
Abstract
Introduction
Melatonin, secreted by the pineal gland during the night phase, is a regulator of the biological clock and sleep tendency. Totally blind subjects frequently report severe, periodic sleep problems, with 50%–75% of cases displaying non-24-hour sleep–wake disorder (N24HSWD) due to inability to synchronize with the environmental day–night cycle. Melatonin immediate-release preparations are reportedly effective in N24HSWD. Here, we studied the efficacy and safety of prolonged-release melatonin (PRM), a registered drug for insomnia, for sleep disorders in totally blind subjects living in normal social environments. The primary endpoint was demonstration of clinically meaningful effects on sleep duration (upper confidence interval [CI] limit >20 minutes whether significant or not) to allow early decision-making on further drug development in this indication.
Trial registration
ClinicalTrials.gov registry – NCT00972075.
Methods
In a randomized, double-blind, placebo-controlled proof-of-principle study, 13 totally blind subjects had 2 weeks’ placebo run-in, 6 weeks’ randomized (1:1) PRM (Circadin®) or placebo nightly, and 2 weeks’ placebo run-out. Outcome measures included daily voice recorded sleep diary, Clinical Global Impression of Change (CGIC), WHO-Five Well-being Index (WHO-5), and safety.
Results
Mean nightly sleep duration improved by 43 minutes in the PRM and 16 minutes in the placebo group (mean difference: 27 minutes, 95% CI: −14.4 to 69 minutes; P=0.18; effect size: 0.82) meeting the primary endpoint. Mean sleep latency decreased by 29 minutes with PRM over placebo (P=0.13; effect size: 0.92) and nap duration decreased in the PRM but not placebo group. The variability in sleep onset/offset and latency tended to decrease during PRM but not placebo treatment. The potentially beneficial effects of PRM persisted during the 2 weeks of discontinuation period, consistent with clock stabilizing effects. PRM was well-tolerated, adverse events were of mild or moderate severity and similar between PRM and placebo.
Conclusion
Nightly use of PRM may potentially improve patient-reported sleep difficulties in totally blind individuals trying to adhere to normal social lifestyle. A larger study powered to demonstrate a statistically significant effect is warranted.
Introduction
The 24-hour rhythm in sleep and wakefulness is regulated by an intrinsic body clock – the suprachiasmatic nucleus (SCN) within the brain that controls the timing of sleep and wake and thereby prepares for the upcoming period of activity.Citation1 The individual period of the endogenous clock is usually longer than 24 hours (average 24.2 hours) and is normally entrained (synchronized) by the daily light–dark cycle to match the environmental 24-hour day.Citation2 The light cues that are necessary for entrainment are perceived by the retina.Citation3 Approximately 55%–70% of totally blind patients are thought to have non-entrained rhythms and if they report periodic difficulties with sleep or daytime alertness, they are diagnosed as having non-24-hour (‘free running’) sleep–wake disorder (N24HSWD).Citation4 In N24HSWD, the free-running sleep–wake rhythm reflects the intrinsic oscillation of the circadian pacemaker and passes periodically out of phase with the social time for sleep and wake.Citation5–Citation9 The rest of totally blind individuals entrain at a normal or abnormal phase in relation to the social day,Citation4,Citation10–Citation12 with a minority of these patients being entrained by light.Citation13–Citation15
Totally blind individuals with abnormal phase or non-entrained rhythms encounter great difficulties when trying to maintain a lifestyle within the societal norm. When forcing themselves into sleep at night, they will experience periods of difficulty initiating sleep at night and waking up in the morning and periods of premature sleep onset with early awakenings. In sleep laboratory assessments, these subjects had significantly lower total sleep time and sleep efficiency (P=0.0001 for both) compared to age-matched, sighted, healthy subjects.Citation9
Melatonin is released from the pineal gland in close association with the light–dark cycle. In sighted humans, melatonin secretion is halted during the light phase and is induced in the evening to reach a peak in the middle of the night.Citation16 Melatonin is involved in the regulation of sleep in two ways: it facilitates synchronization of the circadian clock with the ambient day–night cycle (chronobiotic) and attenuates the wake-promoting signal of the circadian system (soporific).Citation17 During nighttime, there is an increase in endogenous melatonin secretion, which results in higher propensity for sleep. Sleep onset will normally occur 2 hours after the onset of the endogenous melatonin, usually 14 hours after spontaneous wake-up in the morning.Citation18,Citation19 In a totally blind person with N24HSWD, melatonin production will drift continuously through the night and daytime phases. The daytime production of melatonin is associated with daytime naps and difficulty sleeping at night in these patients.Citation20,Citation21
Since melatonin has beneficial effects on sleep in addition to its ability to entrain free-running rhythms to a 24-hour day, melatonin therapy is a rational approach for sleep disorders in the totally blind population.Citation5,Citation7 The administration of melatonin (0.5–10 mg, once daily in the evening for 1 day up to several months) to totally blind individuals with N24HSWD facilitated phase advances and entrainment to the societal sleep/wake norms.Citation20,Citation22–Citation25 In addition, melatonin therapy was reportedly able to entrain endogenous melatonin and cortisol rhythms to the 24-hour cycle.Citation20,Citation22,Citation24,Citation25
A melatonin receptor agonist, tasimelteon, was recently approved by the US Food and Drug Administration (FDA) for the treatment of N24HSWD in the blind.Citation26 The clinical benefit to the patients in terms of ease to fall asleep and total sleep time has however not been rigorously addressed and no data from double-blind placebo-controlled randomized studies are currently available.
