Abstract
Objective
To determine the prevalence of single and mixed dyslipidemias among patients treated with statins in clinical practice in France.
Methods
This is a prospective, observational, cross-sectional, pharmacoepidemiologic study with a total of 2544 consecutive patients treated with a statin for at least 6 months.
Main outcome measures
Prevalence of isolated and mixed dyslipidemias of low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and triglycerides among all patients and among patients at high cardiovascular risk; clinical variables associated with attainment of lipid targets/normal levels in French national guidelines.
Results
At least one dyslipidemia was present in 50.8% of all patients and in 71.1% of high-risk patients. Dyslipidemias of LDL-C, HDL-C, and triglycerides were present in 27.7%, 12.4%, and 28.7% of all patients, respectively, and in 51.0%, 18.2%, and 32.5% of high-risk patients, respectively. Among all subjects with any dyslipidemia, 30.9% had mixed dyslipidemias and 69.4% had low HDL-C and/or elevated triglycerides, while 30.6% had isolated elevated LDL-C; corresponding values for high-risk patients were 36.8%, 58.9%, and 41.1%. Age, gender, body mass index and Framingham Risk Score >20% were the factors significantly associated with attainment of normal levels for ≥2 lipid levels.
Conclusions
At least one dyslipidemia persisted in half of all patients and two-thirds of high cardiovascular risk patients treated with a statin. Dyslipidemias of HDL-C and/or triglycerides were as prevalent as elevated LDL-C among high cardiovascular risk patients.
Introduction
Elevated low-density lipoprotein cholesterol (LDL-C) is the primary treatment target for patients at risk of coronary heart disease (CHD).Citation1,Citation2 Hence, European guidelines for reducing cardiovascular risk focus on lowering serum levels of LDL-C (and total cholesterol [TC]).Citation2,Citation3 However, low serum levels of high-density lipoprotein cholesterol (HDL-C) and elevated levels of triglycerides also increase the risk of CHD,Citation4–Citation9 even in patients treated with statins and with low LDL-C levels.Citation9 Serum levels of HDL-C and triglycerides tend to be inversely correlated, likely reflecting their respective participation in lipid transport and reverse cholesterol transport.Citation10 The inverse relationship holds in the effects of lipid-modifying drugs – niacin,Citation11 fibrates,Citation11 statins,Citation12,Citation13 and cholesteryl ester transfer protein (CETP) inhibitors,Citation14 all concomitantly increase HDL-C and decrease triglyceride levels – and in the effects of certain genetic mutations.Citation15–Citation21 This suggests that the separate dyslipidemias of low HDL-C and elevated triglycerides may be viewed in combination.
Previous studies of dyslipidemia in primary care in France have either focused on LDL-C and/or TCCitation22–Citation24 or have reported values for individual lipids (TC and triglycerides;Citation25 LDL-C, HDL-C, and triglyceridesCitation26) according to NCEP ATP III guidelines.Citation25,Citation26 Studies of mixed dyslipidemias in European countries have applied NCEP ATP III guidelinesCitation27 or modified JES III guidelines.Citation28 Studies set in primary care in France have reported rates of mixed dyslipidemias of LDL-C, HDL-C, and triglycerides according to European JES III guidelines, published in 2003.Citation29,Citation30 Bruckert et al reported rates of mixed dyslipidemias of HDL-C and triglycerides in 11 European countries, including France, according to JES III and NECEP ATP III guidelines.Citation31
In France the Agence Française de Securite Sanitaire des Produits de Sante (AFSSAPS) has developed national guidelines for the management of dyslipidemia that differ in important ways from the European guideline.Citation32 In particular, the thresholds for LDL-C for patients not categorized as high risk differ in the AFSSAPS and JES IV guidelines, and in AFSSAPS the threshold for HDL-C is the same for men and women (). Currently, the AFSSAPS are the most commonly used and recommended guidelines for patients treated with lipid-modifying therapy in France. Accordingly, prior studies assessing achievement of target LDL-C levels among statin-treated patients in France have applied the AFSSAPS definition.Citation23,Citation33,Citation34 The objective of this paper is to further evaluate single and mixed dyslipidemias among patients treated with statins in clinical practice in France, applying the AFSSAPS guidelines.
