Abstract
Purpose
Beliefs about medicines impact on adherence, but eliciting core beliefs about medicines in individual patients is difficult. One method that has the potential to elicit individual core beliefs is the “repertory grid technique.” This study utilized the repertory grid technique to elicit individuals’ beliefs about their heart failure treatment and to investigate whether generated constructs were different between adherent and nonadherent patients.
Methods
Ninety-two patients with heart failure were interviewed using a structured questionnaire that applied the repertory grid technique. Patients were asked to compare and contrast their medicines and self-care activities for their heart failure. This lead to the generation of individual constructs (perceptions towards medicines), and from these, beliefs were elicited about their heart failure treatment, resulting in the generation of a repertory grid. Adherence was measured using the Medication Adherence Report Scale (MARS). Patients with a MARS score ≥ 23 were categorized as “adherent” and those with a score ≤ 22 as “nonadherent.” The generated grids were analyzed descriptively and constructs from all grids themed and the frequency of these constructs compared between adherent and nonadherent patients.
Results
Individual grids provided insight into the different beliefs that patients held about their heart failure treatment. The themed constructs “related to water,” “affect the heart,” “related to weight,” and “benefit to the heart” occurred more frequently in adherent patients compared with nonadherent patients.
Conclusion
The repertory grid technique elicited beliefs of individual participants about the treatment of their heart failure. Constructs from self-reported adherent patients were more likely to reflect that their medicines and self-care activities were related to water and weight, and affect and benefit to the heart. Providing clinicians with better insight into individuals’ beliefs about their treatment may facilitate the development of tailored interventions to improve adherence.
Introduction
Adherence to medication in patients with chronic disease is an acknowledged global problem, with the World Health Organization reporting that up to 50% of these patients do not adhere to their medication.Citation1 Factors that have been suggested to affect adherence relate to the disease, the patient, the social and economic context, behaviors, the physician, and the healthcare system.Citation1–Citation4 Nonadherence can be regarded as either unintentional, relating to issues of cognition (eg, forgetfulness), health literacy and dexterity; or intentional, where beliefs about a medicine (eg, concerns about side effects) or costs of the medicine result in a conscious decision not to take the medication.Citation5 Reminders and dosing aids may help those with unintentional nonadherence.Citation2,Citation3 However, less is understood about intentional nonadherence, particularly where beliefs about medicines impact on nonadherence behaviour.Citation1,Citation2
Questionnaires have been developed to identify individuals’ beliefs about medicines. These include the Belief about Medicines Questionnaire (BMQ),Citation6 the Beliefs and Behaviour Questionnaire,Citation7 the Adherence Estimator,Citation8 and ASK-20.Citation9 The most widely used, the BMQ, is based on a necessity–concerns framework, whereby patients with a high “necessity” score and low “concerns” score are more likely to be adherent.Citation10–Citation13 Other studies have demonstrated that a high “concerns” score and a low “necessity” score is likely to result in low adherence.Citation14–Citation19 The necessity–concerns framework helps to identify patients at potential risk of nonadherence but does not elucidate patients’ individual beliefs that fall outside this framework and that may also impact on adherence.