Melatonin is rapidly metabolized by the liver (half-life ∼40 minutes). Because a short-term increase in melatonin was believed to best facilitate phase shifts in humans, studies in N24HSWD typically used immediate-release melatonin formulations.Citation20,Citation22,Citation24,Citation25,Citation27 Recent studies, however, suggest that modified-release preparations can be as effective for insomnia, as well as for phase resetting in sighted individuals,Citation28–Citation30 but such formulations have not yet been tested in N24HSWD. A prolonged-release melatonin (PRM) formulation (Circadin® 2 mg) is approved for insomnia in many countries.Citation31–Citation33 It was therefore pertinent to ask whether PRM would be effective for sleep disorders in totally blind patients.
The aim of this placebo-controlled randomized study was to evaluate the efficacy and safety of PRM in improving night sleep duration in totally blind subjects living in the community with periodic sleep difficulties while maintaining their habitual lifestyle. It was assumed that due to its potential effects on the biological clock, beneficial effects of PRM, should they exist, would reduce fluctuations in sleep onset/offset times and potentially persist for some time after drug discontinuation.
Materials and methods
Patients and procedures
This was a multi-center, double-blind, placebo-controlled study of a once-daily PRM (Circadin® 2 mg) dose in totally blind subjects with periodic sleep disorders. The study was performed in four centers in the US, under written approval from the appropriate local site’s Independent Ethics Committee/Institutional Review Board (IEC, Helsinki Committee/IRB; ClinicalTrials.gov website registry NCT00972075).
Male or female subjects aged 20–80 years, who had no conscious perception of light (as confirmed by electroretinography) were recruited. Subjects had to meet the criteria for diagnosis of periodic sleep difficulty in the clinical setting: 1) difficulty initiating sleep or difficulty in awakening, with average total night sleep duration <6 hours per night; 2) progressive delays of sleep phase, with inability to maintain entrainment to 24-hour day; and 3) presence of this sleep pattern for at least 6 weeks. Subjects with medical disorders other than those related to blindness and medical treatments that may have influenced melatonin production, sleep or alertness, as ascertained by medical history, were excluded. Use of melatonin during the preceding 2 weeks and use of benzodiazepines or other hypnotics during the study and the preceding 2 weeks or five half-lives, whichever was longer, and throughout the study, was prohibited. All participants signed the Informed Consent form approved by their institutional Ethics Committees.
Some authors from studies of melatonin in the blind have suggested that the time at which the first dosing of melatonin occurs within the individual circadian cycle is critical for entrainment,Citation20 whereas others have suggested that eventual entrainment of the human circadian pacemaker by melatonin is independent of the circadian phase of treatment initiation.Citation25 We chose to start dosing close to enrollment as would be the case in clinical practice. Patients were initially treated with placebo for 2 weeks and then were randomly assigned in a 1:1 ratio to receive PRM 2 mg or placebo for 6 weeks followed by a 2-week washout period. They were instructed to take the study drugs between 9 pm–10 pm and to keep bedtime hours every day between 11 pm–7 am. During the entire study period, daily diary recordings were performed in the morning via an Interactive Voice Response System (IVRS). The IVRS called the subjects every day at a pre-specified time after they got up in the morning and the subjects answered questions related to the previous night’s sleep and daytime napping. The Clinical Global Impression of Change (CGIC; severity of illness score and global improvement score) was evaluated by the investigator during each study visit. WHO-Five Well-being Index (WHO-5) was assessed by the subject and completed by the investigator at each study visit.
Safety and tolerability were assessed with physical examinations, vital signs, clinical laboratory tests (hematology, chemistry, and urinalysis), electrocardiogram (ECG), and adverse events (AEs) assessment. An AE was defined as any noxious, pathological, or unintended change in anatomical, physiological, or metabolic functions as indicated by physical signs, symptoms and/or laboratory changes, or spontaneous reports, whether associated with the study drug, and whether or not considered drug-related. Pulse, blood pressure, and body temperature were collected at each study visit. In addition, the investigator or qualified designee performed a complete physical examination.
