
Abstract
The effects of different intensities of evening exercise on subsequent sleep remain contradictory. Thus, this systematic review and network meta-analysis aimed to compare and rank the effects of different intensities of acute evening exercise on sleep in healthy adults with good sleep. Articles were systematically searched journals indexed in the PubMed, Web of Science, Cochrane Library, Embase, and Scopus databases from inception to the 5th of May, 2022. The basic search terms included exercise, sleep and timing, which were combined with AND. Of the 12,203 retrieved, twenty-eight studies with 325 participants met the inclusion criteria. Results revealed that there were no significant differences in terms of impacts on sleep caused by different intensities of acute evening exercise, except that when compared to no exercise, acute evening high-intensity exercise decreased rapid eye movement sleep (mean difference [MD] = −1.95%, 95% credible interval [CI] = −3.58 to −0.35). Compared to no exercise, acute evening moderate-intensity exercise was ranked as the most potential method to improve sleep, displaying a trend to improve wake time after sleep onset (MD = −2.50 min, 95% CI = −8.17 to 1.62), sleep efficiency (MD = +0.41%, 95% CI = −0.71 to 1.66), the proportion of stage N1 (MD = −0.72%, 95% CI = −2.08 to 0.71) and N3 sleep (slow-wave sleep) (MD = +0.84%, 95% CI = −1.17 to 2.78). Acute evening low-intensity exercise displayed the greatest tendency to shorten sleep onset latency (MD = −1.02 min, 95% CI = −4.39 to 2.50) compared to no exercise. Overall, regardless of intensity, acute evening exercise completed before bedtime does not disrupt subsequent sleep in healthy young and middle-aged adults.
Introduction
Sleep and exercise play the vital role in maintaining human health. The prevalence of insomnia ranges from 10% to 30% in the general population,Citation1 increasing the risk of variable diseases and affecting life expectancy.Citation2–5 Exercise has been proven to be a low-cost and effective way to improve sleep.Citation6,Citation7 A previous systematic review and meta-analysis showed regular exercise and daytime acute exercise had beneficial effects on sleep quality.Citation8 Time-use epidemiology showed that exercising and sleeping time competed with each other in daily life.Citation9 Lack of time has become an obstacle hindering people’s exercise.Citation10 Exercise in the evening progressively becomes a good option for people burdened with day-to-day work. The appearance of 24-hour gym also provides the environment for evening exercise.Citation11 Nonetheless, the American Academy of Sleep Medicine (AASM) does not recommend exercising in the evening as it would cause arousal and disrupt subsequent sleep.Citation12 A cross-sectional study found that most people reported that evening exercise did not disrupt their sleep.Citation13 Some studies also showed that exercise in the evening did not disrupt sleep but rather had small to moderate beneficial effects on sleep.
Dworak et al found that compared to no exercise, only acute evening high-intensity exercise (HIE) made the positive modification to sleep efficiency (SE), sleep onset latency (SOL) and slow-wave sleep (SWS) while evening moderate-intensity exercise (MIE) had no significant effects on sleep in children.Citation14 Not inconsistent with Dworak et al, Oda and Shirakawa suggested acute evening HIE delayed sleep onset (+ 14 min), shortened total sleep time (TST) and decreased SE in active young adults, whereas evening MIE did not disrupt sleep.Citation15 The level of delayed sleep onset found by Oda and Shirakawa was greater than that previously reported in the study of Browman and Tepas (+6.5min).Citation16 Ramos-Campo et al recruited recreational ultra-endurance male runners to conduct acute morning MIE, morning HIE, evening MIE and evening HIE in a random sequence. A significantly higher average time of each awakening was observed in acute evening HIE than in the other three interventions.Citation17 The result of Ramos-Campo et al study suggested that exercise intensity was as important as training time in the evening or the morning.Citation17
Actually, the effects of different evening exercise intensities on sleep are still a hot spot, leading to debates. Vlahoyiannis et al found that acute evening sprint interval training increased TST compared to MIE and no exercise. Moreover, compared to no exercise, sprint interval training also improved SE and shortened wake time after sleep onset (WASO).Citation18 A recent study by Thomas et al of endurance-trained runners showed that compared to no exercise, both acute evening HIE and low-intensity exercise (LIE) increased TST and shortened WASO despite the increase in cardiac autonomic activity.Citation19 Myllymäki et al also found that acute evening LIE, MIE and HIE did not disrupt sleep quality in young adults.Citation20 Conversely, Browman and Tepas found that even evening LIE ended 2 h before bedtime delayed sleep onset compared to no exercise in undergraduates.Citation16 It remains unclear whether acute evening exercise with different intensities disrupts sleep.
The controversies of previous studies might be attributed to the different times of evening exercise, the hours from the cessation of exercise to bedtime, the exercise modality, the physical activity level of participants, and the duration of evening exercise.Citation21,Citation22 Furthermore, there might be an intensity threshold for the effects of evening exercise on sleep. Previous pairwise meta-analyses only focused on comparing high-intensity or moderate-intensity exercise with no-exercise controls, lacking comprehensive comparisons of different intensities of acute evening exercise.Citation21,Citation22 It was necessary to conduct a comprehensive analysis of currently available data regarding acute evening exercise on sleep.
The current systematic review and network meta-analysis (NMA), which would combine direct and indirect evidence to potentially improve the precision of the effect estimates,Citation23,Citation24 aimed to compare and rank different intensities of acute evening exercise on sleep in healthy adults. Owing to the larger magnitude of physiologic excitement that might be induced by HIE, we hypothesized that performing HIE before bedtime would disrupt sleep compared to no exercise, whereas performing MIE and LIE would not.
Materials and Methods
Search Strategy
The search was performed in the PubMed, Web of Science, Cochrane Library, Embase and Scopus databases from inception to the 5th of May, 2022. The basic search strategy consisted of the keywords and MeSH terms related to the intervention (exercise), the outcomes (sleep) and the timing (evening), which was combined with “AND”. The detailed search strategy for Pubmed was: (exercise [mesh] OR sports [mesh] OR physical exertion [mesh] OR “interval training” [tiab] OR aerob* [tiab] OR endurance [tiab] OR strength* [tiab] OR sprint* [tiab] OR anaerob* [tiab] OR exercise [tiab] OR “physical activity” [tiab] OR “high intensity training” [tiab] OR run* [tiab] OR cycling [tiab] OR walk* [tiab] OR swim* [tiab] OR row* [tiab] OR “physical exertion” [tiab] or sport [tiab]) AND (sleep [mesh] OR sleep [tiab] OR “sleep architecture” [tiab] OR “sleep quality” [tiab] OR “sleep efficiency” [tiab] OR polysomnography [tiab] OR actigraphy [tiab]) AND (timing [tiab] OR evening [tiab] OR late-night [tiab] OR bedtime [tiab] OR afternoon [tiab] OR late [tiab] OR “time of day” [tiab] OR time-of-day [tiab] OR “pre sleep” [tiab] OR “before sleep”[tiab] OR pre-sleep [tiab] OR “going to sleep” [tiab] OR “going to bed” [tiab] OR “before bed”[tiab] OR nighttime [tiab] OR night-time [tiab] OR night [tiab]). In addition, we also searched the literature from references cited in the included articles and previous systematic reviews.
Eligibility Criteria
The population, intervention, comparison, outcome and study design (PICOS) framework was used to measure the eligibility criteria. Inclusion criteria for this systematic review and network meta-analysis included: 1) Population: healthy adults (18–65 years) with normal sleep. 2) Intervention: acute exercises in the evening (less than 4h before bedtime or if stated to be conducted in the evening) (high intensity: ≥77% maximal heart rate (HRmax), ≥60% heart rate reserve (HRR) or VO2 reserve (VO2R), ≥64% maximal oxygen consumption (VO2max) or rating of perceived exertion (RPE) ≥14; moderate intensity: 64–76% HRmax, 40–59% HRR or VO2R, 46–63% VO2max or RPE 12–13; low intensity: ≤63% HRmax, ≤39% HRR or VO2R, ≤45% VO2max or RPE ≤11).Citation22,Citation25 3) Comparison: no exercise, LIE, MIE or HIE compared with each other 4) Outcomes: sleep quality and sleep quantity were objectively measured by polysomnography (PSG) and actigraphic sleep parameters and subjectively measured by questionnaires. 5) Study design: randomized controlled trials, randomized crossover trials and within-subject designs written in English were included.
