Abstract
The present study investigates the effects of low-energy defocused extracorporeal generated shock waves on collagen structure of cellulite afflicted skin. Cellulite measurement using high-resolution ultrasound technology was performed before and after low-energy defocused extracorporeal shock wave therapy (ESWT) in 21 female subjects. ESWT was applied onto the skin at the lateral thigh twice a week for a period of six weeks. Results provide evidence that low-energy defocused ESWT caused remodeling of the collagen within the dermis of the tested region. Improving device-parameters and therapy regimes will be essential for future development of a scientific based approach to cellulite treatment.
Introduction
Extracorporeal shock wave therapy (ESWT)
Shock waves appear in the atmosphere when explosive events such as lightning strikes occur. These are audibly perceived as loud “bangs”. They transmit energy from the place of generation to distant areas which may cause window panes to shatter. Shock waves are presented by a single, mainly positive pressure pulse of large amplitude that is followed by comparatively small tensile wave components (CitationWess 2006). When using shock waves for therapy, effects that make the pressure pulse even steeper due to nonlinearities in the propagation medium as well as phenomena such as refraction and diffraction at acoustic interfaces have to be taken into consideration. Besides mechanical effects such as fragmentation of brittle material on acoustic interfaces (ie, glass/air or kidney stone/surrounding tissue), cavitation bubbles (CitationWolfrum et al 2003) are generated in the propagation medium (ie, water or elastic body tissue), which in turn causes needle-like punctures (ie, leading to stimulating effects such as the generation of action potentials of nerve cells).
High-energy extracorporeal generated shock waves in which mechanical energy is transformed from electrical energy by the piezo-effect were first used therapeutically for kidney stone fragmentation (CitationHaeussler and Kiefer 1971; CitationHoff and Behrend 1973). Extracorporeal shock wave therapy (ESWT) is now well established and is used more than 90% world wide, as the principal method for treating kidney and urethral stones. Extracorporeal generated shock waves are a means of bringing therapeutically effective energies to locally limited places in the body in a non-invasive way. The fact that shock waves selectively effect acoustical interfaces (connecting two media, each with a different density, eg, oil/water or stone/tissue) and pass through homogenous elastic tissue without damage to the most part is medically important. The damage outside of the treatment zone is almost completely avoided due to the possibility of concentrating energy through focusing.
The stimulating effect of low-energy defocused extracorporeal generated shock waves on biological processes within the tissues reached has increasingly become the centre of interest in the last few years. The biological mechanism of action after a shock-wave (ie, after the ultra-short physical stress and strain) is still unknown to large extent. It appears that the principle of action is so universal that a multitude of very different indications like musculoskeletal diseases (calcaneal spur, tennis-elbow, golf-arm, lime-shoulder) (CitationWang et al 2006), orthopedics (pseudarthrosis) (CitationSiebert and Buch 1997), chronic skin lesions (ulcus cruris) and burnings (CitationSparsa et al 2005; CitationSchaden et al 2006) respond positively to shock wave therapy. Biological reactions of liberation of different agents (measured by immunohistochemistry) such as VEGF (vascular endothelial growth factor), eNOS (endothelial nitric oxide synthase) and PCNA (proliferating cell nuclear antigen) are reported (CitationWang et al 2006). Shock waves are also effective as a means to increase local blood circulation and metabolism. These effects are considered responsible for final healing. Additionally ESWT seems to have a high anti-bacterial effect. Because of these diverse effects we tested low-energy defocused ESWT for treatment of cellulite.
Cellulite: the patho-physiology, evaluation and treating-attempts
Cellulite (gynoid lipodystrophy) (CitationRossi and Vergnanini 2000; CitationAvram 2006; CitationPavicic et al 2006), the aesthetically disturbing (according to modern taste) dimpling of the skin commonly occurs on the thighs and buttocks affecting most post-adolescent woman of all races. Incipient cellulite is recognized by an “orange peel” aspect while full blown cellulite is characterized by a dimpled skin surface. Cellulite is uncommon in men, the majority of those affected also suffer androgen-deficiency disorders such as Klinefelter-syndrome, hypo-gonadism or cirrhosis (alcoholic liver disease, see ie, Drunken Bacchus by Rubens (1577–1640)). While not potentially hazardous to health (CitationSmith 2002) and even considered normal based upon its frequency of occurrence, cellulite remains nonetheless, an issue of cosmetic concern and may induce negative psycho-social side-effects in those suffering its consequences on their appearance.
