
Abstract
Objective
The objective of this study was to determine the risk of obesity and metabolic syndrome in adults with a history of juvenile arthritis (JA).
Methods
Using the National Health and Nutrition Examination Survey (NHANES), we compared the characteristics of respondents with arthritis (JA vs rheumatoid arthritis [RA]) to those of the control group without arthritis. We used logistic regression analyses, controlling for age, race, and gender, to determine the ORs for metabolic syndrome.
Results
Obesity was increased in the JA group with 67% respondents having body mass index ≥30 kg/m2 vs 55% respondents in the no arthritis cohort (p=0.004). In unadjusted analyses, there was increased odds of metabolic syndrome in JA (OR 6.2, p=0.001) and RA groups compared to those without arthritis (OR 7.7, p=0.001). After adjusting for age, gender, and race, the odds of metabolic syndrome remained increased in JA (OR 5.2, p=0.001) and RA (OR 3.2, p=0.001) groups.
Conclusion
Adults with a history of JA have a significantly increased risk of metabolic syndrome compared to those without arthritis. These findings are important because metabolic syndrome has been associated with an increased risk of cardiovascular disease and death in other populations.
Introduction
Juvenile arthritis (JA) is the most common chronic rheumatic disease in childhood.Citation1 Clinically, JA is defined as arthritis of unknown origin that manifests before the age of 16 years and persists for at least 6 weeks.Citation2 Although these children are known to be at risk for disease-specific complications, such as uveitis or limb length discrepancy, there are little data on long-term body composition and fitness in this cohort.
Adults diagnosed with rheumatoid arthritis (RA) are known to have an increased prevalence of metabolic syndrome defined as central obesity, dyslipidemia, hypertension, and hyperglycemia.Citation3–Citation7 When the specific components of metabolic syndrome were assessed, increased waist circumference, hypertension, and high fasting glucose levels were observed in established RA patients.Citation6,Citation7
Our goal was to examine the associations of JA with obesity and risk factors for metabolic syndrome using a large panel of nationally representative data.
Methods
The National Health and Nutrition Examination Survey (NHANES) is a probability sample survey of civilians in the USA, which includes noninstitutionalized people. Data on prevalence of diseases and comorbidities are collected via interviews, physical examinations, laboratory tests, and radiographs. The data are freely available via the Centers for Disease Control. We linked the 2007–2014 NHANES data sets to assess the weight, body mass index (BMI), physical activity, and laboratory results of children with arthritis.Citation8
Respondents with arthritis responded “yes” to the survey question: “Has a doctor or other health professional ever said you had arthritis?” We included respondents who reported RA or “other” type of arthritis; respondents with osteoarthritis and psoriatic arthritis were excluded. Our comparison group consisted of respondents who answered “no” to the arthritis survey question. We compared characteristics between respondents with arthritis, divided by age of arthritis diagnosis. JA was defined as arthritis diagnosed when ≤16 years old, and RA was defined as arthritis diagnosed when aged >16 years.Citation2 For the comparison group, we selected a random sample from respondents without arthritis in a 4:1 ratio to those with arthritis.
Hypertension was defined as “yes” to the survey question: “Have you ever been told by a doctor or other health professional that you have hypertension, also called high blood pressure?” Diabetes was defined as “yes” to the survey question: “Have you ever been told by a doctor or other health professional that you have diabetes or sugar diabetes?” Normal BMI was defined as per the World Health Organization as 18.5–24.9 kg/m2, overweight as 25–29.9 kg/m2, and obesity as ≥30 kg/m2.Citation9 We also utilized the Stavropoulos-Kalinoglou cutoff classification points for BMI in RA patients for overweight as >23 kg/m2 and obesity as >28 kg/m2.Citation10 Laboratory results were obtained through NHANES sampling. Fasting blood results were reported for glucose, and results for C-reactive protein (CRP), total cholesterol, and direct high-density lipoprotein (HDL) were from nonfasting samples.
We used the US National Cholesterol Education Program Adult Treatment Panel III guidelines for metabolic syndrome, requiring at least three of the following: 1) central obesity defined as waist circumference ≥102 cm or 40 inches for males and ≥88 cm or 35 inches for females; 2) hypertension defined as blood pressure ≥130/85 mmHg (or treated for hypertension); 3) dyslipidemia defined as triglycerides ≥150 mg/dL or HDL <40 mg/dL for males and <50 mg/dL for females; and 4) fasting plasma glucose ≥110 mg/dL.Citation11
We conducted analyses using Stata, version 11.2 (Stata-Corp LP, College Station, TX, USA) and used the survey commands provided to account for the complex sampling design. We used the NHANES sample weights that took into account the unequal selection probabilities resulting from the cluster design and planned oversampling of certain subgroups. All analyses reported incorporated these sample weights. Logistic regression analyses, controlling for age, race, and gender, were used to determine the ORs for metabolic syndrome. p-values <0.05 were considered as significant. This study was exempted from the review of the institutional review board because the data were de-identified.
