
Abstract
Social anxiety disorder is a common condition often associated with severe impairment in educational career. The aim of this paper was to evaluate prevalence rates and correlates of mild, moderate, and severe forms of social anxiety spectrum in a large sample of university students. Overall, 717 university students were assessed with the Social Anxiety Spectrum Self-Report questionnaire. Using two cut-off scores, 61.4% of subjects were classified as low scorers, 10% as medium scorers, and 28.6% as high scorers. Both high and medium scorers reported fears related to social situations. Interpersonal sensitivity and specific phobias were more common among women with low scores. Childhood/adolescence social anxiety features were more common among males with medium scores. Behavioral inhibition was more common among males with high scores. Functional impairment was severe among high scorers and, to a lesser extent, among medium scorers. Social anxiety spectrum is largely represented among university students. Future studies should investigate whether sufferers of social phobia underachieve or end their professional objectives prematurely.
Introduction
Social anxiety disorder (SAD) is a frequent and impairing condition rather neglected in clinical settings but of great interest to researchers. According to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV TR) criteria, lifetime prevalence of SAD in the general population has been reported to range from 1.9% to 13.7%.Citation1 Social anxiety symptoms have an early onset and, in student populations, a tendency to persist throughout the entire school career.Citation2 Several studies have reported that social anxiety can have significant effects in terms of failure to complete school, increased risk of exam failure,Citation3 and failure to graduate.Citation4,Citation5 Clinically significant levels of social anxiety in 10%–16% of students at higher education in the UK and Sweden, respectively, have been documented.Citation6,Citation7 One of the issues at the center of investigation is the definition of a diagnostic threshold of SAD. Davidson et alCitation8 argued that social anxiety might be better described on a continuum of severity rather than a discrete disorder based on an arbitrarily derived threshold. Other epidemiological studiesCitation9,Citation10 support the hypothesis that boundaries of SAD should be determined by its severity rather than by qualitative distinctions.Citation11
In the fifth edition of the DSM,Citation12 some changes reflect a new and broader understanding of the condition in a variety of social situations. In the past, the diagnosis of SAD was primarily characterized by the presence of extreme discomfort or fear when performing in front of other individuals. However, data from research demonstrated that this definition was too narrow. In the DSM-V, SAD can be diagnosed by an individual’s abnormal response in a large array of social situations. For example, the person may be so uncomfortable carrying on a conversation that he/she is unable to talk to others, particularly to strangers or unfamiliar individuals. A person who is concerned over being observed may be unable to go out to dinner because he/she fears being watched while she is eating and drinking. The changes between DSM-IV and DSM-V in the diagnosis of SAD prompts a re-consideration of distribution of symptoms in non-clinical populations, such as university students, for two reasons: 1) the enlargement of the variety of situations in which a person may experience social anxiety symptoms, with the abolition of generalized versus specific forms; and 2) the deletion of the requirement that individuals aged over 18 years recognize that their anxiety is excessive or unreasonable. Instead, the anxiety must be out of proportion to the actual danger or threat in the situation. Therefore, this second requirement has been set to include individuals who judge as normal their reaction in certain situations due to their firm belief in having constitutional shyness or because of a lack of complete awareness of their symptoms. Within this context, the ‘Structured Clinical Interview for the Assessment of Social Anxiety Spectrum’ (SCI-SHY) and the corresponding self-report questionnaire (SHY-SR) appears to be an ideal instrument to explore the entire range of social anxiety symptoms.Citation13 These instruments are based on a conceptualization of the social anxiety spectrum as a condition that spans from simple shyness to severe SAD, including full-blown and typical as well as subclinical and atypical presentations, isolated signs and symptoms, and/or avoidant personality traits. The SCI-SHY and SHY-SR proved to have excellent psychometric properties.Citation13–Citation15
Previously, an epidemiological study was undertaken by our group with the aim to explore differences between the sexes in distribution of social anxiety symptoms among high-school students and to analyze the correlation between these symptoms and mood, anxiety, and eating behavior spectrum symptomatology.Citation15 The results showed that females had more severe social anxiety symptoms than males, and were more frequently associated with depression, obsessive-compulsive symptoms, as well as panic and eating disorder symptoms. In subsequent analyses of this sample, individuals were classified as low scorers, medium scorers, and high scorers according to the SHY-SR. Fears related to social situations, functional impairment defined by avoidance, and school difficulties were reported by both high and medium scorers.Citation16
In this study, we aimed to investigate prevalence rates of mild, moderate, or severe symptoms of social anxiety in a large sample of university students and to evaluate the level of impairment in these individuals. In addition, we also explored differences between the sexes on distribution of social anxiety symptoms. More specifically, our hypothesis was that the female/male ratio was increased in severe forms of social anxiety, as previously found by Merikangas et alCitation17 and that functional impairment was associated with both moderate and severe social anxiety spectrum.