Determination of sample size
Based on previous studiesCitation20 that reported mean + standard deviation (SD) total sleep time of 5.99±0.88 hours in placebo treated and 6.64±1.11 in melatonin treated totally blind subjects groups, 21 subjects per group (42 total) would be required to have at least an 80% chance of detecting a significant difference between the groups at the 0.1 significance level. N24HSWD in totally blind subjects is an orphan disease. Therefore, the number of patients available for trials is very limited. From previous reports in the scientific literature, significant changes in sleep duration between baseline and treatment conditions were observed in groups of 1–10 patients. It was thus decided that 14 patients (seven subjects per group) would be recruited to a pilot study to evaluate the mean and variance in treatment effects. At the planned sample size, we did not expect clinical significance of the difference between the PRM and placebo groups. To allow early decision-making on further development of PRM for this indication, we decided to use, as proposed in a number of studies, the upper limit of 95% confidence intervals (CIs) to help decide if a particular statistical result (whether significant or not) may be of relevance in practice.Citation34,Citation35 Total sleep time values (polysomnography) reported in this patient population were 290 + 80 minutesCitation9 and 314 + 32 minutes.Citation23 In patient-reported assessments, a mean total night sleep duration in this population was 5.99 + 0.88 hours (359.4 + 53 minutes).Citation20 For a baseline value of total sleep time of <390 minutes, we considered an increase in sleep duration of 20 minutes to be clinically relevant.
Statistical analyses
All analyses were performed using SAS® (v8.2 or later; SAS Institute Inc., Cary, NC, USA). The safety population included all subjects who were randomized and received at least one dose of study medication. The full analysis set (FAS) included all subjects in the safety population who satisfied all major entry criteria, and had efficacy data for the primary parameter recorded for at least one post run-in period assessment. Mean and CI values of the diary recorded sleep and morning alertness variables were summarized on a weekly basis in the last 2 weeks of the double-blind period and the 2 weeks of the washout period. The mean rate of change per week in the recorded parameters was calculated for the two randomization groups.
Efficacy analyses
Efficacy assessments included total night sleep duration, sleep latency, sleep onset/offset times, sleep maintenance, sleep quality, feeling upon awakening, morning alertness, and number and duration of naps assessed by a diary via daily recorded telephone calls to a study IVRS. Efficacy assessments also included CGIC and the WHO-5.
The primary efficacy variable was total night sleep duration assessed by daily-recorded telephone calls to an IVRS. A descriptive summary was provided with respect to actual values for baseline (weeks 1–2) and the last 2 weeks of the treatment period (weeks 7–8), change from baseline (weeks 1–2), to the last 2 weeks of the treatment period (weeks 7–8) as well as mean and 95% CI values of the difference of change in total night sleep duration during the last 2 weeks of the 6-week randomized treatment period and the 2 baseline weeks in the two groups. The differences of change from baseline in total night sleep duration to the last 2 weeks of the treatment period was compared between the PRM and placebo groups using one-way analysis of variance (ANOVA). Because of the planned sample size, statistical significance of the difference between the drug and placebo groups (parallel groups) was not expected in this pilot study. In line with GreenhalghCitation34 and Fethney,Citation35 the primary endpoint was demonstration of clinically meaningful effects on sleep duration as evidenced by a treatment effect upper CI limit >20 minutes (whether significant or not).
For the secondary efficacy measures, descriptive summary statistics (n, mean, SD, median, minimum, and maximum) were provided and compared using 95% CI from one-way ANOVA for daily diary records of sleep onset/offset times, sleep latency, sleep maintenance (how many times did you wake up in the night?), sleep quality, number of naps, total duration of naps, feeling upon awakening, and morning alertness for the baseline period (weeks 1–2), the last 2 weeks of the treatment period (weeks 7–8), the washout period (weeks 9 and 10), and changes from baseline, weekly basis in the last week of the treatment period (week 8), the 2 weeks of the washout period (weeks 9 and 10), and change from week 8 to weeks 9 and 10. WHO-5 Well-being Index score and CGIC score for severity of illness and global improvement were compared at baseline (Visit 2), end of randomized treatment, and washout period.
For post-hoc analyses, we calculated the mean standard deviations in the various sleep parameters during the last 2 weeks in each treatment period and compared the variability between baseline and treatment periods in the PRM and placebo groups.
Safety analysis
Descriptive statistics were provided for AEs, change in physical examination parameters, and vital signs. The number of subjects taking concomitant medications during the 6-week treatment period was summarized by WHO drug classification code for each treatment group. AEs were coded using the MedDRA Dictionary (v10.0). The change in laboratory parameters from screening (Visit 1) to the end of the 6-week treatment period (Visit 3) was summarized using shift tables to show the number of subjects having values below, within, and above the normal range for each assessment by treatment group. The change in physical examination parameters from baseline (Visit 2) to the end of the 6-week treatment and washout period (Visit 3) was summarized as the number of subjects who had a normal or abnormal examination at each assessment for each treatment group separately. Vital signs were summarized at baseline (Visit 2), the end of the 6-week treatment period (Visit 3), and at the end of the washout period (Visit 4) in actual values and change from baseline in the melatonin and placebo groups using descriptive statistics.
Results
A total of 25 patients were screened, of whom 13 were confirmed to be totally blind according to electroretinography and were randomized, with five subjects in the PRM group and eight subjects in the placebo group. All 13 subjects completed the study. Subject disposition is presented in . More of the subjects were female (61.5%), the majority of the subjects (76.9%) were Caucasian, and the rest were black (one in the PRM and two in the placebo groups), ranging in age from 37–67 years. Of the 13 enrolled subjects, all 13 (100%) were included in the safety population and the FAS. There were no systematic differences in demographic variables between the PRM and placebo groups ().
