Abstract
Background
Acanthamoeba keratitis (AK) is ever more frequently reported in industrialized countries. The loss of the corneal surface integrity consequent to secondary microtrauma produced by the use of contact lens (CL) favors the penetration of the parasite into the corneal tissue.
Objectives
A scientific review was performed to investigate the association of CL wear as an Acanthamoeba keratitis (AK) risk factor.
Methods
A computerized screening of 7834 Medline articles (4623 from PubMed; 3211 from Scopus) used a strict selection criteria of case-control studies involving CL wear and/or trauma.
Results
The search yielded five case-control studies published from 1995 to 2012. All studies included showed a statistically significant positive association between AK and CL use, with a combined odds ratio (OR) of 10.21 (95%, confidence intervals [CI]; 3.57–27.64).
Statistical analysis
All studies included showed a statistically significant positive association between AK and CL use, though with differing OR values.
Conclusion
Though rare, AK should be held in higher consideration when ophthalmologists are faced with CL users exhibiting simplex-like lesions associated with circular stromal infiltrates and disproportionate ocular pain in respect to the objective clinical picture.
Keywords:
Introduction
Keratitis is an infective process of the cornea which may lead to serious visual impairments.Citation1 The microbiological etiology of the disease is varied and may be of viral, mycotic, or parasitic origin.Citation2
Corneal parasitic infections, which were – up to recently – thought to be associated mostly with poor sociosanitary conditions, are ever more frequent in industrialized countries.Citation1,Citation3–Citation5
Acanthamoeba (A) is a resistant protozoan often found in proximity to freshwater or saltwater sources, in swimming pools, thermal baths, air-conditioning filters, and in contact lens (CL) cleansing solutions.Citation6–Citation8 The first observation of Acanthamoeba keratitis (AK) was reported by Nagington in 1974,Citation9 but it wasn’t until 1975 that a causal relationship between AK and A was reported by Visvesvara et al.Citation10 The species of Acanthamoeba that produces the most serious forms of keratitis in humans are Acanthamoeba castellanii, A. hatchetti, A. polyphaga, A. quina, and A. rhysodes.Citation11
Risk cofactors are particularly associated to the loss of the integrity of the corneal surface,Citation12 be it consequent to trauma or abrasions from an external contaminated object or a secondary microtrauma produced by the use of CL, which both favor the penetration of the parasite into the corneal tissue.Citation13 Moreover, even the exposure to environmental pollution could be associated to the developing of this keratitis, as reported by Lalitha et al.Citation14
There are wide differences in the incidence of the condition around the world and over time, which include the changing CL solution market and local environmental issues, such as water storage and disinfection.
Nevertheless, KA is still a health problem that needs to be clearly faced, according to Ibrahim et al.Citation15
The first phases of AK are characterized by fluctuating epithelial defects, epithelial opacity, pseudodendritis, and bulbar hyperaemia, symptoms which resemble the dendritic keratitis often seen with herpes simplex infection; and these symptoms produce intense eye pain.Citation16
The evolution of the infection causes a stromal ulceration, lysis, and the characteristic circular and perineural infiltrates of the stroma as typical markers of AK. The diagnosis of this condition must be made quickly, because it is a potentially devastating condition which, if untreated, may return even after surgical intervention.Citation17
Objectives
The aim of our study was to review the scientific literature regarding the association between CL use and AK, considering that the use of CL has become more widespread. We aimed to perform a pooled analysis of studies where the results could be combined. The main reason for this is to offer support for the development and communication of preventive strategies (technical brochures conveyed through territorial medicine and pharmacies), focused on implementing targeted educational programs among CL users. This awareness may help alert specialists about markers associated to an appropriate and early diagnosis of AK.
Methods
Identification of relevant studies
The Internet medical databases used for the search were PubMed and Scopus. On Medline and Scopus, we used the keywords “Acanthamoeba keratitis,” “contact lens,” “trauma,” and “case control” linked by the Boolean operators and/or applying the following two algorithms:Citation3 “Acanthamoeba keratitis,” and/or “contact lens,” and/or “case-control study;”Citation6 and “Acanthamoeba keratitis” and/or “contact lens” and/or “microtrauma.”
The identification of relevant studies was carried out within the time window from January 1995 to February 15, 2012, and was restricted to the English language. We only selected studies that clearly reported the following criteria – CL, trauma, and AK – that measured health outcomes on the basis of association measures (odds ratio [OR]). We excluded papers that did not meet these criteria.
Data extracted included first authors, publication year, nation, study design, sample size, OR of cases and controls, and 95% confidence intervals (CI).
Data extraction
To perform the review, we extracted data related to infection by Acanthamoeba keratitis in CL wearers. Extracted data regarded persistent infection, defined by the detection of ulcers in one or more consecutive medical control visits.
Statistical analysis
Pooled analysis was performed using the random-effects model, since heterogeneity was found between studies (P for homogeneity = 0.053). The pooled OR was calculated as the back-transformation of weighted mean of transformed ORs using DerSimonian–Laird weights.