“Beliefs” can be considered assumed truths and are defined in the philosophy literature as propositional attitudes, ie, declarative statements that say something about the world and can be either true or false.Citation20 Examples of propositions are “it rained yesterday,” “the sky is orange,” and “perindopril is for my heart.” When an individual takes the proposition to be true or sufficiently likely to be true so as to influence decisions, it is considered a belief. One method that could be utilized to elicit beliefs is the “repertory grid technique,” developed from George Kelly’s personality theory published in “The Psychology of Personal Constructs” in 1955.Citation21 In this theory, Kelly proposed that all individuals are scientists and as such, form hypotheses in response to events in life, test these hypotheses, and then further refine them depending on the good or bad experience that results. In essence, this is then how individuals understand (construe) their world and as they pass through life, develop a system of personal constructs in response to events. When individuals are confronted with a new event, they use their construct system to make a judgment and then act. Thus, a construct is a way that an individual understands, perceives, or makes sense of something. Kelly developed the repertory grid technique as a method of eliciting an individual’s construct system in a particular area of interest. In this technique, individuals compare and contrast objects of interest (elements) to generate highly individual bipolar statements (constructs) reflecting the way they perceive their world. An interval scale can be placed between the poles of the statements and the individual asked to rate the objects of interest on the scale. In essence, when individuals do this, they generate four propositions and then, through the rating of the object of interest, pick the proposition that is true and therefore reflects their belief about that particular object. Therefore, the repertory grid allows individuals to articulate their own views or opinions to generate their own propositions, rather than responding to a set of predetermined statements that may or may not have relevance to them individually. The repertory grid technique has been utilized in exploring consumers’ beliefs in heart failure,Citation22 the evaluation of complementary medicines,Citation23 treatment decisions in patients with angina,Citation24 and perceptions of medication information sources.Citation25
Individuals with heart failure have to manage the combination of a complex medication regimen and self-care activities (such as exercising, reducing salt and fluid intake, and regular weighing) to reduce mortality and morbidity.Citation26–Citation28 Due to the complexity of the management regimen, it is not surprising that the common reasons reported for acute exacerbations of heart failure are nonadherence to medicationsCitation29–Citation32 and self-care activities.Citation32–Citation34 Eliciting individuals’ beliefs about medicines and self-care activities, in patients with heart failure, may provide an opportunity to develop interventions to change these, which in turn, could improve adherence. However, before an intervention can be developed, the potential of the repertory grid in eliciting beliefs must first be established.
The aim of this study was to utilize the repertory grid technique as a method to elicit individuals’ beliefs about their heart failure management. A further aim was to investigate whether the constructs generated by patients with heart failure were different between adherent and nonadherent patients.
Method
Study design
Data were collected via a structured interview that used the repertory grid technique. Patients were included if they were over the age of 18 years and attended the Heart Failure Service outpatient clinic, Heart Failure Service Programs, or were Heart Failure Service patients admitted to the medical wards at the Royal Brisbane and Women’s Hospital in Brisbane, Australia, between June 2007 and November 2008.
Informed consent was obtained from all participants, and ethical approval was obtained from the Human Research Ethics Committee of the Royal Brisbane and Women’s Hospital.
Interview
The structured interview was based on the repertory grid technique, as described by Fransella et al,Citation35 Jankowicz,Citation36 and Percival et al.Citation22 The interview was divided into five parts. The first three parts involved an adaptation of the repertory grid technique for individuals with heart failure. Part Four of the interview ascertained the participants’ self-reported adherence to their medicines. The fifth part of the interview collected demographic data. The data collection is explained in each of the sections below.
Part one – the elements (objects of interest)
Up to three currently prescribed medicines and four self-management activities (weighing, exercise, and reduction in fluid and salt intake) for heart failure were utilized as the elements. This resulted in a minimum of five (four self-care activities and one medicine) and a maximum of seven elements (four self-care activities and three medicines) used within the repertory grid interviews.
Part two – generating the constructs
Individuals were then presented with series of three elements (a triad) and asked to identify “some important way in which two of them are alike and different from the third.” Thus, two statements were obtained: one for the way the two were alike (termed the “emergent pole”) and one for the way the third one was different (termed the “implicit pole”).Citation35 These two statements helped identify the individual’s construct. Repeating this process with the different triads resulted in the identification of a series of constructs ().
Figure 1 Repertory grid process, generating constructs and rating information.