Data Extractions and Risk of Bias Assessment
Two of the authors independently read the full text of included literature and extracted outcomes in an unblinded manner. Any disagreements were resolved by discussion with a third author to achieve consensus. The extracted information included (1) authorship and study design; (2) participant characteristics (sample size, age, gender, physical activity level); (3) intervention characteristics (exercise intervention type, duration, intensity and timing of exercise before bedtimes); (4) bedtimes; (5) sleep measurements; (6) sleep outcomes. The primary outcomes were: TST, SE, SOL, WASO, and sleep architecture including the proportion of stages N1, N2, N3, SWS, and rapid eye movement (REM) sleep. If a study reported the primary outcomes measured by actigraphy and PSG, the PSG data would be extracted for our network meta-analysis. Actigraphy is one-dimensional, while polysomnography includes at least three different types of data (electroencephalogram, electrooculogram, electromyogram) that together determine whether a person is asleep or awake.Citation26 Therefore, PSG is the “gold standard” for the sleep study.Citation26 The secondary outcome was subjective sleep quality (SSQ).
Risk of bias was measured by using the revised Cochrane risk of bias tool for crossover trials (RoB 2.0), which considered the crossover designs. ROB 2.0 consisted of 5 domains: (1) bias arising from the randomization process; (2) bias due to deviations from the intended intervention; (3) bias due to the missing outcome data; (4) bias in the measurement of the outcome; (5) bias in the selection of the reported result. Each domain had signaling questions, requiring the assessors to respond “probably yes”, “yes”, “probably no”, “no” or “no information”. According to an algorithm to the judgment of each domain, the included studies were rated as “low risk of bias”, “some concerns” or “high risk bias”. The assessment was conducted by two authors independently in an unblinded manner.
Statistical Analysis
Means and standard deviations (SDs) were extracted from included studies. If the study only reported standard errors (SEs), SDs were calculated by the following formula: .
Mean differences (MDs) and 95% credible intervals (CIs) were calculated for measuring the effect sizes of each objective sleep outcome, whereas standardized mean differences (SMDs) and 95% CIs were calculated for measuring the effect sizes of subjective sleep quality because of different evaluation methods in included studies. For this NMA, heterogeneity was assessed by I2 static. Values of I2 ≤25%, 25% < I2 ≤50%, 50% < I2 ≤75%, and I2 > 75% indicated no significant heterogeneity, low heterogeneity, medium heterogeneity, and high heterogeneity, respectively.
Bayesian effects network meta-analysis (NMA) was performed by using the “gemtc” package in R (version 4.2.0). Four Markov chain Monte Carlo chains were used to assess convergence with 20,000 iterations. Posterior summaries were then obtained from 50,000 iterations in each of the four chains. Convergence was assessed by using potential scale reduction factors (PSRF). The value of PSRF approached 1, indicating the convergence of the model was satisfactory.
Network plots were created to describe different intensities of acute evening exercise on outcomes. Nodes in the geometry represented different intensities of acute evening exercise and no-exercise control and the lines represented direct comparisons for interventions. The size of each node and the thickness of each line were proportional to the number of participants.
Global inconsistency was assessed by comparing the difference values of differences in conditions (DIC) between the consistency and inconsistency models. A difference value of DIC >5 indicated an inconsistent model.Citation27 Local inconsistency was evaluated by using the node splitting method. In addition, probability ranking for each intervention was conducted by the surface under the cumulative ranking curve (SUCRA) values ranging from 0% to 100%, where 100% indicated the best intervention.
To test the robustness of the results and examine the effects of potential modifiers on primary outcomes, subgroup analyses were performed according to the following variables: time of evening exercise (early evening: 16:00 to 20:00, late evening: after 20:00), hours from cessation of exercise to bedtime (0.5–1.5 h, 2 or >2–4 h), exercise modality (cycling, running), physical activity level of participants (sedentary, physically fit), exercise duration (25–30 min, >30–60 min). Publication bias was subjectively assessed with comparison-adjusted funnel plots. In all the analyses, a statistical significance was set at p < 0.05.
This systematic review and network meta-analysis was carried out in conformance with the PRISMA Extension for Network Meta-analyses (PRISMA-NMA) checklist.Citation28 The protocol for this systematic review and NMA has been registered on PROSPERO (CRD42022327787).
Results
Study Selection
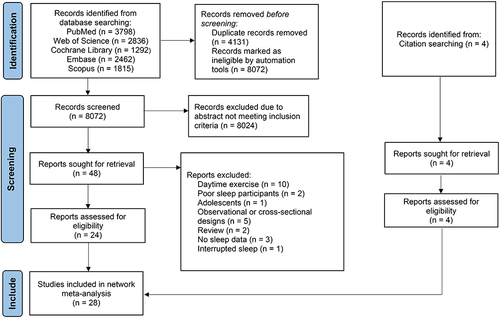
A PRISMA diagram of literature search and selection is presented in . A total of 12,203 studies were initially identified from PubMed, Web of Science, Cochrane Library, Embase, and Scopus databases. After removing duplicates (n = 4131) and reading titles and abstracts (n = 8072), the remaining studies (n = 48) progressed to full-text review and 24 studies met the inclusion criteria. Twenty-four studies were excluded for the following reasons: (1) daytime exercise (n = 10), (2) poor sleep participants (n = 2), (3) adolescents (n = 1), (4) observational or cross-sectional designs (n = 5), (5) review (n = 2), (6) no sleep data (n = 3), (7) interrupted sleep (n = 1). In addition, four additional studies were found from the references of eligible studies. Overall, 28 studies were finally included in this systematic review and network meta-analysis.
Figure 1 PRISMA flow diagram of systematic search and included trials.
Study Characteristics
The characteristics of the included studies are presented in . The SUCRA values were shown in . The network plot of eligible comparisons on objective and subjective sleep quality are shown in . Four nodes were included in the NMA. Each node denoted different interventions: no-exercise control, evening low-intensity exercise (LIE), evening moderate-intensity exercise (MIE), and evening high-intensity exercise (HIE). Among the 28 crossover trials from 1976 to 2021 included in the analyses, 19 studies had two arms,Citation11,Citation16,Citation17,Citation30–45 6 had three armsCitation15,Citation18,Citation19,Citation46–48 and 3 had four arms.Citation20,Citation49,Citation50 There were 325 participants (mean age: 25 years old, range: 18–49 years), of which 290 participants were male, and 35 participants were female. Twenty-three studies were men only,Citation11,Citation15–20,Citation30,Citation31,Citation34,Citation35,Citation37,Citation38,Citation40–48,Citation50 one was women onlyCitation33 and the remaining four included both men and women.Citation32,Citation36,Citation39,Citation49 In addition, most of the participants were physically active or trained populations, and the others were sedentary participants.
Table 1 Descriptive Characteristics of the Included Studies
Figure 2 Network plots for comparisons of outcomes.