Methods
The survey was conducted upon agreement with University of Pisa. In order to maximize the diversity of subjects, an e-mail was sent from the Student’s Office address to all students enrolled in the following four laurea degree courses: social sciences, scientific sciences, humanistics, and medicine. The email provided full information about the nature of the survey. In particular, it stated clearly that the aim of the survey was to investigate the frequency of a large array of social anxiety symptoms among university students. The email gave eligible participants secure one-time access to an online anonymous form of the SHY-SR. Volunteers did not receive any kind of payment or complimentary gifts for participating in the survey. An appropriate self-report form was used to collect socio-demographic variables. Contextually, the same email provided students with a telephone number of a ‘Listening Center’ managed by two psychologists (EM, FG) of the University of Pisa, in case some students needed personal contact with a health care professional for additional questions or information. Informed consent was also obtained via email from each student. All data were retrieved in a database for statistical analyses. Data were collected from May to July 2013.
Instruments
The SHY-SR is an instrument designed to explore the lifetime spectrum of social anxiety with established psychometric properties. Properties of this questionnaire are described in more detail elsewhere.Citation13,Citation14,Citation16 It consists of 168 items grouped into the following domains: ‘childhood and adolescence social anxiety features’ (CA), ‘interpersonal sensitivity’ (IPS), ‘behavioral inhibition and somatic symptoms’ (BI), and ‘specific phobias’ (SP). The questionnaire also includes an appendix on substance abuse that is frequently associated with social anxiety.Citation18 The SHY-SR was derived from the SCI-SHY by modifying the format and the instructions to make the instrument suitable for self-administration. The SHY-SR comprises dichotomous (yes/no) items; thus, the total score and the domain scores are obtained by counting the number of items endorsed. The instrument is designed for administration to adults because it includes social and work situations that are rarely experienced by younger people. The SHY-SR was created by capitalizing on the long-standing clinical experience of Italian and American psychiatrists and psychologists, including one of the authors (LD), who met periodically to select a pool of items, discuss their face validity, and arrange the sequence of items according to relevant ‘domains’ defined a priori. The spectrum interviews and self-report questionnaires (different instruments were created for specific disorders) document the presence/absence of features, in dichotomous form, organized into domains. Domain scores are obtained by counting the number of items endorsed.Citation13,Citation14
Regarding psychometric properties, validity studies have shown that the SHY-SR questionnaire is a reliable and valid measure of social anxiety phenomenology.Citation13
Internal consistency of the SHY-SR domains was satisfactory. Kuder–Richardson coefficients were well above 0.80 for the SHY-SR, and also showed a homogeneous internal structure in terms of correlation between subscales (>0.60), and when correlations between the domains and the corresponding total score were examined (>0.70).
Thresholds for SHY-SR low, medium, and high scorers
In a previous study, we determined two cut-offs for the SHY-SR total score via receiver operating characteristic (ROC) curve analysis.Citation16 We adopted these same two cut-offs in this study in order to characterize individuals with low, medium, and high levels of social anxiety. A diagnostic threshold of 68 was determined by balancing sensitivity (84.8%) and specificity (85.6%) with respect to DSM-IV diagnosis of SAD. In addition, a second threshold of 59 was obtained by maximizing sensitivity (87%), while keeping specificity at a high level (80.8%). This was done with the aim of identifying individuals who reported high scores on the social anxiety spectrum but did not meet the diagnostic criteria for the SAD. Applying these two cut-off scores to the present study sample, we classified our university students into three groups: low scorers (<59 items endorsed), medium scorers (59–67 items), and high scorers (≥68 items).