Table 1 Comparison of French (AFSSAPS) and European guidelines lipid thresholds for dyslipidemia
Methods
Study design and data source
This was a prospective, observational, cross-sectional, pharmacoepidemiologic study of patients receiving lipid-modifying therapies that included a statin. The data source was the 2006 BKL-Thales database.Citation22,Citation33–Citation38 Physicians in the Thales panel compose a nationally representative sample, based on criteria of age, gender, and area of practice. They maintain their patients’ medical and prescription records using proprietary computer software and transmit coded extracts into the Thales database. To collect additional data for this study, a supplementary questionnaire was added to the physicians’ software program. No intervention was made to affect the physicians’ prescribing behavior and the identities of neither the physicians nor patients were recorded in the data set analyzed.
Study sample
The source population consisted of consecutive patients who agreed to participate in the supplementary survey during a routine visit to a general practitioner belonging to the Thales network. Physicians recruited dyslipidemic patients who had been treated with a statin for at least 6 months and who had a complete lipid profile (LDL-C, HDL-C, and triglycerides) within the past 6 months. Patients were excluded from the study if their statin treatment had been modified (indicated by a change in International Nonproprietary Name [INN] or daily dosage) in the 3 months prior to the lipid panel or if they declined to participate.
The 2006 Thales database contains records of the lipid-modifying drug treatment of approximately 150,000 patients by 1200 physicians. The sample size necessary to show that 30% of patients had not attained their LDL-C target with an alpha of 0.05, a delta of 1.6%, and a power of 95% was calculated to be 3151. The target sample size was thus 3000.
Data collection
Seven hundred general practitioners were randomly selected from the Thales panel and sent letters inviting them to participate in the study. Three successive reminder letters were sent to physicians who did not respond. Patient data were collected prospectively via the computer network over a 6-month period from December 2007 to May 2008. Data were collected from existing medical records in the Thales database and via the computerized supplementary questionnaire. Data collected from existing records included the date of consultation, patient age, gender, diagnoses of hypertension and diabetes (treated or not), diagnosis of dyslipidemia, and prescription of a lipid-modifying agent. Data collected from the supplementary questionnaire included the patient’s weight, height, blood pressure, family history of early onset cardiovascular event, and smoking status (current or regular smoker, or stopped within past 3 months). Certain conditions were identified from a combination of the Thales data set and the supplementary questionnaire: proven coronary heart disease (CHD), proven cardiovascular disease (CVD), renal impairment, proteinuria, and microalbuminuria.
Definitions
Permanent hypertension was defined in the Thales data set as 140/90 mmHg (130/90 mmHg if diabetes present), measured as the mean of the last three values recorded. Proven CHD was defined in the Thales data set as a combination of a diagnosis of angina and three prescriptions per year of a nitrate derivative, beta-blocker, calcium channel inhibitor, or amiodarone. High cardiovascular risk was defined by a diagnosis of cardiovascular disease, a diagnosis of high-risk type 2 diabetes, and/or a 10-year CHD risk >20% computed with the Framingham equation.Citation39 High-risk diabetes was defined as diabetes mellitus with concomitant renal disease and/or at least two of the following cardiovascular risk factors: age, family history of coronary disease, HDL-C <40 mg/dL, and microalbuminuria (>30 mg/24 hours). Cardiovascular risk factors were as defined by the AFSSAPS 2005 French national guideline ().Citation32 Obesity was defined as body mass index (BMI) ≥ 30 kg/m2 and abdominal obesity as a waist measurement >88 cm in women and >102 cm in men. Thresholds for dyslipidemia were as defined in the AFSSPAS guideline ().Citation32
Data analysis
A descriptive analysis of patient characteristics and the prevalence of individual dyslipidemias (of LDL-C, HDL-C, or triglycerides) was carried out. Seven categories of mutually exclusive dyslipidemias were defined:Citation29 isolated elevated LDL-C, isolated low HDL-C, isolated elevated triglycerides, elevated LDL-C and low HDL-C, elevated LDL-C and elevated triglycerides, low HDL-C and elevated triglycerides, and all three lipid abnormalities. Combinations of two or more dyslipidemias were called ‘mixed’. The proportions of all combinations of normal and abnormal lipid values were determined for the total study population and for high-risk patients. The distribution of dyslipidemias among subjects with dyslipidemia was also reported. Clinical factors associated with attainment of AFSSAPS lipid threshold levels were assessed in multivariate regression models. The likelihood of attaining target/normal levels for individual lipid parameters, ie, LDL-C, HDL-C, and triglycerides was computed, adjusting for age (per 1 year increase), gender, BMI category, smoking status, hypertension, diabetes, history of cardiovascular disease, Framingham score risk >20%, and year of index prescription (2008 versus 2007). The same covariates were adjusted for in an analysis of attainment of two or more lipid target/normal levels (among LDL-C, HDL-C, and triglycerides) versus attainment of LDL-C only. Analyses were performed using SAS software (v 9; SAS Institute, Cary, NC).
