
Abstract
The C-MAC videolaryngoscope is the first Macintosh-typed videolaryngoscope. Since the advent of its original version video Macintosh system in 1999, this device has been modified several times. A unique feature of C-MAC device is its ability to provide the 2 options of direct and video laryngoscopy with the same device. The available evidence shows that in patients with normal airways, C-MAC videolaryngoscope compared with direct laryngoscopy can provide comparable or better laryngeal views and exerts less force on maxillary incisors, but does not offer conclusive benefits with regard to intubation time, intubation success, number of intubation attempts, the use of adjuncts, and hemodynamic responses to intubation. In patients with predicted or known difficult airways, C-MAC videolaryngoscope can achieve a better laryngeal view, a higher intubation success rate and a shorter intubation time than direct laryngoscopy. Furthermore, the option to perform direct and video laryngoscopy with the same device makes C-MAC videolaryngoscope exceptionally useful for emergency intubation. In addition, the C-MAC videolaryngoscope is a very good tool for tracheal intubation teaching. However, tracheal intubation with C-MAC videolaryngoscope may occasionally fail and introduction of C-MAC videolaryngoscope in clinical practice must be accompanied by formal training programs in normal and difficult airway managements.
Introduction
In the past decade, videolaryngoscopy-assisted tracheal intubation has extensively been applied in airway management because of several significant advantages. These include: 1) improved laryngeal visualization without the need for aligning 3 airway axes, especially in difficult airway conditions.Citation1 2) The high-quality, magnified airway image makes it easy to identify the airway anatomical structures and anomalies, and facilitates manipulation of airway devices.Citation2 3) The entire team can see laryngoscopy and intubation process on the monitor, rather than only the intubator. This multi-person visualization feature can facilitate communication and cohesion of team, improve coordination between intubator and assistant, and thus simply change difficult airway management from “I” to “we”.Citation3,Citation4 Furthermore, the ability of videolaryngoscopy to provide a shared view can make it useful for teaching tracheal intubation.Citation5
There are a number of videolaryngoscopes available, with the number constantly increasing and many existing devices being modified. Each device’s features may offer advantages or disadvantages, depending on the situations the clinicians have to manage.Citation6 Of these devices, videolaryngoscopes with the Macintosh blades can offer the unique benefit of both direct and indirect laryngoscopy in a single intubation attempt. A typical example of such a device is C-MAC videolaryngoscope, which is the first Macintosh-type videolaryngoscope, with a great number of publications. This review was aimed to describe the features of C-MAC videolaryngoscope and summarize the evidences regarding efficacy of this device in adult airway management and its role in tracheal intubation teaching according to the literatures published in peer-reviewed journals.
Device description
C-MAC videolaryngoscope was developed and manufactured by the Karl Storz GmbH & Co. KG (Tuttlingen, Germany) in 1999. The video Macintosh system in the original model operates with a small color video camera housed to a conventional laryngoscope handle. A Macintosh blade is attached to the handle and a combined image/light bundle is threaded into a small metal guide tube, recessed 40 mm from the blade tip. The camera cable is attached to a control unit and the light cable to the light source. The video Macintosh system is installed on a small cart so that the device is easily moved. The cart supports an 8-inch monitor mounted on a swivel arm placed on the patient’s left side ().Citation7,Citation8
Figure 1 The video Macintosh system.
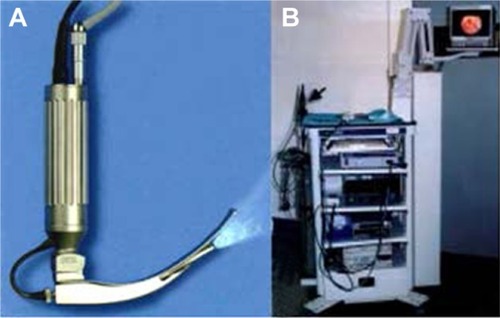
The modified version of video Macintosh system is the Storz direct-coupled interface, Berci-Kaplan or V-MAC videolaryngoscope, which consists of a laryngoscope, a bulk 8-inch monitor, a light source and a camera control unit.Citation5 A fiber light cord and a camera cable emerge from the top of the handle (), which connect to the light source and the camera control unit, respectively.
Figure 2 The C-MAC videolaryngoscope system.

Figure 3 C-MAC videolaryngoscope with disposable plastic blade.

The C-MAC or Boedeker–Dörges videolaryngoscope is a modification of the V-MAC device. It includes an electronic module utilizing semiconductor chip technology and only consists of 3 parts, a laryngoscope, electronic module and separate 7-in (18 cm) monitor (). The monitor connects to the electronic module that plugs into a laryngoscope. The weight of monitor with battery is about 1 kg. The key innovation of C-MAC device is a completely portable setup that features an improved image quality. The main differences between C-MAC and V-MAC devices are that the C-MAC videolaryngoscope includes improved optics, field of view, interface for adjusting video quality, and easy recording of imaging. Moreover, the manufacturer provides the C-MAC device with a 2-inch pocket monitor attached to the handle (). This portable device is specially developed for pre-hospital and in-hospital first aid. The device incorporates lithium-ion battery technology with at least 2 hours capacity and the pocket monitor can display a clear image under the strong light.Citation1,Citation6–Citation9
The C-MAC device can create continuous video recording or static pictures onto a removable secure digital card.Citation8 The electronic module includes 2 buttons for photo and video capture. In addition, C-MAC device’s images can also be displayed on other devices or recorded by a standard video output port.
There are 3 C-MAC reusable metal Macintosh blades (sizes 2–4) available for adult patients.Citation6 The reusable blades have a closed design without gaps for hygienic traps and the edges are slanted to avoid tissue damage.Citation10 The proximal flange of C-MAC reusable blade is significantly bigger than those of Glidescope and McGrath videolaryngoscopes and is about 2.5 cm high at its base versus Glidescope videolaryngoscope, which is 1.5 cm and McGrath videolaryngoscope, which is 1.25 cm. This provides more space for manipulating the tracheal tube with the C-MAC device. In addition, the proximal shape and size of the C-MAC reusable blade make tube passage to the glottis more straightforward compared with that of the Glidescope or McGrath videolaryngoscope. Compared with smaller fanged videolaryngoscopes, however, a disadvantage of the larger proximal flange of C-MAC video-laryngoscope may be the need of a greater mouth opening.Citation11
The tip of the C-MAC reusable blade contains a 320×240 pixel complementary metal oxide semiconductor video chip and fog-resistant lens. The camera with the light source is located close to the tip of the blade and has an 80° view angle, allowing for a wide angle of viewing at the blade tip and a high-resolution color image on the monitor.Citation8 Because the view obtained by C-MAC device includes the blade tip (), it allows for guiding the blade tip into the epiglottic vallecula under vision.Citation10 The reusable blades require sterilization between each patient.