The patho-physiology of cellulite is understood today as being gender-specific to female skin (CitationMüller and Nürnberger 1972; CitationNürnberger and Müller 1978; CitationScherwitz and Braun-Falco 1978; CitationQuatresooz et al 2006). Based upon anatomy and histology of skin Nürnberger and Müller formulated a scheme for development of cellulite (see ). In skin of men the septa of subcutaneous connective tissue are thick, parallel to the surface and criss-crossing, causing the polygonal fat-cell chambers to be small. In contrast, in skin of women the septa of the subcutaneous connective tissue are thin, perpendicular to the surface resulting in formation of large standing fat-cell chambers. In subjects with high BMIs, the fat-cell chambers herniate into the corium forming papillae adiposae, which aggravate the dimpling appearance of cellulite, causing protrusions and pits (CitationPierard et al 2000).
Figure 1 Schema representing the gender difference of the inner structure of skin and subcutaneous tissue. Modified from CitationMüller and Nürnberger (1972).
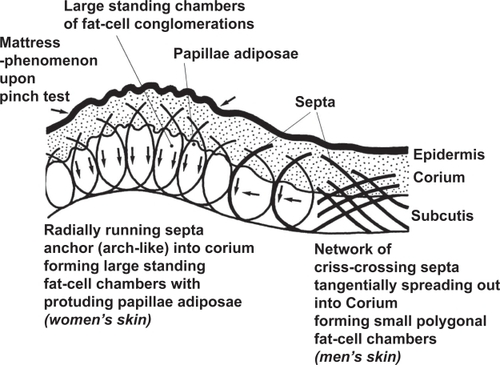
Incipient cellulite recognized by an “orange peel” appearance represents focally enlarged fibro-sclerotic strands partitioning the hypodermis and limiting the out pouching of fat lobules. In contrast, full blown cellulite recognized by a dimpled skin surface represents subjugation of the hyper-trophic response of the hypodermal connective tissue strands when the resistance is overcome by progressive fat accumulation that protrudes into the lower reticular dermis. A simple grading-score of cellulite by inspection () was given by CitationNürnberger and Müller (1978).
Table 1 Grading of cellulite
Other attempts to describe the etiology of cellulite include:
The deterioration of dermal vasculature (alteration of the pre-capillary arteriolar sphincter) causing edema and tissue hypoxia with thickening and sclerosis of the fibrous septa (CitationLotti et al 1990; CitationCurri 1993) and
The chronic inflammatory processes with diffuse infiltration of macrophages and lymphocytes into the fibrous septa (CitationDraelos and Marenus 1997; CitationKligman 1997).
Three dimensional skin surface topography (3-D-SST) by Laser (CitationSmalls et al 2005),
Collagenometry with HF-ultrasound at skin (CitationTikjob et al 1984; CitationRosenbaum et al 1998; CitationMole et al 2004),
MRI imaging of the subcutaneous adipose tissue (CitationQuerleux et al 2002; CitationMirrashed et al 2004) and
Histology.
Low-energy defocused ESWT is a new approach for cellulite treatment. It represents an easy to handle, non-invasive, side effect free, local therapy type with short application periods. CitationSiems et al (2005) found increased concentrations of serum malondialdehyde (MDA) and plasma protein carbonyls in cellulite patients with edematous and lipid enriched dermis resulting from oxidative stress. Concentrations of both these substances decreased after application of ESWT with or without complex physical decongestive therapy (CPDT). Also lipid peroxidation products were released demonstrating the sclerosis-preventing effect of ESWT and/or CPDT (smoothening of dermis and hypodermis). Expression of factors stimulating angiogenesis and lymphangiogenesis was not induced by ESWT and/or CPDT (CitationSiems et al 2005).
Methods and human resources
Criteria for inclusion and exclusion of subjects
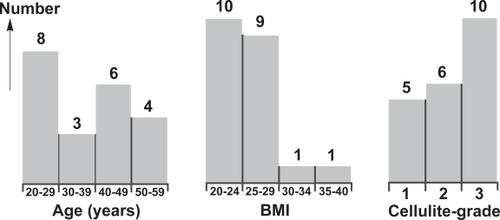
21 female, non-pregnant, healthy test persons of age between 20 and 60 years with cellulite parameters were selected to participate in the study (). Exclusion criteria related to health status were:
Disease of the skin,
Thrombosis or post-thrombosis syndrome,
Known malignoma or chemotherapy,
Anti-coagulation therapy,
Cortisone-therapy,
Known metabolic disorder (ie, diabetes-mellitus, hypercholesterinemia etc.),
Inflammation within treatment area and
Other simultaneous treatment of cellulite.
