
Abstract
Background
Proprotein convertase subtilisin/kexin type 9 inhibitors, Praluent (alirocumab [ALI]) and Repatha (evolocumab [EVO]) have been approved as adjuncts to the standard-of-care maximal-tolerated dose (MTD) of low-density lipoprotein cholesterol (LDLC)-lowering therapy (LLT), statin therapy, in heterozygous (HeFH) (ALI or EVO) or homozygous (EVO) familial hypercholesterolemia, or clinical atherosclerotic cardiovascular disease (CVD) where LDLC lowering is insufficient (both). Since LDLC lowering has been revolutionized by ALI and EVO, specialty pharmaceutical pricing models will be applied to a mass market.
Methods
We applied US Food and Drug Administration (FDA) and insurance eligibility criteria for ALI and EVO to 1090 hypercholesterolemic patients serially referred over 3 years who then received ≥2 months maximal-tolerated dose of standard-of-care LDL cholesterol-lowering therapy (MTDLLT) with follow-up LDLC ≥70 mg/dL. MTDLLT did not include ALI or EVO, which had not been commercially approved before completion of this study.
Results
Of the 1090 patients, 140 (13%) had HeFH by clinical diagnostic criteria and/or CVD with LDLC >100 mg/dL despite ≥2 months on MTDLLT, meeting FDA insurance criteria for ALI or EVO therapy. Another 51 (5%) patients were statin intolerant, without HeFH or CVD.
Conclusion
If 13% of patients with HeFH-CVD and LDLC >100 mg/dL despite MTDLLT are eligible for ALI or EVO, then specialty pharmaceutical pricing models (~$14,300/year) might be used in an estimated 10 million HeFH-CVD patients. Whether the health care savings arising from the anticipated reduction of CVD events by ALI or EVO justify their costs in populations with HeFH-CVD and LDLC >100 mg/dL despite MTDLLT remains to be determined.
Introduction
Proprotein convertase subtilisin/kexin type 9 (PCSK9) is an enzyme expressed throughout the body,Citation1,Citation2 which functions to promote lipoprotein homeostasis, and has been implicated in many other disease processes.Citation1,Citation3,Citation4 PCSK9 binds low-density lipoprotein (LDL) receptors, promoting LDL receptor degradation. This process prevents the receptor from returning to the cell surface, where the receptor could remove more LDL particles. However, if the PCSK9 molecule is blocked, LDL receptors are recycled, returned to the surface of cells, and remove more LDL particles from circulation. Further, PCSK9 inhibitors have been shown to reduce lipoprotein (a) [Lp(a)], which has been associated independently with cardiovascular risk.Citation5–Citation7 PCSK9 inhibition has shown great promise to lower LDL concentrations and decrease cardiovascular risk.Citation8,Citation9
The newly approved PCSK9 inhibitors, alirocumab (ALI) and evolocumab (EVO), are the most powerful agents currently available for lowering low-density lipoprotein cholesterol (LDLC).Citation10–Citation17 EVO facilitates regression of coronary atherosclerotic plaque, as shown by the GLAGOV Trial.Citation16,Citation18 ALI or EVO is approved for patients with heterozygous familial hypercholesterolemia (HeFH), EVO for homozygous familial hypercholesterolemia, and both for patients with atherosclerotic cardiovascular disease (CVD) unable to achieve LDLC goals despite maximal-tolerated standard-of-care dose (MTD) LDL cholesterol-lowering therapy (LLT), specifically statins, including zero-dose tolerance (statin intolerance).Citation13,Citation15,Citation19 Preliminary results of safety- and efficacy-controlled clinical trials, although not powered or designed to definitively assess CVD events, revealed a 50% risk reduction in CVD events.Citation13–Citation15 Building on this preliminary data, Sabatine et al documented a 15% reduction of CVD events.Citation20