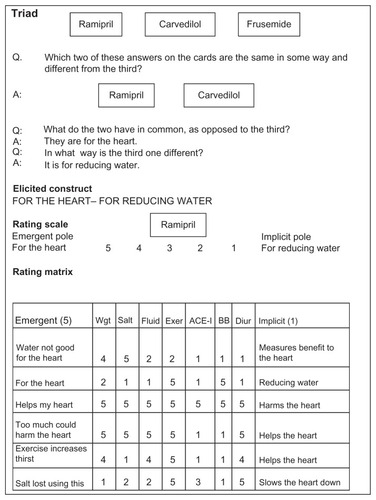
This process was repeated for further sets of triads until a maximum of twelve had been presented to the participant, until a range of constructs were produced that covered the topic, or until the participant was not generating any new constructs. The elements selected within the triads were chosen arbitrarily by using a balanced incomplete block design, as described by Leach et al.Citation37 The triads could be composed of only medicines (eg, angiotensin converting enzyme-inhibitor (ACE) or angiotensin receptor blocker, beta-blocker, diuretic), only self-care activities (eg, exercise, weighing, decreasing salt), or a combination of medicines and self-care activities (eg, beta-blocker, decreasing salt, reducing fluid).
Part three – eliciting beliefs
Participants were then shown a list of their generated constructs that consisted of the two opposing poles, eg, “for the heart” and “reducing water” (). A scale numbered 1 to 5 was placed between the opposing poles (). The participants were then given a card listing one of their elements and asked to rate the element against each of the generated constructs using this scale. Consider, in , the participant rating the ramipril against the construct “for the heart – reducing water.” The participant could produce four propositions: ramipril is for the heart (rated as 4 or 5); ramipril is for reducing water (rated 1 or 2); ramipril is both for the heart and reducing water (rated as 3); or ramipril is neither for the heart nor reducing water (rated as 0). Therefore, the participants, by rating the medicine, identified which proposition they thought to be true, generating their beliefs. In , the patient rated ramipril as 5, and therefore, his/her belief was that ramipril is for the heart.
Part four – self-reported adherence
Participants were asked to complete the Medication Adherence Report Scale (MARS). The MARS has been used as a self-reported measure of adherence in a number of chronic diseases, including chronic obstructive pulmonary disease,Citation38 asthma,Citation39 chronic pain management in cancer,Citation40 bipolar disorder,Citation17 and inflammatory bowel disease.Citation41,Citation42 The MARS includes a preamble encouraging honest responses. This is followed by a series of five statements that reflect adherent behavior. The individual selects one of five options ranging from “never” (scored as 5 by the researcher) to “always” (scored as 1) to reflect how often he/she adopts this behavior. It is then possible to calculate an overall adherence score and to dichotomize this based on a predefined cut-off score (good or poor adherence). A higher score (maximum 25) reflects more adherent behavior.
Part five – demographic data
The final part of the interview recorded participants’ demographic details: age, gender, concurrent medical complaints, and regular prescription medicines. These details, including their age, were confirmed and ambiguities clarified by reference to their medical notes.
Analysis
The demographic data were analyzed descriptively using SPSS® Version 13 (IBM, Armonk, NY, USA). Those participants with a MARS score ≥ 23 were categorized as “adherent” and those with a score ≤ 22 as “nonadherent.” The use of a MARS score of 23 to dichotomize the self-reported adherence has been described by others,Citation19,Citation43 and reflects the answers of “sometimes” to one question and “rarely” to two questions.
The repertory grids that were generated for the participants were analyzed qualitatively on an individual basis to explore whether the technique elicited individuals’ beliefs about their heart failure management. Four grids (two from patients categorized as adherent and two from patients categorized as nonadherent) have been included in the Results section of this paper to illustrate that the technique elicited individuals’ beliefs about management of their heart failure.
Comparison of the constructs elicited between the adherent and nonadherent participants was undertaken utilizing content analysis, as described by Jankowicz.Citation36 The first construct was reviewed by one of the researchers and themed according to the meaning that it appeared to be expressing. The next construct was reviewed, and if its meaning appeared to differ from that of the first construct, it was labeled with another theme. This process was repeated for all of the constructs, and a number of themes were developed until fewer than 5% of the constructs were compiled into a “miscellaneous” category. Once all the constructs had been assigned a theme by the first researcher, a second researcher reviewed the original constructs and the themes to which they were allocated. Where there was disagreement about placing the original construct into a theme, discussion took place to reach consensus. The frequency of the generated constructs was compared between the adherent and nonadherent groups, using the Fisher’s exact test.