Results
Study population
Patient characteristics
Of 2707 patients treated with a statin, 2544 met the study inclusion–exclusion criteria (). Of these, 1201(47.2%) were at high risk of cardiovascular events. The mean patient age was 65.8 years, 59.1% were men, and 71.7% had hypertension (). A history of cardiovascular disease was recorded for 31.8% of patients and 3.3% had a Framingham risk score >20%.
Figure 1 Sample selection.
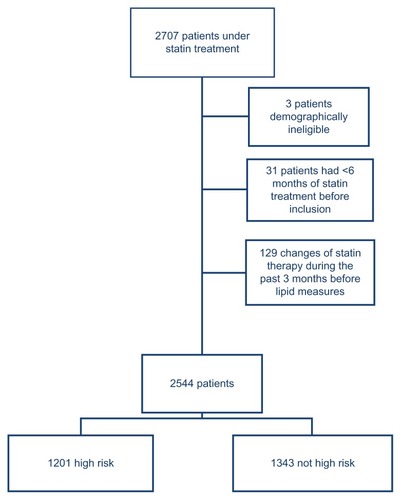
Table 2 Patient characteristics
Lipid-modifying drug therapies
Statin monotherapies were taken by 92.7% of the total patient sample (not tabulated). Statins were taken in combination with cholesterol absorption inhibitors by 4.8% and with other lipid-modifying therapies by 2.5% of patients. No patient received a statin in combination with a fibrate. Among the high-risk subgroup, 90.4% received statin monotherapies and statins were used in combination with cholesterol absorption inhibitors, omega-3 triglycerides, and other therapies by 7.2%, 2.8%, and 1.8% of patients, respectively.
Prevalence of dyslipidemias
At least one dyslipidemia was present in 50.8% of all subjects. As seen in , the most prevalent dyslipidemias in the entire population were elevated triglycerides (28.7%) and elevated LDL-C (27.7%), while 12.4% had low HDL-C. Among all subjects with any dyslipidemia, 30.9% had mixed dyslipidemias (). Low HDL-C and/or elevated triglycerides occurred in 69.4% of patients with any dyslipidemia, compared to 30.6% for isolated elevated LDL-C ().
Figure 2 Prevalence of dyslipidemias in all patients.*
Abbreviations: HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; TG, triglycerides.
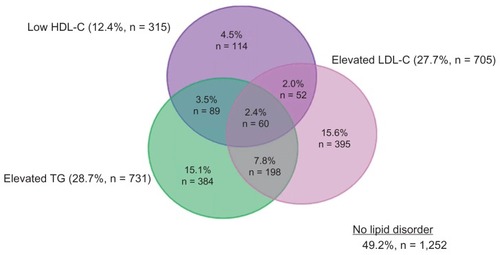
Table 3 Prevalence of dyslipidemias among all subjects and high-risk subjects with at least one dyslipidemia
At least one dyslipidemia was present in 71.1% of high-risk subjects. Elevated LDL-C was the most prevalent dyslipidemia (51.0%), while dyslipidemias of elevated triglycerides and low HDL-C occurred in 32.5% and 18.2%, respectively, of high-risk patients (). Among those at high risk with any dyslipidemia, 36.8% had mixed dyslipidemias (). Low HDL-C and/or elevated triglycerides occurred in 58.9% of high-risk patients with any dyslipidemias, compared to 41.1% for isolated elevated LDL-C ().