Priced as a specialty drug for a common disease, insurance companies have implemented prior authorizations to limit use to high-risk patients who meet approved specifications. The process of obtaining prior authorization is arduous, requiring significant amount of uncompensated time and effort. This process requires an estimated 4–6 hours per patient to navigate the prior authorization system.Citation21 In our center the prior authorization process takes ~6 hours of uncompensated staff time per patient. Despite this considerable amount of work, access to valuable PCSK9 inhibitors is still denied at times. The insurance-imposed barrier requires a streamlined process of appropriate selection and documentation to ensure medication approval without significant amounts of patient, staff, and clinician frustration. To meet this need, frameworks have been developed to identify appropriate patients for PCSK9 inhibitor therapy. Saeed et al have published an algorithm to specifically identify eligible patients and facilitate the prior authorization process for PCSK9 inhibitors.Citation21
If the annual cost of the ALI or EVO were to remain ~$14,000–14,600 per patient, then specialty pharmaceutical pricing models previously reserved for drugs that benefited limited patient populations will collide with prospective treatment cohorts in the tens of millions of patients with HeFH and/or CVD, or at high risk for CVD, optimally treated with ALI or EVO.Citation13–Citation15,Citation22–Citation24 We have previously applied US Food and Drug Administration (FDA)-approved and commercial insurance eligibility criteria for PCSK9 inhibitor use in 734 patients serially referred to our cholesterol center and receiving ≥2 months maximal-tolerated dose of standard-of-care LDL cholesterol-lowering therapy (MTDLLT) with follow-up LDLC ≥70 mg/dL.Citation22 We reported that 30% of these 734 hypercholesterolemic patients had clinically defined HeFH and/or CVD and retained LDLC >100 mg/dL despite MTDLLT,Citation22 thus meeting FDA and commercial insurance eligibility for ALI or EVO treatment using LDLC goal-based guidelines.Citation25,Citation26 From our initial assessment,Citation22 we speculated that ALI or EVO might be given to an estimated 13–23 million patients, costing $185–342 billion/year, but with an estimated 50% reduction in CVD events,Citation13,Citation15 resulting in $245 billion/year in savings to society, between the ALI or EVO costs of $185–342 billion.Citation22 Using a simulation model of US adults aged 35–94 years, Kazi et al concluded that “PCSK9 inhibitor use in all eligible patients was estimated to reduce cardiovascular care costs by $29 billion over 5 years, but drug costs increased by $592 billion (a 38% increase over 2015 prescription drug expenditures)”.Citation27
In a new, previously unstudied group of 1090 hypercholesterolemic patients serially referred over 3 years for diagnosis and treatment of high LDLC, who then received ≥2 months MTDLLT, but maintained LDLC ≥70 mg/dL, our specific aim was to apply FDA and insurance eligibility criteria for ALI and EVO, and estimate costs of therapy and costs to society.
Materials and methods
The study followed a protocol (12-03) approved by the Jewish Hospital Institutional Review board, with signed informed consent.
We assessed 1090 previously unstudied and unreported hypercholesterolemic patients serially referred to our Cholesterol Center over 3 years up to June 2016, who subsequently received ≥2 months of MTDLLT, with last follow-up LDLC ≥70 mg/dL. All patients were instructed in a cholesterol-lowering diet by a registered dietitian, and received MTDLLT, predominantly with statins; a small percentage took ezetimibe and/or colesevelam, either with or without statins. None of these patients received PCSK9 inhibitors ALI or EVO because they received MTDLLT before commercial release of ALI or EVO.
After an overnight fast, lipids and lipoprotein cholesterols were serially measured by LabCorp with direct measurement of LDLC if triglycerides were >400 mg/dL. Some but not all patients had initial measurement of Lp(a). HeFH was defined by LDLC ≥190 mg/dL and the presence of tendon xanthomas and/or by hypercholesterolemic first-degree relatives (Simon Broome criteriaCitation28). CVD included documented coronary, carotid, aortic, or peripheral artery atherosclerosis, as well as transient ischemic attack and ischemic stroke. While statin intolerance is a controversial issue and appropriate documentation of statin intolerance is difficult,Citation29 we accepted patients intolerant to ≥3 statin medications because of development of myalgia–myositis within 2 weeks after initiation of statin therapy as “statin intolerant.”
