Abstract
The United States Food and Drug Administration (FDA) approved naltrexone, a synthetic competitive antagonist at opioid receptors, in oral form in 1984 for use in the management of opioid abuse and addiction. Because naltrexone and its major metabolite, 6-β-naltrexone, are both competitive antagonists at opioid receptors – and thereby inhibit opioid agonist-induced effects including those desired by abusers – it was hypothesized that once maintained on naltrex-one, opioid-induced desirable effects would be diminished to the point that relapse to illicit use would decline because it was no longer rewarding. However, good medication compliance is a requisite for such a strategy to be effective and a systematic review of oral naltrexone concluded that this method of treatment was not superior for any outcomes measured (ie, retention, abstinence, or side effects) to placebo, psychotherapy, benzodiazepines, or buprenorphine treatment. In addition, the retention rate on oral naltrexone was very low (less than 30%). Recently, the FDA approved an extended-release formulation (intramuscular depot injection) of naltrexone for prevention of relapse to opioid dependence following opioid detoxification and to be used along with counseling and social support. Since it needs to be administered only monthly, as opposed to the daily administration required for the oral formulation, naltrexone injection has the potential for increasing adherence and retention rates. Concerns include liver damage at high doses (oral formulation) and possible opioid overdose if an attempt is made to surmount receptor antagonism by taking higher doses of an opioid agonist or if opioid receptors become “sensitized” under long-term antagonism. The focus of the present review is the current information regarding the safety and efficacy of naltrexone extended-release therapy.
Introduction
Incidence and prevalence of opioid abuse
The rate of both illicit and prescription drug misuse and abuse has steadily risen throughout the United States. According to the 2009 National Survey on Drug Use and Health report, illicit drug use (eg, cocaine and heroin) grew from 8.3% in 2002 to 8.9% in 2010 in persons aged 12 years or older.Citation1 In addition, the efforts by health care providers to provide better treatments for pain have consequently caused a rise in misuse, abuse, addiction, and diversion of many prescription opioids.Citation2 A prime example of the misuse and abuse of prescription opioids occurred in the state of Florida, where the death rate for prescription drugs increased approximately 84%, from 7.3 to 13.4 per 100,000 of the population from 2003 to 2009, with the greatest increase for prescription oxycodone (264.6%), methadone (79.2%), hydrocodone (34.9%), and morphine (26.2%).Citation3 Since the effects of opioid abuse can go beyond the individual and cause multiple social, economic, and health problems,Citation4–Citation6 effective treatment options are critical for both the illicit drug and prescription opioid abuser.
Management of opioid abuse
Opioid abuse can be a lifelong battle that requires substantial resources and therapeutic efforts by the patient, health care providers, regulatory agencies, and others. Additionally, opioid abusers come from different backgrounds and have different motivations and intentions when it comes to abuse. In an effort to accommodate the entire spectrum of opioid abusers, different prevention methods have been employed by physicians, regulatory bodies, and pharmaceutical companies. In an effort to counter potential short-term abuse, newer formulations of opioid agonists have come onto the market in order to make the product more tamper resistant and/or less desirable or appealing to abusers.Citation7–Citation9 Many extended-release formulations (eg, Remoxy®, King Pharmaceuticals, Inc, Cary, NC; Acuracet®, Acura Pharmaceuticals, Inc, Palatine, IL; Exalgo®, Mallinckrodt Inc, Hazelwood, MO) in addition to tamper-resistant (eg, Embeda®, Alpharma Pharmaceuticals LLC, Bridgewater, NJ) and dependence-deterrent formulations (Oxytrex®, Pain Therapeutics, Inc, San Francisco, CA; Suboxone®, Reckitt Benckiser Pharmaceuticals Inc, Richmond, VA) of agonist-antagonist combinations have been designed as abuse barriers. However, these formulations provide little benefit to the opioid-dependent patients looking to quit long-term abuse and thus these patients require other methods of treatment. Current therapies for opioid-dependent patients include (1) an agonist-based approach such as methadone, buprenorphine, or a buprenorphine-naloxone combination; (2) an antagonist-based approach, which includes the daily administration of the opioid antagonist naltrexone; or (3) a pharmacological approach combined with psychotherapy and patient supervision. The choice of approach is usually based on patient and physician preference along with the patient’s past medical and treatment history and even their financial status.Citation10–Citation14
Agonist-based approach
In its simplest form, agonist therapy is a supervised administration of a long-acting opioid receptor agonist with the goal to reduce or eliminate illicit drug use, increase retention in treatment, and help reduce many of the risk factors associated with illicit drug use (crime, infections, and so forth).Citation15,Citation16 Current therapies for opioid dependence may consist of methadone (Dolophine®, Roxane Laboratories, Inc, Columbus, OH; Methadose®, Mallinckrodt Specialty Chemicals Company, St Louis, MO), buprenorphine (Subutex® and Suboxone, Reckitt Benckiser Pharmaceuticals Inc), and the less frequently used levomethadyl acetate.Citation17 Methadone treatment was the first treatment to become available (in the 1960s), followed by the use of buprenorphine in doctors’ offices around the year 2000. Guidelines put forth by the World Federation of Societies of Biological Psychiatry,Citation16 two Cochrane reviews,Citation18,Citation19 and the World Health OrganizationCitation20 have concluded that there is an excellent evidence base supporting the efficacy of both methadone and buprenorphine for the treatment of opioid withdrawal and maintenance. Despite evidence of efficacy of agonist therapies, many countries and some US states have made agonist therapies unavailable or have severely restricted their access.Citation21 Even when therapies are available, not all patients are eligible or accepted for such treatment, owing to long waiting lists, lack of money or health insurance, or failure to produce a photo identification card on request.Citation22,Citation23 Furthermore, not all treatment providers or patients agree on this method of therapy, especially in patients who are young, have short dependence histories, or just do not want to take part in a lengthy detoxification therapy.Citation23 In addition, some practitioners are concerned about the side effects associated with long-term use of these opioids (eg, hypogonadism or immune suppression).Citation24,Citation25 Even though the agonist approach is effective, the limitations and concerns associated with this therapy have created a need for introducing effective antagonist treatments.