Figure 3 Prevalence of dyslipidemias in high-risk patients.*
Abbreviations: HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; TG, triglycerides.
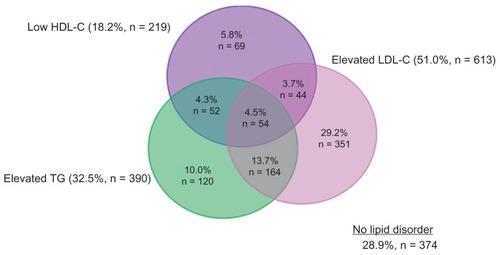
All three dyslipidemias occurred in 4.6% of all patients and 6.3% of high-risk patients with any dyslipidemia ().
Variables associated with lipid goal attainment
A Framingham risk score >20% was the factor most strongly associated with attainment of lipid goal/normal level, with odds ratio (OR) values of 0.011, 0.210, and 0.564 for LDL-C, HDL-C, and triglycerides, respectively (P < 0.01 for all effects; ). A history of CVD/CHD was also associated with attainment of goals/normal level for all lipid parameters except triglycerides, for which the effect did not reach statistical significance.
Table 4 Clinical factors associated with attainment of targets/normal levels for individual lipids and two or more lipids among the total population
Several variables were significantly associated with normal level attainment for HDL-C and/or triglycerides but not LDL-C goal, or vice versa. Older age was associated with greater odds of attaining normal level for HDL-C and triglycerides but not the LDL-C goal. Similarly, a diagnosis of diabetes and BMI categories of 25–30 kg/m2 and >30 kg/m2 were associated with reduced odds of attaining normal levels for HDL-C and triglycerides but not the LDL-C goal. Conversely, being a current smoker reduced the odds of LDL-C goal attainment but not attainment of normal levels for HDL-C or triglycerides. Male gender increased the odds of attaining the LDL-C target but decreased the odds of attaining the normal level for HDL-C.
The odds of attaining goal/normal level for ≥2 lipid parameters followed the pattern for HDL-C and triglycerides for age, BMI categories, smoking status, Framingham risk score, and history of cardiovascular disease. Year of index statin prescription had no statistically significant association with any lipid goal attainment.
Comment
The proportion of patients meeting AFSSAPS criteria for high cardiovascular risk in this study (47.2%) was similar to the 51.2% in a previous study of mixed dyslipidemias in patients treated with lipid-modifying drugs in French general practice.Citation29 The present study differs, however, in methodology and results for dyslipidemias. The previous study applied lipid thresholds defined in JES III rather than in the AFSSAPS guideline.Citation29 The principal difference between the two guidelines is that AFSSAPS has less stringent targets for LDL-C for patients not at high risk (). In addition, patients in the earlier study were selected for being prescribed either a statin or fibrate, so that 67.1% used statin monotherapy and 31.8% used fibrate monotherapy. In the current study 92.7% of patients received statin monotherapy and none received fibrates. Possibly for these reasons, the proportions of patients with elevated LDL-C differed in the two studies: 73.2% in the previous study and 27.7% in the present study. The proportions of patients with low HDL-C and elevated triglycerides were similar in the two studies but the relative contributions differed. Dyslipidemias of HDL-C and/or triglycerides were present in 46.3% of patients with any dyslipidemia in the previous study versus 69.4% in the present study. Results for the high-risk group in the current study more closely resembled those in the previous study, possibly because the lipid thresholds for high-risk patients are nearly identical in the AFSSAPS and JES guidelines. Isolated LDL-C occurred in 41.1% of high-risk patients with any dyslipidemia in the current study versus 53.7% in the previous study. Corresponding values for dyslipidemias of HDL-C and/or triglycerides are 58.9% and 46.3%, respectively.