Figure 1 Overall study patient disposition.
Abbreviations: FAS, full analysis set; PRM, prolonged-release melatonin.
Table 1 Demographics and caffeine/alcohol history for safety population
Total sleep duration
The primary efficacy variable was total night sleep time assessed by a diary via daily-recorded telephone calls to an IVRS. The mean change from baseline to end of treatment in total night sleep duration for the PRM 2 mg group was 0.72±0.699 (95% CI: −0.14 to 1.59) hours (43 minutes) and for the placebo group it was 0.27±0.449 (95% CI: −0.11 to 0.64) hours (16.2 minutes) with a mean difference between groups of 27 minutes (P=0.18; 95% CI: −0.24 to 1.15 hours; effect size: 0.82; ). The upper limit of the 95% CI of the difference between PRM and placebo treatment effects on total sleep duration was 1.15 hours (69 minutes), namely larger than the predefined difference of 20 minutes, thus meeting the primary endpoint. No systematic difference was observed between the groups at baseline in the FAS population (). In the PRM group, despite the small sample, sleep duration under treatment was significantly longer at the 0.1 level of significance than at baseline (P=0.08). No such improvement was found in the placebo-treated group (P=0.232). Individual changes from baseline to end of treatment in total nighttime sleep duration for the PRM and placebo groups are also depicted (). Four of the five individuals in the PRM group showed >30 minutes of improvement in sleep duration and none had clinically meaningful deterioration, whereas in the placebo group, only two of the eight subjects improved by >30 minutes, and one deteriorated (). In the washout period, the total night sleep duration was still longer in the PRM than the placebo-treated group, suggesting persistence of the effects beyond the active treatment period ().
Figure 2 Endpoint of sleep variables: sleep duration.
Abbreviations: PRM, prolonged-release melatonin; SEM, standard error of the mean; WO, washout.
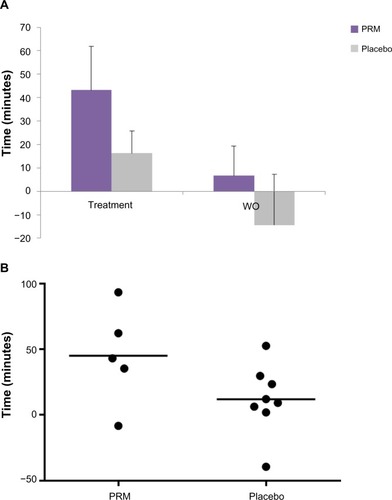
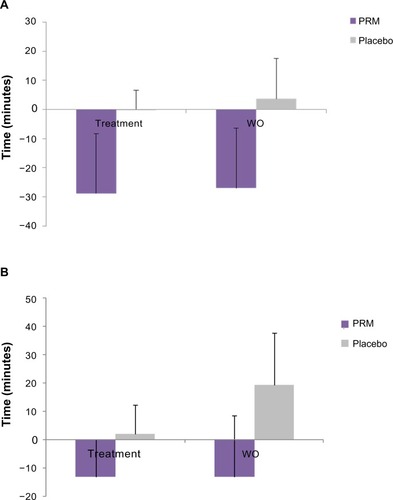
Figure 3 Endpoint of sleep variables: sleep latency and daytime naps.
Abbreviations: PRM, prolonged-release melatonin; SEM, standard error of the mean; WO, washout.
Sleep latency
Sleep latency was defined as the answer to the question ‘how long did it take you to fall asleep last night?’ as assessed by telephone calls to an IVRS. The mean change from baseline to end of treatment for sleep latency (measured in hours), was −0.48±0.765 (−28.8 minutes; 95% CI: −1.43 to 0.46) for the PRM group and −0.001±0.314 (−0.06 minutes; 95% CI: −0.26 to 0.26) for the placebo group (). There was a mean difference of 29 minutes between the PRM- and placebo-treated groups that did not reach statistical significance at this sample size (P=0.13; ). During the washout period, the mean difference from baseline to discontinuation in sleep latency for the PRM group was −0.45±0.766 (95% CI: −1.40 to 0.50) hours (−27 minutes) and for the placebo group, it was 0.062±0.6523 (95% CI: −0.48 to 0.61) hours (+3.7 minutes; ).
Sleep onset/offset time
Sleep onset was the time subjects started trying to fall asleep. The results demonstrated a slight change in sleep onset time for subjects in the PRM group (8 minutes earlier) and no change for the placebo group. Essentially, there was no difference between the groups.
Sleep offset was the time subjects woke up. The results demonstrated a delay in sleep offset time for PRM subjects (37 minutes later) and advance for placebo (8 minutes earlier). Because total sleep time is a main complaint in the patients, the delay in sleep offset of 37 minutes represented an improvement, which was consistent with the improvement in total sleep time. There was a mean difference of 45 minutes in total sleep time between the PRM- and placebo-treated groups that showed a trend for a significant improvement (P=0.11; data not shown).