Antagonist-based approach
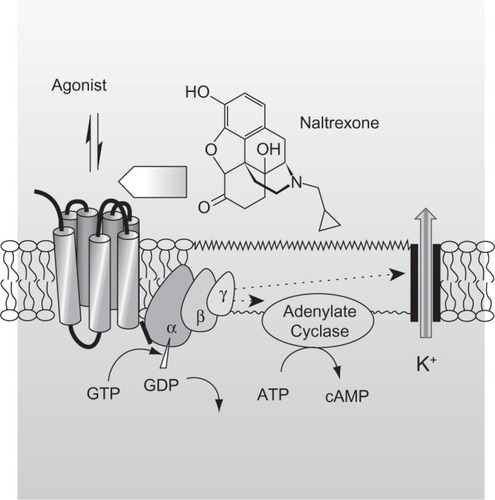
Opioid-dependent patients may be placed on an antagonist therapy. Opioid receptor antagonists block the effects generated by opioid agonists without producing any agonist effects of their own (). Thus, they have no abuse liability, no overdose potential, and they do not require special waivers to be prescribed.Citation26–Citation28 Currently, naltrexone (Depade®, Mallinckrodt Specialty Chemicals Company; Revia®, Bristol-Myers Squibb Pharma Company, Princeton, NJ) is a recommended opioid antagonist both for opioid withdrawal and for maintenance. Naltrexone therapy may be useful in preventing relapse in patients who have withdrawn from opioids and/or those motivated enough to abstain from opioid use.Citation20 However, the effectiveness of the antagonist-based approach has been somewhat disappointing and there is insufficient evidence to unequivocally support the clinical effectiveness of oral naltrexone in the treatment of opioid dependence.Citation29,Citation30 Its ineffectiveness can largely be traced to lack of patient adherence and retention. Thus, oral naltrexone has become a therapy mainly for the highly motivated individual.
Figure 1 Mechanism of action of naltrexone. The reversible interaction of an opioid agonist with opioid receptors, which are part of the seven-transmembrane, G-protein-coupled receptor family, elicits opioid-induced effects, including those desired by abusers. Opioid receptor antagonists such as naltrexone also reversibly bind to opioid receptors, but they lack intrinsic activity and thus do not elicit an opioid-like effect. However, their binding limits the number of unoccupied receptors and, consequently, the magnitude of agonist-induced opioid effects. Naltrexone, 17-(cyclopropylmethyl)-4,5α-epoxy-3,14-dihydroxymorphinan-6-one, is a substituted oxymorphone (the tertiary amine methyl group is replaced with methylcyclopropane) and the N-cyclopropylmethyl derivative of oxymorphone. Naltrexone’s major metabolite, 6-β-naltrexone, is also a competitive antagonist at opioid receptors.