Recently, the manufacturer has amended the relatively large and bulky handles of C-MAC devices. The new handles are truncated and thinned with a light weight and multifunction C-MAC system interface (). Furthermore, the manufacturer has released the disposable C-MAC device, with 2 adult blades (sizes 3 and 4) available ().Citation80 The disposable C-MAC device contains a disposable Macintosh plastic blade, an image tube with a camera and a monitor. The image tube is inserted into the disposable plastic blade to be protected from oral contamination. However, the disposable plastic blade is not completely the same as the reusable metal blade. Both the web and flange sections of the disposable plastic blades are significantly thickened to avoid breakage during use. These additional bulk can reduce the pharyngeal view and limit space for manipulating the tracheal tube when using the disposable plastic blade.Citation12
As C-MAC videolaryngoscope uses a Macintosh blade, the larynx can be seen either under direct vision or on a monitor. That is, the airway view on the monitor is similar to what is seen when looking directly into the mouth.Citation7 Thus, this device is unique among videolaryngoscopes as it allows for use as a videolaryngoscope while simultaneously functioning as a direct laryngoscope. This feature may be useful in the case of video failure or secretions on the lens.Citation6 However, a shortcoming of using a Macintosh blade is the frequent needs for alignment of 3 airway axes and external laryngeal pressure to obtain a good laryngeal view during laryngoscopy.
Intubation procedure with C-MAC videolaryngoscope
When using as direct laryngoscopy, the intubation procedure with C-MAC videolaryngoscope is identical to conventional Macintosh laryngoscope. The device is inserted into the right side of the mouth, the tongue is moved to the left by the blade flange, the blade tip is advanced into the epiglottic valecula, and then the device is raised to obtain the laryngeal view.Citation11 If a poor laryngeal view is obtained, the optimization maneuver includes external laryngeal pressure and blade position adjustment, such as the straight blade technique, to elevate the epiglottis.Citation13 Tracheal tube insertion depends on intubator’s preference for direct laryngoscopy, when required to use a stylet and the bend angles of the styletted tube.Citation8
When using as a videolaryngoscopy, a midline insertion technique without sweep of the tongue can achieve an unobstructed view of the larynx, given the vantage point from beneath the base of the tongue.Citation7 Although a stylet is not always required, it can be very helpful for bringing the tube tip up to the glottis, especially in patients with a difficult airway. A study comparing performance of different videolaryngoscopes in patients with a normal airway shows that a stylet is required in 10%, 76% and 60% of cases with C-MAC, McGrath and Glidescope videolaryngoscopes, respectively.Citation14 In patients undergoing elective cervical spine surgery with head and neck stabilized by manual in-line stabilization, the use of stylet significantly reduces the intubation difficulty scale score, intubation time and the use of gum-elastic bougie with C-MAC videolaryngoscope.Citation15 When a stylet is used for C-MAC videolaryngoscope, however, a sharp distal bend of the styletted tube is not required as the proximal shape of the blade offers a relatively straighter route for tube insertion, especially in patients with a normal airway. In contrast, sharply-angled videolaryngoscopes, such as Glidescope videolaryngoscopes, a significant distal bend angle of the styletted tube is often required to pass the tracheal tube “around the corner” up to the glottis.Citation11
Performance of C-MAC videolaryngoscope versus direct laryngoscopy
Normal airways
The videolaryngoscope was originally designed as a device to manage difficult intubation with direct laryngoscopy.Citation6 Although this certainly is true, it misses the point, which limits its use only to the intubations predicted to be difficult or proven difficult after failed intubations with direct laryngoscopy. In fact, success with the application of any device can be enhanced as experience with the intervention accumulates. If videolaryngoscopy is used for all patients, experience and skill would undoubtedly increase, the number of intubation attempts and complications of multiple attempts would decrease, and patient care would improve.Citation4,Citation16 It has been suggested that optimal videolaryngoscope should be offered to all patients without significant limitations and not restricted to only those considered most difficult.Citation17 In addition, advantages of C-MAC videolaryngoscope combining the benefits of direct and video laryngoscopy in one device also make it suitable to serve as a standard intubation tool for routine airway management.Citation7
In available literatures, 3 observational trials comparing direct and indirect (video monitor) laryngeal views using a V-MAC or C-MAC videolaryngoscope in adult patients with a normal airway showed that compared with direct visualization, video-assisted laryngoscopy provided an improved laryngeal view.Citation14,Citation18,Citation19 Furthermore, there are several randomized controlled trials (RCTs) comparing the performance of V-MAC or C-MAC videolaryngoscope and direct laryngoscope for orotracheal intubation in adult patients with a normal airway.Citation10,Citation20–Citation25 Cavus et alCitation10 found that C-MAC videolaryngoscope provided comparable or better laryngeal views than direct laryngoscopy, and the intubation time was comparable between direct and video laryngoscopy. Sarkılar et alCitation20 compared performance and hemodynamic response to intubation with Macintosh laryngoscope and C-MAC videolaryngoscope and demonstrated that C-MAC device offered a better laryngeal view and a longer intubation time, but the number of intubation attempts, the use of external laryngeal pressure or stylet, and hemodynamic response to orotracheal intubation were comparable between 2 devices. Lee et alCitation21 found that compared with Macintosh laryngoscope, V-MAC device provided a better laryngeal view, required a less number of intubation attempts and a shorter intubation time. In patients who were put in a right lateral position, Bhat et alCitation22 showed that the laryngeal view was improved, intubation time, airway mucosal injury and use of external laryngeal manipulation were reduced with C-MAC videolaryngoscope, but overall success rate of intubation and number of intubation attempts were comparable between C-MAC and Macintosh devices. Three RCTsCitation21,Citation23,Citation24 prove that the force exerted on maxillary incisors during laryngoscopy is lower with V-MAC and C-MAC videolaryngoscopes compared with direct laryngoscope. However, a prospective randomized parallel group study confirms that C-MAC videolaryngoscope results in significantly increased hemodynamic responses to intubation than Macintosh laryngoscope.Citation25
A retrospective analysis compared the double-lumen tube placement using Macintosh laryngoscope and C-MAC videolaryngoscope in patients without predictors of difficult intubation and showed that C-MAC device provided an improved laryngeal view and increased the ease of procedure, but did not offer any benefit on the number of intubation attempts.Citation26
Difficult airways
As the original aim of the videolaryngoscopy design was to solve the main issue of difficult airways, difficult intubation, it has rapidly become a first-line strategy for potential and/or encountered difficult intubation.Citation6 Furthermore, most of the current algorithms for difficult airway management recommend videolaryngoscopy as a rescue strategy for difficult or failed intubation with direct laryngoscopy.Citation27–Citation29 There have been many studies assessing the application and role of C-MAC videolaryngoscope in difficult airway management.