Results
There were 38,909 total respondents. After the 4:1 control to arthritis random selection, there were a total of 22,807 participants in the data set. There were 232 respondents who reported a diagnosis of arthritis ≤16 years old (JA) and 1,028 randomly selected respondents with no arthritis (). At the time of the NHANES, the respondents with JA were older than those without arthritis (47.7 vs 43.7 years, p=0.001). Respondents with JA were heavier than those without arthritis (BMI 30.2 vs 28.2 kg/m2, p=0.006), and obesity was increased in the JA group with 67% having BMI ≥30 kg/m2 vs 55% in the no arthritis cohort (p=0.004). There was significantly more hypertension and diabetes in the JA group compared to controls. The mean duration of JA was not recorded in the NHANES. The duration of hypertension from time of diagnosis to the time of survey was increased in the JA group compared to controls (14.3 vs 10 years, p=0.002). There was no significant difference in the duration of diabetes between JA and control groups (11.9 vs 11.3 years, p=0.8).
Table 1 Comparison of JA and no arthritis groups
We next compared respondents with JA to those with RA (). Despite being significantly younger at the time of the survey, respondents with JA were as obese as those with RA (79% JA vs 84% RA with BMI >28 kg/m2, p=0.07). There was an increased prevalence of hypertension and diabetes in the RA group compared to those with JA (). There was no significant difference in the time from hypertension diagnosis to time of survey (14.3 years in the JA group vs 14.3 years in the RA group, p=0.8) and no significant difference in diabetes duration (11.9 years in the JA group vs 12.7 years in the RA group, p=0.7). As shown in , metabolic syndrome varied by age in the different cohorts. There was no significant difference between JA and the no arthritis groups, but those with JA presented with metabolic syndrome at younger ages compared to those with RA.
Figure 1 Prevalence of metabolic syndrome by age and diagnosis.
Abbreviations: JA, juvenile arthritis; RA, rheumatoid arthritis.
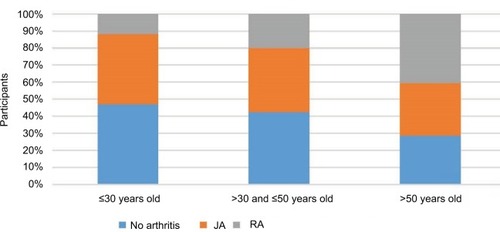
Table 2 Comparison of JA and RA groups
We performed logistic regression analyses to determine the odds of metabolic syndrome in those with JA and RA, using those with no arthritis as the referent population (). In unadjusted analyses, there was increased odds of metabolic syndrome in those with JA (OR 6.2, p=0.001) and RA compared to controls (OR 7.7, p=0.001). After adjusting for age, gender, and race, the odds of metabolic syndrome remained increased in those with JA (OR 5.2, p=0.001) and RA (OR 3.2, p=0.001).
Table 3 Odds of metabolic syndrome in JA and RA groups compared to the no arthritis group
We explored possible reasons for the increased obesity found in the JA group. There was no significant difference in physical activity between groups (3.7 days/week in the JA group, 3.3 days/week in the no arthritis group, and 3.6 days/week in the RA group, p=0.2). A surrogate for inflammation, CRP level, was collected from respondents during NHANES years 2007–2008 and 2009–2010. Respondents with JA had higher mean CRP levels compared to those without arthritis (0.6 mg/dL vs 0.3 mg/dL, p=0.001), but there was no significant difference between JA and RA groups (0.6 mg/dL vs 0.7 mg/dL, p=0.5).
Discussion
In this study, using the NHANES 2007–2014 annual survey data, we have shown that respondents with JA have increased odds of metabolic syndrome as well as increased obesity, waist circumference, hypertension, and diabetes compared to respondents without arthritis.
Several studies have demonstrated that children with JA have high obesity rates with increased fat mass compared to healthy age-matched peers.Citation12,Citation13 The etiology of this increased obesity is thought to be multifold with decreased physical activity, glucocorticoids, and increased disease activity all contributing.Citation12–Citation14 Our analyses have shown that this increased obesity persists into adulthood, despite adequate physical activity.
In the current study, only 37% of JA respondents had obtained CRP levels, but the trend showed increased levels compared to those without arthritis. In women with RA, increased truncal fat has been associated with elevated CRP levels.Citation15 This suggests that the trend of elevated CRP in JA noted in this study could be due to inherent inflammation or adiposity rather than complications from medication use.