Statistical methods
Data were processed using SAS version 9.4. Comparisons of entry LDLC and levels after 2 months on MTDLLT were made with paired Wilcoxon nonparametric tests.
Results
The 1090 hypercholesterolemic patients had LDLC ≥70 mg/dL despite ≥2 months MTDLLT. Mean±SD and median LDLC of the 1090 patients were 121±42 and 113 mg/dL at study entry, and 101±29, 94 mg/dL after ≥2 months on MTDLLT. Of the 1090 patients, 138 (13%) had HeFH by clinical diagnosis, 245 (22%) had CVD, and 96 (9%) were statin intolerant (). Of the 245 patients who had CVD, their first CVD event was at age 62±13, median 63 years. After ≥2 months on MTDLLT, mean±SD and median LDLC in patients with HeFH were 126±45 and 121 mg/dL, 94±24 and 86 mg/dL in those with CVD events, and 118±42 and 111 mg/dL in statin-intolerant patients ().
Figure 1 HeFH and atherosclerotic CVD in 1090 patients with LDLC ≥70 mg/dL after ≥2 months maximal-tolerated cholesterol-lowering therapy.
Abbreviations: CVD, cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; LDLC, low-density lipoprotein cholesterol; MTDLLT, maximal-tolerated dose of standard-of-care LDL cholesterol-lowering therapy; PCSK9, proprotein convertase subtilisin/kexin type 9.
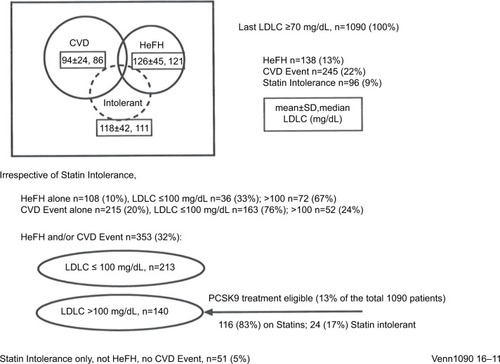
Of the 1090 patients, 353 (32%) had HeFH and/or a CVD event (). Mean±SD and median LDLC at entry in these 353 patients were 137±53 mg/dL and 127 mg/dL, and after 2 months of MTDLLT, had fallen to 105±36 and 93 mg/dL, p<0.0001. Of these 353 patients, 213 (60%) had LDLC ≤100 mg/dL on MTDLLT, while 140 (13% of the original 1090 patients) had LDLC >100 mg/dL on MTDLLT (). Mean±SD Lp(a) for these 353 patients was 40±48, median 21 mg/dL. Patients with elevated Lp(a), defined as ≥35 mg/dL, comprised 37% of this population ().
Table 1 LDLC in 353 patients with HeFH and/or CVD at entry and after 2 months on maximal-tolerated LDLC-lowering therapy
In the 353 patient population, 140 patients were eligible by both FDA and commercial insurance criteria for ALI or EVO treatment, by virtue of having HeFH and/or CVD (). Within these 140 patients, 116 (83%) were taking statins, and 24 (17%) were unable to take any statins, being intolerant to ≥3 different statins (). In these 140 patients, median LDLC at entry was 147 mg/dL, and at 2 months on MTDLLT, 132 mg/dL, p=0.002 (). Mean±SD Lp(a) for this group (n=84) was 40±48, median 23 mg/dL. Lp(a) ≥35 mg/dL was found in 37% of these patients (). In the 213 patients whose follow-up LDLC on MTDLLT was ≤100 mg/dL (; ), mean±SD and median initial LDLC was 126±50 and 113 mg/dL. On follow-up these values decreased to 83±9 and 82 mg/dL, respectively, p<0.0001 ().
In the full cohort of 1090 patients, statin intolerance was present in 96 (9%) patients, and in those with neither HeFH nor CVD, in 51 (5%) ().