Two RCTs comparing the effectiveness of V-MAC and C-MAC videolaryngoscopes versus direct laryngoscope for orotracheal intubation in patients with predicted difficult airways demonstrate that videolaryngoscopy provides improved laryngeal views, more successful intubations on the first attempt, shorter laryngoscopy and intubation times, and decreased needs of adjuncts, but did not affect incidence of complications.Citation30,Citation31
The patients with cervical spine injury often require the use of semi-rigid cervical collar or manual in-line stabilization to prevent neck movements, which may lead to poor laryngeal view on direct laryngoscopy and lead to difficulty with intubation.Citation2 In patients with a simulated difficult airway by cervical spine immobilization, C-MAC videolaryngoscope compared with direct laryngoscope offers an improved laryngeal view,Citation15,Citation32,Citation33 but no conclusive benefits with regard to intubation time, number of intubation attempts, intubation success, and incidence of complications.Citation15,Citation32 Furthermore, the tracheal tube placement may occasionally fail despite a good laryngeal view.Citation33 In morbidly obese patients, V-MAC or C-MAC videolaryngoscope compared with Macintosh laryngoscope improves the laryngeal view and allows for fast tracheal intubation.Citation34,Citation35
In 51 patients with an unexpected Cormack and Lehane grade 3 or 4 view with Macintosh laryngoscope, the laryngeal views are improved and successful intubation is achieved with C-MAC videolaryngoscope in 49 patients (94%).Citation36 In 42 patients whose intubation attempts using Macintosh laryngoscope had failed, C-MAC videolaryngoscope produced improved laryngeal views, achieved a 86% success rate of intubation at the first attempt and a 100% total success rate of intubation without severe complications other than minor airway damage.Citation37 In a morbidly obese (body mass index [BMI] 36 kg/m2) patient, 3 attempts at Macintosh direct laryngoscopy failed with each resulting in a Cormack–Lehane grade 4 view.Citation38 However, tracheal intubation using V-MAC videolaryngoscope was successful on the first attempt. These data provide evidence for the clinical effectiveness of C-MAC videolaryngoscope as an effective rescuing device for unexpected difficult laryngoscopy or failed intubations in routine anesthesia care.
Emergency airways
Patients requiring tracheal intubations in emergency department, intensive care unit (ICU) and prehospital setting are typical emergency situations associated with hemodynamic compromise and respiratory dysfunction. Due to many reasons, these patients often have a high risk of difficult laryngoscopy and intubation, even when clinicians have adequate airway skills. If inexperienced clinicians are responsible for managing the airway under such challenging conditions, the risk of difficult laryngoscopy and intubation can be further compounded.Citation2 Thus, there are increased incidences of failed attempts and complications during emergency intubation compared with elective intubation in the operating room. Furthermore, the complications of emergency intubation have been associated independently with repeated attempts.Citation39 Given that the goal of emergency intubation is the first-attempt success, the use of videolaryngoscopy in emergency airway management has significantly increased; it has also been shown to increase intubation success rate at the first attempt.Citation40
The option to perform direct and video laryngoscopy with the same device makes C-MAC device exceptionally useful for emergency intubation. In the event of a failed direct laryngoscopy attempt, the intubators can immediately switch to the videolaryngoscopy to successfully complete the intubation without having to make a second attempt, and vice versa.Citation41,Citation42 Several observational and retrospective studies from emergency department, prehospital and ICU patients showed that a V-MAC or C-MAC device, compared with a direct laryngoscope, was associated with a significantly better visualization of the larynx and a higher proportion of successful intubations, especially for patients with predicted difficult intubations.Citation43–Citation47 Furthermore, the use of C-MAC videolaryngoscope during emergency intubation was associated with significantly fewer esophageal intubations compared with direct laryngoscopy.Citation43,Citation48,Citation49
In a retrospective analysis including 619 consecutive emergency patients, Vassiliadis et alCitation50 found that C-MAC videolaryngoscope overall did not provide improved laryngeal views than Macintosh laryngoscope, but it was superior to Macintosh laryngoscope when the Cormack–Lehane grade was at least grade 3; that is, the chance of intubation success was increased by more than 3-fold by using a C-MAC videolaryngoscope. After the emergency intubation at the first attempt fails, regardless of the initial devices used, C-MAC videolaryngoscope has been shown to be more successful than direct laryngoscope when used for the second attempt.Citation51
In the available literature, however, there are the ineffectual outcomes of V-MAC or C-MAC videolaryngoscope in emergency intubation. In the study by Brown et alCitation46 comparing direct and indirect laryngeal views obtained by V-MAC videolaryngoscope, a small percentage of patients (3%) had worse laryngeal views when switched from direct laryngoscopy to videolaryngoscopy and 6% of all intubation attempts with videolaryngoscopy failed. A multicenter, observational study by Cavus et alCitation41 evaluating C-MAC videolaryngoscope during prehospital emergency intubation performed by physicians showed a failure rate of 7.5%. In the 2 studies, the reasons for failed videolaryngoscopy included technical problems (monitor malfunctions and low battery) or obstructed views due to airway blood and secretions. Furthermore, tracheal intubation with direct laryngoscopy (using C-MAC blade as a conventional Macintosh blade) is the main rescue measure of a failed videolaryngoscopy.Citation41,Citation46
A nonrandomized group-controlled trial comparing C-MAC videolaryngoscope and direct laryngoscope in a critical care transport service demonstrates that the laryngeal view is better with C-MAC device, but number of attempt, first-pass success rate and use of rescue airways are similar between devices.Citation52 As yet, there are 3 RCTs that have compared C-MAC videolaryngoscope and direct laryngoscopy for emergency intubation and all of them also show no benefit on intubation success rate and intubation time with the videolaryngoscope.Citation49,Citation53,Citation54 In the trial by Sulser et al,Citation53 rapid sequence emergency intubation was performed by experienced anesthetists. The results showed that the laryngeal visualization was improved with C-MAC videolaryngoscope, but better laryngeal visualization did not improve intubation success rate at the first attempt and intubation time. The study by Goksu et al,Citation49 in which tracheal intubation was performed by emergency residents and attending physicians in the blunt trauma patients, demonstrated that C-MAC videolaryngoscope and direct laryngoscopy were comparable in terms of the overall intubation success rate and intubation time, despite C-MAC device provided the improved laryngeal views. The trial by Driver et alCitation54 in emergency patients did also not detect differences between direct and video laryngoscopy in the intubation success rate at the first attempt, intubation time, aspiration pneumonia, or hospital length of stay when tracheal intubation was performed by senior residents and direct laryngoscopy was used for the first attempt.