Results
During the study period, 97 patients were approached to participate, of whom 92 agreed. The mean (±SD) age of the study participants was 67.4 (±14.5) years (minimum age 22 years, maximum 88 years), and 35 (38.0%) were female. Further demographics, including prescribed medicines and comorbidities, are shown in .
Table 1 Paticipant demographics
There were 82 (89.1%) of the participants that were categorized as adherent (MARS score ≥ 23), and the remaining 10 were categorized nonadherent (MARS score ≤ 22).
A total of 88 grids were generated from the participants. The remaining four patients were unable to generate a grid, as they could not distinguish between their medicines and self-care activities. An example of two grids generated by participants categorized as adherent is shown in and a further two, by patients categorized as nonadherent, in , along with an interpretation of the grids reflecting the beliefs held by the individuals about their medicines and self-care activities.
Figure 2 Repertory grid for two participants categorized as adherent (MARS ≥ 23). Both participants (A) and (B) had MARS score = 25.
Abbreviations: MARS, Medication Adherence Report Scale; Dec, decreasing; Red, reducing; ACE-I, angiotensin converting enzyme-inhibitor.
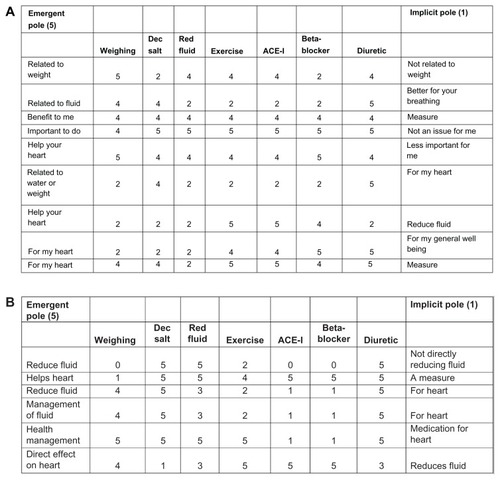
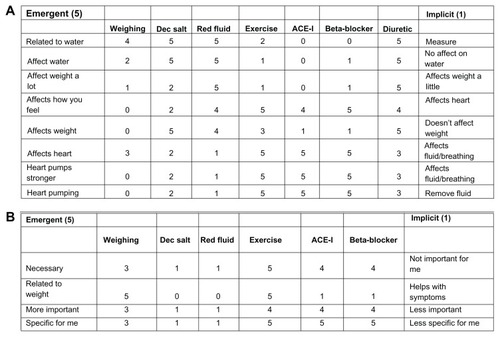
Figure 3 Repertory grid for two participants categorized as nonadherent (MARS ≤ 22). Both participants (A) and (B) had MARS score = 22.
Abbreviations: MARS, Medication Adherence Report Scale; Dec, decreasing; Red, reducing; ACE-I, angiotensin converting enzyme-inhibitor.
A total of 482 constructs were generated from the 88 grids, and from these, 21 themes were identified. Examples of the constructs and the themes to which they were allocated are shown in . The six most common themed constructs were “related to water,” “affect the heart,” “related to weight,” “remove fluid,” “necessary,” and “benefit to the heart.” Four constructs, “related to water,” “affect the heart,” “related to weight,” and “benefit to the heart,” occurred more frequently in the adherent group (MARS score ≥ 23) than in the nonadherent group (MARS score ≤ 22); however, this was not a significant difference ().
Table 2 Examples of some of the individual generated constructs for the six most common themed constructs
Table 3 Comparison between levels of self-reported adherence (from dichotomized MARS score) and the generated themed constructs
Discussion
In a sample of patients with heart failure, use of the repertory grid technique allowed patients to articulate their beliefs about their medicines and self-care activities, reflecting the management of their heart failure. The frequencies of the generated statements were not significantly different between adherent and nonadherent patients. However, the four constructs, “related to water,” “affect the heart,” “related to weight,” and “benefit to the heart,” occurred more frequently in the adherent group.