Number and duration of daytime naps
At baseline, the mean number of daytime naps was not high for either group. Nevertheless, mean duration of naps in the PRM group demonstrated an improvement (reduction) at the end of treatment of 13 minutes compared to 2 minutes increase in mean nap duration in the placebo group. This effect was maintained during discontinuation for the PRM group, with a mean decrease from baseline to washout of 13 minutes, while in the placebo group, the mean duration of naps increased by 19 minutes from baseline values, demonstrating continued improvement in total duration of naps for the PRM subjects but not for the placebo subjects ().
CGIC and WHO-5 did not show differences between the two groups.
Onset and offset of treatment effects
Mean sleep duration and sleep latency by study week are presented in . As can be seen in , sleep duration increased at each time point in the PRM treated group reaching a peak at week 6, whereas the placebo treated group did not show the same trend. The mean sleep duration in the PRM-treated group showed a gradual decline toward baseline levels, but by the end of the discontinuation period (weeks 9 and 10) it was still better than that in the placebo group, suggesting persistence of the effect beyond the active treatment period ().
Figure 4 Onset and offset of treatment effects on sleep.
Abbreviations: PRM, prolonged-release melatonin; BL, baseline; SEM, standard error of the mean; WO, washout.
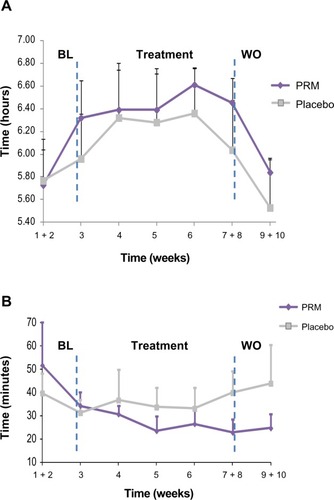
Mean week-by-week sleep latency values in the placebo group changed in a periodic manner, consistent with the cyclic nature of the sleep disorder. With PRM, the subject’s sleep latency demonstrated a gradual improvement (decrease), reaching a plateau level at week 5 (). The results after discontinuation showed gradual increase in sleep latency toward baseline values but continued to show shorter mean sleep latency values for the PRM-treated group but not for the placebo group, compared to baseline, demonstrating persistence of the effect beyond treatment ().
Variability in sleep parameters
To demonstrate stabilization in sleep phase, the variability among individual patients in sleep onset/offset and latency should decrease during treatment. The variability represented by the mean standard deviation (SD) in sleep parameters (eg, sleep onset/offset and sleep latency), during the last 2 weeks of the double-blind treatment period was compared to the variability during the 2-week placebo baseline period on a patient-by-patient basis (paired t-test; ).
Figure 5 Mean SD of the individual changes in sleep onset/offset and latency variability during baseline and the last 2 weeks of PRM and placebo treatment.
Abbreviations: PRM, prolonged-release melatonin; SD, standard deviation.
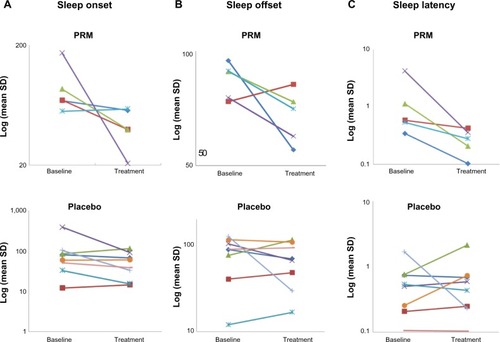
The mean SD of the sleep onset time values tended to decline with PRM treatment (P=0.078, N=5) but not with placebo treatment (P=0.12, N=8). As can be seen in , during treatment, variability in sleep onset decreased in four (80%) of the five patients in the PRM group and in four (50%) of the eight patients in the placebo group. The SD of the mean sleep offset time values declined significantly with PRM treatment (P=0.05, N=5), but not with placebo (P=0.19, N=8). As can be seen in , during treatment, the mean SD in sleep offset time decreased in four (80%) of five patients treated with PRM, and in four (50%) of those treated with placebo.
There was a similar trend in sleep latency: the mean SD of the sleep latency time values tended to decline with PRM treatment (P=0.099, N=5) but not with placebo treatment (P=0.44, N=8). As can be seen in , variability decreased in five out of five (100%) patients in the PRM-treated group but only four of eight (50%) in the placebo-treated group.
Safety
Of the 13 safety subjects, one (20%) PRM and two (25%) placebo subjects experienced one or more treatment-emergent AEs during the study. All of the AEs experienced were considered mild in severity and none led to study withdrawal. There were no serious AEs reported during the study, and there were no deaths. No clinically significant changes in physical examinations or vital signs were observed during the study. There were no distinct trends or clinically meaningful differences between treatment groups for any hematology and blood biochemistry and urinalysis parameters. No individual changes in hematology and blood biochemistry parameters were considered clinically significant.