Pharmacological approach in combination with psychosocial therapy
In an effort to increase therapy retention rates, increase reduction in illicit opioid use, and help improve patients’ quality of life, the concurrent use of psychosocial interventions has been recommended for both agonist and antagonist therapies.Citation20 Psychosocial interventions may include cognitive and behavioral approaches, as well as contingency management techniques. A recent systematic review of the literature identified 28 randomly controlled trials that address the advantage of combining psychosocial therapy with agonist maintenance treatments.Citation31
When a comparison was made between psychosocial plus maintenance pharmacological treatment and standard maintenance treatment, the results did not indicate any benefit in retention rate (relative risk [RR]: 1.02; 95% confidence interval [CI]: 0.97, 1.07), opiate use during the treatment (RR: 0.86; 95% CI: 0.65, 1.13), compliance (mean difference [MD]: 0.43; 95% CI: −0.05, 0.92), psychiatric symptoms (MD: 0.02; 95% CI: −0.19, 0.23), depression (MD: −1.30; 95% CI: −3.31, 0.72), or number of participants still in treatment at the end of the follow-up (RR: 0.91; 95% CI: 0.77, 1.06). However, the number of participants abstinent at the end of the follow-up showed a benefit in favor of the associated treatment (RR: 1.15; 95% CI: 1.01, 1.32).Citation31 In addition, psychosocial programs in combination with antagonist treatment have demonstrated effectiveness in maintaining abstinence and retention.Citation32,Citation33 For example, in a study with 127 detoxified opioid-dependent patients, patients utilizing both naltrexone treatment and a contingency program versus naltrexone alone showed both treatment retention (7.4 vs 5.6 weeks; P = 0.05) and reduction of opioid use (19 vs 14 opioid-free urine samples; P = 0.04).Citation32
Each of the approaches described here has its advantages and its disadvantages; however, underutilization of agonist therapies, unavailability of treatments, and inadequate success rates have created a need for other approaches. The focus of the present review is the current information regarding the safety and efficacy of naltrexone extended-release therapy.
Methods
The search strategy for the identification of studies included the electronic searching of the PubMed/MEDLINE database, Embase, and The Cochrane Library from database inception through to July 2011. Search terms used individually or in combination included “naltrexone,” “extended release naltrexone,” “injectable naltrexone,” “opioid antagonist,” and “opioid dependence.” The identified citations were then further limited to any clinical study or review article describing clinical use of injectable extended-release naltrexone. The goal was to present the reader with all published studies regardless of their design type. Studies exclusively describing other forms of naltrexone, including oral or implantable naltrexone, were eliminated. To identify any articles missed by the electronic search, the bibliographies of the electronically identified articles were analyzed and any appropriate articles, based on title and abstract, were retrieved.
Discussion
New formulations
Antagonist approach
Physicians originally had high hopes for antagonist therapies due to the pharmacological profile of these agents in the laboratory. However, clinicians soon realized that the effectiveness of the antagonists in the laboratory could not always be duplicated so readily in the clinic. Because the antagonist approach relies so heavily on a motivated and conscientious individual to maintain good compliance, a requirement of multiple oral dosing can represent a significant impediment to achieving successful treatment. In an effort to abrogate the problem of patient noncompliance with oral dosing, extended-release, injectable (depot) formulations of the antagonist naltrexone have been developed by three companies. Such an approach would seem to be a desirable method for delivering an opioid antagonist to opioid-dependent patients.Citation34
Extended-release naltrexone formulations
Currently there are three depot injection formulations available for extended-release naltrexone treatment, each providing therapeutic blood levels for approximately 4 weeks. There are two that have not yet been approved by the US Food and Drug Administration (FDA): Depotrex® (Biotek Inc, Woburn, MA) and Naltrel® (DrugAbuse Sciences SAS, Paris, France). Vivitrol® (Alkermes, Waltham, MA) was originally approved for alcohol dependence and received FDA approval for opioid dependence in late 2010. In addition to these depot extended-release injection formulations, biodegradable polylactic acid-based polymer naltrexone implant formulations are currently under investigation.Citation35–Citation38 The clinical safety and efficacy of these implants are beyond the scope of this review; rather, focus will be on the extended-release injection formulation.
Extended-release naltrexone: efficacy studies
Comer et alCitation39 examined the safety and efficacy of 192 mg (n = 6) and 384 mg (n = 6) doses of a sustained-release naltrexone (Depotrex) on twelve heroin-dependent patients in an 8-week inpatient study. After a 1-week detoxification period, participants were treated with either dose of naltrexone, followed by 6 weeks of challenge with heroin (0, 6.25, 12.5, 18.75, 25 mg, intravenously). Various subjective, performance, and physiological effects were measured before and after the heroin administration. Both doses of sustained-release naltrexone antagonized the heroin-induced subjective, performance, and physiological effects; the 192 mg dose did so for up to 3 weeks, and the 384 mg dose for up to 5 weeks. In addition, participants did not experience any major side effects except discomfort associated with the initial injection of the naltrexone. These initial results seemed promising for a new treatment therapy.