Of the 140 patients having HeFH and/or a CVD event with LDLC >100 mg/dL on MTDLLT (), 72 had HeFH alone, with LDLC on therapy 150±44, median 144 mg/dL, 52 had CVD events alone, with LDLC on therapy 121±19, median 113 mg/dL, and 16 had both HeFH and CVD, with LDLC on therapy 140±24, median 139 mg/dL. In the 68 patients with CVD, the first CVD event occurred at age 61±12, median 60 years.
Discussion
ALI and EVO are the most powerful agents currently available for lowering LDLC.Citation10,Citation12–Citation16 Further studies have shown that the drugs are also able to decrease Lp(a),Citation6,Citation7 a molecule implicated to work synergistically with LDLC to cause CVD events.Citation30–Citation33 PCSK9 inhibitors were previously thought to decrease CVD events by 50%Citation13–Citation15,Citation24; more recent outcomes data have shown a 15%–20% reduction.Citation24 Priced as a specialty drug for a common disease, $14,000–14,600 per patient annually, the cost of the drug class has been highly controversial as the treatment cohort may reach in the tens of millions of patients, thereby significantly increasing the cost of cardiovascular care.
Our current analysis is focused on those high-risk patients for whom ALI or EVO is specifically indicated,Citation13–Citation15 restricted by medical insurance carriers, as an adjunct to MTDLLT in adults with HeFH or CVD who require additional lowering of LDLC. The population cost of ALI or EVO therapy largely depends on the number of subjects judged to be at high risk by virtue of HeFH with high LDLC,Citation34–Citation36 and/or by CVD with LDLC above target goals,Citation25 despite MDTLLT. At the bottom end of the number of patients with HeFH eligible for ALI or EVO, genetic testing within a single US health care system provided an estimated prevalence of HeFH of 0.39% in unselected patients, and 0.84% in those recruited from the cardiac catheterization laboratory.Citation37 Highlighting the undertreatment of HeFH variant carriers,Citation38 only 46% of HeFH carriers had LDLC on statin therapy <100 mg/dL,Citation37 the on-therapy cutpoint used in our current study to identify candidates with HeFH and/or CVD for ALI or EVO treatment. Retrospectively applying clinical criteria for diagnosis of HeFH to the same cohort, probable HeFH was diagnosed in 24% of familial hypercholesterolemic variant carriers.Citation37 Large-scale, whole-exome sequencing studies suggest that HeFH has a prevalence of ~1 in 217 (0.46%) northern European individuals.Citation39 At the upper end of the number of patients with HeFH eligible for ALI or EVO, in 313 patients with severe hypercholesterolemia (LDLC >194 mg/dL), Wang et alCitation40 reported that 47.3% had monogenic familial hypercholesterolemia, 53.7% if polygenic scores were present, and 67.1% with extreme polygenic scores.
Of our 1090 patients in the current study referred for diagnosis and treatment of hypercholesterolemia, 140 (13%) were eligible for ALI or EVO treatment by virtue of HeFH and/or CVD events and LDLC >100 mg/dL after 2 months of MTDLLT. In a previously reported cohort of 734 patients referred for diagnosis and treatment of hyperlipidemia,Citation22 30% would be eligible for ALI or EVO therapy by virtue of HeFH and/or CVD and LDLC >100 mg/dL despite MTDLLT. The previously reported cohort of 734 patients had much higher LDLC after ≥2 months MTDLLT, with LDLC 25th, 50th, and 75th percentiles 89, 105, and 141, significantly higher than 80, 94, and 114 mg/dL in the current 1090 patients. The previously reported cohortCitation22 had 48% of patients with HeFH and/or CVD compared to 32% in the current study. These differences in sequentially analyzed referral cohorts emphasize that the percentage of hypercholesterolemic patients eligible for PCSK9 inhibitor therapy depends on the severity of hypercholesterolemiaCitation40 in the referred population.