The only drug-related clinically significant laboratory value reported during the study was in the placebo group. This subject had 3+ fold leukocytes present, which was considered to be clinically significant and reported as an AE. At a follow-up visit, the subject had trace leukocytes still present, but the finding was not considered to be clinically significant.
Discussion
The study provides preliminary evidence of beneficial effects of PRM on sleep duration and latency in totally blind subjects reporting disturbed sleep. The mean difference between the change from baseline in sleep duration in the PRM and placebo groups of 27 minutes is of relevance in practice and may justify a larger trial to confirm a significant treatment benefit. Another way of interpreting the study results is calculation of the effect size. Effect size is a name given to a family of indices that measure the magnitude of a treatment effect. Unlike significance tests, these indices are independent of sample size. Thus, this is a good measure for interpreting this trial with a limited sample size.Citation36 Accordingly, effect sizes are defined as ‘small, d=0.2’, ‘medium, d=0.5’, and ‘large, d=0.8’. For total sleep time, the mean change of 27 minutes over placebo represented an effect size (‘Cohen’s d’) of 0.82. This is a point estimate of effect size, and this estimate has a CI that we cannot calculate. Similarly, for sleep latency, the mean difference of 29 minutes between the groups represented an estimated effect size of 0.92. The estimated large effect sizes of PRM of 0.82 and 0.92 thus suggest a potentially strong treatment effect of PRM over that of placebo on total night sleep duration and sleep latency, respectively.
Three studies reported on the effects of regular melatonin formulations on sleep in totally blind subjects. Acute administration of regular-release melatonin 5 mg or placebo to 12 totally blind subjects for 1 hour before bedtime resulted in significantly longer mean total sleep time (by 89.8 minutes) and delayed sleep offset, recorded by polysomnography after melatonin, than placebo intake in the subjects, whereas sleep latency did not differ between the treatments.Citation23 In another study, repeated administration of regular-release melatonin 0.5 mg or placebo single-blind, to ten totally blind subjects daily at 9 pm (treatment duration varied between 26–81 days depending on the individuals’ circadian period) resulted in a significant increase in mean nighttime sleep duration (by 39 minutes), reduction in daytime nap number (by 0.33 naps per day on average), and mean nap duration (by 18.6 minutes) as recorded by daily sleep and nap diaries during the melatonin period compared to the placebo period. Mean sleep offset was delayed by 15 minutes, and there was no significant effect on sleep latency or onset.Citation20 In a third study, 10 mg melatonin or placebo was administered daily to seven totally blind free-running subjects 1 hour before their preferred bedtime for 3–9 weeks before being switched over to the other treatment; there was less time awake after sleep onset (77.5 minutes) and higher sleep efficiency (16.7%) as assessed by polysomnography by the end of the melatonin and placebo treatment periods, whereas total sleep time and sleep latency did not differ.Citation24 The results of the current study with PRM 2 mg for sleep in the totally blind subjects are thus consistent in nature and magnitude to those observed with 0.5 and 5 mg regular-release melatonin.
A limitation in our study is that we did not measure circadian variation in neuroendocrine markers, and we are thus unable to determine whether the improvement in sleep represents adjustment of the biological clock to the night phase. Nevertheless, there are some hints that there is a stabilization of the clock phase with PRM treatment. First, the changes in mean total sleep duration and sleep latency in the placebo group are consistent with the periodic nature of the sleep disorder in the study population. With PRM, the mean subjects’ sleep variables improved gradually with treatment time rather than improving immediately as would occur in the case of hypnotic drugs. Secondly, the variability in sleep onset/offset and sleep latency during the last 2 weeks of treatment declined in 80%–100% of patients treated with PRM but only 50% patients treated with placebo. Last but not least, the treatment effect did not dissipate immediately following discontinuation of PRM, but rather, declined gradually in the 2 weeks withdrawal period toward baseline values. Furthermore, there was a reduction in daytime napping, which is also consistent with better sleep at night and possibly also phase adjustment to the nightly melatonin signal.
These effects of PRM as demonstrated in the present study are compatible with melatonin’s effects at the biological clock to control circadian phase stability.Citation37–Citation39 It should be noted that the treatment period of 6 weeks might have been too short to attain synchronization in some patients.Citation25 Also, in our study, the ingested melatonin at treatment initiation did not coincide with the circadian phase, and some patients may have started the treatment when their endogenous phases were too far off the environmental night phase to allow effective response to melatonin.Citation20
Melatonin administration can elicit phase advances between 13 and 5 hours before sleep mid-point (essentially overlapping afternoon–evening hours) and phase delays between 5–7 hours after sleep mid-point (essentially overlapping the early morning hours).Citation30,Citation40–Citation43 While the phase-advancing effects of appropriately timed melatonin have been confirmed across many studies, the phase-delaying efficiency of morning melatonin ingestion is smaller and not as certain.Citation44
This is the first demonstration of efficacy of a PRM in totally blind persons. It adds to published data from studies in sighted subjects indicating that slow-release melatonin preparations are at least as effective as immediate-release preparations in phase shifting of the clock in healthy individuals kept in near darkness environmentCitation28,Citation29 and facilitating early circadian sleep in operational air transport aircrews.Citation45 In another study, modified- and slow-release melatonin preparations were found to be at least as effective as immediate-release preparations in advancing the clock phase under laboratory conditions mimicking eastward and westward travel.Citation30 Also, timed β1-adrenergic antagonists and PRM treatment was reported to reset the clock and restore sleep in a circadian disorder, Smith–Magenis syndrome.Citation46 Apparently, if the time of administration ‘hits’ the phase-advance period, PRM and immediate-release melatonin will both be effective even if PRM (which releases melatonin over 8 hours) is ‘spilling over’ this period, because melatonin does not phase shift the clock during the 8 hours night phase anyway. However, if the time of administration ‘hits’ the phase delay period, PRM but not immediate-release melatonin (which provides melatonin for ∼2 hours) will be able to counteract the phase delay effects, by ‘spilling over’ into the phase advance period of the clock on the very same day. Such studies extend the utility of PRM to the treatment of circadian rhythm sleep disorders.