Results show that prevalence rates of dyslipidemia in France, as observed in this study, are lower than those seen throughout Europe and Canada. Compared to results seen in the Dyslipidemia International Study (DYSIS) (an epidemiologic multi-center, cross-sectional study of lipid profiles of 22,063 statin-treated outpatients in 11 European countries and Canada), French patients have a lower prevalence of low HDL-C (12.4% vs 26.3%), elevated LDL-C (27.7% vs 48.2%), and elevated triglycerides (28.7% vs 38.2%).Citation41
Factors associated with lipid goal attainment have been reported in several cross-sectional studies of patients treated with lipid-modifying drugs in France.Citation23,Citation26,Citation29 Dallongeville et al reported that increased waist circumference was associated with a reduced likelihood of achieving the triglyceride normal level of 150 mg/dLCitation26 – equivalent to the relationship between BMI and attainment of a normal triglyceride level observed in the present study. In the study reported by Ferrieres et al, variables associated with a reduced likelihood of achieving the 2005 AFSSAPS target for LDL-C – smoking status, diabetes, hypertension, CHD, and increased risk of CVD – matched those in the present study (with the exception of diabetes).Citation23 Applying JES III criteria, Van Ganse et al reported that each additional cardiovascular risk factor increased the occurrence of dyslipidemias of HDL-C and/or triglycerides (with normal LDL-C), the joint dyslipidemia of LDL-C and triglycerides (with normal HDL-C), and all three dyslipidemias.Citation29 These results correspond to the finding in the current study that a Framingham risk score >20% was associated with a reduced likelihood of attaining targets/normal levels for ≥2 lipids.
Except for Framingham risk score and history of CVD/CHD, cardiovascular risk factors tended to be significantly associated either with attainment of normal levels for HDL-C and/or triglycerides but not LDL-C goal, or vice versa. This may be related to the fact that statins, which primarily affect LDL-C, were the only lipid-modifying drug used by 92.7% of patients, or it may be a reflection of the structure of the AFSSAPS guideline, in which risk factors escalate the target for LDL-C but not the normal levels for other lipids. Current smoking and hypertension are risk factors that trigger a more stringent LDL-C target in the AFSSAPS guideline, and this may explain their association with a reduced likelihood of attaining the LDL-C goal. However, other risk factors – diabetes and age – were not significantly associated with LDL-C goal attainment. A relationship between male gender and a higher rate of LDL-C goal attainment has been reported previously.Citation40–Citation42 The explanation for this is unclear, although it is possible that men either receive more aggressive treatmentCitation40 or are more adherent to statin regimens than are women.43,44 Not surprisingly, the pattern of risk factors associated with goal/normal level attainment for mixed dyslipidemias (interpreted as ≥2 lipids versus LDL-C alone) tended to follow the pattern for HDL-C and triglycerides – specifically for age, BMI categories, smoking status, Framingham risk score, and history of cardiovascular disease. Unfortunately, the electronic database did not include reliable information on dietary behaviors and exercise, which can also impact goal/normal lipid level attainment. Additional studies are needed to assess the differential impact of these factors, controlling for the abovementioned characteristics, on the prevalence of dyslipidemias despite lipid-modifying treatment.
Conclusion
By applying French national guidelines, we observed at least one dyslipidemia to be present among more than half (50.8%) of these primary care patients treated with statins. About one-third (30.9%) of patients with any dyslipidemia had mixed dyslipidemias, with low HDL-C and/or elevated triglycerides occurring in more than two-thirds (69.4%) of patients with any dyslipidemia, compared to 30.6% for isolated elevated LDL-C.
According to most guidelines, elevated LDL-C is one of, if not the primary, treatment target for reducing cardiovascular risk.Citation1–Citation3 The persistence of elevated LDL-C, even among patients already on lipid-modifying therapy, and particularly among patients at high cardiovascular risk, suggests that current statin treatment (with which >90% of patients in this sample were treated) is not adequate. In light of evidence showing that low HDL-C and elevated TGs are also associated with increased risk of CHD,Citation4–Citation9 along with our observations of the prevalence of mixed dyslipidemias both before and after lipid modifying therapies, suggests that patients may benefit from the addition of therapies targeting HDL-C and/or triglycerides.