In the NHANES 2003–2006 general population data,Citation36 27% of subjects had high LDLC. In a 1999–2010 general population survey, LDLC was ≥130 mg/dLCitation35 in 28% of adults. If 21%–36.7%Citation19,Citation35,Citation36,Citation41 of the general adult US population is judged to have high LDLC, then a high LDLC cohort would include an estimated 45–78 million subjects. Extrapolating from our referral cohort where 13% of hypercholesterolemic patients had HeFH and/or CVD with LDLC ≥100 mg/dL despite MTDLLT, it is possible that 5.9–10 million patients (13% of 45–78 million) might be candidates for treatment with ALI or EVO.
As for the general population, hypercholesterolemia is undertreated.Citation19,Citation42 Thirty-seven percent (78 million) adults (>21 years) were eligible for cholesterol-lowering medication, but of this group, only 55% were actively taking a cholesterol-lowering medication (~90% a statin drug).Citation19
The advent of large-scale genetic identificationCitation37,Citation40 of hypercholesterolemia, particularly in a population referred for diagnosis and therapy of hypercholesterolemia like oursCitation22 and others,Citation40 might increase the treatment population, particularly for HeFH, adding to our projected 10 million adults identified clinically.
Large numbers of subjects with elevated LDLC fail to achieve treatment targets,Citation43–Citation46 for many reasons.Citation43,Citation47,Citation48 Beyond statin effects, ALI and EVO should optimize LDLC in most patients with HeFH, CVD, and statin intolerance.Citation10,Citation14,Citation15,Citation18,Citation24,Citation26,Citation49 The paradigm-shifting improvement in LDLC lowering by ALI or EVO,Citation13,Citation15,Citation50 however, comes at an annual price of $14,000–14,600 per patient.
Using a simulation model of US adults aged 35–94 years, Kazi et alCitation27 concluded that “…reducing annual drug costs to $4536 per patient or less would be needed for PCSK9 inhibitors to be cost-effective at <$100,000 per QALY.” Rather than a simulation model, our estimates of candidates for ALI or EVO are based on real-world referrals for diagnosis and therapy of hypercholesterolemia. For the 10 million eligible patients based on the characteristics of our current hypercholesterolemic referral group, at $14,000/patient, yearly costs of ALI or EVO might total $140 billion. In 2010, CVD-related direct medical costs in the USA were estimated to be $273 billion, and indirect costs $172 billion, $445 billion total.Citation51 If ALI or EVO therapy reduced CVD event rates by 15%,Citation13,Citation15,Citation20,Citation50 then using 2010 direct and indirect medical cost estimates, ~$67 billion would be saved. If using the secondary endpoint data (decrease of cardiovascular death, myocardial infarction, or stroke by 20%) reported by Sabatine et alCitation20 then ~$89 billion would be saved. The researchers also reported an increase in the magnitude of risk reduction in both their primary endpoints and secondary endpoints – 12%–19% and 16%–25%, respectively, from the first year to the second year. If these risk reductions continue with prolonged use of PCSK9 inhibitors, we may see further cost savings. Programs targeted to prevention of CVD should provide substantial overall cost savings.Citation52,Citation53 Studies with statinsCitation54 have previously reported that prevention or reduction in CVD events results in overall cost savings, and it is possible that PCSK9 inhibitors could reduce CVD events a further 15%–20% beyond statin therapy.Citation13,Citation15,Citation20
Estimating from our data, if CVD were reduced by 15%Citation20 then CVD care would save $67 billion. For 10 million patients, PCSK9 inhibitors cost should be less than $6,700 per patient per year for the savings to outweigh the costs. Likewise, if CVD is reduced by 20%,Citation20 CVD care is reduced by ~$89 billion. From our data we estimate that treating ~10 million patients, the cost of PCSK9 inhibitors should be <$8,900 per patient per year for care savings to outweigh the costs of the expensive, specialty drug.
Overall costs to society also need to include analysis of any potential adverse effects arising from ALI or EVO use. In a meta-analysis of 25 randomized controlled trials with PCSK9 inhibitors, Zhang et alCitation50 “detected largely no significant difference in major adverse events rates between PCSK9 inhibitor therapy and placebo and no difference between different dosages of EVO.” Within this frame of reference,Citation50 we speculate that costs to society arising from adverse effects specifically attributed to ALI or EVO may be minimal.