Conclusion
Totally blind subjects with periodic sleep-wake disorder may potentially benefit from PRM given orally once daily between 9 pm–10 pm, in improving the patient-reported duration of sleep and sleep latency and attaining greater stability of sleep onset/offset times. Treatment effects appear to persist beyond the treatment phase into the withdrawal period, without rebound, consistent with stabilization of the circadian clock. Treatment with 2 mg daily of PRM was safe and well-tolerated in this group of patients. A larger study powered to demonstrate a statistically significant effect is warranted.
Author contributions
NZ and TN were responsible for the integrity of the work as a whole, from inception to the published article. NZ and TN made substantial contribution to the conception and design of the study and were involved in drafting the protocol, interpretation of data, and preparation of the manuscript. TR was a consultant and contributed to the interpretation of data and critical revision of the manuscript. All authors approve the final version.
Acknowledgments
The authors would like to acknowledge and thank the general practitioners Dr Alan Lankford and partners and Dr Russell Rosenberg and partners, who all managed the patients so admirably. They are also indebted to the research nurses and management staff of Premier Research Group Plc, without whom the study would not have taken place; we would especially like to thank the biostatisticians Rui Zhang and Li Qin who were responsible for the statistical plan and all statistical analyses. We would like to thank Best Practice for consulting and clinical monitoring.
Disclosure
The study was funded by Neurim Pharmaceuticals, Tel Aviv, Israel. TR has acted as a paid consultant to Neurim Pharmaceuticals. NZ and TN have disclosed that they are employees of Neurim Pharmaceuticals.
References
- MooreRYCircadian rhythms: basic neurobiology and clinical applicationsAnn Rev Med1997482532669046960
- CzeislerCADuffyJFShanahanTLStability, precision, and near-24-hour period of the human circadian pacemakerScience199928454232177218110381883
- CampbellSIs there an intrinsic period of the circadian clock?Science200028854691174117510841737
- SkeneDJLockleySWArendtJMelatonin in circadian sleep disorders in the blindBiol Signals Recept199981–2909510085469
- SackRLLewyAJCircadian rhythm sleep disorders: lessons from the blindSleep Med Rev20015318920612530986
- UchiyamaMShibuiKHayakawaTLarger phase angle between sleep propensity and melatonin rhythms in sighted humans with non-24-hour sleep-wake syndromeSleep2002251838811833864
- ZisapelNCircadian rhythm sleep disorders: pathophysiology and potential approaches to managementCNS Drugs200115431132811463135
- TabandehHLockleySWButteryRDisturbance of sleep in blindnessAm J Ophthalmol199812657077129822235
- LegerDGuilleminaultCSantosCPaillardMSleep/wake cycles in the dark: sleep recorded by polysomnography in 26 totally blind subjects compared to controlsClin Neurophysiol2002113101607161412350437
- LockleySWSkeneDJTabandehHBirdACDefranceRArendtJRelationship between napping and melatonin in the blindJ Biol Rhythms199712116259104687
- SackRLBloodMLLewyAJMelatonin rhythms in night shift workersSleep19921554344411455127
- LewyAJNewsomeDADifferent types of melatonin circadian secretory rhythms in some blind subjectsJ Clin Endocrinol Metab1983566110311076841552
- ZaidiFHHullJTPeirsonSNShort-wavelength light sensitivity of circadian, pupillary, and visual awareness in humans lacking an outer retinaCurr Biol200717242122212818082405
- KlermanEBShanahanTLBrotmanDJPhotic resetting of the human circadian pacemaker in the absence of conscious visionJ Biol Rhythms200217654855512465888
- CzeislerCAShanahanTLKlermanEBSuppression of melatonin secretion in some blind patients by exposure to bright lightN Engl J Med199533216117990870
- LewyAJWehrTAGoodwinFKNewsomeDAMarkeySPLight suppresses melatonin secretion in humansScience19802104475126712697434030
- WyattJKDijkDJRitz-de CeccoARondaJMCzeislerCASleep-facilitating effect of exogenous melatonin in healthy young men and women is circadian-phase dependentSleep200629560961816774150
- ShochatTLuboshitzkyRLaviePNocturnal melatonin onset is phase locked to the primary sleep gateAm J Physiol19972731 Pt 2R364R3709249573
- LewyAJThe dim light melatonin onset, melatonin assays and biological rhythm research in humansBiol Signals Recept199981–2798310085467