Acknowledgment
Medical writing assistance was provided by Julia Vishnevetsky in collaboration with SCRIBCO.
Disclosure
Funding for this study was provided by Merck and Co, Inc.
References
- GrundySMCleemanJIMerzCNImplications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelinesCirculation2004110222723915249516
- GrahamIAtarDBorch-JohnsenKEuropean guidelines on cardiovascular disease prevention in clinical practice: executive summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by representatives of nine societies and by invited experts)Eur Heart J200728192375241417726041
- De BackerGAmbrosioniEBorch-JohnsenKEuropean guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical PracticeEur Heart J200324171601161012964575
- KannelWBHigh-density lipoproteins: epidemiologic profile and risks of coronary artery diseaseAm J Cardiol19835249B12B
- GordonTCastelliWPHjortlandMCKannelWBDawberTRHigh density lipoprotein as a protective factor against coronary heart disease. The Framingham StudyAm J Med1977625707714193398
- GoldbourtUMedalieJHHigh density lipoprotein cholesterol and incidence of coronary heart disease – the Israeli Ischemic Heart Disease StudyAm J Epidemiol19791093296308222135
- AssmannGSchulteHRelation of high-density lipoprotein cholesterol and triglycerides to incidence of atherosclerotic coronary artery disease (the PROCAM experience). Prospective Cardiovascular Munster studyAm J Cardiol19927077337371519522
- SacksFMTonkinAMShepherdJEffect of pravastatin on coronary disease events in subgroups defined by coronary risk factors: the Prospective Pravastatin Pooling ProjectCirculation2000102161893190011034935
- BarterPGottoAMLaRosaJCHDL cholesterol, very low levels of LDL cholesterol, and cardiovascular eventsN Engl J Med2007357131301131017898099
- MorrisonAHokansonJEThe independent relationship between triglycerides and coronary heart diseaseVasc Health Risk Manag200951899519436658
- BirjmohunRSHuttenBAKasteleinJJStroesESEfficacy and safety of high-density lipoprotein cholesterol-increasing compounds: a meta-analysis of randomized controlled trialsJ Am Coll Cardiol200545218519715653014
- EdwardsJEMooreRAStatins in hypercholesterolaemia: a dose-specific meta-analysis of lipid changes in randomised, double blind trialsBMC Fam Pract200341814969594
- LawMRWaldNJRudnickaARQuantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysisBMJ20033267404142312829554
- DavidsonMHMcKenneyJMShearCLRevkinJHEfficacy and safety of torcetrapib, a novel cholesteryl ester transfer protein inhibitor, in individuals with below-average high-density lipoprotein cholesterol levelsJ Am Coll Cardiol20064891774178117084249
- OramJFTangier disease and ABCA1Biochim Biophys Acta200015291–332133011111099
- BenlianPEtienneJde GennesJLHomozygous deletion of exon 9 causes lipoprotein lipase deficiency: possible intron-Alu recombinationJ Lipid Res19953623563667751824
- BenlianPDe GennesJLFoubertLZhangHGagneSEHaydenMPremature atherosclerosis in patients with familial chylomicronemia caused by mutations in the lipoprotein lipase geneN Engl J Med1996335128488548778602
- HokansonJEFunctional variants in the lipoprotein lipase gene and risk cardiovascular diseaseCurr Opin Lipidol199910539339910554701
- WittrupHHTybjaerg-HansenANordestgaardBGLipoprotein lipase mutations, plasma lipids and lipoproteins, and risk of ischemic heart disease. A meta-analysisCirculation199999222901290710359734
- ThornJANeedhamEWMattuRKStocksJGaltonDJThe Ser447- Ter mutation of the lipoprotein lipase gene relates to variability of serum lipid and lipoprotein levels in monozygotic twinsJ Lipid Res19983924374419508003
- GagneSELarsonMGPimstoneSNA common truncation variant of lipoprotein lipase (Ser447X) confers protection against coronary heart disease: the Framingham Offspring StudyClin Genet199955645045410450862