Strengths of our study include documentation that, of patients referred to a regional center for therapy of high LDLC, ≥70 mg/dL despite MTDLLT, 32% had HeFH and/or CVD, and 13% retained LDLC >100 mg/dL despite MTDLLT, meeting both FDA indicationsCitation14 and commercial insurance coverage eligibility.
Limitations of our study include bias toward higher LDLC and CVD by virtue of referral to a regional cholesterol treatment center, which would increase the percentage of hypercholesterolemic patients with HeFHCitation40 and/or CVD eligible for insurance coverage of ALI or EVO.
Conclusions
Of our 1090 patients in the current study referred for diagnosis and treatment of hypercholesterolemia, 140 (13%) were eligible for ALI or EVO treatment by virtue of HeFH and/or CVD events and LDLC >100 mg/dL after 2 months of MTDLLT.
For the 10 million eligible patients based on the characteristics of our current hypercholesterolemic referral group, at $14,000/patient, yearly costs of ALI or EVO might total $140 billion. In 2010, CVD-related direct medical costs in the United States were estimated to be $273 billion, and indirect costs $172 billion, $445 billion total.Citation51 If ALI or EVO therapy reduced CVD event rates by 15%,Citation13,Citation15,Citation20,Citation50 then using 2010 direct and indirect medical cost estimates, ~$67 billion would be saved. If using the secondary endpoint data (decrease of cardiovascular death, myocardial infarction, or stroke by 20%) reported by Sabatine et alCitation20 then ~$89 billion would be saved.
Whether the health care savings arising from the anticipated reduction of CVD on the ALI or EVO justify the broad use of these specialty priced agents remains to be determined.
Authors’ contribution
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data. All were involved in the drafting, revising, and finalization of the article. Further, all authors agree to be accountable for the accuracy and integrity of the work.
Acknowledgments
The study followed a protocol approved by the Jewish Hospital Institutional Review Board. The data sets used and analyzed during the current study are available from the corresponding author upon request ([email protected]). Support was provided from the Lipoprotein Research Fund of the Jewish Hospital of Cincinnati.
Disclosure
The authors report no conflicts of interest in this work.
References
- SeidahNGBenjannetSWickhamLThe secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiationProc Natl Acad Sci U S A2003100392893312552133
- NorataGDTavoriHPirilloAFazioSCatapanoALBiology of pro-protein convertase subtilisin kexin 9: beyond low-density lipoprotein cholesterol loweringCardiovasc Res2016112142944227496869
- IbarretxeDGironaJPlanaNCirculating PCSK9 in patients with type 2 diabetes and related metabolic disordersClin Investig Arterioscler20162827178
- ZhangLSongKZhuMProprotein convertase subtilisin/kexin type 9 (PCSK9) in lipid metabolism, atherosclerosis and ischemic strokeInt J Neurosci2016126867568026040332
- FerdinandKCNasserSAPCSK9 Inhibition: discovery, current evidence, and potential effects on LDL-C and Lp(a)Cardiovasc Drugs Ther201529329530826068408
- RaalFJGiuglianoRPSabatineMSPCSK9 inhibition-mediated reduction in Lp(a) with evolocumab: an analysis of 10 clinical trials and the LDL receptor’s roleJ Lipid Res20165761086109627102113
- RaalFJGiuglianoRPSabatineMSReduction in lipoprotein(a) with PCSK9 monoclonal antibody evolocumab (AMG 145): a pooled analysis of more than 1,300 patients in 4 phase II trialsJ Am Coll Cardiol201463131278128824509273
- JosephLRobinsonJGProprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition and the future of lipid lowering therapyProg Cardiovasc Dis2015581193125936907
