Abstract
Many men with erectile dysfunction (ED) also have associated underlying cardiovascular and metabolic conditions, for which they are likely to be taking medication. Therefore, cardiovascular safety and potential drug interactions are two of the major concerns when using PDE-5 inhibitors in these patients. The PDE-5 inhibitor, vardenafil, is characterized by a rapid onset of action, increased duration of erection, high rates of first-dose success and reliable efficacy that can be maintained with continued use. In both clinical trials and real-life observational studies, vardenafil has demonstrated a favorable efficacy and safety profile in men with ED, including those with associated underlying conditions such as diabetes, hypertension and dyslipidemia. Importantly, the concomitant use of medication for these conditions is not associated with any noteworthy changes in the efficacy and safety of vardenafil. The evidence presented in this review supports the use of vardenafil as a first-line treatment for men with ED, including those with underlying conditions.
Introduction
Erectile dysfunction (ED) is a common condition affecting an estimated 150 million men worldwide.Citation1,Citation2 ED is frequently associated with loss of self esteem and can impact significantly on the quality of life and well being of both members of a couple.Citation3–Citation6 Organic ED and cardiovascular disease share the same risk factors, including diabetes, hypertension, dyslipidemia, obesity and smoking.Citation7,Citation8 These two conditions also share the same pathophysiology, with endothelial dysfunction, inflammatory and endothelial-prothrombotic activation, and oxidative stress being their common denominators.Citation9,Citation10 It is increasingly being recognized by researchers that ED may be considered a predictor for the development of cardiovascular disease.Citation11–Citation13 Biennial screening of a random sample of community-dwelling men (n = 1402) over a 10-year period revealed that the presence of ED was associated with an approximately 80% higher risk of subsequent coronary artery disease (CAD).Citation14 A study conducted in men with type 2 diabetes who had silent CAD (n = 291) found that patients who experienced major adverse cardiac events over a follow-up period of approximately 4 years were significantly more likely to have ED than those who did not (61% vs 36%, respectively; P < 0.001).Citation15 There is evidence that in patients with established CAD, ED symptoms appeared an average of 2 to 5 years earlier than those of CAD itself.Citation16,Citation17 A diagnosis of ED therefore provides a golden opportunity for clinicians to assess men’s cardiovascular health, and intervene at an early stage in the disease pathway.
The introduction in the late 1990s of highly effective oral pharmacotherapies for ED transformed ED management and led to an increase in the number of men seeking treatment.Citation18 Nevertheless, the rate of ED sufferers seeking medical help is still low,Citation19,Citation20 despite the dramatic impact on overall quality of life and the potential as an indicator for cardiovascular prevention. Current guidelines recommend the phosphodiesterase type 5 (PDE-5) inhibitors, vardenafil, sildenafil and tadalafil, as firstline therapy for ED of varying etiologies and severity.Citation21,Citation22 Vardenafil is a selective PDE-5 inhibitor, with a profile characterized by rapid onset of action, increased duration of erection, high rates of first-dose success and reliable efficacy that can be maintained with continued use.Citation23–Citation31
This review examines the epidemiology of ED, in particular, in men with associated underlying conditions, and evaluates the evidence compiled on the clinical efficacy and safety of vardenafil.
Epidemiological evidence demonstrating the association between ED and underlying conditions
Large-scale epidemiological studies have found the prevalence of ED in the general population of men aged 18 to 64 years to be 10% to 16%.Citation20,Citation32 The prevalence and severity of ED increases with age.Citation18,Citation33–Citation35 In the Epidemiologia de la Disfuncion Erectil Masculina (EDEM) study, ED prevalence rates were 3.9% in the 25- to 39-year age group, rising to 32.3% in those men aged 50 to 70 years.Citation34 The Massachusetts Male Aging Study (MMAS) found that between the age of 40 and 70 years, the probability of having complete ED increased 3-fold from 5% to 15%, with a corresponding 2-fold increase from 17% to 34% in the probability of having moderate ED.Citation18
Numerous studies have explored the close association between ED and cardiovascular disease. Evidence shows that cardiovascular risk factors (CRFs) are present in the majority of men with ED, while men with ED are more likely to have CRFs than those with no ED.Citation20,Citation36,Citation37 A high prevalence of ED has been reported in patients with CAD, with rates ranging from 44% to 75%.Citation38,Citation39 In men with diabetes, ED prevalence rates can vary between 35% and 90%.Citation40–Citation42 A prospective cohort study of men over 50 years of age (n = 31,027) found the prevalence of ED in men with diabetes to be almost double that in men without diabetes (46% vs 24%, respectively). ED in men with diabetes is also frequently more severe, compared with the general ED population.Citation43