In patients with RA, obesity is common.Citation4–Citation7,Citation15,Citation16 Increased inflammatory cytokines can also lead to changes in body composition such as loss of muscle mass and concomitant increase in fat mass, particularly abdominal adiposity.Citation15 In our study, the respondents with JA had increased waist/height ratios compared to those without arthritis, but there was no significant difference between RA and JA respondents. This is concerning because of the known risk of abdominal fat with cardiovascular disease. In a report by Giles et al,Citation16 higher levels of visceral abdominal fat in RA patients were associated with cardiometabolic risk factors including elevated fasting glucose, hypertension, and metabolic syndrome.
Our study has several limitations. NHANES uses patients’ self-reported diagnoses that may be an inaccurate way to define medical conditions, since a proportion of individuals may not seek medical care; therefore, these individuals may be underdiagnosed and uncounted in the final analyses. This is a concern for patients with few or no symptoms who may not yet be diagnosed with hypertension or metabolic syndrome. NHANES does not collect data on arthritis activity or joint exam, and we found no JA participants taking prednisone, methotrexate, or TNF alpha therapy. This raises a limitation of the accuracy of the information, either in diagnosis or treatment. Participants who reported a previous diagnosis of JA or RA may have been misdiagnosed by other health professionals. It has been reported that a diagnosis of RA by a primary care physician is often modified once evaluated by a rheumatologist.Citation17 Misclassification or recall bias may affect both the age and type of arthritis classification, impacting the numbers of respondents in each group. The strengths of our study include the use of the NHANES data set, which is based on a large, nationally representative survey of the US adult population.
Conclusion
We found that adults with a history of JA have sixfold increased risk of metabolic syndrome compared to those without arthritis. These findings are important because metabolic syndrome has been associated with an increased risk of cardiovascular disease and death in other populations, and adults with JA should be monitored closely for these complications.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors confirm that this manuscript has not been submitted elsewhere and that no portion of the data has been or will be published in proceedings or transactions of meetings or symposium volumes.
Disclosure
The authors report no conflicts of interest in this work.
References
- ThierrySFautrelBLemelleIGuilleminFPrevalence and incidence of juvenile idiopathic arthritis: a systematic reviewJoint Bone Spine201481211211724210707
- PettyRESouthwoodTRMannersPInternational League of Associations for RheumatologyInternational league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001J Rheumatol200431239039214760812
- DesseinPHStanwixAEJoffeBICardiovascular risk in rheumatoid arthritis versus osteoarthritis: acute phase response related decreased insulin sensitivity and high-density lipoprotein cholesterol as well as clustering of metabolic syndrome features in rheumatoid arthritisArthritis Res200245R512223108
- DesseinPHTobiasMVellerMGMetabolic syndrome and subclinical atherosclerosis in rheumatoid arthritisJ Rheumatol200633122425243217080519
- ChungCPOeserASolusJFPrevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosisAtherosclerosis2008196275676317266963
- da CunhaVRBrenolCVBrenolJCMetabolic syndrome prevalence is increased in rheumatoid arthritis patients and is associated with disease activityScand J Rheumatol201241318619122416768
- CrowsonCSMyasoedovaEDavisJM3rdIncreased prevalence of metabolic syndrome associated with rheumatoid arthritis in patients without clinical cardiovascular diseaseJ Rheumatol2011381293520952464
- Centers for Disease Control and PreventionNational Center for Health Statistics (NCHS) National Health and Nutrition Examination Survey DataHyattsvilleU.S. Department of Health and Human Services, Centers for Disease Control and Prevention20072014
- World Health OrganizationObesity: Preventing and Managing the Global Epidemic. Report of a WHO ConsultationWorld Health Organ Tech Rep Ser20008941253
- Stavropoulos-KalinoglouAMetsiosGSKoutedakisYKitasGDObesity in rheumatoid arthritisRheumatology201150345046220959355
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final reportCirculation2002106253143342112485966
- GuzmanJKerrTWardLMGrowth and weight gain in children with juvenile idiopathic arthritis: results from the ReACCh-Out cohortPediatr Rheumatol Online J2017151687928830457
- TakkenTvan der NetJKuisWHeldersPJPhysical activity and health related physical fitness in children with juvenile idiopathic arthritisAnn Rheum Dis200362988588912922964
- SchenckSNiewerthMSenlgerCPrevalence of overweight in children and adolescents with juvenile idiopathic arthritisScand J Rheumatol201544428829525742802
- GilesJTBartlettSJAndersenRThompsonRFontaineKRBathonJMAssociation of body fat with C-reactive protein in rheumatoid arthritisArthritis Rheum20085892632264118759279
- GilesJTAllisonMBlumenthalRSAbdominal adiposity in rheumatoid arthritisArthritis Rheum201062113173318220589684
- Gamez-NavaJIGonzalez-LopezLDavisPSuarez-AlmazorMEReferral and diagnosis of common rheumatic diseases by primary care physiciansBr J Rheumatol19983711121512199851272