In a previous study,Citation16 by using the three cut-off scores described above, about 73% of subjects were classified as low scorers, 9% as medium scorers, and 17.7% as high scorers. Statistical analyses indicated that the mean scores on each of the four SHY-SR domains increased significantly across the three groups. Therefore, although we did not adopt a purely dimensional approach, individuals were classified by these thresholds (low, medium, high) on the basis of scores laid on a continuum. This approach allowed comparisons among groups of individuals with different levels of severity of social anxiety symptoms.
Statistical analyses
Mean domain scores were compared between sexes via the independent t-test and across groups via the one-way analysis of variance (ANOVA). Categorical data (frequency of endorsement of individual items) were compared between males and females and across the three groups via the chi-squared (χ2) test. Post hoc pairwise comparisons between low, medium, and high scorers were performed via Sheffe’s pairwise comparisons and applying Bonferroni’s correction to the alpha level (0.05/3=0.016).
Results
Overall, 717 students filled out the SHY-SR and provided additional information requested by email. They were aged 18–28 years (mean age 21.12±1.77). Of these, 440 (61.4%) were females and 277 (38.6%) were males. The distribution of the sexes with respect to all students contacted by email was 3.07% for males and 4.8% for females. Using the cut-off scores described above, 61.4% of subjects were classified as low scorers, 10% as medium scorers and 28.6% as high scorers.
One-way ANOVA, followed by post hoc comparisons, indicated that the mean scores on each of the four SHY-SR domains increased significantly across the three groups ().
Table 1 SHY-SR domains score: comparisons among low, medium, and high scorers
The sex distribution differed significantly among the three categories: women were significantly more likely to be high scorers (31.6% vs 23.8%) and less likely to be low scorers (57.5% females and 67.5% males), while the distribution in the medium scorers group was similar (10.0% males and 8.7% females).
In order to analyze, in more detail, which domains accounted for these differences between the sexes, we compared the SHY-SR symptom profile of males and females across the three groups (). Among low scorers, females reported higher levels of ‘interpersonal sensitivity’ (t=2.11, df=438, P=0.035) and ‘specific phobias’ (t=4.81, df=438, P<0.001) than males. Among intermediate scorers, males reported higher levels of ‘childhood and adolescence social features’ (t= −2.13, df=70, P=0.037); while, in high scorers, males reported higher levels of ‘behavioral inhibition’ and ‘somatic symptoms’ (t= −3.46, df=203, P=0.001).
Table 2 SHY-SR domains scores: sex comparisons in low, medium, and high scorers
In the whole sample, the rate of endorsement was above 60% for 12 items. The two most common fears relative to social situations and performances experienced in the overall sample were “Have you often felt more comfortable in small groups?” and “Have you often felt embarrassed or uncomfortable when you had to express romantic feelings to someone you liked?”.
As shown in , frequency of social fears varied across the three levels of severity on the social anxiety spectrum. Both medium and high scorers had a significantly higher frequency of endorsement than low scorers.
Table 3 Most common social situations and performances feared in the total sample and in the three severity groups
To investigate functional impairment associated with social anxiety symptoms, we selected the SHY-SR items exploring ‘school impairment’ and ‘avoidant behavior’. The two questions exploring school impairment are item #5: “When you were a child or an adolescent, do you remember (or have you ever been told) that you did poorly at school because of shyness?” and item #112: “Did you ever drop out of school or interrupt your education, for these reasons?” Positive answers to item 5 were given by 1.8% of low scorers, 4.2% of medium scorers, and 12.7% of high scorers (χ2=30.56, df=2, P<0.001); for item #112, the percentages were, respectively, 2.3% of low scorers, 4.2% of medium scorers, and 16.1% of high scorers (χ2=40.33, df=2, P<0.001). Eighteen questions explored the avoidant behavior. High scorers most frequently endorsed all of these items, but a large percentage of medium scorers reported avoiding a variety of situations (see ).
Figure 1 Percentage of endorsement of the SHY-SR items related to avoidant behavior, arranged by decreasing frequency among high scorers (>68) as compared with medium (59–67) and low (0–58) scorers.