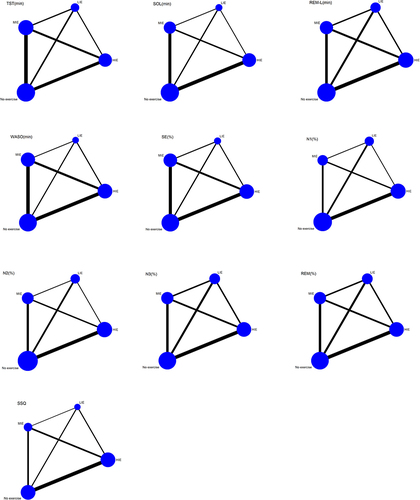
Table 2 SUCRA Values of Different Intensities of Acute Evening Exercise for Sleep Outcomes
In terms of sleep outcomes, 22 of 28 studies reported on the results of the TSTCitation11,Citation15–20,Citation31,Citation34–39,Citation41,Citation44–50 and SOL.Citation11,Citation15,Citation18,Citation19,Citation30–39,Citation42,Citation44–50 18 of 28 studies reported on the results of the SE.Citation11,Citation15,Citation17,Citation18,Citation20,Citation30,Citation31,Citation34,Citation35,Citation37–39,Citation42,Citation45,Citation46,Citation48–50 Two studies did not report SE and calculations were conducted by TST and TIB.Citation19,Citation36 Half of the studies (n = 14) reported on the results of the WASOCitation11,Citation15,Citation18,Citation19,Citation31,Citation34,Citation35,Citation38,Citation39,Citation44–46,Citation49,Citation50 and SSQ (n = 14).Citation11,Citation15,Citation17,Citation19,Citation20,Citation30,Citation31,Citation33,Citation36,Citation37,Citation40,Citation41,Citation43,Citation44 Less than half of the studies reported the latency of rapid eye movement (REM-L) (n = 12),Citation15,Citation16,Citation19,Citation31,Citation33,Citation34,Citation37,Citation38,Citation46,Citation47,Citation49,Citation50 the proportion of REM sleep (n = 11),Citation16,Citation19,Citation31,Citation32,Citation34,Citation36,Citation38,Citation46,Citation47,Citation49,Citation50 the proportion of stage N3 sleep (SWS) (n = 11),Citation16,Citation19,Citation31,Citation32,Citation34,Citation36,Citation38,Citation46,Citation47,Citation49,Citation50 the proportion of stage N1 sleep (n = 9),Citation16,Citation19,Citation31,Citation34,Citation36,Citation38,Citation46,Citation47,Citation50 and the proportion of N2 sleep (n = 10).Citation16,Citation19,Citation31,Citation32,Citation34,Citation36,Citation38,Citation46,Citation47,Citation50
The evening exercises ranged from 25 min to 3 h and comprised cycling or running. Eleven of the included studies used early evening protocol (16:00–20:00),Citation18–20,Citation33–35,Citation37,Citation38,Citation45,Citation47,Citation49 and thirteen of the studies used late-evening protocol (after 20:00).Citation11,Citation15–17,Citation31,Citation32,Citation36,Citation40–42,Citation44,Citation46,Citation48 Three of the remaining studies used both early evening and late-evening protocols,Citation30,Citation39,Citation43 while one study did not mention the time to exercise in the evening.Citation50 Evening exercise ended 0.5 to 4 h before bedtime.
Quality Assessment
Details of RoB 2.0 in each included study were shown in Supplementary Table S1. The majority of included studies showed low risk bias, while eight studies had “some concerns” regarding the randomization process, wash-out period or missing outcome data.Citation11,Citation16,Citation20,Citation33,Citation35,Citation40,Citation48,Citation49 Both “low risk bias” studies and “some concerns” studies were included in this network meta-analysis.
Network Meta-Analysis
TST
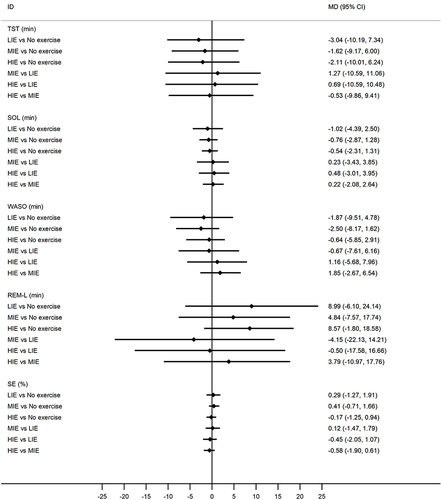
No significant difference was observed in regard to TST among these groups. In comparison with no exercise, the ranking probability based on the SUCRA values indicated that acute evening MIE had the lowest impact on TST (MD = −1.62 min, 95% CI = −9.17 to 6.00, SUCRA = 47.3%), followed by HIE (MD = −2.11 min, 95% CI = −10.01 to 6.24, SUCRA = 44.2%) and LIE (MD = −3.04 min, 95% CI = −10.19 to 7.34, SUCRA = 37.0%). Compared with LIE, acute evening MIE and HIE were comparable to each other in terms of the effects of increased TST, and no significant difference was found. Compared to MIE, though acute evening HIE reduced TST, no significant difference was observed ().
Figure 3 Forest plots of network meta-analysis of all comparisons for TST, SOL, WASO, REM-L, and SE.
SOL
No significant difference was observed in regard to SOL among these groups. In comparison with no exercise, according to the SUCRA values, acute evening LIE was ranked to be better for the shortening of SOL (MD = −1.02 min, 95% CI = −4.39 to 2.50, SUCRA = 61.7%), followed by MIE (MD = −0.76 min, 95% CI = −2.87 to 1.28, SUCRA = 60.3%) and HIE (MD = −0.54 min, 95% CI = −2.31 to 1.31, SUCRA = 50.4%). Compared with LIE, acute evening MIE and HIE were comparable to each other in terms of the effects of increased SOL, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE increased SOL ().
WASO
Regarding WASO, no statistically significant difference was observed among these groups. In comparison with no exercise, the SUCRA revealed that acute evening MIE was ranked the best method to shorten WASO (MD = −2.50 min, 95% CI = −8.17 to 1.62, SUCRA = 74.8%), followed by LIE (MD = −1.87 min, 95% CI = −9.51 to 4.78, SUCRA = 59.4%) and HIE (MD = −0.64 min, 95% CI = −5.85 to 2.91, SUCRA = 39.4%). Compared with LIE, acute evening MIE shortened WASO and HIE increased WASO, respectively, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE increased WASO ().
SE
Acute evening LIE, MIE and HIE yielded no significant effects on SE compared with no exercise. The MDs and 95% CIs of SE in the acute evening LIE, MIE, and HIE were +0.29% (95% CI = −1.27 to 1.91), +0.41% (95% CI = −0.71 to 1.66), and −0.17% (95% CI = −1.25 to 0.94), respectively. Acute evening MIE had the highest probability of being the best option to improve SE, based on the SUCRA values (72.1%). Compared with LIE, acute evening MIE improved SE, while HIE decreased SE, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE decreased SE ().
REM-L
In comparison with no exercise, although there were no significant effects, acute evening HIE was ranked the best intervention to increase REM-L (MD = +8.57 min, 95% CI = −1.80 to 18.58, SUCRA = 71.0%), followed by LIE (MD = +8.99 min, 95% CI = −6.10 to 24.14, SUCRA = 69.3%) and MIE (MD = +4.84 min, 95% CI = −7.57 to 17.74, SUCRA = 46.9%). Compared with LIE, acute evening MIE and HIE resulted in similar results, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE increased REM-L ().
The Proportion of Stage N1 Sleep
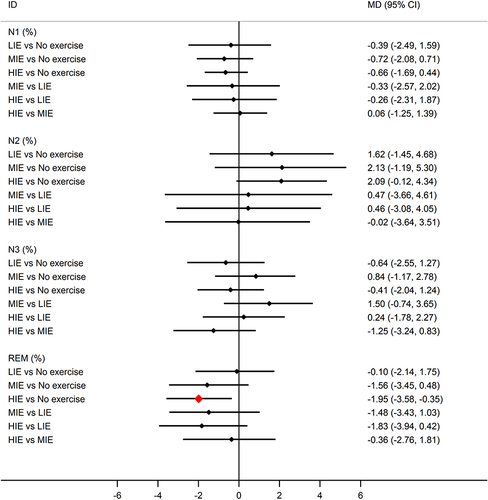
In comparison with no exercise, acute evening LIE, MIE, and HIE did not show significant reductions in the proportion of stage N1 sleep, showing MDs of −0.39% (95% CI = −2.49 to 1.59), −0.72% (95% CI = −2.08 to 0.71), and −0.66% (95% CI = −1.69 to 0.44), respectively. The ranking probability based on the SUCRA values indicated that acute evening MIE had the highest probability of being the best option to reduce the proportion of stage N1 sleep (SUCRA = 67.2%). Compared with LIE, both acute evening MIE and HIE resulted in a reduction of the proportion of stage N1 sleep, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE increased stage N1 sleep ().
