- GarridoGBarriosMPenadésRCognition, Self-esteem and Quality of Life in Schizophrenia; A 12 Month Follow-up Cognitive Remediation Clinical TrialSchizophr Res2014153S257S258
- HarrisARogersPMooreGToscanoDRedoblado-HodgeACognitive remediation in first-episode and chronic schizophreniaActa Neuropsychiatr2006186253
- FisherMHollandCMerzenichMMVinogradovSUsing Neuroplasticity-Based Auditory Training to Improve Verbal Memory in SchizophreniaAm J Psychiatry2009166780581119448187
- HolzerLUrbenSPassiniCMA randomized controlled trial of the effectiveness of computer-assisted cognitive remediation (CACR) in adolescents with psychosis or at high risk of psychosisBehav Cogn Psychother201442442143423631951
- HolzerLUrbenSPihetSJaugeyLA randomized controlled trial of the effectiveness of a computer-assisted cognitive remediation (CACR) program in adolescents with psychosis or at high risk of psychosis: Short-term and long-term outcomesNeuropsychiatr Enfance Adolesc2012605S71
- TorrisiRHolzerLPihetSComputer-assisted cognitive remediation program for adolescents at high risk of psychosis or with psychotic disorders: preliminary resultsInt Clin Psychopharmacol201126e85e86
- HookerCBruceLFisherMVeroskySMiyakawaAVinogradovSNeural activity during emotion recognition after combined cognitive plus social cognitive training in schizophreniaSchizophr Res20121391322647883
- HookerCIBruceLFisherMVeroskySCMiyakawaAVinogradovSNeural activity during emotion recognition after combined cognitive plus social cognitive training in schizophreniaSchizophr Res20121391535922695257
- HoranWPKernRSTrippCEfficacy and specificity of Social Cognitive Skills Training for outpatients with psychotic disordersJ Psychiatr Res20114581113112221377168
- JaugeyLShort-and Long-Term Outcomes of a Randomized Controlled Trial of a Computer-Assisted Cognitive Remediation (CACR) Program in Adolescents with Psychosis or at High Risk of PsychosisBiol Psychiatry201271884s84s
- LeeWKEffectiveness of computerized cognitive rehabilitation training on symptomatological, neuropsychological and work function in patients with schizophreniaAsia-Pac Psychiatry20135290100
- KeefeRSEVinogradovSMedaliaAFeasibility and Pilot Efficacy Results From the Multisite Cognitive Remediation in the Schizophrenia Trials Network (CRSTN) Randomized Controlled TrialJ Clin Psychiatry20127371016102222687548
- BucciPPiegariGMucciANeurocognitive individualized training versus social skills individualized training: A randomized trial in patients with schizophreniaSchizophr Res20131501697523962828
- PiskulicDBarbatoMLiuLAddingtonJPilot study of cognitive remediation therapy on cognition in young people at clinical high risk of psychosisPsychiatry Res20152251–2939825467705
- PiskulicDBarbatoMAddingtonJEffects of Cognitive Remediation on Cognition in Young People at Clinical High Risk of PsychosisSchizophrneia Res153S128
- PolettiSAnselmettiSBechiMComputer-aided neurocognitive remediation in schizophrenia: durability of rehabilitation outcomes in a follow-up studyNeuropsychol Rehabil201020565967420661811
- RassOForsythJKBolbeckerARComputer-assisted cognitive remediation for schizophrenia: A randomized single-blind pilot studySchizophr Res20121391–3929822682988
- StürzKHartmannSEder-PelzerBGüntherVComputer assisted cognitive training advances mood and psychological wellbeing – a comparison to paper pencil training relating to neuropsychological parameters, mood and cognitionsResearchGate20112528592
- VesteragerLChristensenTØOlsenBBCognitive training plus a comprehensive psychosocial programme (OPUS) versus the comprehensive psychosocial programme alone for patients with first-episode schizophrenia (the NEUROCOM trial): A study protocol for a centrally randomised, observer-blinded multi-centre clinical trialTrials [Internet]201112 [cited 2016 Aug 15];12(1). Available from: http://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-12-35
- VitaADe PeriLBarlatiSEffectiveness of different modalities of cognitive remediation on symptomatological, neuropsychological, and functional outcome domains in schizophrenia: A prospective study in a real-world settingSchizophr Res20111331–322323121907544
- AhmedAOHunterKMGoodrumNMA randomized study of cognitive remediation for forensic and mental health patients with schizophreniaJ Psychiatr Res20156881826228394
- BellMBrysonGGreigTCorcoranCWexlerBENeurocognitive enhancement therapy with work therapy: effects on neuropsychological test performanceArch Gen Psychiatry200158876376811483142
- McGurkSRMueserKTFeldmanKWolfeRPascarisACognitive Training for Supported Employment: 2–3 Year Outcomes of a Randomized Controlled TrialAm J Psychiatry2007164343744117329468
- McGurkSRMueserKTPascarisACognitive training and supported employment for persons with severe mental illness: one-year results from a randomized controlled trialSchizophr Bull200531489890916079391
- GrynszpanOPerbalSPelissoloAEfficacy and specificity of computer-assisted cognitive remediation in schizophrenia: a meta-analytical studyPsychol Med201141116317320380784
- LecardeurLStipEGiguereMBlouinGRodriguezJ-PChampagne-LavauMEffects of cognitive remediation therapies on psychotic symptoms and cognitive complaints in patients with schizophrenia and related disorders: a randomized studySchizophr Res20091111–315315819395240
- HermanutzMGestrichJComputer-assisted attention training in schizophrenics. A comparative studyEur Arch Psychiatry Clin Neurosci19912404–52822871829004
- BeebeLSmithKDPhillipsCA Comparison of Telephone and Texting Interventions for Persons with Schizophrenia Spectrum DisordersIssues Ment Health Nurs201435532332924766166
- LeffJWilliamsGHuckvaleMAArbuthnotMLeffAPComputer-assisted therapy for medication-resistant auditory hallucinations: proof-of-concept studyBr J Psychiatry2013202642843323429202