The repertory grid provided a unique insight into individuals’ beliefs about the management of their heart failure. The two grids represented in , from patients categorized as adherent (MARS = 25), reflect the belief that their medicines and exercise were “for the heart” (benefit or helping) and “important.” Their remaining self-care activities and the diuretic were believed to be related to fluid and water but also to have an “effect on the heart” and were important. The interpretation of these two grids illustrates these patients’ beliefs about their heart failure management and relates to findings from other studies of heart failure that have reported knowledge of medicines and disease symptoms, and the integration of this knowledge, improves overall adherence to medicines and self-care activities in the management of heart failure.Citation30,Citation34,Citation44–Citation46
The two grids in , from patients categorized as nonadherent (MARS = 22), illustrate visually different findings from . In , the patient’s ACE-inhibitor, beta-blocker, and exercise were believed to affect the heart, with the diuretic and the remaining self-care activities affecting water and breathing. At first, there appears to be no obvious link between the beliefs and the lower self-reported adherence score. However, on more detailed inspection of the original grid, there is one construct of particular interest. On the construct “affect the heart–affects how you feel,” the ACE-inhibitor and beta-blocker are aligned with the “affects how you feel” pole. In this example, during the interview, the patient was asked to clarify what he/she meant by “affects how you feel,” to ensure that the meaning implied in this pole of the construct was understood. The patient responded with the answer that he/she felt “overmedicated,” and this may account for the lower self-reported adherence score. A lack of belief in medication is related to withdrawal from medication,Citation47 and patient-perceived barriers to medication have been reported to result in lower levels of adherence in heart failure.Citation48–Citation51 For this patient, “affect me” may have contributed to a “concerns” belief about his/her medicines, which could account for the reduced self-reported adherence to medication. In , the patient believed his/her ACE-Inhibitor and beta-blocker to be “necessary” and “important,” whereas reducing fluid and decreasing salt were believed to be unimportant, and this was reflected in that he/she did not “do” these. This patient was not prescribed a diuretic, which may account for this belief. This patient believed that his/her medication was “necessary,” but despite this, he/she had lower self-reported adherence. However, a potential explanation arose during the interview when it was found that this patient held the belief that “nothing” would happen if the medicine was “unable to be taken.” For this individual, although he/she held the belief that the medicines were “necessary,” this was not transferring into behavior.
The beliefs elicited from the repertory grids described above reflect beliefs elicited from qualitative interviews with patients with heart failure. The beliefs (in our study) that identified something to do with water, removing fluid, or related to weight appear consistent with the benefit belief “taking water pills lessens my swelling” used in the Beliefs about Medicines Compliance Scale (BMCS), a validated questionnaire that uses prepared statements to identify beliefs about heart failure medicines.Citation45,Citation50,Citation52 Conversely, beliefs that identify effect on the heart and benefit to the heart appear to be related to “taking my medicines improves my quality of life” from the BMCS.Citation45,Citation50,Citation52 Percival et alCitation22 utilized the repertory grid to interview patients with heart failure and then related the generated constructs to the BMQ. The results found a limited relationship between the BMQ and the constructs from the repertory grid; however, our study was different in that it focused on elicitation and description of the beliefs from individual grids.
In reviewing the beliefs elicited using the repertory grid technique, it is important to consider how “beliefs” and “knowledge” are related. As described in the introduction, when an individual takes the proposition to be true or sufficiently likely to be true so as to influence decisions, it is considered a “belief.” A common analysis of “knowledge” is that this is “justified true belief.” For an individual to be said to have knowledge of a proposition, the following three must hold: the proposition is true; an individual believes the proposition is true; and the individual is justified in believing the proposition is true.Citation20 If one of these three does not hold, the individual would not be regarded as having “knowledge” of the proposition.