Figure 2 Human resources: distributions of 21 female test persons. Left: histogram for age, middle: histogram for body mass index (BMI), right: histogram for grading of cellulite according to .
High-resolution ultrasound of the skin
The high-resolution ultrasound of the skin represents an imaging-producing and non-invasive diagnostic tool, which is able to give an exact representation of the skin and its adnexa. The ultrasound system (Collagenoson®) used in this study included a probe of 22 MHz (yielding a high-resolution axial of 50 μm, lateral of 200 μm and a depth of 6 mm) that was placed upon wet skin. It measured the micro-structure of the mesenchymal connective tissue and the collagen structures within the extra-cellular matrix of the dermis (collagenometry), showing both the epidermis and the boundary between dermis and sub-cutis. With this device the structure and the quality of the collagen and thus the result of therapy could be exactly evaluated.
Application of ESWT and device-parameters
The low-energy defocused ESWT was applied according to the following parameters:
ActiVitor-Derma® (shock waves are produced by electrohydraulic means) with ActiVitor Probe D0 corresponding to a depth of entrance of 5 mm and surface focus of 25 mm times 25 mm,
Energy flow density per shot set at 0.018 mJ/mm2,
Skin of lateral left and right thigh treated with 40000 shots onto surface of 160 cm2 per side (shots homogenously distributed by partitioning 160 cm2 into 8 times 5 squares of 4 cm2 with 100 shots per square).
Course of study
Collagenometry was carried out before and after low energy defocused ESWT to selected areas of the skin of the thighs (lateroposterio) twice a week during a treatment period of 6 weeks. At the end of the treatment period (equivalent to 96000 shots per person) a questionnaire was filled out concerning the tolerance (pain and side effects) and the subjective outcome of cellulite.
Analysis of the image from high-resolution ultrasound
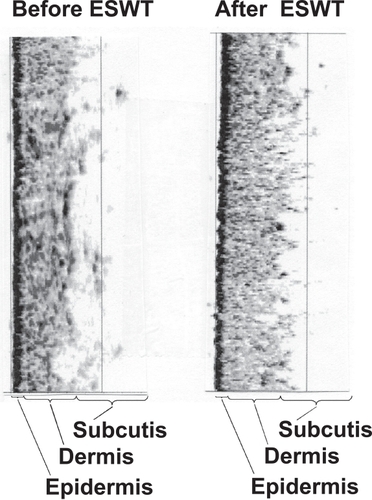
A remodeling of collagen within the dermis can be imaged by collagenometry (). Dividing the dermis into the side to the epidermis and into the side to the sub-cutis and analyzing the change in the distributions of each side the following rating scale was used:
−1: a change to more irregular,
0: no change,
1: a change to more regular
Figure 3 Collagenometry (Collagenoson®) taking high-frequency high-resolution ultrasound measurements of the extra-cellular matrix of the skin before and after treatment with low energy defocused extracorporeal shock wave therapy (ESWT). Case of improvement-score of +2 (clear improvement). Both ultrasound samples taken from the treated area. Determination of improvement-score: dividing the dermis into the side to the epidermis and into the side to the sub-cutis and analyzing the change in the distributions of each side (−1: change to more irregular, 0: no change, 1: change to more regular).
Results
The above improvement-scoring procedure analyzing changes in the microstructure of the skin by collagenometry is presented in (upper part). The data indicate that low-energy defocused ESWT may be effective in treating cellulite by remodeling collagen within the skin. From this small sample of test persons we cannot conclude that there are differential effects of treatment based upon age or cellulite stage.