In a second study, Comer et alCitation40 conducted a double-blind, 8-week randomized trial on 60 heroin addicts. During weeks 1 and 5, participants received a single injection of placebo or extended-release naltrexone (Depotrex; either 192 mg or 384 mg) in addition to biweekly preventive therapy sessions. The main outcome measures included retention of treatment and percentage of opioid-negative urine samples. At the end of 8 weeks, 39% (7/18) of those treated with placebo, 60% (12/20) of those treated with naltrexone 192 mg, and 68% (15/22) of those treated with naltrexone 384 mg remained in the treatment. There were also statistically significant differences (P < 0.002) in mean dropout time in the placebo group (27 days), the naltrexone 192 mg group (36 days), and the naltrexone 384 mg group (48 days). When urine samples were tested for traces of opioids, differences were noted between the placebo (25.3%) and naltrexone 192 mg (47.1%) groups and between the placebo and naltrexone 384 mg (61.9%) groups; however, when adjusted for missed visits or samples, the differences were not statistically significant (P = 0.85). Although patients in the naltrexone groups reported “needing heroin less,” there was no difference in those “wanting heroin.” Similar to the previous study, side effects included induration (hardness) and pain at the injection site.
Brooks et alCitation41 utilized a quasi-experimental uncontrolled design to analyze and compare extended-release and oral naltrexone. At the time there was no study with a head-to-head comparison of investigative depot formulations and approved oral naltrexone. In this study, Brooks et al analyzed treatment retention and opioid use in heroin-dependent patients during an 8-week period where patients were treated with either long-acting injectable naltrexone or oral naltrexone with psychosocial intervention. In Comer et al’sCitation40 injectable naltrexone study already described, patients receiving injectable naltrexone (n = 42) remained on the treatment longer than patients on oral naltexone (n = 69) (42.3 vs 31.9 days; P = 0.012) after 8 weeks. During the 8 weeks of detoxification, injectable naltrexone patients had a similar level of negative urine tests to those in the oral naltrexone group (55% vs 50%). However, when missing urine samples were considered positive, injectable naltrexone patients had statistically fewer positive urine tests than the oral naltrexone patients (P = 0.024). No patient in these studies was seen to attempt overriding naltrexone. Even though the results of this study point to extended-release naltrexone as superior to oral naltrexone, the analytical approach should be considered exploratory; a true comparative trial is lacking.
Krupitsky et alCitation42 assessed the efficacy and safety of extended-release injectable naltrexone 380 mg (Vivitrol) in 250 opioid-dependent patients. The primary end points were urine drug tests and self-reporting of abstinence during weeks 5–24. Secondary end points consisted of self-reported opioid-free days, opioid-craving scores, number of days of retention, and relapse. During weeks 5–24, a median of 90% were confirmed abstinent weeks (by urine analysis) in the treatment group, compared with 35% in the placebo group (P = 0.0002). Those in the treatment group self-reported a median of 99% opioid-free days, compared with 60% reported by the placebo group. In addition, there were statistically significant differences (P < 0.0001) between the naltrexone and the placebo groups in craving reduction (mean score = −10.1 vs 0.7, respectively) and retention (median = 168 vs 96 days, respectively; P = 0.0042). During the 24-week study, more participants in the naltrexone group experienced one or more adverse events (including nasopharyngitis, insomnia, hypertension, influenza, pain at the injection site, toothache, and headache) than in the placebo group. There were no overdose events, suicide attempts, or deaths reported.
A retrospective study by Fishman et alCitation43 analyzed an open-label case series to assess acceptability, feasibility, and preliminary outcomes in opioid-dependent adolescents and young adults (average age 18.5 years) using extended-release naltrexone (Vivitrol) once every 4 weeks. Primary end points consisted of number of doses received after a 4-month treatment period and reduction in illicit opioid use. Sixteen of the 19 patients analyzed returned for at least one outpatient follow-up after receiving extended-release naltrexone. Of these sixteen patients, two (12.5%) dropped out after one follow-up session and ten (63%) remained in treatment for 4 months. The mean number of doses of nal-trexone received during the 4 months after initiation was 2.5 (median 3), with twelve patients (75%) receiving at least two doses. Seven patients (44%) continued naltrexone beyond 4 months, eleven (69%) were abstinent or had significant reductions in opioid use, and nine (56%) met the criteria for a “good” outcome at 4 months. In terms of safety, the only side effect examined was reports of overdose, of which none were documented.
In order to determine if extended-release naltrexone plus employment-based reinforcement can foster longer-term adherence, DeFulio et alCitation44 conducted a randomized trial of unemployed heroin-dependent patients (N = 38). Participants were given either extended-release naltrexone (Vivitrol) (n = 19) or the same plus a contingency program (n = 19) for 24 weeks. The contingency program consisted of a therapeutic workplace where participants could earn vouchers for attendance and participation in training programs. To stay within the program, they were required to receive naltrexone injections at 4-week intervals, but they could earn vouchers independent of their acceptance of naltrexone. Those in the employment-based contingency group accepted significantly more naltrexone injections than those in the naltrexone-only group (87% vs 52%; P = 0.002) and were more likely to accept the total of six injections (74% vs 26%; P = 0.004). However, there was no statistical difference between groups for opiate-negative (72% vs 65%; P = 0.56) or cocaine-negative (58% vs 54%; P = 0.75) urine samples.