Figure 4 Forest plots of network meta-analysis of all comparisons for N1, N2, N3, and REM sleep.
The Proportion of Stage N2 Sleep
In comparison with no exercise, although there were no significant effects, acute evening HIE was regarded as the best method to increase the proportion of stage N2 sleep (MD = +2.09%, 95% CI = −0.12 to 4.34, SUCRA = 68.9%), followed by MIE (MD = +2.13%, 95% CI = −1.19 to 5.30, SUCRA = 66.6%) and LIE (MD = +1.62%, 95% CI = −1.45 to 4.68, SUCRA = 55.2%). Compared with LIE, both acute evening MIE and HIE resulted in increasing the proportion of N2 sleep, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE decreased stage N2 sleep ().
The Proportion of Stage N3 Sleep (SWS)
There was no significant difference observed in regard to the proportion of N3 sleep among these groups. In comparison with no exercise, the SUCRA revealed that acute evening MIE ranked the highest in terms of improving the proportion of N3 sleep (MD = +0.84%, 95% CI = −1.17 to 2.78, SUCRA = 86.2%), followed by HIE (MD = −0.41%, 95% CI = −2.04 to 1.24, SUCRA = 33.9%) and LIE (MD = −0.64%, 95% CI = −2.55 to 1.27, SUCRA = 25.0%). Compared with LIE, both acute evening MIE and HIE resulted in increasing the proportion of N3 sleep, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE shortened stage N3 sleep ().
The Proportion of REM Sleep
The NMA suggested that, in comparison with no exercise, acute evening HIE was ranked to be significantly better for the shortening of REM (MD = −1.95%, 95% CI = −3.58 to −0.35, SUCRA = 85.4%), followed by MIE (MD = −1.56%, 95% CI = −3.54 to 0.48, SUCRA = 73.6%) and LIE (MD = −0.10%, 95% CI = −2.14 to 1.75, SUCRA = 23.1%). Compared with LIE, both acute evening MIE and HIE resulted in shortening REM, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE shortened REM ().
SSQ
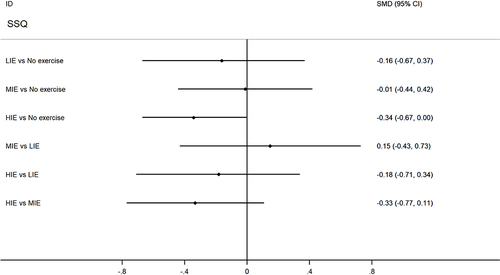
In comparison with no exercise, although there were no significant effects, the ranking probability based on the SUCRA values indicated that acute evening MIE had the lowest impact on SSQ (SMD = −0.01, 95% CI = −0.44 to 0.42, SUCRA = 73.1%), followed by LIE (SMD = −0.16, 95% CI = −0.67 to 0.37, SUCRA = 43.9%) and HIE (SMD = −0.34, −0.67 to 0.00, SUCRA = 11.2%). Compared with LIE, acute evening MIE improved SSQ, while HIE decreased SSQ, and no significant difference was found. Compared to MIE, no significant difference was observed while acute evening HIE decreased SSQ ().
Figure 5 A forest plot of network meta-analysis of all comparisons for SSQ.
The test of global inconsistency did not show any significant difference between the consistency and inconsistency models for all outcomes (all difference values of DIC were <5). Similarly, the node splitting method, which tested local inconsistency, showed that all comparisons among direct and indirect estimates were consistent for all outcomes (all p values >0.5, Supplementary Table S12). In addition, no significant global heterogeneity of the NMA was found (I2 = 0%). There was no significant local heterogeneity in most of the comparisons in this NMA (I2 = 0% or 5.2%) except that only three comparisons showed low local heterogeneity (I2 = 15.6%, 24.7% and 29.1%) (Supplementary Tables S2–S11). The comparison-adjusted funnel plots for the outcomes suggested publication bias was not evident (Supplementary Figures S1–S10).
The subgroup NMA explored the effects of time of evening exercise, hours from cessation of exercise to bedtime, exercise modality, physical activity level, and exercise duration of acute evening exercise on objective sleep quality. The results of NMA of all outcomes were not modified in most of the comparisons. Different intensities of exercise performed in early- and late-evening had no negatively impact on objective sleep quality. The timeslot between the end of exercise and bedtime (0.5–1.5 h, 2 h, >2–4 h) had no effects on objective sleep quality. In addition, regardless of sedentary or physically fit participants, different intensities of evening exercise had no effects on objective sleep quality. However, compared with no exercise, MIE with cycling significantly increased REM-L (MD = 38.78 min, 95% CI = 3.99 to 73.80) and a longer (>30–60 min) HIE decreased REM sleep (MD = −2.50%, 95% CI = −4.74 to −0.35) (Supplementary Table S13).
Discussion
This systematic review and network meta-analysis explored the effects of acute evening exercise with different intensities on sleep in healthy adults. In contrast to our hypothesis, no significant differences were observed in both objective and subjective sleep quality with different evening exercise intensities. The present findings were in line with a study showing that different intensities of acute evening exercises did not disrupt sleep in healthy young and middle-aged adults.Citation20 However, in line with our hypothesis and Frimpong et al's pairwise meta-analysis, 30–60 min duration with acute evening HIE resulted in a decrease in the REM sleep, which might worsen sleep quality.Citation21 In addition, acute MIE with cycling in the evening resulted in an improvement on REM-L.
Sufficient sleep plays an important role in restoring the consumption of the nervous system and metabolization in the waking stage,Citation51 and daytime exercise has been proven to be positive for sleep.Citation8 TST was associated with daytime sleepiness.Citation52 Furthermore, a previous study from the Asia Cohort Consortium suggested that TST was a behavioral risk factor in mortality in both men and women and TST of seven hours was recommended.Citation53 Oda and Shirakawa found a reduction in TST after acute HIE was completed one hour before bedtime compared with no exercise while TST in MIE did not change in twelve young males.Citation15 Not in line with Oda and Shirakawa, a recent study reported, compared with no exercise, acute evening HIE did not disrupt TST in 12 healthy males.Citation41 Thomas et al also found that acute evening HIE and LIE resulted in similar improvements in TST.Citation19 The crossover trial of Miller et al suggested that 30 min cycling at 75% HRmax ended 1.5 h before bedtime did not affect TST in 12 young males.Citation11 The results of the present NMA also supported the notion that acute evening exercise did not disrupt TST regardless of exercise intensities in healthy young and middle-aged adults. The results of Frimpong et al's pairwise meta-analysis were consistent with the current study that evening HIE did not significantly disrupt TST (+ 2.34 min).Citation21
In addition to TST, knowledge about SOL, WASO, and SE was also important, because SOL, WASO, and SE could predict the perceived sleep quality in healthy subjects.Citation54 SOL could be recalled easily in the morning, which might result in increment in the perception of daytime dysfunction as well as perceived poor sleep quality.Citation55 The current study found there was a trend of shortening SOL after acute evening exercise compared to no exercise, and LIE might be the best method for the improvement of SOL (- 1.02 min). Oda and Shirakawa found a delay in SOL (+ 14 min) after HIE in the evening,Citation15 which was contrary to the current study that acute evening HIE did not delay sleep onset (−0.54 min). In line with our findings, Hayashi et al suggested relative to no exercise, acute evening HIE and MIE could significantly shorten SOL in nine sedentary college students.Citation50 In Myllymäki et al study, some indications of shortened SOL were also observed after acute evening HIE.Citation36 In addition, Ramos-Campo et al found average time of each awakening was significantly higher when 14 recreational male runners conducted acute evening HIE compared to MIE.Citation17 Conversely, a previous meta-analysis found that exercise conducted at any time of the day had a significantly positive result for WASO.Citation8 The current NMA revealed a decreased trend of WASO after acute evening exercise and the largest decrease in WASO was observed after acute evening MIE compared to no exercise (−2.50 min). In consistent with our findings, a recent crossover trial also found acute evening MIE did not affect WASO compared with no exercise in 16 healthy college students.Citation39 In regard to SE, although our study found acute evening exercise did not disrupt SE, different trends of SE after different intensities of acute evening exercise were observed. The current NMA resulted in improved trends of SE after acute evening LIE (+ 0.29%) and MIE (+ 0.41%), while the worsening trend of SE was observed after HIE (- 0.17%) compared with no exercise. This was supported by a study conducted in eight physically active college students, which revealed that SE was not worsened after acute evening MIE and LIE.Citation48 In regard to acute evening HIE, compared to no exercise, a recent pairwise meta-analysis revealed similar trends of SE (−0.22%) with the findings in our study.Citation21 Disturbances of SOL and SE were associated with an increased risk of mortality.Citation56 The non-disruptive findings of SOL, WASO, and SE in the current NMA were of potential clinical significance.