The most common underlying themes from the 482 constructs generated by the sample patients were “related to water,” “affect the heart,” “related to weight,” “remove fluid,” “necessary,” and “benefit to the heart.” When reflecting on the generated constructs categorized into the themes (examples in ), these suggest that the patients in this sample held the perception that their self-care activities and medicines were for fluid management, related to weight, and had beneficial effects on the heart. The perceptions generated by this sample of patients with heart failure are not dissimilar to perceptions of importance,Citation34,Citation45 necessity,Citation53 and benefitCitation47 in qualitative interviews of patients with heart failure. Although there was not a statistical significant difference in the frequency of the elicited perceptions between adherent and nonadherent patients, there was a trend towards “related to water,” “affect the heart,” “related to weight,” and “benefit to the heart” occurring more frequently in those with higher levels of self-reported adherence. Therefore, this difference may be applied clinically for individual patients who are nonadherent to their heart failure treatment. This suggests that the adherent patients were more likely to hold the perception that their medicines and self-care activities were related to water and weight (both are important in managing heart failure), and affect and benefit the heart. Those with a lower level of adherence were less likely to hold this perception about their heart failure management. This can be related to studies reporting that those patients with a better knowledge of their disease and management (self-care activities and medicines) in relation to fluid and weight were more likely to be adherent.Citation34,Citation45,Citation54
There are limitations that should be considered in interpreting the findings of our study. Not all patients were prescribed three medications; some were prescribed two medications for their heart failure. Therefore, for example, a patient who was not prescribed a diuretic might not have discussed salt and fluid, and might have been less likely to hold the belief that these were important for his/her heart failure management.
The patient sample was dominated by those with high self-reported adherence, probably consequential to their motivation to attend the Heart Failure Service programs/clinic on a regular basis. Whilst a nonsignificant trend was observed in this study, it is likely this would have reached clinical and statistical significance with a more general heart failure population. Further, the measurement of adherence was by self-report; this is not ideal due to the risk of overestimation of adherence but is still regarded as the most practical method.Citation2
A further point to note is that the repertory grid generates highly individualized data for each patient, and this may be of value clinically in eliciting beliefs to understand how an individual conceptualizes his/her heart failure management. It may allow clinicians to individualize education to a particular patient, based on his/her beliefs, with the hope of reducing nonadherence. Use of the repertory grid to elicit individual beliefs may help clinicians to identify a belief that is linked to nonadherence for that individual. Discussing and addressing this belief may result in a change in the belief and a resultant change in adherence. For example, consider the patient in who was reported to be nonadherent due to a belief that he/she was “overmedicated.” Discussing the importance of his/her medication may lead to a change in this belief and a change in adherence.
This is the first application of the repertory grid in exploring whether there is an association between individuals’ beliefs about their treatment for a condition and adherence. Although heart failure was the condition explored in this study, use of the repertory grid technique should be transferable to other chronic conditions, providing a unique insight into the understanding individuals have for the management of their condition.
Conclusion
The repertory grid technique elicited beliefs that individual participants held toward their medicines and self-care activities undertaken to manage their heart failure. There was a nonsignificant trend in the frequency of generated constructs between adherent and nonadherent patients. Patients who were adherent were more likely to hold the perception that their medicines and self-care activities were related to water and weight and to affect and benefit the heart. The repertory grid technique offers a novel method by which clinicians can gain insight into patients’ beliefs about their medications, which in turn, could lead to the development of interventions tailored to improve adherence.
Disclosure
The authors have no conflicts of interest to disclose in regards to the contents of the manuscript.