Using the same experimental protocol, Everly et alCitation45 tested the adherence rate to extended-release naltrexone (Depotrex) in conjugation with an employment-based contingency program. Similar to the results of the previous study, the group that received both naltrexone and an employment-based reinforcement accepted significantly more naltrexone injections than the naltrexone-only group (81% vs 42%; P = 0.008) over the 24-week study, and they were more likely to accept all of the injections (66% vs 35%). However, both groups had similar numbers of opiate-negative (74% vs 62%; P = 0.413) or cocaine-negative (56% vs 54%; P = 0.939) urine samples.
Extended-release naltrexone: safety studies
In the clinical studies summarized, the acute side effects reported following administration of extended-release injectable naltrexone were mainly the same as those observed following oral administration of naltrexone. They included nausea, vomiting, decreased appetite, somnolence, fatigue, headache, dizziness, and anxiety. Systematic reviews of the effectiveness and safety of sustained-release naltrexone for opioid dependenceCitation46,Citation47 concluded that adverse events of extended-release naltrexone were similar to that of oral naltrex-one, but these events were more prominent in the naltrexone groups than in the placebo groups. Several of the studies documented irritation, induration, and pain at the site of injection. These adverse effects were not seen in the placebo groups and thus warnings are currently on the label of Vivitrol.Citation47
A potential risk that may be unique to extended-release formulations of naltrexone is the possibility that patients may attempt to remove the medication from within the site of injection. However, to the authors’ knowledge, no documented cases have appeared in the literature. Other potential side effects may include impairment in liver function and sexual dysfunction. Some early studies using oral formulations of naltrexone have suggested that naltrexone may produce hepatotoxicity and thus current warnings are listed on the prescription label of Vivitrol.Citation48,Citation49 Other data have disputed this,Citation50 but it is still a boxed warning. There has been no conclusive evidence reported of liver damage in patients receiving the recommended dosages of naltrexone.Citation51,Citation52 A report warned of sexual dysfunction with long-term oral naltrexone use, but confirmatory investigation is needed since prior long-term opioid agonist use may have led to the sexual dysfunction.Citation53
Opioid overdose
A concern raised about extended-release naltrexone is opioid agonist overdose. It is cautioned that this may occur in two ways, the first at accustomed doses of opioid agonist due to unanticipated opioid receptor “sensitization” during extended antagonist exposure and the second at unaccustomed high doses of opioid agonist during an intentional attempt to “override” the receptor antagonism. It is well known that in many model systems extended exposure to opioid antagonists can upregulate opioid receptors and increase their density throughout the central nervous system.Citation54–Citation59 These changes can result in functional supersensitivity,Citation60,Citation61 and an accidental “overdose” may occur even if agonist dose is not increased and antagonist treatment has been discontinued.
An abuser may attempt to override naltrexone’s receptor blockade with higher doses of opioid agonists, or by taking opioids at the end of naltrexone’s dosing interval, a time when plasma levels are decreasing and the blockade is diminishing.Citation49,Citation62 None of the studies presented in this review indicated any overdose cases, but there have been reports of opioid overdose in patients after discontinuation of oral naltrexone maintenance.Citation63,Citation64 To further investigate these overdose scenarios, future studies may look to increase follow-up assessments and treatment periods.
Antagonism of pain medication
Patients who are on extended-release naltrexone have diminished capacity to experience the analgesic effects of opioid agonists. Pain management may become a challenge because analgesia will not be possible with administration of opioids. Patient cases have been reported where successful analgesia was achieved using nonopioid analgesics or a local anesthetic technique.Citation65
Conclusion
Systematic reviews support the safety and efficacy of the “agonist approach” (mainly methadone and buprenorphine), albeit with long-term success rates having been a matter of debate.Citation66–Citation73 Less evidence supports the utility of the “antagonist approach” (mainly naltrexone), despite the fact that the approach is seemingly so logical (reduced receptor access to an agonist should attenuate agonist-induced rewarding effects). Part of the problem is that a high level of motivation and compliance is necessary.
Naltrexone initially was available only in an oral formulation. A once-monthly injectable (depot) form was developed in order to improve the chances of compliance. The FDA approved Vivitrol in October 2010 for prevention of relapse to opioid dependence following opioid detoxification, to be used along with concurrent counseling and social support. Approval was based mainly on a single study and this has generated some criticism of the process. However, the safety and effectiveness of Vivitrol will now be validated, or not, in clinical use. To the authors’ knowledge, no controlled studies directly compare the safety and efficacy of the extended-release formulation and the oral formulation, or methadone or buprenorphine maintenance treatment.