- HackLMLockleySWArendtJSkeneDJThe effects of low-dose 0.5-mg melatonin on the free-running circadian rhythms of blind subjectsJ Biol Rhythms200318542042914582858
- LockleySWSkeneDJButlerLJArendtJSleep and activity rhythms are related to circadian phase in the blindSleep199922561662310450596
- FolkardSArendtJAldhousMKennettHMelatonin stabilises sleep onset time in a blind man without entrainment of cortisol or temperature rhythmsNeurosci Lett199011321931982377316
- FischerSSmolnikRHermsMBornJFehmHLMelatonin acutely improves the neuroendocrine architecture of sleep in blind individualsJ Clin Endocrinol Metab200388115315532014602767
- SackRLBrandesRWKendallARLewyAJEntrainment of free-running circadian rhythms by melatonin in blind peopleN Engl J Med2000343151070107711027741
- LewyAJEmensJSBernertRALeflerBJEventual entrainment of the human circadian pacemaker by melatonin is independent of the circadian phase of treatment initiation: clinical implicationsJ Biol Rhythms2004191687514964705
- DhillonSClarkeMTasimelteon: first global approvalDrugs201474450551124610704
- SackRLLewyAJBloodMLStevensonJKeithLDMelatonin administration to blind people: phase advances and entrainmentJ Biol Rhythms1991632492611773095
- RajaratnamSMDijkDJMiddletonBStoneBMArendtJMelatonin phase-shifts human circadian rhythms with no evidence of changes in the duration of endogenous melatonin secretion or the 24-hour production of reproductive hormonesJ Clin Endocrinol Metab20038894303430912970302
- RajaratnamSMMiddletonBStoneBMArendtJDijkDJMelatonin advances the circadian timing of EEG sleep and directly facilitates sleep without altering its duration in extended sleep opportunities in humansJ Physiol2004561Pt 133935115459246
- PaulMAMillerJCGrayGWLoveRJLiebermanHRArendtJMelatonin treatment for eastward and westward travel preparationPsychopharmacology (Berl)2010208337738620013115
- LemoinePZisapelNProlonged-release formulation of melatonin (Circadin) for the treatment of insomniaExpert Opin Pharmacother201213689590522429105
- CardinaliDPVidalMFVigoDENew developments in the treatment of primary insomnia in elderly patients:focus on prolonged-release melatoninChronophysiol Ther201226779
- WadeAGFordICrawfordGNightly treatment of primary insomnia with prolonged release melatonin for 6 months: a randomized placebo controlled trial on age and endogenous melatonin as predictors of efficacy and safetyBMC Med201085120712869
- GreenhalghTHow to read a paper. Statistics for the non-statistician. II: “Significant” relations and their pitfallsBMJ199731571054224259277611
- FethneyJStatistical and clinical significance, and how to use confidence intervals to help interpret bothAust Crit Care2010232939720347326
- CohenJStatistical Power Analysis for the Behavioral Sciences2ndHillsdale, NJLawrence Earlbaum Associates1988
- GubinDGGubinGDWaterhouseJWeinertDThe circadian body temperature rhythm in the elderly: effect of single daily melatonin dosingChronobiol Int200623363965816753947
- CzeislerCADumontMDuffyJFAssociation of sleep-wake habits in older people with changes in output of circadian pacemakerLancet199234088259339361357348
- CardinaliDPGarciaAPCanoPEsquifinoAIMelatonin role in experimental arthritisCurr Drug Targets Immune Endocr Metabol Disord20044111015032620
- LewyAJBauerVKAhmedSThe human phase response curve (PRC) to melatonin is about 12 hours out of phase with the PRC to lightChronobiol Int199815171839493716
- PaulMAMillerJCLoveRJLiebermanHBlazeskiSArendtJTiming light treatment for eastward and westward travel preparationChronobiol Int200926586789019637048
- RevellVLEastmanCIHow to trick mother nature into letting you fly around or stay up all nightJ Biol Rhythms200520435336516077154
- BurgessHJRevellVLMolinaTAEastmanCIHuman phase response curves to three days of daily melatonin: 0.5 mg versus 3.0 mgJ Clin Endocrinol Metab20109573325333120410229
- ArendtJSkeneDJMelatonin as a chronobioticSleep Med Rev200591253915649736
- PaulMAGrayGSardanaTMPigeauRAMelatonin and zopiclone as facilitators of early circadian sleep in operational air transport crewsAviat Space Environ Med200475543944315152897
- De LeersnyderHBressonJLde BloisMCBeta 1-adrenergic antagonists and melatonin reset the clock and restore sleep in a circadian disorder, Smith-Magenis syndromeJ Med Genet2003401747812525548