References
- World Health OrganizationAdherence to Long-Term Therapies: Evidence for ActionGenevaWorld Health Organization2003 Available from: http://whqlibdoc.who.int/publications/2003/9241545992.pdfAccessed January 10, 2013
- VermeireEHearnshawHVan RoyenPDenekensJPatient adherence to treatment: three decades of research. A comprehensive reviewJ Clin Pharm Ther200126533134211679023
- KruegerKPBergerBAFelkeyBMedication adherence and persistence: a comprehensive reviewAdv Ther200522431335616418141
- HaynesRBTaylorDWSackettDLCompliance in Health CareBaltimoreJohn Hopkins University Press1979
- NunesVNeilsonJO’FlynnNMedicines Adherence: Involving Patients in Decisions About Prescribed Medicines and Supporting AdherenceLondonNational Collaborating Centre for Primary Care and Royal College of General Practitioners2009 Available from: http://www.nice.org.uk/nicemedia/pdf/CG76FullGuideline.pdfAccessed January 10, 2013
- HorneRWeinmanJHankinsMThe beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medicationPsychol Health1999141124
- GeorgeJMackinnonAKongDCStewartKDevelopment and validation of the Beliefs and Behaviour Questionnaire (BBQ)Patient Educ Couns2006641–3506016843634
- McHorneyCAThe Adherence Estimator: a brief, proximal screener for patient propensity to adhere to prescription medications for chronic diseaseCurr Med Res Opin200925121523819210154
- HahnSRParkJSkinnerEPDevelopment of the ASK-20 adherence barrier surveyCurr Med Res Opin20082472127213818554431
- BarberNParsonsJCliffordSDarracottRHorneRPatients’ problems with new medication for chronic conditionsQual Saf Health Care200413317217515175485
- NicklasLBDunbarMWildMAdherence to pharmacological treatment of non-malignant chronic pain: the role of illness perceptions and medication beliefsPsychol Health200925560161520204936
- ByerBMyersLBPsychological correlates of adherence to medication in asthmaPsychol Health Med200054389393
- ConnKMHaltermanJSLynchKCabanaMDThe impact of parents’ medication beliefs on asthma managementPediatrics20071203e521e52617766496
- ByrneMWalshJMurphyAWSecondary prevention of coronary heart disease: patient beliefs and health-related behaviourJ Psychosom Res200558540341516026655
- BrownCBattistaDRBruehlmanRSereikaSSThaseMEDunbar-JacobJBeliefs about antidepressant medications in primary care patients: relationship to self-reported adherenceMed Care200543121203120716299431
- RussellJKazantzisNMedication beliefs and adherence to antidepressants in primary careN Z Med J20081211286142019098944
- ClatworthyJBowskillRParhamRRankTScottJHorneRUnderstanding medication non-adherence in bipolar disorders using a Necessity-Concerns FrameworkJ Affect Disord20091161–2515519101038
- PhatakHMThomasJ3rdRelationships between beliefs about medications and nonadherence to prescribed chronic medicationsAnn Pharmacother200640101737174216985088
- MårdbyACAkerlindIJorgensenTBeliefs about medicines and self-reported adherence among pharmacy clientsPatient Educ Couns2007691–315816417913439
- SchwitzgebelEBeliefZaltaENThe Stanford Encyclopedia of PhilosophyWinter 2011StanfordStanford University2011 Available from: http://plato.stanford.edu/archives/win2011/entries/belief/Accessed January 10, 2013
- KellyGAThe Psychology of Personal Constructs. Vol One: A Theory of PersonalityNew YorkNorton1955
- PercivalMCottrellWNJayasingheRExploring the beliefs of heart failure patients towards their heart failure medicines and self care activitiesInt J Clin Pharm201234461862522717778
- LewithGTChanJAn exploratory qualitative study to investigate how patients evaluate complementary and conventional medicineComplement Ther Med2002102697712481954
- RoweGLambertNBowlingAEbrahimSWakelingIThomsonRAssessing patients’ preferences for treatments for angina using a modified repertory grid methodSoc Sci Med200560112585259515814183
- TioJLaCazeACottrellWNAscertaining consumer perspectives of medication information sources using a modified repertory grid techniquePharm World Sci2007292738017187220
- FoodyJMFarrellMHKrumholzHMbeta-Blocker therapy in heart failure: scientific reviewJAMA2002287788388911851582