Oral naltrexone carries a warning for hepatocellular injury when given in excessive doses and it is contraindicated in acute hepatitis or liver failure; its use in patients with active liver disease must be carefully considered in light of its hepatotoxic effects. Vivitrol does not appear to be a hepatotoxin at the recommended doses, but the margin of separation between the apparently safe dose and the dose causing hepatic injury is stated to be only fivefold or less.
Given the important medical and societal needs for treatment of opioid abuse and the absence of a current 100% effective treatment, an extended-release opioid antagonist (naltrexone) appears to offer the hope of overcoming the compliance issues of oral naltrexone. Switching from a once-daily (oral) to a once-monthly (injectable) schedule of administration may also provide a psychological advantage, uncoupling drug taking from rewarding effect. Current research does not provide sufficient evidence to make conclusions about the effectiveness or safety of injectable naltrexone in the management of opioid dependence; further research is needed to put this question to rest.
Disclosure
Dr Pergolizzi is a consultant for ENDO Pharmaceuticals, Baxter Healthcare, Purdue Pharma, King Pharmaceuticals, Johnson and Johnson, and Grünenthal. Prof Raffa is a speaker, consultant, and/or basic science investigator for several pharmaceutical companies involved in analgesics research, but receives no royalty (cash or otherwise) from the sale of any product.
References
- Substance Abuse and Mental Health Services AdministrationResults from the 2010 National Survey on Drug Use and Health: Summary of National Findings NSDUH Series H-41 HHS Publication No. (SMA) 11-4658Rockville, MDSubstance Abuse and Mental Health Services Administration2011
- StagnittiMNTrends in Outpatient Prescription Analgesics Utilization and Expenditures for the US Civilian Noninstitutionalized Population, 1996 and 2006Rockville, MDAgency for Healthcare Research and Quality2009
- Centers for Disease Control and Prevention (CDC)Drug overdose deaths: Florida, 2003–2009MMWR Morb Mortal Wkly Rep2011602686987221734633
- GoldsteinAHerreraJHeroin addicts and methadone treatment in Albuquerque: a 22-year follow-upDrug Alcohol Depend19954021391508745136
- HulseGKEnglishDRMilneEHolmanCDThe quantification of mortality resulting from the regular use of illicit opiatesAddiction199994222122910396790
- DarkeSRossJSuicide among heroin users: rates, risk factors and methodsAddiction200297111383139412410779
- SchneiderJPMatthewsMJamisonRNAbuse-deterrent and tamper-resistant opioid formulations: what is their role in addressing prescription opioid abuse?CNS Drugs2010241080581020839893
- HamedEMoeDDevelopment of tamper deterrent formulations: state of the pharmaceutical industryCurr Drug Abuse Rev20103313914621054261
- RaffaRBPergolizziJVJrOpioid formulations designed to resist/deter abuseDrugs201070131657167520731474
- KleberHDPharmacologic treatments for opioid dependence: detoxification and maintenance optionsDialogues Clin Neurosci20079445547018286804
- CastellsXKostenTRCapellàDVidalXColomJCasasMEfficacy of opiate maintenance therapy and adjunctive interventions for opioid dependence with comorbid cocaine use disorders: a systematic review and meta-analysis of controlled clinical trialsAm J Drug Alcohol Abuse200935533934920180662
- AmatoLMinozziSDavoliMVecchiSFerriMMMayetSPsychosocial and pharmacological treatments versus pharmacological treatments for opioid detoxificationCochrane Database Syst Rev20084CD00503118843675
- WittchenHUApeltSMSoykaMFeasibility and outcome of substitution treatment of heroin-dependent patients in specialized substitution centers and primary care facilities in Germany: a naturalistic study in 2694 patientsDrug Alcohol Depend200895324525718337025
- MattickRPBreenCKimberJDavoliMMethadone maintenance therapy versus no opioid replacement therapy for opioid dependenceCochrane Database Syst Rev20093CD00220919588333
- Van den BrinkWHaasenCEvidenced-based treatment of opioid-dependent patientsCan J Psychiatry2006511063564617052031
- SoykaMKranzlerHRvan den BrinkWKrystalJMöllerHJKasperSWFSBP Task Force on TreatmentGuidelines for Substance Use DisordersThe World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of substance use and related disorders: Part 2. Opioid dependenceWorld J Biol Psychiatry201112316018721486104
- NichollsLBragawLRuetschCOpioid dependence treatment and guidelinesJ Manag Care Pharm2010161 Suppl BS14S2120146550