Abbreviation: SHY-SR, self-report questionnaire of the Structured Clinical Interview for the Assessment of Social Anxiety Spectrum.
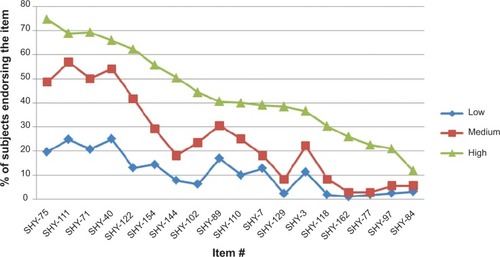
In particular, medium and high scorers showed a similar frequency of endorsement of the following items: #111 (oral examination), #40 (expressing disagreement), #89 (using a public restroom), #3 (social life at school), and #84 (signing official documents and writing in front of others).
Finally, the three groups were compared on the 18-item ‘Avoidant Behavior’ sub-scale total score reported in . Low scorers scored 2.0±1.8, medium scorers scored 4.5±1.7, and high scorers scored 8.0±3.2 (Tukey’s post hoc tests: low < medium, P<0.001; medium < high, P<0.001; low < high, P<0.001).
Secondary analyses were conducted to clarify whether subjects reporting that they had physical symptoms during childhood/adolescence when exposed to social situations were more prone to react in the same way in young adulthood than those not having these symptoms.
Inspection of the odds ratios for each of the seven physical symptoms explored by the SHY-SR indicated that subjects somatizing their social anxiety during childhood/adolescence were between 1.7 and 8.1 times more likely than non-somatizers to display physical symptoms later in their life (). All the odds ratios were significant at P<0.002.
Table 4 Odds ratios and 95% confidence interval of endorsing seven physical symptoms in social situations for subjects who reported experiencing physical symptoms during childhood/adolescence
Discussion
In our study, we found three groups of students characterized, respectively, by low, medium, and high frequency of social anxiety symptoms according to the SHY-SR. In particular, 38.6% (medium plus high scorers) of students reported at least 59 (35%) of 168 SHY-SR lifetime symptoms of the social anxiety spectrum. This large array of social anxiety symptoms among university students is consistent with a previous study conducted in Brazil in which a large percentage of screened individuals exhibited social avoidance symptoms and 11.6% fulfilled diagnostic criteria for SAD.Citation19,Citation20 In these two studies, sub-threshold SAD demonstrated intermediate characteristics between those with full-fledged diagnosis and the control group. In addition, prevalence of axis I psychiatric comorbidities and psychosocial impairment had dose-dependent values through the SAD spectrum.
Our rates of social anxiety symptoms confirmed those reported in previous surveys conducted in young adult populations. For instance, Essau et alCitation21 reported that 47.2% of their sample reported ‘social fears’ and Wittchen et alCitation22 reported that a strong fear of at least one social situation was acknowledged in their survey by 22.3% of males and 32% of females. In a French survey about common fears, 51% adults, found that symptoms of social anxiety were present in 42% of their sample. Of these, 6% reached a diagnostic level and 36% reached a sub-threshold level (defined as one social phobia symptom plus avoidance) or a single symptom level.
In our previous survey conducted among high-school students (aged 18–19 years, attending the last [fifth] year of school), the following five were the most common social fears: fears related to oral examination; performing in front of an audience; expressing romantic feelings; and speaking, singing, dancing in front of others.Citation16 The present study has now also confirmed the high frequency of these symptoms in university students. Moreover, seven additional symptoms were endorsed by more than 50% of the overall sample. It is noteworthy that among these, there were items typically related to social situations that were more likely to be encountered by university students than by high-school youngsters, for example “Have you often felt more comfortable in small groups?”, “Have you often felt you were physically unattractive?”, “Have you often felt embarrassed and uncomfortable when you had to ask someone you liked to go out on a date, like to a movie, to dinner or to a club?”. In addition, we found a high frequency of endorsement of “Do you worry a lot about having to perform in public or taking an oral examination?”. This finding is probably because, in Italian universities, unlike in other countries, most examinations are orally performed in front of other students. It is worthy of note that these specific social fears were significantly more represented among high and medium scorers than low scorers.