Figure 4 Results: distributions of 21 female test persons. Upper left: histogram for improvement score (see , −2 (![]()
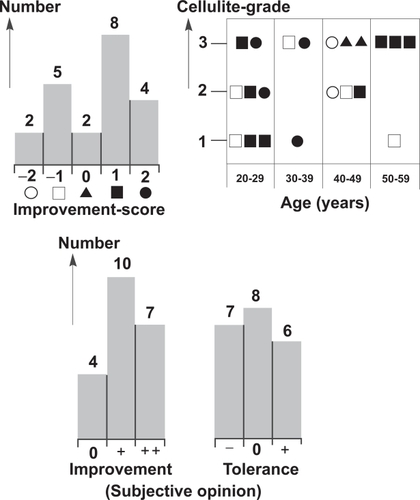
Questionnaire responses are summarized in (lower part). Most subjects reported an improvement of the skin treated. Seven reported a clear improvement (cellulite reduction, skin more tight, finer fabric of skin and underlying tissue). A few subjects reported that treatment was unacceptable because it caused some pain. After two months the subjective evaluation of effects on the locally treated skin was reevaluated. At that time six test persons reported an improvement (cellulite reduction, skin more tight, finer fabric of skin and underlying tissue) after a delay of 2–4 weeks (an effect well known in treatment of calcaneal spurs by ESWT). Ten subjects did not identify any local change since the end of treatment. Five subjects reported a re-occurrence of cellulite. The therapist who applied ESWT complained that the sound associated with treatment was irritating and required ear protection.
Discussion and conclusion
The results of this study suggest that low-energy defocused ESWT is effective in treating cellulite through the remodeling of skin collagen. This effect can be corroborated by measuring the microstructure of the skin using high frequency ultrasound (Collagenoson®) as well as by the subjective comments of the subjects. The data also suggest that improvement from treatment may have a latent period of from 2 to 6 months. It may also be possible that successful cellulite treatment will result from low-energy defocused ESWT using higher energy flow density, ie, more than 0.018 mJ/mm2. Alternative wrapping of the machine to protect patients and therapist from too loud sound exposure is also suggested as well as different techniques for applying the low-energy defocused ESWT to make it more suitable, eg, whole-body skin treatment under water in an ordinary bath tub by low-energy unfocused (plane-wave) ESWT.
Further investigation is needed to determine whether a scientific based therapy concept for cellulite can be developed by optimizing device-parameters such as the applied energy flow density and the shape of focus as well as therapy regimes, age and cellulite grade specific parameters. Depending upon the outcomes of these investigations, low-energy defocused ESWT may become one of the few evidence-based therapies for future clinical management of cellulite.
Acknowledgements
Evelyn Hemmer, Klinik Piano (Measurements and Treatment); Sarah Baccolini, Klinik Piano (Organisation); SwiThech Medical AG, CH-8280 Kreuzlingen, Switzerland (Providing device for low energy defocused ESWT ActiVitor Ortho/Derma).
References
- AlsterTSTanziEL2005Cellulite treatment using a novel combination radiofrequency, infraredlight and mechanical tissue manipulation deviceJ Cosmet Laser Ther781516537213
- AlsterTSTehraniM2006Treatment of cellulite with optical devices: an overview with practical considerationsLasers Surg Med387273016988953
- AvramMM2006Cellulite: a review of its physiology and treatmentJ Cosmet Laser Ther6181516020201
- BertinCZuninoHPittetJC2001A double-blind evaluation of the activity of an anti-cellulite product containing retinol, caffeine and ruscogenine by a combination of several non-invasive methodsJ Cosmet Sci5419921011479653
- CurriSB1993Cellulite and fatty tissue microcirculationCosmet Toilet108518
- DraelosZMarenusKD1997Cellulite etiology and purported treatmentDermatol Surg23117981
- GherardiniGMatarassoASerureAS1997Standardization in photography for body contour surgery and suction-assisted lipectomyPlast Reconstr Surg100227379207680
- HaeusslerEKieferW1971Anregung von Stoßwellen in Flüssigkeiten durch
- Hochgeschwindigkeits-WassertropfenVerhandlungen Dtsch Phys GesellschaftVI6786
- HexselDMMazzucoR2000Subcision: a treatment for celluliteInt J Dermatol395394410940122
- HoffGBehrendA1973Einrichtung zum Zertrümmern von im Körper eines Lebewesens befindlichen KonkrementenDP 2351247235
- KligmanAM1997Cellulite: facts and fictionJ Geriatr Dermatol51369
- Lis-BalchinM1999Parallel placebo-contolled clinical study of a mixture of herbs sold as a remedy for cellulitePhytother Res13627910548762
- LottiTGhersetichIGrapponeC1990Proteoglycans in so-called celluliteInt J Dermatol2927242370117