- MattickRPKimberJBreenCDavoliMBuprenorphine maintenance versus placebo or methadone maintenance for opioid dependenceCochrane Database Syst Rev20032CD00220712804429
- MattickRPBreenCKimberJDavoliMMethadone maintenance therapy versus no opioid replacement therapy for opioid dependenceCochrane Database Syst Rev20032CD00220912804430
- World Health Organization (WHO)Guidelines for the psychoso-cially assisted pharmacological treatment of opioid dependenceDepartment of Mental Health and Substance AbuseAbuseGenevaWHO Press20091110
- MathersBMDegenhardtLAliHHIV prevention, treatment, and care services for people who inject drugs: a systematic review of global, regional, and national coverageLancet201037597191014102820189638
- FriedmannPDLemonSCSteinMDD’AunnoTAAccessibility of addiction treatment: results from a national survey of outpatient substance abuse treatment organizationsHealth Serv Res200338388790312822917
- PetersonJASchwartzRPMitchellSGWhy don’t out-of-treatment individuals enter methadone treatment programmes?Int J Drug Policy2010211364218805686
- ReeceASDiffering age related trajectories of dysfunction in several organ systems in opiate dependenceAging Clin Exp Res Epub2212011
- ToskulkaoTPornchaiRAkkarapatumwongVVatanatunyakumSGovitrapongPAlteration of lymphocyte opioid receptors in methadone maintenance subjectsNeurochem Int201056228529019913582
- MartinWRJasinskiDRManskyPANaltrexone, an antagonist for the treatment of heroin dependence: effects in manArch Gen Psychiatry19732867847914707988
- MelloNKMendelsonJHKuehnleJCSellersMSOperant analysis of human heroin self-administration and the effects of naltrexoneJ Pharmacol Exp Ther1981216145547452507
- WalshSLSullivanJTPrestonKLGarnerJEBigelowGEEffects of naltrexone on response to intravenous cocaine, hydromorphone and their combination in humansJ Pharmacol Exp Ther199627925245388930154
- MinozziSAmatoLVecchiSDavoliMKirchmayerUVersterAOral naltrexone maintenance treatment for opioid dependenceCochrane Database Syst Rev20061CD00133316437431
- MinozziSAmatoLVecchiSDavoliMKirchmayerUVersterAOral naltrexone maintenance treatment for opioid dependenceCochrane Database Syst Rev20114CD00133321491383
- AmatoLMinozziSDavoliMVecchiSFerriMMMayetSPsychosocial combined with agonist maintenance treatments versus ago-nist maintenance treatments alone for treatment of opioid dependenceCochrane Database Syst Rev20084CD00414718843654
- CarrollKMBallSANichCTargeting behavioral therapies to enhance naltrexone treatment of opioid dependence: efficacy of contingency management and significant other involvementArch Gen Psychiatry200158875576111483141
- Fals-StewartWO’FarrellTJBehavioral family counseling and nal-trexone for male opioid-dependent patientsJ Consult Clin Psychol200371343244212795568
- ComerSDSullivanMAHulseGKSustained-release naltrexone: novel treatment for opioid dependenceExpert Opin Investig Drugs200716812851294
- BrewerCStreelERecent developments in naltrexone implants and depot injections for opiate abuse: the new kid on the block is approaching adulthoodAdicciones201022428529121152846
- KellyKIMcBrideANaltrexone implantsBr J Psychiatry2010196177 author reply 7720044669
- KunøeNLobmaierPVederhusJKNaltrexone implants after in-patient treatment for opioid dependence: randomised controlled trialBr J Psychiatry2009194654154619478295
- WaalHFrogopsahlGOlsenLChristophersenASMørlandJNaltrexone implants: duration, tolerability and clinical usefulness; a pilot studyEur Addict Res200612313814416778434
- ComerSDCollinsEDKleberHDNuwayserESKerriganJHFischmanMWDepot naltrexone: long-lasting antagonism of the effects of heroin in humansPsychopharmacology (Berl)2002159435136011823887
- ComerSDSullivanMAYuEInjectable, sustained-release naltrexone for the treatment of opioid dependence: a randomized, placebo-controlled trialArch Gen Psychiatry200663221021816461865
- BrooksACComerSDSullivanMALong-acting injectable versus oral naltrexone maintenance therapy with psychosocial intervention for heroin dependence: a quasi-experimentJ Clin Psychiatry201071101371137820673549
- KrupitskyENunesEVLingWIlleperumaAGastfriendDRSilvermanBLInjectable extended-release naltrexone for opioid dependence: a double-blind, placebo-controlled, multicentre randomised trialLancet201137797761506151321529928
- FishmanMJWinstanleyELCurranEGarrettSSubramaniamGTreatment of opioid dependence in adolescents and young adults with extended release naltrexone: preliminary case-series and feasibilityAddiction201010591669167620626723
- DeFulioAEverlyJJLeoutsakosJMEmployment-based reinforcement of adherence to an FDA approved extended release formulation of naltrexone in opioid-dependent adults: a randomized controlled trialDrug Alcohol Depend Epub7202011