Based on available evidence from above studies on emergency intubation, it may be concluded that C-MAC videolaryngoscope can offer improved laryngeal views compared with direct laryngoscopy, but there are conflicting results about whether the improved laryngeal views may result in increased intubation success rate and decreased intubation time. Visualization of the airway on a monitor may be helpful for less experienced intubators in airway management and possibly decreases the rate of esophageal tube misplacements.
Performance of C-MAC videolaryngoscope versus other devices
There are many videolaryngoscopes available and their efficacies may be different due to their different designs and shapes. To facilitate the suitable choice of these devices for managing various airway conditions, comparing performance of different videolaryngoscopes in patients with diverse conditions is needed. In patients with normal airways requiring orotracheal intubation, Lee et alCitation55 compared the Bonfils intubation fiberscope and C-MAC videolaryngoscope and showed that intubation success rate at the first attempt was not different between the 2 devices, but intubation with C-MAC device required a shorter time, and resulted in significantly attenuated hemodynamic responses. In healthy volunteers undergoing awake upright laryngoscopy, Glidescope videolaryngoscope provides the superior views to C-MAC videolaryngoscope, but laryngoscopy time and number of intubation attempts are similar between devices.Citation56
In a prospective RCT performed on patients with predicted difficult airways, Glidescope videolaryngoscope enables significantly better laryngeal views than C-MAC videolaryngoscope, but laryngoscopy time, number of intubation attempts and intubation success rate did not differ between instruments.Citation57 In an RCT comparing McGrath and C-MAC videolaryngoscopes in adult patients with potential difficult airways, Ng et alCitation58 found that the C-MAC device allowed a quicker intubation time, a fewer number of intubation attempts and a greater ease of intubation compared with the McGrath device. In patients with cervical spine disorders and immobilization, Glidescope and C-MAC videolaryngoscopes provide comparable laryngeal views, but the C-MAC device has a higher first-attempt failure rate, and requires significantly more intubation attempts and optimizing manoeuvers.Citation59 Moreover, a RCT trial in obese patients undergoing bariatric surgery shows that V-MAC videolaryngoscope significantly reduces the intubation time compared with the McGrath and Glidescope devices, and requires a fewer number of intubation attempts and a less frequent use of ancillary intubating devices compared to McGrath device.Citation35 In addition, a retrospective study comparing Glidescope and C-MAC videolaryngoscopes in patients requiring emergency intubation showed that both the first-pass success rate and overall success rate were similar with 2 devices.Citation60
By a prospective, randomized study, Yumul et alCitation61 compared C-MAC videolaryngoscope and flexible fiberoptic scope in patients with cervical spine immobilization and found that the C-MAC device significantly decreased the times required to obtain laryngeal view and successful intubation.
In a multicenter, prospective, non-randomized clinical trial comparing C-MAC and KingVision videolaryngoscopes for prehospital emergency intubation, C-MAC device provides a significantly higher intubation success rate at the first attempt and overall success rate, and needs a less number of intubation attempts, but both the devices are similar in term of intubation complication.Citation62
The above findings suggest that when attempting to secure the airway, there is no single device that is better than others in all conditions. Each device has unique properties that may be advantageous in some conditions, but limiting in other situations.Citation6 Thus, health care providers involved in airway management must master several different devices. Furthermore, videolaryngoscopes must be selected based on indications.Citation4
C-MAC videolaryngoscope and tracheal intubation teaching
Teaching direct laryngoscopy to the student may be associated with anxiety for both teacher and student. This can be attributed partly to the fact that the teacher cannot see what the intubator is (or is not) visualizing during the procedure. The videolaryngoscopy provides a shared view for both the teacher and student; that is, the high-quality, magnified picture on videolaryngoscopy monitor allows the teacher to explain the anatomy of the upper airway and procedures of laryngoscopy and intubation to student.Citation1 Also, when a student is attempting intubation, the teacher can see the monitor and provide a real-time feedback. With videolaryngoscopy, thus, the “peer over my shoulder” teaching method is displaced, and considerable time is saved and many unessential intubation attempts can be avoided.Citation5
The C-MAC videolaryngoscope is a very good tool for tracheal intubation teaching, as it has a standard Macintosh blade and thus the intubation procedure is identical to the traditional one. It has been shown that compared with the training with a direct laryngoscope, video-assisted instruction with V-MAC or C-MAC videolaryngoscope may shorten the learning curve of direct laryngoscopy and intubation for students, improve intubation success rate and decrease the rate of esophageal intubation.Citation63,Citation64 Following training, the novices trained by using C-MAC videolaryngoscope perform better with respect to number of intubation attempts, number of repositioning maneuvers required and teeth trauma in simulated difficult airway conditions compared with those trained by using Macintosh laryngoscope.Citation65 Because of a compact video system, C-MAC videolaryngoscope has also been showed to be well received by the trainees during intubation training in a simulated field hospital setting.Citation66
However, a randomized, cross-over study assessing the retention of laryngoscopy skills in medical students shows no significant difference in median intubation time after training between students trained using C-MAC and Macintosh devices, but median intubation time after a brief period of no practice is longer for the students trained by using C-MAC device compared with those trained using the Macintosh device.Citation67 This suggests that intubation skill acquisition with C-MAC videolaryngoscope can be achieved after a brief period of learning and practice, but skill maintenance requires regular practice.