In regard to sleep architecture, compared to no exercise, the current NMA did not find significant changes in the proportion of stages N1, N2, N3 sleep as well as REM-L after different intensities of acute evening exercise, while the proportion of REM sleep was significantly decreased after acute evening HIE. There was an indication of increased stage N1 sleep during the whole night in Aloulou et al study, and they also observed the proportion of stage N1 sleep was higher during the first 180 min of the night after acute evening HIE compared with no exercise.Citation31 Not inconsistent with the findings of Aloulou et al, Flausino et al found that the stage N1 sleep significantly decreased after acute evening HIE and MIE compared with no exercise.Citation46 The results of the current study showed a declining trend in stage N1 sleep after acute evening exercise compared to no exercise. As stage N1 sleep represented light sleep, acute evening MIE might be the best method to shorten the proportion of stage N1 sleep in our findings (−0.72%). A previous pairwise meta-analysis also supported our results that stage N1 sleep was not significantly changed after evening HIE compared to no exercise.Citation21 SWS, a component of non-rapid eye movement (NERM) sleep, was associated with increased growth hormone and decreased cortisol secretion.Citation47,Citation57 Therefore, it has been proved to be the most restorative sleep stage. There were different trends in SWS after different intensities of acute evening exercise observed in the current findings. The positive modification of SWS was observed after acute evening MIE (+ 0.84%) while shortened SWS was observed after acute evening LIE (−0.64%) and HIE (−0.41%) compared to no exercise. In contrast to our findings, the randomized crossover trial of Dworak et al found that acute evening HIE completed 3–4 h before bedtime resulted in a significantly increased proportion of SWS, and this change was not found in acute evening MIE.Citation14 The discrepancy might be attributed to the population. The current study focused on young and middle-aged adults, whereas children (mean: 12.6 years old) were recruited in the study of Dworak et al. However, Hayashi et al study echoed the current results. Although Hayashi et al did not find significant difference, they found a tendency for an increase in the proportion of SWS after acute evening MIE compared to no exercise in nine sedentary college students (mean: 22.8 years old).Citation50 Considering that the sample size of included studies was small, the effects of evening MIE on SWS needed to be further researched.
Our study found REM sleep was significantly shortened after acute evening HIE compared to no exercise (−1.95%), which was consistent with Frimpong et al pairwise meta-analysis (−2.34%).Citation21 Previous studies found the similar effects of evening exercise on REM sleep. The meta-analysis of Stutz et al revealed that, after sensitivity analysis, the decrease of REM sleep became a trend or significant after acute evening exercise compared to no exercise (−0.69%).Citation22 Both Larsen et al and Aloulou et al observed a tendency for decreased REM sleep during the whole night after acute evening HIE compared to no exercise in healthy young adults.Citation31,Citation34 Moreover, there was also a tendency for decreased REM sleep after acute evening LIE (−0.10%) and MIE (−1.56%) in the present study, which conformed to the result of Wong et al study.Citation49 Wong et al showed that there was a trend of a reduced proportion of REM sleep with increased evening exercise intensity.Citation49 The results of our study showed that acute evening HIE decreased REM sleep, whereas LIE and MIE did not. What is more, previous analyses found even if exercise during the day, REM sleep still decreased.Citation7,Citation8,Citation58 However, decreased REM sleep was not necessarily harmful. A previous study found that decreased REM sleep could reflect the consolidation of REM sleep and could also be the result of enhanced SWS.Citation59 The PSG data from Larsen et al showed decreased REM sleep predominantly within the initial 180 min of sleep after acute evening HIE, in keeping with the findings of Netzer et al and Robey et alCitation38,Citation60 Furthermore, Netzer found that an increase in norepinephrine after intense exercise was associated with decreased REM sleep and increased REM-L.Citation60 Indeed, the results of the current NMA revealed a tendency for increased REM-L after acute evening exercise compared to no exercise, and acute evening HIE was regarded as the best intervention to increase REM-L (+ 8.57 min). After HIE, the release of norepinephrine was 14.5 higher than MIE,Citation61 which might result in delayed REM sleep.
In addition, most of the included studies assessed SSQ. There were disagreements about whether evening exercise was beneficial to SSQ among previous studies. Both Aloulou et al and Arias et al reported SSQ was impaired after acute evening HIE while good SSQ was observed without evening exercise.Citation30,Citation31 Delayed onset muscle soreness after HIE might be the reason for poor SSQ the next morning.Citation62,Citation63 In contrast to Aloulou et al and Arias et al, some studies revealed that SSQ was not affected after acute evening LIE, MIE and HIE compared to no exercise.Citation11,Citation20,Citation36 Compared with no exercise, acute evening MIE and HIE did not negatively affect subjective TST and WASO.Citation11,Citation31,Citation37 Oda & Shirakawa found that compared with no exercise, subjective SOL was negatively affected by acute evening HIE but not by acute evening MIE.Citation15 Conversely, some studies also supported the notion that neither acute evening MIE nor HIE would negatively affect subjective SOL compared to no exercise.Citation11,Citation17,Citation44 As we mentioned above, the SOL would be easily recalled in the next morning, which might affect the perceived SSQ of participants. The present NMA did not find distorted SOL after evening exercise, and the results supported the notion that evening exercise regardless of low-, moderate- and high intensity did not disrupt SSQ in young and middle-aged adults.
Previous pairwise meta-analyses suggested that the time of evening exercise, the hours from cessation of exercise to bedtime, the exercise modality, the physical activity level of participants, and the duration of evening exercise should be considered when analyzing the effects of acute evening exercise on objective sleep quality.Citation21,Citation22 Subgroup analyses in the current study revealed a long duration (>30–60 min) of acute evening HIE significantly decreased the proportion of REM sleep compared to no exercise (−2.50%). Considering increased norepinephrine levels after HIE,Citation60 long duration might be a potential factor to facilitate this process. The results of Youngstedt et al study also showed acute evening HIE with 3 hours did not disrupt subsequent sleep in 16 cyclists.Citation44 Given that active participants might recover in a short period of time after exercise, the physical activity level of participants was considered in subgroup analysis. The present NMA subgroup analysis of physical activity level did not show any significant effects of acute evening exercise on objective sleep quality. In addition, cycling with acute evening MIE had significantly positive effects on REM-L compared to no exercise (+ 38.78 min), while there were no effects observed after running. Meanwhile, although a study had proven that running was more likely to induce higher levels of muscle damage and inflammation compared to cycling,Citation64 no sufficient evidence showed that muscle damage and inflammation affect sleep negatively.