- WeinreichMFrishmanWHAntihyperlipidemic therapies targeting PCSK9Cardiol Rev201422314014624407047
- EverettBMSmithRJHiattWRReducing LDL with PCSK9 inhibitors–the clinical benefit of lipid drugsN Engl J Med2015373171588159126444323
- LeporNEKereiakesDJThe PCSK9 inhibitors: a novel therapeutic target enters clinical practiceAm Health Drug Benefits20158948348926834934
- LipinskiMJBenedettoUEscarcegaROThe impact of proprotein convertase subtilisin-kexin type 9 serine protease inhibitors on lipid levels and outcomes in patients with primary hypercholesterolaemia: a network meta-analysisEur Heart J201637653654526578202
- RobinsonJGFarnierMKrempfMEfficacy and safety of alirocumab in reducing lipids and cardiovascular eventsN Engl J Med2015372161489149925773378
- RobinsonJGKasteleinJJPCSK9 inhibitors and cardiovascular eventsN Engl J Med20153738774
- SabatineMSGiuglianoRPWiviottSDEfficacy and safety of evolocumab in reducing lipids and cardiovascular eventsN Engl J Med2015372161500150925773607
- ReinerZPCSK9 inhibitors–past, present and futureExpert Opin Drug Metab Toxicol201511101517152126329686
- PecinIReinerZAlirocumab: targeting PCSK9 to treat hypercholesterolemiaDrugs Today (Barc)2015511268168726798848
- NichollsSJPuriRAndersonTEffect of evolocumab on progression of coronary disease in statin-treated patients: the GLAGOV randomized clinical trialJAMA2016316222373238427846344
- MercadoCDeSimoneAKOdomEGillespieCAyalaCLoustalotFPrevalence of cholesterol treatment eligibility and medication use among adults - United States, 2005–2012MMWR Morb Mortal Wkly Rep201564471305131126633047
- SabatineMSGiuglianoRPKeechACEvolocumab and clinical outcomes in patients with cardiovascular diseaseN Engl J Med2017376181713172228304224
- SaeedAViraniSSJonesPHNambiVZochDBallantyneCMA simplified pathway to proprotein convertase subtilisin/kexin type 9 inhibitor prior authorization approval: a lipid clinic experienceJ Clin Lipidol201711359659928506382
- GlueckCJShahPGoldenbergNEligibility for PCSK9 treatment in 734 hypercholesterolemic patients referred to a regional cholesterol treatment center with LDL cholesterol >/=70 mg/dl despite maximal tolerated cholesterol lowering therapyLipids Health Dis20161515526968977
- RothEMAlirocumab for hyperlipidemia: ODYSSEY phase III clinical trial results and US FDA approval indicationsFuture Cardiol201612211512826785741
- SabatineMSWassermanSMSteinEAPCSK9 inhibitors and cardiovascular eventsN Engl J Med20153738774775
- GrundySMCleemanJIMerzCNImplications of recent clinical trials for the national cholesterol education program adult treatment panel III guidelinesCirculation2004110222723915249516
- ShrankWHBarlowJFBrennanTANew therapies in the treatment of high cholesterol: an argument to return to goal-based lipid guidelinesJAMA2015314141443144426258765
- KaziDSMoranAEBibbins-DomingoKCost-effectiveness of PCSK9 inhibitor therapy-replyJAMA2016316202152
- Risk of fatal coronary heart disease in familial hypercholesterolaemiaScientific Steering Committee on behalf of the Simon Broome Register GroupBMJ199130368078938961933004
- RosensonRSBakerSKJacobsonTAKopeckySLParkerBAThe national lipid association’s muscle safety expertPAn assessment by the statin muscle safety task force: 2014 updateJ Clin Lipidol201483 SupplS58S7124793443
- DaneshJCollinsRPetoRLipoprotein(a) and coronary heart disease. Meta-analysis of prospective studiesCirculation2000102101082108510973834
- KamstrupPRTybjaerg-HansenANordestgaardBGLipoprotein(a) and risk of myocardial infarction–genetic epidemiologic evidence of causalityScand J Clin Lab Invest2011712879321231777
- NordestgaardBGChapmanMJRayKLipoprotein(a) as a cardiovascular risk factor: current statusEur Heart J201031232844285320965889