- GargRYusufSOverview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor TrialsJAMA199527318145014567654275
- WrightSPWalshHIngleyKMUptake of self-management strategies in a heart failure management programmeEur J Heart Fail20035337138012798837
- ClineCMBjörck-LinnéAKIsraelssonBYWillenheimerRBErhardtLRNon-compliance and knowledge of prescribed medication in elderly patients with heart failureEur J Heart Fail19991214514910937924
- RogersAAddington-HallJMMcCoyASA qualitative study of chronic heart failure patients’ understanding of their symptoms and drug therapyEur J Heart Fail20024328328712034153
- SchiffGDFungSSperoffTMcNuttRADecompensated heart failure: symptoms, patterns of onset, and contributing factorsAm J Med2003114862563012798449
- TsuyukiRTMcKelvieRSArnoldJMAcute precipitants of congestive heart failure exacerbationsArch Intern Med2001161192337234211606149
- CarlsonBRiegelBMoserDKSelf-care abilities of patients with heart failureHeart Lung200130535135911604977
- RiegelBCarlsonBFacilitators and barriers to heart failure self-carePatient Educ Couns200246428729511932128
- FransellaFBellRBannisterDA Manual for Repertory Grid Technique2nd edChichesterJohn Wiley & Sons Ltd2004
- JankowiczDThe Easy Guide to Repertory GridsChichesterJohn Wiley & Sons2003
- LeachCFreshwaterKAldridgeJSunderlandJAnalysis of repertory grids in clinical practiceBr J Clin Psychol200140Pt 322524811593952
- GeorgeJKongDCThomanRStewartKFactors associated with medication nonadherence in patients with COPDChest200512853198320416304262
- MenckebergTTBouvyMLBrackeMBeliefs about medicines predict refill adherence to inhaled corticosteroidsJ Psychosom Res2008641475418157999
- JacobsenRMøldrupCChristrupLSjøgrenPHansenOBThe Danish version of the Medication Adherence Report Scale: preliminary validation in cancer pain patientsPain Pract2009911719019056
- EdigerJPWalkerJRGraffLPredictors of medication adherence in inflammatory bowel diseaseAm J Gastroenterol200710271417142617437505
- HorneRParhamRDriscollRRobinsonAPatients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel diseaseInflamm Bowel Dis200915683784419107771
- HedenrudTJonssonPLindeMBeliefs about medicines and adherence among Swedish migraineursAnn Pharmacother2008421394518073328
- HorowitzCRReinSBLeventhalHA story of maladies, misconceptions and mishaps: effective management of heart failureSoc Sci Med200458363164314652059
- van der WalMHJaarsmaTMoserDKVeegerNJvan GilstWHvan VeldhuisenDJCompliance in heart failure patients: the importance of knowledge and beliefsEur Heart J200627443444016230302
- WuJRMoserDKChungMLLennieTAObjectively measured, but not self-reported, medication adherence independently predicts event-free survival in patients with heart failureJ Card Fail200814320321018381183
- EkmanIAnderssonGBomanKAdherence and perception of medication in patients with chronic heart failure during a five-year randomised trialPatient Educ Couns200661334835316139468
- GeorgeJShalanskySJPredictors of refill non-adherence in patients with heart failureBr J Clin Pharmacol200763448849317076693
- van der WalMHJaarsmaTAdherence in heart failure in the elderly: problem and possible solutionsInt J Cardiol2008125220320818031843
- van der WalMHJaarsmaTMoserDKvan GilstWHvan VeldhuisenDJUnraveling the mechanisms for heart failure patients’ beliefs about complianceHeart Lung200736425326117628194
- WuJRMoserDKChungMLLennieTAPredictors of medication adherence using a multidimensional adherence model in patients with heart failureJ Card Fail200814760361418722327
- BennettSJPerkinsSMLaneKAForthoferMABraterDCMurrayMDReliability and validity of the compliance belief scales among patients with heart failureHeart Lung200130317718511343003
- ArtinianNTMagnanMSloanMLangeMPSelf-care behaviors among patients with heart failureHeart Lung200231316117212011807
- NiHNaumanDBurgessDWiseKCrispellKHershbergerREFactors influencing knowledge of and adherence to self-care among patients with heart failureArch Intern Med1999159141613161910421285