Given that an acute psychophysiological response was induced by an acute exercise, exercise in the early evening might have sufficient recovery for a psychophysiological response that might not disrupt subsequent sleep, whereas exercise in the late evening might negatively affect sleep. However, the subgroup analysis of time of evening exercise in the present study found exercise in the early and late evening did not disrupt sleep regardless of exercise intensity. A previous meta-analysis found early evening HIE shortened SOL (−4.6 min), and late-evening exercise had no negative effects on sleep.Citation21 When considering the hours from cessation of exercise to bedtime, exercise performed close to bedtime might disrupt sleep especially HIE.Citation65 Oda and Shirakawa found that compared with no exercise, evening HIE end 1 h before bedtime delayed sleep onset (+14 min) and decreased TST and SE.Citation15 Conversely, the study of Youngstedt et al suggested that even acute evening HIE ended 0.5 h before bedtime did not disturb sleep.Citation44 Thus, the subgroup analysis was conducted to explore the effects of the hours from cessation of exercise to bedtime. The results of the present study showed that evening exercise regardless of intensity ended 0.5–1.5 h, 2 h and >2–4 h before bedtime did not disrupt sleep. In line with the present results, evening MIE ended 1h or 0.5 h before bedtime had no effects on sleep in previous studies.Citation15,Citation48 The meta-analysis of Frimpong et al also showed that evening HIE ended 2 h before bedtime significantly decreased SOL and increased TST.Citation21 Although some studies found that compared with no exercise, evening HIE and MIE ended 2–4 h before bedtime decreased REM sleep,Citation21,Citation45,Citation47 the decreases in REM sleep were also found in daytime exerciseCitation6–8 and, as we discussed above, the decreases in REM sleep did not necessarily indicate a negative effect on sleep. These results of subgroup analyses consolidated the main finding that evening exercise regardless of intensity did not disrupt subsequent sleep.
The chronotypes of participants might be a potential factor modulating the effects of evening exercise on sleep. Six of included studies reported the chronotypes of participants.Citation17–19,Citation31,Citation39,Citation42 The study of Aloulou et al found that, compared with no exercise, late-evening HIE ended 2 h before bedtime had negative impacts on sleep in neither-type participants.Citation31 Not consistent with Aloulou et al, Thomas et al and Vlahoyiannis et al reported that evening HIE ended 3–3.5 h before bedtime improved sleep quality in neither-type participants.Citation18,Citation19 Moreover, the positive changes of sleep quality induced by evening LIE ended 3.5 h before bedtime were comparable to those induced by evening HIE in neither-type participants.Citation19 Saidi et al also showed that early evening MIE ended 4 h before bedtime had positive effects on sleep quality in neither-type participants.Citation39 The study of Vitale et al, which involved both morning-type and evening-type participants, demonstrated that the sleep quality of morning-type participants was negatively affected by late evening HIE while that of evening-type participants was not affected.Citation42 However, morning HIE did not negatively affect the sleep quality of both morning-type and evening-type participants.Citation42 A recent cross-sectional study investigated 909 college students, and showed chronotype moderated the relationship between exercise timing and bedtime.Citation66 For every minute of delay in exercise timing, bedtime was delayed by 6.1 minutes for morning-type participants and only 3.6 minutes for evening-type participants.Citation66 Existing studies mainly focus on neither-type participants, while only one of included studies considered morning-type and evening-type participants. Few studies had taken chronotype into consideration when exploring the effects of evening exercise on sleep quality. Therefore, how chronotype modulates the relationship between different intensities of evening exercise and subsequent sleep needs to be further researched.
The potential complicated mechanisms between acute evening exercise and sleep were still unclear and were roughly clarified as the thermoregulation hypothesis, body recovery hypothesis, and energy storage hypothesis.Citation67–69 Some previous studies reported the rising body temperature induced by exercise made a positive effect on the proportion of SWS.Citation70,Citation71 The study of Horne and Moore, who used extra clothes (hot) to elevate body temperature, found only exercise in hot conditions increased SWS.Citation70 Actually, during the period of high core body temperature (CBT), the human body was awake and active while during the period of low CBT, the body was inactive and asleep.Citation72 Based on this view and in consideration of previously mentioned studies which showed rising body temperature associated with the improvement of SWS were not conducted in the evening,Citation70,Citation71 it seemed that high CBT close to bedtime was detrimental to subsequent sleep. However, some studies were in contrast with this notion. Youngstedt et al recruited 16 healthy cyclists, and the results showed that rising CBT caused by acute evening HIE with 3 hours completed 30 min before bedtime did not disrupt sleep.Citation44 The study of Aloulou et al showed that, although CBT significantly increased at the end of acute evening HIE (+1.40 ± 0.43°C) and remained high during the first 3 hours of sleep compared with no exercise, the objective sleep quality was not distorted by the elevated temperature.Citation31 Another notion that the decrease of CBT after exercise rather than absolute CBT was the inducement of sleep onset was worth mentioning to illustrate the influence of evening exercise on sleep.Citation73 Nevertheless, Miller et al found that CBT elevated during acute evening MIE and CBT returned to its pre-exercise level when going to bed, but no positive modification of SOL was observed.Citation11 Flausino et al did not find peripheral body temperature would increase with the increment of exercise intensity, nor did they find that the peripheral body temperature played a vital role in the delay of sleep latency and TST reduction.Citation46 CBT also declined rapidly after acute evening exercise, yet it did not make an improvement on SOL in Flausino et al study.Citation46 The present NMA subgroup analysis of hours from the cessation of exercise to bedtime (0.5–2 h, 2h, >2–4 h) did not show any significant difference between acute evening exercise on subsequent objective sleep quality regardless of exercise intensity, which disproved the thermoregulation hypothesis indirectly. However, complete clinical trials are also needed to directly verify whether the thermoregulation hypothesis can explain the effects of acute evening exercise with different intensities on sleep.
The body recovery and energy storage hypothesis suggested the quantity of TST and SWS would increase with the increased energy consumption.Citation68,Citation69 High catabolic activity during awake was beneficial to anabolic activity during sleep.Citation46 As a previous study found, the growth hormone released during the SWS phase was beneficial to physical and mental health.Citation58 However, as existing studies did not measure energy consumption during different intensities of evening exercise, future studies could focus on this area. Moreover, hormone secretion after evening exercise might also affect subsequent sleep. As was mentioned in the study of Netzer et al, more norepinephrine released after HIE compared to MIE was associated with induced delayed REM sleep and the shortened proportion of REM sleep.Citation60 Buxton et al and Miyazaki et al found both the onset and peak phase of plasma melatonin were earlier after an acute exercise compared to no exercise.Citation74,Citation75 How hormone secretion after different intensities of acute evening exercise affected subsequent sleep needed to be further researched.
To the best of our knowledge, this NMA represented the most comprehensive analysis of currently available data regarding different effects of intensities of acute evening exercise on subsequent sleep. The convergence of the current NMA was good (PSRF = 1 or 1.01) and the global heterogeneity was low (I2 = 0%). However, some limitations should be noted in this study. The sample size of included studies was small (ranged 5 to 23) and most of the participants were males, which might cause bias in the results. In addition, this systematic review and network meta-analysis focused on acute evening exercise. Thus, the effects of different intensities of chronic evening exercise on sleep needed to be further researched. Our study did not find positive effects of acute evening exercise on subsequent sleep due to ceiling and floor effects, which meant that it would be more effective for participants who were already presented impaired sleep to exercise before sleep.Citation76 Also, only good sleepers were explored in our study, limiting the application of the findings to a broad population.
Conclusion
This systematic review and network meta-analysis found that acute evening exercise regardless of intensity completed before bedtime did not disrupt subsequent sleep in healthy young and middle-aged adults without sleep disorders. The modality and duration of evening exercise should be considered when developing sleep hygiene recommendations.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors thank Ruicong Liu for advice during research writing.
References
- Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6(2):97–111. doi:10.1053/smrv.2002.0186
- Lovato N, Lack L. Insomnia and mortality: a meta-analysis. Sleep Med Rev. 2019;43:71–83. doi:10.1016/j.smrv.2018.10.004
- Bertisch SM, Pollock BD, Mittleman MA, et al. Insomnia with objective short sleep duration and risk of incident cardiovascular disease and all-cause mortality: sleep Heart Health Study. Sleep. 2018;41(6). doi:10.1093/sleep/zsy047
- Ogilvie RP, Patel SR. The epidemiology of sleep and diabetes. Curr Diab Rep. 2018;18(10):82. doi:10.1007/s11892-018-1055-8
- Jarrin DC, Alvaro PK, Bouchard MA, Jarrin SD, Drake CL, Morin CM. Insomnia and hypertension: a systematic review. Sleep Med Rev. 2018;41:3–38. doi:10.1016/j.smrv.2018.02.003
- Kubitz KA, Landers DM, Petruzzello SJ, Han M. The effects of acute and chronic exercise on sleep. A meta-analytic review. Sports Med. 1996;21(4):277–291. doi:10.2165/00007256-199621040-00004
- Youngstedt SD, O’Connor PJ, Dishman RK. The effects of acute exercise on sleep: a quantitative synthesis. Sleep. 1997;20(3):203–214. doi:10.1093/sleep/20.3.203
- Kredlow MA, Capozzoli MC, Hearon BA, Calkins AW, Otto MW. The effects of physical activity on sleep: a meta-analytic review. J Behav Med. 2015;38(3):427–449. doi:10.1007/s10865-015-9617-6
- Pedišić Ž, Dumuid D, Olds TS. Integrating sleep, sedentary behaviour, and physical activity research in the emerging field of time-use epidemiology definitions, concepts, statistical methods, theoretical framework, and future directions. Kinesiology. 2017;49(2):252–269.