Most avoidance behaviors were also reported by a large percentage of subjects with moderate levels of social anxiety, including poor school performance and interrupting school. Overall, our results indicate that students with moderate forms of social anxiety were likely to have psychosocial impairment to a significant extent, corroborating previous data previously reported in the literature.Citation8,Citation11,Citation19–Citation21 In addition, the female/male ratio was increased among high scorers (31.6% versus 23.8%), in line with our previous study in high-school youngsters and other reports.Citation15–Citation17,Citation20
As far as differences between sexes are concerned, among low scorers, women reached higher scores in the domains ‘interpersonal sensitivity’ and ‘phobias related to exposure in social situations’ (for instance, speaking or eating in public, participate in social activities). These data corroborate the notion that mild social anxiety symptoms, borderline shyness, are probably more typical of the female sex.Citation1
Medium scorers reported higher levels of childhood and adolescence social anxiety features, seemingly suggesting that more structured forms of social anxiety may be associated with an early onset of symptoms; this has also been hypothesized by with the stereotypical view of males as self-confident and rarely ashamed, these data suggest that males with severe social anxiety may not have effective compensatory strategies when faced with social performance expectations.Citation25 It will be interesting to explore in further research whether this relationship would be mediated by lower frequency of activation of problem-focused coping strategies and higher frequency of engagement in dysfunctional coping strategies.Citation26
Overall, our data suggest that, when the level of social anxiety increases, differences between sexes become quantitatively more pronounced and the symptom profile becomes qualitatively different between the two sexes. Important novel findings include the corroboration of the notion that social anxiety is associated with functional impairment and that social anxiety seems to be a one-dimensional construct with a tendency to a dose–response relationship between number of fears and degree of impairment.Citation1 Of note, we found that subjects reporting the experience of physical symptoms in social situations during childhood/adolescence were more likely to have the same symptoms during young adulthood. This result suggests that subjects with a tendency to somatize their emotional distress may identify a homogeneous subgroup of individuals suffering from social anxiety.
Some limitations of this study must be acknowledged. The study may have a selection bias due to the possible exclusion from the study of those subjects who left university because of severe social anxiety symptoms. On the other hand, it is also possible that students who participated in the survey might be more aware of their social anxiety symptoms and of related impairment than those who did not complete the questionnaire. This may be particularly true for females, who responded to the email at a significantly higher rate than males.
Second, the methods for participant recruitment may not have been optimal for studying social anxiety as a continuum, as there is no means of knowing whether those individuals who chose not to return the questionnaire may have represented specific areas in the presumed continuum. Third, the fact that the study was conducted in a single university limits the generalizability of our results to the entire population of Italian university students. Finally, as our correlations stem from non-longitudinal data, they can neither rule out the possibility of third variables (for instance psychiatric comorbidity) causing co-variation between our focus variables nor establish paths of causality.
Conclusion
Our study confirms the results from previous studies suggesting the wide spread of social anxiety symptoms in young adulthood and the presence of functional impairment, defined by avoidance and school difficulties, not only among students who reported the highest scores for social anxiety but also in those with moderate social anxiety. For severe social anxiety, we found a male preponderance and differences in symptom profile in the two sexes.
To be diagnosed with SAD, the individual must suffer significant distress or impairment that interferes with his or her ordinary routine in social settings, at work or school, or during other everyday activities. It is interesting to note that, unlike in the DSM-IV, which requires that the individual recognize that his or her response is excessive or unreasonable, the DSM-V criteria shift that judgment to the clinician. Therefore, further studies are warranted to explore in more detail the possibilities of prevention of social anxiety symptoms among non-clinical populations and implementation of non-conventional treatments as has recently been suggested.Citation27
Acknowledgments
The authors thank the coordinator of the students sector of the Board of Education and Student Services of Pisa University, L Rivetti.
Disclosure
The authors report no conflicts of interest in this work.