Comments
Videolaryngoscopy creates a visual advantage by placing the intubator’s eye near the blade tip, beyond the obstructing anatomy of the upper airway. During the past decade, videolaryngoscopes have been receiving plenty of attention as new airway devices. In current clinical practice, videolaryngoscopy has actually been used in any instance in which tracheal intubation is required and resulted in significant changes in airway management strategy.Citation6 Videolaryngoscopy has even been considered a feasible alternative to direct laryngoscopy.Citation4,Citation68 Importantly, however, new intubation devices should prove to be at least as safe and more effective than direct laryngoscope to justify the expense of acquisition and the demand that we become proficient with them.
The available evidence shows that in patients with normal airways, V-MAC or C-MAC videolaryngoscope, compared with direct laryngoscopy, can provide comparable or better laryngeal views and exert less force on maxillary incisors, but does not offer conclusive benefits with regard to intubation time, intubation success, number of intubation attempts, use of adjuncts, and hemodynamic responses to intubation.Citation10,Citation14–Citation26 It should be noted that current airway assessment is predicated on difficult intubation with direct laryngoscopy, but a predicated difficult intubation with direct laryngoscopy does not mean that intubation will be difficult with videolaryngoscopy and vice versa.Citation69 Furthermore, a good visualization of the larynx during intubation has been shown to directly affect safety and morbidity of patients.Citation70 Thus, it is important to have high-performance devices for airway management. Given that C-MAC videolaryngoscope with a standard blade combines the benefits of direct and video laryngoscopy in one device, we agree with other authors that C-MAC video-laryngoscope may serve as a standard intubation device for routine airway management.Citation4,Citation10
The benefits of C-MAC videolaryngoscope are most significant in patients with difficult airways, as it can convert “blind” intubations into intubations under visual control. In patients with predicted or known difficult airways, C-MAC device can achieve a better laryngeal view, higher intubation success rate and shorter intubation time than direct laryngoscopy.Citation30,Citation31,Citation34,Citation35 Furthermore, C-MAC device has been shown to be an effective rescuing device for unexpectedly difficult laryngoscopy or failed intubations.Citation36–Citation38 Thus, C-MAC videolaryngoscope may produce clinically relevant improvement of intubation conditions and can be recommended for difficult airway management. In patients with a difficult airway by cervical spine immobilization, however, the intubation time may be prolonged and tracheal intubation may occasionally fail with C-MAC device despite very good laryngeal visualization.Citation32,Citation33 Furthermore, Glidescope videolaryngoscope performs better than C-MAC videolaryngoscope in patients with cervical spine immobilization.Citation59 These issues should be noted when a suitable videolaryngoscope for managing a special airway condition is selected.
For emergency airways, most observational and retrospective studies indicate that C-MAC device performs better than direct laryngoscope, especially for patients with a Cormack–Lehane grade 3 or 4.Citation41–Citation48,Citation50,Citation51 After a failed first intubation attempt in the emergency department, C-MAC device is more successful at second attempt than the direct laryngoscope.Citation51 However, all the available RCTs comparing C-MAC videolaryngoscope and direct laryngoscope for emergency intubation show no benefit on the intubation success rate and intubation time with C-MAC videolaryngoscope.Citation49,Citation53,Citation54 The detailed reasons for inconsistent findings obtained from the observational and randomized controlled studies are unclear, but several important issues may be considered. First, observational and retrospective studies have major methodological weaknesses and potentially introduce a number of confounding variables. Second, the patient’s position is not clearly descibed in most studies. This may be unimportant for videolaryngoscopy that does not require alignment of the airway axes to expose the larynx.Citation6 However, patients’ head and neck position can significantly affect performance of direct laryngoscopy that needs to align the airway axes into a more straight line.Citation71 Third, most studies require some training and practice with the studied devices prior to the study, but do not give clear definitions of competence with studied devices for intubators. Moreover, most intubations at the first attempt are done by inexperienced intubators. In fact, experience with a standard laryngoscope does not equate skill with a videolaryngoscope.Citation4 With videolaryngoscopy, the main challenges for the intubator are to become familiar with the view on the monitor, and coordinate the eyes and hands appropriately.Citation1 If intubators have more experience with direct laryngoscopy versus videolaryngoscopy, a higher intubation success rate is associated with former device. If intubators are inexperienced in direct laryngoscopy, videolaryngoscopy may be associated with better intubation success. Thus, the differences in intubation performances between C-MAC videolaryngoscope and direct laryngoscopy in these studies may be contributed to their different learning curves. It has been emphasized that for the results of a comparative study to be valid, participants must be equally proficient with each airway device to avoid bias.Citation72 Fourth, the use of neuromuscular blocking agents has been shown to improve the first-attempt success rate of emergency intubation,Citation73,Citation74 but this factor is significantly different among studies. Fifth, some studies exclude patients with anticipated or known difficult airways, though C-MAC videolaryngoscope is more effective than direct laryngoscopy for such conditions.Citation50,Citation51