- Cerin E, Leslie E, Sugiyama T, Owen N. Perceived barriers to leisure-time physical activity in adults: an ecological perspective. J Phys Act Health. 2010;7(4):451–459. doi:10.1123/jpah.7.4.451
- Miller DJ, Sargent C, Roach GD, Scanlan AT, Vincent GE, Lastella M. Moderate-intensity exercise performed in the evening does not impair sleep in healthy males. Eur J Sport Sci. 2020;20(1):80–89. doi:10.1080/17461391.2019.1611934
- American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago: American Academy of Sleep Medicine; 2001. Available from: https://cir.nii.ac.jp/crid/1571135650687048576. Accessed June 13, 2022.
- Buman MP, Phillips BA, Youngstedt SD, Kline CE, Hirshkowitz M. Does nighttime exercise really disturb sleep? Results from the 2013 national sleep foundation sleep in America Poll. Sleep Med. 2014;15(7):755–761. doi:10.1016/j.sleep.2014.01.008
- Dworak M, Wiater A, Alfer D, Stephan E, Hollmann W, Strüder HK. Increased slow wave sleep and reduced stage 2 sleep in children depending on exercise intensity. Sleep Med. 2008;9(3):266–272. doi:10.1016/j.sleep.2007.04.017
- Oda S, Shirakawa K. Sleep onset is disrupted following pre-sleep exercise that causes large physiological excitement at bedtime. Eur J Appl Physiol. 2014;114(9):1789–1799. doi:10.1007/s00421-014-2873-2
- Browman CP, Tepas DI. The effects of presleep activity on all-night sleep. Psychophysiology. 1976;13(6):536–540. doi:10.1111/j.1469-8986.1976.tb00876.x
- Ramos-Campo DJ, Ávila-Gandía V, Luque AJ, Rubio-Arias J. Effects of hour of training and exercise intensity on nocturnal autonomic modulation and sleep quality of amateur ultra-endurance runners. Physiol Behav. 2019;198:134–139. doi:10.1016/j.physbeh.2018.10.020
- Vlahoyiannis A, Aphamis G, Eddin DA, Giannaki CD. The effect of evening cycling at different intensities on sleep in healthy young adults with intermediate chronobiological phenotype: a randomized, cross-over trial. J Sports Sci. 2021;39(2):192–199. doi:10.1080/02640414.2020.1812194
- Thomas C, Jones H, Whitworth-Turner C, Louis J. High-intensity exercise in the evening does not disrupt sleep in endurance runners. Eur J Appl Physiol. 2020;120(2):359–368. doi:10.1007/s00421-019-04280-w
- Myllymäki T, Rusko H, Syväoja H, Juuti T, Kinnunen ML, Kyröläinen H. Effects of exercise intensity and duration on nocturnal heart rate variability and sleep quality. Eur J Appl Physiol. 2012;112(3):801–809. doi:10.1007/s00421-011-2034-9
- Frimpong E, Mograss M, Zvionow T, Dang-Vu TT. The effects of evening high-intensity exercise on sleep in healthy adults: a systematic review and meta-analysis. Sleep Med Rev. 2021;60:101535. doi:10.1016/j.smrv.2021.101535
- Stutz J, Eiholzer R, Spengler CM. Effects of evening exercise on sleep in healthy participants: a systematic review and meta-analysis. Sports Med. 2019;49(2):269–287. doi:10.1007/s40279-018-1015-0
- Mills EJ, Thorlund K, Ioannidis JPA. Demystifying trial networks and network meta-analysis. BMJ. 2013;346:f2914. doi:10.1136/bmj.f2914
- Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004;23(20):3105–3124. doi:10.1002/sim.1875
- Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–1359. doi:10.1249/MSS.0b013e318213fefb
- Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26(3):342–392. doi:10.1093/sleep/26.3.342
- Liang M, Pan Y, Zhong T, Zeng Y, Cheng ASK. Effects of aerobic, resistance, and combined exercise on metabolic syndrome parameters and cardiovascular risk factors: a systematic review and network meta-analysis. Rev Cardiovasc Med. 2021;22(4):1523. doi:10.31083/j.rcm2204156
- Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
- Liberati A, Altman DG and Tetzlaff J, et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ, 339(jul21 1), b2700–b2700. 10.1136/bmj.b2700
- Arias P, Madinabeitia-Mancebo E, Santiago M, Corral-Bergantinos Y, Robles-Garcia V. Effects of early or late-evening fatiguing physical activity on sleep quality in non-professional sportsmen. J Sports Med Phys Fitness. 2016;56(5):597–605.
- Aloulou A, Duforez F, Bieuzen F, Nedelec M. The effect of night‐time exercise on sleep architecture among well‐trained male endurance runners. J Sleep Res. 2020;29(6). doi:10.1111/jsr.12964
- Bulckaert A, Exadaktylos V, Haex B, De Valck E, Verbraecken J, Berckmans D. Elevated variance in heart rate during slow-wave sleep after late-night physical activity. Chronobiol Int. 2011;28(3):282–284. doi:10.3109/07420528.2011.552820
- Driver HS, Meintjes AF, Rogers GG, Shapiro CM. Submaximal exercise effects on sleep patterns in young women before and after an aerobic training programme. Acta Physiol Scand Suppl. 1988;574:8–13.