References
- RuscioAMBrownTAChiuWTSareenJSteinMBKesslerRCSocial fears and social phobia in the USA: results from the National Comorbidity Survey ReplicationPsychol Med2008381152817976249
- Van RoyBKristensenHGroholtBClench-AasJPrevalence and characteristics of signicant social anxiety in children aged 8–13 years: a Norwegian cross-sectional population studySoc Psychiatry Psychiatr Epidemiol200944540741519015797
- SteinMBKeanYMDisability and quality of life in social phobia: epidemiologic findingsAm J Psychiatry2000157101606161311007714
- WittchenHUFehmLEpidemiology and natural course of social fears and social phobiaActa Psychiatr Scand Suppl2003108Suppl 41741812950432
- RussellGTophamPThe impact of social anxiety on student learning and well-being in higher educationJ Ment Health201221437538522823093
- RussellGShawSA study to investigate the prevalence of social anxiety in a sample of higher education students in the United KingdomJ Mental Health2009183198206
- TillforsMFurmarkTSocial phobia in Swedish university students: prevalence, subgroups and avoidant behaviorSoc Psychiatry Psychiatr Epidemiol2007421798617160591
- DavidsonJRHughesDCGeorgeLKBlazerDGThe boundary of social phobia. Exploring the thresholdArch Gen Psychiatry199451129759837979886
- FurmarkTSocial Phobia: From Epidemiology to Brain Function Comprehensive Summaries of Uppsala Dissertation from the Faculty of Social Sciences n 97UppsalaActa Universitatis Upsaliensis2009
- KesslerRCSteinMBBerglundPSocial phobia subtypes in the National Comorbidity SurveyAm J Psychiatry199815556136199585711
- SteinDJRuscioAMLeeSSubtyping social anxiety disorder in developed and developing countriesDepress Anxiety201027439040320037919
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders5th edArlingtonAmerican Psychiatric Publishing2013
- Dell’OssoLRucciPCassanoGBMeasuring social and obsessive-compulsive spectrum disorders: comparison of interviews and self-report instrumentsCompr Psychiatry2002432818711893984
- RucciPMaserJDInstrument development in the Italy-USA Collaborative Spectrum ProjectEpidemiol Psichiatr Soc20009424925611256057
- Dell’OssoLSaettoniMPapasogliASocial anxiety spectrum: gender differences in Italian high school studentsJ Nerv Ment Dis2002190422523211960083
- Dell’OssoLRucciPDucciFSocial anxiety spectrumEur Arch Psychiatry Clin Neurosci2003253628629114714117
- MerikangasKRAvenevoliSAcharyyaSZhangHAngstJThe spectrum of social phobia in the Zurich cohort study of young adultsBiol Psychiatry2002511819111801233
- MerikangasKRStevensDEFentonBCo-morbidity and familial aggregation of alcoholism and anxiety disordersPsychol Med19982847737889723135
- FilhoASHetemLAFerrariMCSocial anxiety disorder: what are we losing with the current diagnostic criteria?Acta Psychiatr Scand2010121321622619694635
- BaptistaCALoureiroSRde Lima OsórioFSocial phobia in Brazilian university students: prevalence, under-recognition and academic impairment in womenJ Affect Disord2012136385786122018945
- EssauCConradtJPetermannFFrequency and comorbidity of social phobia and social fears in adolescentsBehav Res Ther199937983184310458047
- WittchenHUSteinMBKesslerRCSocial fears and social phobia in a community sample of adolescents and young adults: prevalence, risk factors and co-morbidityPsychol Med199929230932310218923
- AndréCLégeronPLa Peur des Autres: Trac, Timidité et Phobie Sociale [The fear of others: fright, shyness and social phobia]ParisOdile Jacob1995 French
- MorcilloCDuarteCSSalaRConduct disorder and adult psychiatric diagnoses: associations and gender differences in the U.S. adult populationJ Psychiatr Res201246332333022172996
- Ein-DorTMikulincerMShaverPRAttachment insecurities and the processing of threat-related information: Studying the schemas involved in insecure people’s coping strategiesJ Pers Soc Psychol20111011789321355660
- ThomassonPPsouniESocial anxiety and related social impairment are linked to self-efficacy and dysfunctional copingScand J Psychol201051217117819500297
- VanniFConversanoCDel DebbioAA survey on virtual environment applications to fear of public speakingEur Rev Med Pharmacol Sci201317121561156823832719