Results
Identification of relevant studies
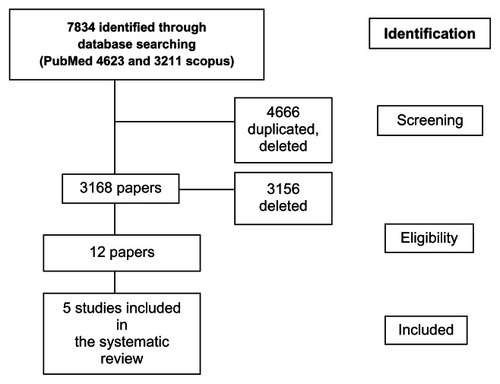
From Medline, we retrieved 7834 articles (4623 from PubMed and 3211 from Scopus). After sorting for duplicates, removing ineligible studies through PRISMA methods (Liberati et alCitation18), and screening for titles and abstracts, we were left with twelve eligible full-text articles. Moreover, after a first analysis, seven of these full-text papers were excluded because of the lack of data regarding the association measures we were most interested in. This criteria led to a strict selection of sorted articles. PubMed is a highly sensitive search tool and retrieves many articles, although in a much less selective way. If the same article was found in more than one database, it was only used once. The eligible papers were obtained as full text.
The process of data extraction was performed by two independent researchers.
In the end, five studies were included in the systematic review (). All studies were case-control studies published from 1995 to 2012.
Figure 1 Flow diagram of AK studies selected.
The sample size ranged from 89 to 714 individuals. Three studies were published in the USA, one in Italy, and one in the UK. The characteristics of each study are shown in .
Table 1 Results of case-control studies of keratitis caused by Acanthamoeba published from 1995 to 2012
ORs ranged from 3.57 (95%, CI; 1.86–6.87), Verani et al,Citation19 to 27.64 (95%, CI; 6.46–135.54), Radford et al.Citation20 The five selected studies analyzed all involved CL wearers who subsequently developed AK.
Statistical analysis
All studies included showed a statistically significant association between AK and CL use, though with different OR values: The study by Radford et al showed a statistically significant association with higher OR (OR = 27.64; 95%, CI; 6.46–135.54), while another three studies showed an association of more than 10 (Meier et alCitation21 [OR = 11; 95%, CI; 1.48–228.1], Joslin et alCitation22 [OR = 13.16; 95%, CI; 3.55–35.57], Pacella et alCitation23 [OR = 17.68; 95%, CI; 2.25–138.89]). In the remaining study, the OR value was less than 10 (Verani et alCitation19 [OR = 3.57; 95%, CI; 1.86–6.87]). Pooled OR scores produced a value of 10.21 (95%, CI; 4.01–25.99) and a P for homogeneity = 0.053.
Other relevant risk factors
According to the results from Joslin et al,Citation22 the reuse of solution more than five times per month is another CL significant risk factor for AK (at unconditional multivariate analysis OR = 4.20; 95%, CI; 1.25–14.10). Moreover, additional hygiene-related variables, such as lack of “rubbing” and showering with CL, as well as ocular traumaCitation22,Citation23 may play an important role in the pathogenesis of this keratitis.
Discussion
This review takes into consideration five case-control studies published from 1995 to 2012, and in each study, a statistically significant positive association between AK and CL use was found. The strength of this work is that, for the first time, it summarizes a pooled measure of association (OR = 10.21).
Early diagnosis is certainly of primary importance for the prognosis and outcome of AK because of the devastating nature of this infection. All too often, pharmacological treatment does not produce effective results, and the condition may return even after surgical intervention.
The diagnosis of AK is based on an accurate anamnesis which is fundamental for the identification of probable associated risk factors. It relies on techniques such as confocal microscopy, which allows the examination of the human cornea in real time. This technique visualizes microorganisms present on the cornea and identifies them as highly reflective, oval, or circular bodies, with a diameter of 10 μm–25 μm. These organisms are then analyzed in the laboratory after swab specimens have been obtained by scraping the epithelium. The stroma specimens are obtained with the use of a Kimura spatula. The scraping of the cornea must always be carried out to obtain an epithelial and subepithelial culture coloration.Citation24
The pharmacological treatment consists of an intense initial phase in which a combination of biguanide (propamidine isethionate 0.1% or chlorhexidine) and benzamidine (propamidine or pentamidine) is used to prevent the protozoan developing a chemical resistance. Subsequently, there was a maintenance period of variable duration, depending on the seriousness of the condition (which may even last up to 1 year).Citation22 In the most serious cases, inflammatory necrosis leads to the formation of corneal scars that require keratoplasty for the treatment of this perforation as part of the course of visual rehabilitation associated with anti-amoeba prophylaxis.Citation25,Citation26
The number of cases recorded and described in the literature is notably on the increase,Citation16–Citation20 and the aim of this study was to report the information pertinent to CL users and inform them about the diffusion and resistance of Acanthamoeba spp. in freshwater sources, including tap water.