- Van GanseESouchetTLaforestLIneffectiveness of lipid-lowering therapy in primary careBr J Clin Pharmacol200559445646315801941
- FerrieresJGousseETFabryCHermansMPAssessment of lipid-lowering treatment in France–the CEPHEUS studyArch Cardiovasc Dis2008101955756319041840
- Van GanseELaforestLAlemaoEDaviesGGutkinSYinDLipid- modifying therapy and attainment of cholesterol goals in Europe: the Return on Expenditure Achieved for Lipid Therapy (REALITY) studyCurr Med Res Opin20052191389139916197657
- DupuyAMCarriereIScaliJLipid levels and cardiovascular risk in elderly women: a general population study of the effects of hormonal treatment and lipid-lowering agentsClimacteric2008111748318202967
- DallongevilleJBringerJBruckertEAbdominal obesity is associated with ineffective control of cardiovascular risk factors in primary care in FranceDiabetes Metab2008346 Pt 160661119019717
- KolovouGDAnagnostopoulouKKDamaskosDSGender differences in the lipid profile of dyslipidemic subjectsEur J Intern Med200920214515119327602
- LozanoJVPallaresVCea-CalvoLSerum lipid profiles and their relationship to cardiovascular disease in the elderly: the PREV-ICTUS studyCurr Med Res Opin200824365967018218194
- Van GanseELaforestLBurkeTPhatakHSouchetTMixed dyslipidemia among patients using lipid-lowering therapy in French general practice: an observational studyClin Ther20072981671168117919548
- De BackerGAmbrosioniEBorch-JohnsenKEuropean guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts)Eur J Cardiovasc Prev Rehabil2003104S11014555889
- BruckertEBaccara-DinetMMcCoyFChapmanJHigh prevalence of low HDL-cholesterol in a pan-European survey of 8545 dyslipidaemic patientsCurr Med Res Opin200521121927193416368042
- Agence Française de Sécurité Sanitaire des Produits de SantéPrise en charge thérapeutique du patient dyslipidémiqueSaint-Denis Cedex, FranceAFSSPS2005 French
- LaforestLMoulinPSouchetTCorrelates of LDL-cholesterol goal attainment in patients under lipid lowering therapyAtherosclerosis2008199236837718191135
- Van GanseESouchetTLaforestLLong-term achievement of the therapeutic objectives of lipid-lowering agents in primary prevention patients and cardiovascular outcomes: an observational studyAtherosclerosis20061851586416038912
- ChassanyOLe-JeunnePDuracinskyMSchwalmMSMathieuMDiscrepancies between patient-reported outcomes and clinician-reported outcomes in chronic venous disease, irritable bowel syndrome, and peripheral arterial occlusive diseaseValue Health200691394616441523
- AmouyelPLamarqueHGayetJLTreatment with statins in general medicine: dosage and effectiveness. Results of the observational study STATIMEDArch Mal Coeur Vaiss2005981212061211 French16435599
- GraesslinOHoffetMBarjotPPreliminary results from the OPNI observatory: long-term follow-up of a cohort of women using the progestagen contraceptive implant ImplanonGynecol Obstet Fertil2005335315321 French15878686
- BoueeSCharlemagneAFagnaniFChanges in osteoarthritis management by general practitioners in the COX2-inhibitor era-concomitant gastroprotective therapyJoint Bone Spine200471321422015182793
- WilsonPWD’AgostinoRBLevyDBelangerAMSilbershatzHKannelWBPrediction of coronary heart disease using risk factor categoriesCirculation19989718183718479603539
- PutzerGRoetzheimRRamirezAMSneedKBrownleeHJJrCampbellRJCompliance with recommendations for lipid management among patients with type 2 diabetes in an academic family practiceJ Am Board Fam Pract200417210110715082668
- ParrisESLawrenceDBMohnLALongLBAdherence to statin therapy and LDL cholesterol goal attainment by patients with diabetes and dyslipidemiaDiabetes Care200528359559915735194
- SchultzJSO’DonnellJCMcDonoughKLSasaneRMeyerJDeterminants of compliance with statin therapy and low-density lipoprotein cholesterol goal attainment in a managed care populationAm J Manag Care200511530631215898219