- EverlyJJDeFulioAKoffarnusMNEmployment-based reinforcement of adherence to depot naltrexone in unemployed opioid-dependent adults: a randomized controlled trialAddiction201110671309131821320227
- LobmaierPKornørHKunøeNBjørndalASustained-release naltrexone for opioid dependenceCochrane Database Syst Rev20082CD00614018425938
- LobmaierPPKunøeNGossopMWaalHNaltrexone depot formulations for opioid and alcohol dependence: a systematic reviewCNS Neurosci Ther Epub9232010
- MalcolmRO’NeilPMSexauerJDRiddleFECurreyHSCountsCA controlled trial of naltrexone in obese humansInt J Obes1985953473533908352
- Vivitrol (naltrexone for extended-release injectable suspension) [prescribing information]Dublin, IrelandAlkermes Inc2010
- BrewerCWongVSNaltrexone: report of lack of hepatotoxicity in acute viral hepatitis, with a review of the literatureAddict Biol200491818715203443
- YenMHKoHCTangFILuRBHongJSStudy of hepatotoxicity of naltrexone in the treatment of alcoholismAlcohol200638211712016839858
- GarbuttJCEfficacy and tolerability of naltrexone in the management of alcohol dependenceCurr Pharm Des201016192091209720482515
- RamdurgSAmbekarALalRSexual dysfunction among male patients receiving buprenorphine and naltrexone maintenance therapy for opioid dependenceJ Sex Med Epub322011
- SirohiSKumarPYoburnBCMu-opioid receptor up-regulation and functional supersensitivity are independent of antagonist efficacyJ Pharmacol Exp Ther2007323270170717698975
- ZakiPAKeithDEJrBrineGACarrollFIEvansCJLigand-induced changes in surface mu-opioid receptor number: relationship to G protein activation?J Pharmacol Exp Ther200029231127113410688632
- RajashekaraVPatelCNPatelKPurohitVYoburnBCChronic opioid antagonist treatment dose-dependently regulates mu-opioid receptors and trafficking proteins in vivoPharmacol Biochem Behav200375490991312957235
- YoburnBCShahSChanKDuttaroyADavisTSupersensitivity to opioid analgesics following chronic opioid antagonist treatment: relationship to receptor selectivityPharmacol Biochem Behav1995512–35355397667382
- LesscherHMBaileyABurbachJPVan ReeJMKitchenIGerritsMAReceptor-selective changes in mu-, delta- and kappa-opioid receptors after chronic naltrexone treatment in miceEur J Neurosci20031751006101212653976
- PatelCNRajashekaraVPatelKPurohitVYoburnBCChronic opioid antagonist treatment selectively regulates trafficking and signaling proteins in mouse spinal cordSynapse2003501677612872295
- YoburnBCInturrisiCEModification of the response to opioid and nonopioid drugs by chronic opioid antagonist treatmentLife Sci19884218168916963362035
- YoburnBCKreuscherSPInturrisiCESierraVOpioid receptor upregulation and supersensitivity in mice: effect of morphine sensitivityPharmacol Biochem Behav19893237277312544906
- FishmanMPrecipitated withdrawal during maintenance opioid blockade with extended release naltrexoneAddiction200810381399140118855831
- DigiustoEShakeshaftARitterAO’BrienSMattickRPNEPOD Research GroupSerious adverse events in the Australian National Evaluation of Pharmacotherapies for Opioid Dependence (NEPOD)Addiction200499445046015049745
- RitterAJNaltrexone in the treatment of heroin dependence: relationship with depression and risk of overdoseAust N Z J Psychiatry200236222422811982544
- O’BrienBCodyCAnalgesia and sedation in the presence of a naltrexone implant: a novel pharmacological challengeEur J Emerg Med200613531531616969243
- WardJMattickRPHallWThe effectiveness of methadone maintenance treatment: an overviewDrug Alcohol Rev199413332733516818345
- FiellinDAMooreBASullivanLELong-term treatment with buprenorphine/naloxone in primary care: results at 2–5 yearsAm J Addict200817211612018393054
- HubbardRLMarsdenMECavanaughERachalJVGinzburgHMRole of drug-abuse treatment in limiting the spread of AIDSRev Infect Dis19881023773843259712
- SimpsonDDJoeGWBroomeKMA national 5-year follow-up of treatment outcomes for cocaine dependenceArch Gen Psychiatry200259653854412044196
- SimpsonDDTreatment for drug abuse: follow-up outcomes and length of time spentArch Gen Psychiatry19813888758807259424
- HubbardRLCraddockSGAndersonJOverview of 5-year followup outcomes in the drug abuse treatment outcome studies (DATOS)J Subst Abuse Treat200325312513414670518
- GottheilESterlingRCWeinsteinSPDiminished illicit drug use as a consequence of long-term methadone maintenanceJ Addict Dis199312445578292639
- MaremmaniIPaniPPPaciniMPerugiGSubstance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroin-addicted patientsJ Subst Abuse Treat72007331919817588494