A correct prevention envisages a scrupulous cleaning of CLs and their correct use, using ad hoc communication strategies that use the most efficient means of communication (information leaflets in pharmacies, doctor’s waiting rooms, etc).Citation1,Citation25
Conclusion
Because of the disease’s rare nature, it should be held in higher consideration when the ophthalmologist is faced with a CL user exhibiting simplex-like lesions associated with circular stromal infiltrates and disproportionate ocular pain in respect to the objective clinical picture. The temporal trend of publications has shown a steady increase from 1984 to the current time, testifying the interest in this rare disease among members of the international scientific community. In any case, we recommend that case-control studies need to be intensified to support risk evaluation, management, and communication better.
Disclosure
The authors report no conflicts of interest in this work.
References
- BonnetMVillonJCLa cornée (Kératites inflammatoires)The cornea (inflammatory keratitis)Arch Ophtalmol Rev Gen Ophtalmol1973332155166 French4354667
- KeayLEdwardsKNaduvilathTMicrobial keratitis predisposing factors and morbidityOphthalmology2006113110911616360210
- BuckSLRosenthalRASchlechBAMethods used to evaluate the effectiveness of contact lens care solutions and other compounds against Acanthamoeba: a review of the literatureCLAO J2000262728410810937
- BourcierTThomasFBorderieVChaumeilCLarocheLBacterial keratitis: predisposing factors, clinical, and microbiological review of 300 casesBr J Ophthalmol200387783483812812878
- SchaeferFBruttinOZografosLGuex-CrosierYBacterial keratitis: a prospective clinical and microbiological studyBr J Ophthalmol200185784284711423460
- SaeedAD’ArcyFStackJCollumLMPowerWBeattySRisk factors, microbiological findings, and clinical outcomes in cases of microbial keratitis admitted to a tertiary referral center in IrelandCornea200928328529219387229
- JoslinCETuEYMcMahonTTPassaroDJStaynerLTSugarJEpidemiological characteristics of a Chicago-area Acanthamoeba keratitis outbreakAm J Ophthalmol2006142221221716876498
- LamDSHouangEFanDSIncidence and risk factors for microbial keratitis in Hong Kong: comparison with Europe and North AmericaEye (Lond)200216560861812194077
- NagingtonJWatsonPGPlayfairTJMcGillJJonesBRSteeleADAmoebic infection of the eyeLancet197427896153715404140981
- VisvesvaraGSJonesDBRobinsonNMIsolation, identification, and biological characterization of Acanthamoeba polyphaga from a human eyeAm J Trop Med Hyg1975245784790811126
- CerulliLMancinoRPalmaSTomeiMCheratiti da AcanthamoebaScuderiGLa CorneaMasson199814303306
- TuEYJoslinCEMicrosporidia and Acanthamoeba: the role of emerging corneal pathogensEye (Lond)201226222222722173072
- BaconASFrazerDGDartJKMathesonMFickerLAWrightPA review of 72 consecutive cases of Acanthamoeba keratitis, 1984–1992Eye19937Pt 67197258119418
- LalithaPLinCCSrinivasanMAcanthamoeba keratitis in South India: a longitudinal analysis of epidemicsOphthalmic Epidemiol201219211111522364672
- IbrahimYWBoaseDLCreeIAFactors affecting the epidemiology of Acanthamoeba keratitisOphthalmic Epidemiol2007142536017464851
- PacellaEPacellaFTurchettiPPiratinoDCBalacco GabrieliCCheratite da acanthamoebaAcanthamoerba keratitisMontraneFSuperfice Oculare Up To DateBari, ItalyART STAMPA2009 Italian. Press Jun 2009, Eds ART STAMPA Monopoli (BA – Italy)197210
- SarnicolaVContiLSignoriCLa cheratite da AcanthamoebaAcanthamoerba keratitisProceedings of the Societa’ Italiana Cellule Staminali e Superficie Oculare2005 November 24Milan, ItalyMilanSocieta Oftalmologica Italiana2005
- LiberatiAAltmanGDTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaborationItal J Public Health200964354391
- VeraniJRLorickSAYoderJSNational outbreak of Acanthamoeba keratitis associated with use of a contact lens solution, United StatesEmerg Infect Dis20091581236124219751585
- RadfordCFBaconASDartJKMinassianDCRisk factors for Acanthamoeba keratitis in contact lens users: a case-control studyBMJ1995310156715707787645
- MeierPAMathersWDSutphinJEFolbergRHwangTWenzelRPAn epidemic of presumed Acanthamoeba keratitis that followed regional flooding. Results of a case-control investigationArch Ophthalmol19981168109010949715690
- JoslinCETuEYShoffMEThe association of contact lens solution use and Acanthamoeba keratitisAm J Ophthalmol2007144216918017588524
- PacellaEPacellaFImpallaraDThe role of contact lenses and ocular trauma in determining Acanthamoeba keratitis: a case-control study in ItalyItal J Public Health20129197102
- AlizadehHNiederkornJYMc CullenJPAcanthamoeba keratitisKrachmerJHMannisMJHollandEJCorneaSt Louis, MOMosby199712671273
- SealDTreatment of Acanthamoeba keratitisExpert Rev Anti Infect Ther20031220520815482114
- KitzmannASGoinsKMSutphinJEWagonerMDKeratoplasty for treatment of acanthamoeba keratitisOphthalmology2009116586486919410943