- MirrashedFSharpJCKrauseV2004Pilot study of dermal and subcutaneous fat structures by MRI in individuals who differ in gender, BMI, and cellulite gradingSkin Research and Technology1016115225265
- MoleBBlanchemaisonPEliaD2004High frequency ultrasonography and celluscore: an improvement in the objective evaluation of cellulite phenomenonAnnales de chirurgie plastique esthétique4938795
- MulhollandRS2004Bipolar radiofrequency, infrared heat and pulsatile suction in the non-surgical treatment of focal lipodystrophy and celluliteAustralian Cosmetic Surgery261013
- MüllerGNürnbergerF1972Anatomical principles of the so-called “cellulite”Arch Dematol Forsch2441712
- NürnbergerFMüllerG1978So-called cellulite: an invented diseaseJ Dermatol Surg Oncol42219632386
- PavicicTBorelliCKortingHC2006Cellulite—the greatest skin problem in healthy people? An approachJDDG108617017010177
- PierardGENizedJLPierard-FranchimontC2000Cellulite: from standing fat herniation to hypodermal stretch marksAm J Dermatopathol2234710698214
- Pierard-FranchimontCPierardGEHenryF2000A randomized, placebo-controlled trial of topical retinol in the treatment of celluliteAm J Clin Dermatol13697411702613
- QuatresoozPXhauflaire-UhodaEPiérard-FranchimontC2006Cellulite histopathology and related mechanobiologyInternational Journal of Cosmetic Science282071018489276
- QuerleuxBCornillonCJolivetO2002Anatomy and physiology of subcutaneous adipose tissue by in vivo magnetic resonance imaging and spectroscopy: relationships with sex and presents of celluliteSkin Research and Technology81182412060477
- RaoJPaaboKEGoldmanMP2004A double-blinded randomized trial testing the tolerability and efficacy of a novel topical agent with and without occlusion for the treatment of cellulite: a study and review of literatureJournal of Drugs in Dermatology34172615303786
- RosenbaumMPrietoVHellmerJ1998An exploratory investigation of the morphology and biochemistry of cellulitePlastic & Reconstructive Surgery101193499623840
- RossiABVergnaniniAL2000Cellulite: a reviewJ Eur Acad Dermatol Venereol142516211204512
- RotundaAMAvramMMAvramAS2005Cellulite: is there a role for injectables?J Cosmet Laser Ther71475416414902
- SadickNSMulhollandRS2004A prospective clinical study to evaluate the efficacy and safety of cellulite treatment using the combination of optical and RF energies for subcutaneous tissue heatingJ Cosmet Laser Ther61879016020202
- SainioELRantanenTKanervaL2000Ingredients and safety of cellulite creamsEur J Dermatol1059660311125320
- SchadenWThieleRKölplC2006Extracorporeal shock wave therapy (ESWT) in skin lesions. 9th International Congress of the International Society for Musculoskeletal Shockwave Therapy (ISMST)News Letter ISMST1
- ScherwitzCBraun-FalcoO1978So-called celluliteJ Dermatol Surg Oncol42304632387
- SiebertWBuchM1997Extracorporeal shockwaves in orthopedicsSpringer
- SiemsWGruneTVossP2005Anti-fibrosclerotic effects of shock wave therapy in lipedema and celluliteBioFactors242758216403988
- SmallsLKLeeCYWhitestoneJ2005Quantitative model of cellulite: three dimensional skin surface topography, biophysical characterization and relationship to human perceptionJ Cosmet Sci561052015868063
- SmallsLKHicksLKPasserettiD2006Effect of weight loss on cellulite: gynoid lypodystrophyPlast Reconstr Surg11851016874227
- SmithR2002In search of “non-disease”BMJ324883511950739
- SparsaALesauxNKesslerE2005Treatmernt of cutaneus calcinosis in CREAST syndrome by extracorporal shock wave lithotripsyJ Am Acad Dermatol532635
- TikjobGKassisVSondergaardJ1984Ultrasonic B-scanning of the human skin. An introduction of a new ultrasonic skin scannerActa Derm Venereol6467706203286
- WangC-JWangF-SYangKD2006Biological Mechanism of musculoskeletal shockwaves. 9th International Congress of the International Society for Musculoskeletal Shockwave Therapy (ISMST)News Letter ISMST1
- WessO2006Physics and technology of shock wave and pressure wave therapy. 9th International Congress of the International Society for Musculoskeletal Shockwave Therapy (ISMST)News Letter ISMST1
- WolfrumBOhlC-DMettinR2003Die Bedeutung von Kavitationsblasen für transiente Membranpermeabilisierung und ZellschädigungFortschritte der Akustik—DAGA 2003Aachen, 8267 M. Vorländer, Deutsche Gesellschaft für Akustik e.V. (DEGA) Oldenburg.