It must be emphasized that when considering the role of C-MAC videolaryngoscope in securing an airway for patients requiring emergency intubation, an important fact that a device can provide 2 options of direct and video laryngoscopy cannot be neglected. That is, when one option at the first attempt fails, the intubators can immediately switch to another option to successfully complete the intubation without having to make a second attempt.Citation41,Citation42 This unique feature of C-MAC device is significantly different from the angulated videolaryngoscopes, such as C-MAC D-Blade and Glidescope devices which can only provide the videolaryngoscopic option. Given that no algorithm can reliably predict the difficult emergency intubation with direct or video laryngoscopy prior to intubation and emergency patients do not allow multiple intubation attempts,Citation50,Citation51,Citation75 we argue that the use of C-MAC videolaryngoscope with 2 options as a main device for emergency intubation may be a safe procedure and should be used as the first-line device in all emergency intubations. A recent meta-analysis of observational, retrospective and randomized data comparing video versus direct laryngoscopy for orotracheal intubation in the ICU patients shows that the first-attempt success is twice as likely to occur with the use of a videolaryngoscope.Citation40 Furthermore, a largest propensity-matched analysis comparing video and direct laryngoscopy in the ICU to date demonstrates a higher odds of first-attempt success and a lower incidence of complications with videolaryngoscopy.Citation76 Thus, some emergency medicine airway experts have called that videolaryngoscopy should replace direct laryngoscopy for tracheal intubation in all emergency patients.Citation16,Citation50,Citation51,Citation68,Citation77,Citation78
However, clinicians should bear in mind that no single device can offer a solution to all airway conditions. The C-MAC videolaryngoscope provides a high intubation success rate, but does not give a 100% success rate.Citation33,Citation41,Citation46 To manage airway conditions expeditiously and safely, the practitioners must master the several different airway devices and techniques. Furthermore, any difficult airway management strategy, including videolaryngoscopes must include a contingency plan for failure.Citation79
Finally, there are some limitations of this review. First, there are high heterogeneity among included studies, such as levels of intubators’ experience and skill with the studied devices, intubation strategies and definitions of primary outcomes. Second, none of the RCTs included in this review is a double-blinded study because it is impossible to make the intubators unaware of the devices they would use for intubation. Third, most of the studies have a small sample size and patients have different airway conditions. Fourth, many studies on difficult and emergency intubations only assess differences in intubation variables between C-MAC videolaryngoscope and direct laryngoscope, but do not evaluate the clinical outcomes, such as morbidity and mortality of patients. Thus, it is unclear whether favorable effect of C-MAC videolaryngoscope on intubation outcomes can be translated to clinical benefits. These factors may complicate the interpretation for clinical performance of C-MAC videolaryngoscope.
Conclusion
A unique feature of C-MAC videolaryngoscope with a Macintosh blade is its ability to provide both the options of direct and video laryngoscopy in the same device. It makes the use of C-MAC videolaryngoscope very appealing. As yet, the roles of C-MAC videolaryngoscope in airway management and education have been well established by published literatures. The available evidence supports that C-MAC videolaryngoscope can be used as a primary intubation tool, particularly when the intubators have less experience of airway management and preoperative airway screening suggests intubation difficulty. It may improve patient safety by avoiding unnecessary intubation attempts and facilitate learning of both direct and video laryngoscopy. Thus, the advent of C-MAC videolaryngoscope expands the armamentarium for health care providers who are involved in airway management. However, the biggest impediment to the widespread use of this device is likely to be the cost, as it is one of currently most expensive videolaryngoscopes. Furthermore, the introduction of C-MAC device in clinical practice must be accompanied by formal training programs in normal and difficult airway managements.
Authors’ contribution
FS Xue made substantial contributions to acquisition of data and interpretation of data, drafted and revised this manuscript, and is responsible for this manuscript. HX Li, YY Liu and GZ Yang made substantial contributions to acquisition of data and interpretation of data, and helped write the manuscript. All authors had read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- NiforopoulouPPantazopoulosIDemestihaTKoudounaEXanthosTVideolaryngoscopes in the adult airway management: a topical review of the literatureActa Anaesthesiol Scand20105491050106120887406
- MaldiniBHodžovićIGoranovićTMesarićJChallenges in the use of video laryngoscopesActa Clin Croat201655Suppl 14150
- PaoliniJBDonatiFDroletPReview article: videolaryngoscopy: another tool for difficult intubation or a new paradigm in airway management?Can J Anesth201360218419123233395
- KellyFECookTMSeeing is believing: getting the best out of videolaryngoscopyBr J Anaesth2016117Suppl 1913
- KaplanMBWardDSBerciGA new video laryngoscope-an aid to intubation and teachingJ Clin Anesth200214862062612565125
- XueFSLiuQJLiHXLiuYYVideolaryngoscopy assisted intubation–new era for airway managementJ Anesth Perioper Med201636258269
- AzizMBrambrinkAThe Storz C-MAC video laryngoscope: description of a new device, case report, and brief case seriesJ Clin Anesth201123214915221377082
- Green-HopkinsINaglerJEndotracheal intubation in pediatric patients using video laryngoscopy: an evidence-based reviewPediatr Emerg Med Pract2015128122
- Holm-KnudsenRThe difficult pediatric airway-a review of new devices for indirect laryngoscopy in children younger than two years of agePediatr Anesth201121398103