- SchreinerPJMorrisettJDSharrettARLipoprotein[a] as a risk factor for preclinical atherosclerosisArterioscler Thromb19931368268338499402
- ElshazlyMBMartinSSBlahaMJNon-high-density lipoprotein cholesterol, guideline targets, and population percentiles for secondary prevention in 1.3 million adults: the VLDL-2 study (very large database of lipids)J Am Coll Cardiol201362211960196523973689
- FryarCDChenTCLiXPrevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999–2010NCHS Data Brief201210318
- TothPPPotterDMingEEPrevalence of lipid abnormalities in the United States: the national health and nutrition examination survey 2003–2006J Clin Lipidol20126432533022836069
- Abul-HusnNSManickamKJonesLKGenetic identification of familial hypercholesterolemia within a single U.S. health care systemScience20163546319aaf7000-1aaf7000-728008010
- ReinerZManagement of patients with familial hypercholesterolaemiaNat Rev Cardiol2015121056557526076948
- BennMWattsGFTybjaerg-HansenANordestgaardBGMutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the copenhagen general population study estimated a prevalence of 1 in 217Eur Heart J201637171384139426908947
- WangJDronJSBanMRPolygenic versus monogenic causes of hypercholesterolemia ascertained clinicallyArterioscler Thromb Vasc Biol201636122439244527765764
- KuklinaEVCarrollMDShawKMHirschRTrends in high LDL cholesterol, cholesterol-lowering medication use, and dietary saturated-fat intake: United States, 1976–2010NCHS Data Brief201311718
- KnickelbineTLuiMGarberichRMiedemaMDStraussCVan-WormerJJFamilial hypercholesterolemia in a large ambulatory population: statin use, optimal treatment, and identification for advanced medical therapiesJ Clin Lipidol20161051182118727678435
- HsiaSHDesnoyersMLLeeMLDifferences in cholesterol management among states in relation to health insurance and race/ethnicity across the United StatesJ Clin Lipidol20137667568224314367
- MannDReynoldsKSmithDMuntnerPTrends in statin use and low-density lipoprotein cholesterol levels among US adults: impact of the 2001 national cholesterol education program guidelinesAnn Pharmacother20084291208121518648016
- WatersDDBrotonsCChiangCWLipid treatment assessment project 2: a multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goalsCirculation20091201283419546386
- ZimmermanMPHow do PCSK9 inhibitors stack up to statins for low-density lipoprotein cholesterol control?Am Health Drug Benefits20158843644226702335
- GlueckCJBudhaniSBMasineniSSVitamin D deficiency, myositis-myalgia, and reversible statin intoleranceCurr Med Res Opin20112791683169021728907
- KhayznikovMHemachrandraKPanditRKumarAWangPGlueckCJStatin intolerance because of myalgia, myositis, myopathy, or myonecrosis can in most cases be safely resolved by vitamin D supplementationN Am J Med Sci201573869325838999
- SteinEARaalFJLipid-lowering drug therapy for CVD prevention: looking into the futureCurr Cardiol Rep2015171110426385394
- ZhangXLZhuQQZhuLSafety and efficacy of anti-PCSK9 antibodies: a meta-analysis of 25 randomized, controlled trialsBMC Med20151312326099511
- HeidenreichPATrogdonJGKhavjouOAForecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart AssociationCirculation2011123893394421262990
- MilaniRVLavieCJImpact of worksite wellness intervention on cardiac risk factors and one-year health care costsAm J Cardiol2009104101389139219892055
- ArenaRGuazziMBriggsPDPromoting health and wellness in the workplace: a unique opportunity to establish primary and extended secondary cardiovascular risk reduction programsMayo Clin Proc201388660561723726400
- GroverSAHoVLavoieFCoupalLZowallHPiloteLThe importance of indirect costs in primary cardiovascular disease prevention: can we save lives and money with statins?Arch Intern Med2003163333333912578514