- Larsen P, Marino F, Melehan K, Guelfi KJ, Duffield R, Skein M. Evening high‐intensity interval exercise does not disrupt sleep or alter energy intake despite changes in acylated ghrelin in middle‐aged men. Exp Physiol. 2019;104(6):826–836. doi:10.1113/EP087455
- Miura A, Myouken S, Yamada M, et al. Effects of aerobic exercise in early evening on the following nocturnal sleep and its haemodynamic response. Res Sport Med. 2016;24(1):16–29. doi:10.1080/15438627.2015.1076415
- Myllymäki T, Kyröläinen H, Savolainen K, et al. Effects of vigorous late-night exercise on sleep quality and cardiac autonomic activity: late-night exercise and sleep. J Sleep Res. 2011;20(1pt2):146–153. doi:10.1111/j.1365-2869.2010.00874.x
- Park I, Díaz J, Matsumoto S, et al. Exercise improves the quality of slow-wave sleep by increasing slow-wave stability. Sci Rep. 2021;11(1):4410. doi:10.1038/s41598-021-83817-6
- Robey E, Dawson B, Halson S, et al. Effect of evening postexercise cold water immersion on subsequent sleep. Med Sci Sports Exerc. 2013;45(7):1394–1402. doi:10.1249/MSS.0b013e318287f321
- Saidi O, Davenne D, Lehorgne C, Duche P. Effects of timing of moderate exercise in the evening on sleep and subsequent dietary intake in lean, young, healthy adults: randomized crossover study. Eur J Appl Physiol. 2020;120(7):1551–1562. doi:10.1007/s00421-020-04386-6
- Uçar C, Özgöçer T, Yildiz S. Late-night exercise affects the autonomic nervous system activity but not the hypothalamo-pituitary-adrenal axis in the next morning. J Sports Med Phys Fitness. 2017;58(1–2). doi:10.23736/S0022-4707.16.06766-9
- Vincent GE, Sargent C, Roach GD, et al. Exercise before bed does not impact sleep inertia in young healthy males. J Sleep Res. 2020;29(3):e12903. doi:10.1111/jsr.12903
- Vitale JA, Bonato M, Galasso L, et al. Sleep quality and high intensity interval training at two different times of day: a crossover study on the influence of the chronotype in male collegiate soccer players. Chronobiol Int. 2017;34(2):260–268. doi:10.1080/07420528.2016.1256301
- Yoshida H, Ishikawa T, Shiraishi F, Kobayashi T. Effects of the timing of exercise on the night sleep. Psychiatry Clin Neurosci. 1998;52(2):139–140. doi:10.1111/j.1440-1819.1998.tb00994.x
- Youngstedt SD, Kripke DF, Elliott JA. Is sleep disturbed by vigorous late-night exercise? Med Sci Sports Exerc. 1999;31(6):864–869. doi:10.1097/00005768-199906000-00015
- Yamanaka Y, Hashimoto S, Takasu NN, et al. Morning and evening physical exercise differentially regulate the autonomic nervous system during nocturnal sleep in humans. Am J Physiol Regul Integr Comp Physiol. 2015;309(9):R1112–R1121. doi:10.1152/ajpregu.00127.2015
- Flausino NH, Da Silva Prado JM, Queiroz SS, Tufik S, Mello MT. Physical exercise performed before bedtime improves the sleep pattern of healthy young good sleepers: exercising before bedtime and sleep pattern. Psychophysiol. 2012;49(2):186–192. doi:10.1111/j.1469-8986.2011.01300.x
- Kern W, Perras B, Wodick R, Fehm HL, Born J. Hormonal secretion during nighttime sleep indicating stress of daytime exercise. J Appl Physiol. 1995;79(5):1461–1468. doi:10.1152/jappl.1995.79.5.1461
- O’Connor PJ, Breus MJ, Youngstedt SD. Exercise-induced increase in core temperature does not disrupt a behavioral measure of sleep. Physiol Behav. 1998;64(3):213–217. doi:10.1016/S0031-9384(98)00049-3
- Wong SN, Halaki M, Chow CM. The effects of moderate to vigorous aerobic exercise on the sleep need of sedentary young adults. J Sports Sci. 2013;31(4):381–386. doi:10.1080/02640414.2012.733823
- Hayashi Y, Nishihira Y, Higashiura T, Usui S. The effects of different intensities of exercise on night sleep. Adv Exerc Sport Physiol. 2014;20(1):19–24.
- Assefa Z, Diaz-Abad M, Wickwire M, Scharf M. The Functions of Sleep. neuroscience. 2015;2(3):155–171. doi:10.3934/Neuroscience.2015.3.155
- Carskadon MA, Dement WC, Carskadon MA, Dement WC. Nocturnal determinants of daytime sleepiness. Sleep. 1982;5(suppl_2):S73–S81. doi:10.1093/sleep/5.S2.S73
- Svensson T, Saito E, Svensson AK, et al. Association of sleep duration with all- and major-cause mortality among adults in Japan, China, Singapore, and Korea. JAMA Netw Open. 2021;4(9):e2122837. doi:10.1001/jamanetworkopen.2021.22837
- Goelema MS, Regis M, Haakma R, van den Heuvel ER, Markopoulos P, Overeem S. Determinants of perceived sleep quality in normal sleepers. Behav Sleep Med. 2019;17(4):388–397. doi:10.1080/15402002.2017.1376205
- Halson SL, Johnston RD, Appaneal RN, et al. Sleep quality in elite athletes: normative values, reliability and understanding contributors to poor sleep. Sports Med. 2022;52(2):417–426. doi:10.1007/s40279-021-01555-1
- Dew MA, Hoch CC, Buysse DJ, et al. Healthy older adults’ sleep predicts all-cause mortality at 4 to 19 years of follow-up: psychosomatic medicine. Mol Cell Proteomics. 2003;65(1):63–73. doi:10.1097/01.PSY.0000039756.23250.7C
- Obal F, Krueger JM. GHRH and sleep. Sleep Med Rev. 2004;8(5):367–377. doi:10.1016/j.smrv.2004.03.005
- Driver HS, Taylor SR. Exercise and sleep. Sleep Med Rev. 2000;4(4):387–402. doi:10.1053/smrv.2000.0110
- Lucidi F, Devoto A, Violani C, De Gennaro L, Mastracci P, Bertini M. Rapid eye movements density as a measure of sleep need: REM density decreases linearly with the reduction of prior sleep duration. Electroencephalogr Clin Neurophysiol. 1996;99(6):556–561. doi:10.1016/S0013-4694(96)95671-0
- Netzer NC, Kristo D, Steinle H, Lehmann M, Strohl KP. REM sleep and catecholamine excretion: a study in elite athletes. Eur J Appl Physiol. 2001;84(6):521–526. doi:10.1007/s004210100383
- Boutcher SH. High-intensity intermittent exercise and fat loss. J Obes. 2011;2011:868305. doi:10.1155/2011/868305
- Lewis PB, Ruby D, Bush-Joseph CA. Muscle soreness and delayed-onset muscle soreness. Clin Sports Med. 2012;31(2):255–262. doi:10.1016/j.csm.2011.09.009
- MacIntyre DL, Reid WD, McKenzie DC. Delayed muscle soreness: the inflammatory response to muscle injury and its clinical implications. Sports Med. 1995;20(1):24–40. doi:10.2165/00007256-199520010-00003
- Nieman DC, Luo B, Dréau D, et al. Immune and inflammation responses to a 3-day period of intensified running versus cycling. Brain Behav Immun. 2014;39:180–185. doi:10.1016/j.bbi.2013.09.004
- Fullagar H, Skorski S, Duffield R, Meyer T. The effect of an acute sleep hygiene strategy following a late-night soccer match on recovery of players. Chronobiol Int. 2016;33(5):490–505. doi:10.3109/07420528.2016.1149190
- Glavin EE, Ceneus M, Chanowitz M, et al. Relationships between sleep, exercise timing, and chronotype in young adults. J Health Psychol. 2021;26(13):2636–2647. doi:10.1177/1359105320926530
- McGinty D, Szymusiak R. Keeping cool: a hypothesis about the mechanisms and functions of slow-wave sleep. Trends Neurosci. 1990;13(12):480–487. doi:10.1016/0166-2236(90)90081-K
- Adam K, Oswald I. Protein synthesis, bodily renewal and the sleep-wake cycle. Clin Sci. 1983;65(6):561–567. doi:10.1042/cs0650561
- Berger RJ, Phillips NH. Comparative aspects of energy metabolism, body temperature and sleep. Acta Physiol Scand Suppl. 1988;574:21–27.
- Horne JA, Moore VJ. Sleep EEG effects of exercise with and without additional body cooling. Electroencephalogr Clin Neurophysiol. 1985;60(1):33–38. doi:10.1016/0013-4694(85)90948-4
- Horne JA, Staff LH. Exercise and sleep: body-heating effects. Sleep. 1983;6(1):36–46. doi:10.1093/sleep/6.1.36
- Van Dongen HPA, Dinges DF. Circadian rhythms in fatigue, alertness and performance. Principle Pract Sleep Med. 2000;20:391–399.
- Murphy PJ, Campbell SS. Nighttime drop in body temperature: a physiological trigger for sleep onset? Sleep. 1997;20(7):505–511. doi:10.1093/sleep/20.7.505
- Buxton OM, Lee CW, L’Hermite-Baleriaux M, Turek FW, Van Cauter E. Exercise elicits phase shifts and acute alterations of melatonin that vary with circadian phase. Am J Physiol Regul Integr Comp Physiol. 2003;284(3):R714–R724. doi:10.1152/ajpregu.00355.2002
- Miyazaki T, Hashimoto S, Masubuchi S, Honma S, Honma KI. Phase-advance shifts of human circadian pacemaker are accelerated by daytime physical exercise. Am J Physiol Regul Integr Comp Physiol. 2001;281(1):R197–R205. doi:10.1152/ajpregu.2001.281.1.R197
- Youngstedt SD. Ceiling and floor effects in sleep research. Sleep Med Rev. 2003;7(4):351–365. doi:10.1053/smrv.2001.0239