- CavusETheeCMoellerTKieckhaeferJDoergesVWagnerKA randomized, controlled crossover comparison of the C-MAC videolaryngoscope with direct laryngoscopy in 150 patients during routine induction of anesthesiaBMC Anesthesiol201111621362173
- LevitanRMHeitzJWSweeneyMCooperRMThe complexities of tracheal intubation with direct laryngoscopy and alternative intubation devicesAnn Emerg Med201157324024720674088
- GreenlandKBDisposable C-MAC® videolaryngoscope blade-not the same as the re-usable bladeAnesthesia2014691214021403
- CavusEKieckhaeferJDoergesVMoellerTTheeCWagnerKThe C-MAC videolaryngoscope: first experiences with a new device for videolaryngoscopy-guided intubationAnesth Analg2010110247347719917623
- van ZundertAMaassenRLeeRA Macintosh laryngoscope blade for videolaryngoscopy reduces stylet use in patients with normal airwaysAnesth Analg2009109382583119690253
- GuptaNRathGPPrabhakarHClinical evaluation of C-MAC video-laryngoscope with or without use of stylet for endotracheal intubation in patients with cervical spine immobilizationJ Anesth201327566367023475442
- BrownCA3rdPallinDJWallsRMVideo laryngoscopy and intubation safety: the view is becoming clearCrit Care Med201543371771825700064
- AgroFEDoyleDJVennariMUse of GlideScope® in adults: an overviewMinerva Anestesiol201581334235124861718
- KaplanMBHagbergCAWardDSComparison of direct and video-assisted views of the larynx during routine intubationJ Clin Anesth200618535736216905081
- ShimadaNMogiKNiwaYThe C-MAC videolaryngoscope: its utility in tracheal intubation by novice personnelMasui201261664945222746034
- SarkılarGSargınMSarıtaşTBHemodynamic responses to endotracheal intubation performed with videoand direct laryngoscopy in patients scheduled for major cardiac surgeryInt J Clin Exp Med201587114771148326379966
- LeeRAvan ZundertAAMaassenRLWieringaPAForces applied to the maxillary incisors by video laryngoscopes and the Macintosh laryngoscopeActa Anaesthesiol Scand201256222422922091734
- BhatRSanickopCSPatilMCUmraniVSDhorigolMGComparison of Macintosh laryngoscope and C-MAC video laryngoscope for intubation in lateral positionJ Anaesthesiol Clin Pharmacol201531222622925948906
- PietersBMaassenRVan EigEMaathuisBVan Den DobbelsteenJVan ZundertAIndirect videolaryngoscopy using Macintosh blades in patients with non-anticipated difficult airways results in significantly lower forces exerted on teeth relative to classic direct laryngoscopy: a randomized crossover trialMinerva Anestesiol201581884685425311949
- LeeRAvan ZundertAAMaassenRLForces applied to the maxillary incisors during video-assisted intubationAnesth Analg2009108118719119095848
- BuhariFSSelvarajVRandomized controlled study comparing the hemodynamic response to laryngoscopy and endotracheal intubation with McCoy, Macintosh, and C-MAC laryngoscopes in adult patientsJ Anaesthesiol Clin Pharmacol201632450550928096584
- PuruggananRVJacksonTAHeirJSWangHCataJPVideo laryngoscopy versus direct laryngoscopy for double-lumen endotracheal tube intubation: a retrospective analysisJ Cardiothorac Vasc Anesth201226584584822361488
- ApfelbaumJLHagbergCACaplanRAPractice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult AirwayAnesthesiology2013118225127023364566
- FrerkCMitchellVSMcNarryAFDifficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adultsBr J Anaesth2015115682784826556848
- Japanese Society of AnesthesiologistsJSA airway management guideline 2014: to improve the safety of induction of anesthesiaJ Anesth201428448249324989448
- JungbauerASchumannMBrunkhorstVBörgersAGroebenHExpected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patientsBr J Anaesth2009102454655019233881
- AzizMFDillmanDFuRBrambrinkAMComparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airwayAnesthesiology2012116362963622261795
- ByhahnCIberTZacharowskiKTracheal intubation using the mobile C-MAC video laryngoscope or direct laryngoscopy for patients with a simulated difficult airwayMinerva Anestesiol201076857758320661197
- AkbarSHOoiJSComparison between C-Mac videolaryngoscope and Macintosh direct laryngoscope during cervical spine immobilizationMiddle East J Anaesthesiol2015231435026121894
- GaszyńskiTClinical experience with the C-Mac videolaryngoscope in morbidly obese patientsAnaesthesiol Intensive Ther2014461141624643921
- YumulRElvir-LazoOLWhitePFComparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: a randomized controlled trialJ Clin Anesth201631717727185681
- PiephoTFortmuellerKHeidFMSchmidtmannIWernerCNoppensRRPerformance of the C-MAC video laryngoscope in patients after a limited glottic view using Macintosh laryngoscopyAnesthesia2011661211011105
- KilicaslanATopalATavlanAErolAOtelciogluSEffectiveness of the C-MAC video laryngoscope in the management of unexpected failed intubationsBraz J Anesthesiol2014641626524565390
- MaassenRLeeRvan ZundertACooperRThe videolaryngoscope is less traumatic than the classic laryngoscope for a difficult airway in an obese patientJ Anesth200923344544819685133
- CookTMWoodallNHarperJBengerJMajor complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departmentsBr J Anaesth2011106563264221447489
- De JongAMolinariNConseilMVideo laryngoscopy versus direct laryngoscopy for orotracheal intubation in the intensive care unit: a systematic review and meta analysisIntensive Care Med201440562963924556912
- CavusECalliesADoergesVThe C-MAC videolaryngoscope for prehospital emergency intubation: a prospective, multicentre, observational studyEmerg Med J201128865065321422034
- SaklesJCMosierJMPatanwalaAEArcarisBDickenJMThe Utility of the C-MAC as a Direct Laryngoscope for Intubation in the Emergency DepartmentJ Emerg Med201651434935727471132
- SaklesJCMosierJChiuSCosentinoMKalinLA comparison of the C-MAC video laryngoscope to the Macintosh direct laryngoscope for intubation in the emergency departmentAnn Emerg Med201260673974822560464
- NoppensRRGeimerSEiselNDavidMPiephoTEndotracheal intubation using the C-MAC video laryngoscope or the Macintosh laryngoscope: a prospective, comparative study in the ICUCrit Care2012163R10322695007
- HossfeldBFreyKDoergesVLamplLHelmMImprovement in glottic visualization by using the C-MAC PM videolaryngoscope as a first-line device for out-of-hospital emergency tracheal intubation: An observational studyEur J Anaesthesiol201532642543125886716
- BrownCA3rdBairAEPallinDJLaurinEGWallsRMNational Emergency Airway Registry (NEAR) InvestigatorsImproved glottic exposure with the Video Macintosh Laryngoscope in adult emergency department tracheal intubationsAnn Emerg Med2010562838820202720
- JonesBMAgrawalASchulteTEAssessing the efficacy of video versus direct laryngoscopy through retrospective comparison of 436 emergency intubation casesJ Anesth201327692793023760512
- SaklesJCJavedaniPPChaseEGarst-OrozcoJGuillen-RodriguezJMStolzUThe use of a video laryngoscope by emergency medicine residents is associated with a reduction in esophageal intubations in the emergency departmentAcad Emerg Med201522670070725996773
- GoksuEKilicTYildizGUnalAKartalMComparison of the C-MAC video laryngoscope to the Macintosh laryngoscope for intubation of blunt trauma patients in the EDTurk J Emerg Med2016162535627896321
- VassiliadisJTzannesAHitosKBrimbleJFoggTComparison of the C-MAC video laryngoscope with direct Macintosh laryngoscopy in the emergency departmentEmerg Med Australas201527211912525640845
- SaklesJCMosierJMPatanwalaAEDickenJMKalinLJavedaniPPThe C-MAC video laryngoscope is superior to the direct laryngoscope for the rescue of failed first-attempt intubations in the emergency departmentJ Emerg Med201548328028625498851
- GuyetteFXFarrellKCarlsonJNCallawayCWPhrampusPComparison of video laryngoscopy and direct laryngoscopy in a critical care transport servicePrehosp Emerg Care201317214915423231426
- SulserSUbmannDSchlaepferMC-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department: a randomized clinical trialEur J Anaesthesiol2016331294394827533711
- DriverBEPrekkerMEMooreJCSchickALReardonRFMinerJRDirect versus video laryngoscopy using the C-MAC for tracheal intubation in the emergency department, a randomized controlled trialAcad Emerg Med201623443343926850232
- LeeAHNorNMIzahamAYahyaNTangSSManapNAComparison of the Bonfils intubation fibrescope versus C-MAC videolaryngoscopeMiddle East J Anaesthesiol201623551752527487637
- DrenguisASCarlsonJNGlideScope versus. C-MAC for awake upright laryngoscopyJ Emerg Med201549336136825989968
- SerockiGBeinBScholzJDörgesVManagement of the predicted difficult airway: a comparison of conventional blade laryngoscopy with video-assisted blade laryngoscopy and the GlideScopeEur J Anaesthesiol2010271243019809328
- NgIHillALWilliamsDLLeeKSegalRRandomized controlled trial comparing the McGrath videolaryngoscope with the C-MAC videolaryngoscope in intubating adult patients with potential difficult airwaysBr J Anaesth2012109343944322677878
- BrückSTrautnerHWolffAComparison of the C-MAC and GlideScope videolaryngoscopes in patients with cervical spine disorders and immobilizationAnesthesia2015702160165
- MosierJChiuSPatanwalaAESaklesJCA comparison of the GlideScope video laryngoscope to the C-MAC videolaryngoscope for intubation in the emergency departmentAnn Emerg Med201361441442023374414
- YumulRElvir-LazoOLWhitePFComparison of the C-MAC video laryngoscope to a flexible fiberoptic scope for intubation with cervical spine immobilizationJ Clin Anesth201631465227185677
- BurnettAMFrasconeRJWewerkaSSComparison of success rates between two video laryngoscope systems used in a prehospital clinical trialPrehosp Emerg Care201418223123824400965
- Howard-QuijanoKJHuangYMMatevosianRKaplanMBSteadmanRHVideo-assisted instruction improves the success rate for tracheal intubation by novicesBr J Anaesth2008101456857218676418
- HerbstreitFFassbenderPHaberlHKehrenCPetersJLearning endotracheal intubation using a novel videolaryngoscope improves intubation skills of medical studentsAnesth Analg2011113358659021680859
- LowDHealyDRasburnNThe use of the BERCI DCI Video Laryngoscope for teaching novices direct laryngoscopy and tracheal intubationAnesthesia2008632195201
- BoedekerBHBernhagenMAMillerDJMiljkovicNKuperGMMurrayWBField use of the STORZ C-MAC video laryngoscope in intubation training with the Nebraska National Air GuardStud Health Technol Inform2011163808221335765
- HunterIRamanathanVBalasubramanianPEvansDAHardmanJGMcCahonRARetention of laryngoscopy skills in medical students: a randomized, cross-over study of the Macintosh, A.P. Advance™, C-MAC and Airtraq® laryngoscopesAnesthesia2016711011911197
- ZaouterCCalderonJHemmerlingTMVideolaryngoscopy as a new standard of careBr J Anaesth2014114218118325150988
- AzizMFBrambrinkAMHealyDWSuccess of intubation rescue techniques after failed direct laryngoscopy in adults: a retrospective comparative analysis from the multicenter perioperative outcomes groupAnesthesiology2016125465666627483124
- CookTMWoodallNFrerkCFourth National Audit ProjectMajor complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anesthetists and the Difficult Airway Society. Part 1: anesthesiaBr J Anaesth2011106561763121447488
- El-OrbanyMWoehlckHSalemMRHead and neck position for direct laryngoscopyAnesth Analg2011113110310921596871
- BehringerECKristensenMSEvidence for benefit versus novelty in new intubation equipmentAnesthesia201166Suppl 25764
- LyonRMPerkinsZBChatterjeeDLockeyDJRussellMQKent, Surrey & Sussex Air Ambulance TrustSignificant modification of traditional rapid sequence induction improves safety and effectiveness of pre-hospital trauma anesthesiaCrit Care20151913425879683
- MarschSCSteinerLBucherESuccinylcholine versus rocuronium for rapid sequence intubation in intensive care: a prospective, randomized controlled trialCrit Care2011154R19921846380
- NattBSMaloJHypesCDSaklesJCMosierJMStrategies to improve first attempt success at intubation in critically ill patientsBr J Anaesth2016117Suppl 1i60i6827221259
- HypesCDStolzUSaklesJCVideo laryngoscopy improves odds of first attempt success at intubation in the ICU: a Propensity-matched analysisAnn Am Thorac Soc201613338239026653096
- ChhaviSAbhyudayKParinLVideo laryngoscope as the new standard of care in trauma EDAm J Emerg Med20163471313131427165719
- SaklesJCRodgersRKeimSMOptical and video laryngoscopes for emergency airway managementIntern Emerg Med20083213914318274712
- ZaouterCCalderonJHemmerlingTMVideolaryngoscopy as a new standard of careBr J Anaesth2015114218118325150988
- Karl Storz GmbH & Co. KG Tuttlingen, Germany Available from: http://www.karlstorz.de/cps/rde/xchg/SID-E5A329DA-B9AE794B/karlstorz-en/hs.xsl/9549.htmAccessed May 4, 2017