Research has demonstrated a considerable difference in hypertension prevalence rates between patients with and without ED (41% vs 19%, respectively).Citation37 A correlation has also been observed between increasing hypertension prevalence and increased ED severity.Citation44 Studies have documented the association between ED and serum lipid levels. An analysis of a nationally representative man-aged care claims database in the United States found the prevalence rate of hyperlipidemia to be 42% among men with ED.Citation45 In a study of 215 men with ED and 100 men without ED, the prevalence of hypercholesterolemia (total cholesterol >200 mg/dL or 5.17 mmol/L) was 71% vs 52%, respectively (P = 0.06). Both high-density lipoprotein (HDL) cholesterol and total cholesterol/HDL cholesterol ratios were shown to be significant predictors of ED (P = 0.011 and P < 0.0001, respectively).Citation46
The Massachusetts Male Aging Study, a community-based, random sample of men aged 40 to 70 years, found an inverse correlation between age-adjusted probability of ED and levels of HDL cholesterol.Citation18 In men aged 40 to 55 years, the age-adjusted probability of having moderate ED increased from 7% to 25% with a decrease in HDL cholesterol levels from 90 mg/dL (2.3 mmol/L) to 30 mg/dL (0.9 mmol/L). Similarly, other studies have found correlations between ED and both decreased HDL cholesterol and elevated total cholesterol/HDL cholesterol ratio.Citation47,Citation48
The cluster of cardiovascular and metabolic risk factors that are often described as the “metabolic syndrome” include increased abdominal obesity, elevated triglycerides, reduced HDL cholesterol, hypertension, increased fasting plasma glucose and hyperinsulinemia.Citation49–Citation52 There is a close association between metabolic syndrome, and both ED and hypogonadism.Citation53,Citation54 In a study of 1086 men with ED, the prevalence of metabolic syndrome was 32% using the National Cholesterol Education Program-Third Adult Treatment Panel (NCEP-ATP III) definition, and 45% using the International Diabetes Federation definition.Citation50
Testosterone regulates the formation of cyclic guanosine monophosphate (cGMP), through its effect on nitric oxide synthase expression, and on cGMP catabolism, through its effect on PDE-5 isoenzyme expression. Hypogonadism is believed to play a major role in the pathophysiology of ED, with a minimum threshold testosterone level required for normal erectile function.Citation55 Prevalence rates of hypogonadism in men with ED range from 2% to 35%.Citation56,Citation57 The close association between testosterone deficiency, ED and underlying conditions may contribute to a decline in men’s overall health, if left untreated.Citation52
Efficacy of vardenafil in men with ED
Clinical efficacy
Diabetes
The trend towards the onset of diabetes at a younger age within the general population, combined with a higher prevalence of childhood type 2 diabetes, is expected to lead to an increase in men developing diabetes-related ED.Citation58 Management of ED in patients with diabetes can be challenging, since ED is often more severe and resistant to long-term treatment in this patient group.Citation43,Citation59 Furthermore, worsening glycemic control is associated with greater impairment of erectile function.Citation60
Favorable efficacy of vardenafil in men with diabetes has been demonstrated in a number of clinical trials. A double-blind, placebo-controlled trial in men with type 1 or type 2 diabetes (n = 452) demonstrated significant improvements in the erectile function domain of the International Index of Erectile Function (IIEF-EF) scores and Sexual Encounter Profile question 2 (SEP2: “Were you able to insert your penis into your partner’s vagina?”) and 3 (SEP3: “Did your erection last long enough for you to have successful intercourse?”) success rates following 12 weeks of treatment with 10 mg or 20 mg vardenafil compared with placebo (all P < 0.0001). After 12 weeks, changes from baseline in IIEF-EF scores were 5.9 and 7.8 for 10 mg and 20 mg vardenafil, respectively, compared with 1.4 for placebo (P < 0.0001).Citation61 No relationship between response to vardenafil and level of glycemic control (defined as level of glycosylated hemoglobin [HbA1c]) was observed. For men with ED and good-to-moderate (HbA1c > 6 but < 8%; n = 64) or poor (HbA1c ≥ 8%; n = 71) glycemic control, SEP3 success rates were 50% and 54%, respectively, in those taking 20 mg vardenafil, compared with 20% (n = 56) and 23% (n = 77) for placebo-treated men. SEP3 responses were significantly superior to placebo for both 10 mg and 20 mg vardenafil in all glycemic control subgroups.
Similar findings were reported in a randomized, double-blind, placebo-controlled trial in Japan in men with diabetes (defined as levels of HbA1c > 6.5% or receiving hypoglycemic drug treatment).Citation62 IIEF-EF scores improved significantly from 13.6 and 13.9 at baseline to 21.8 and 22.9 at last observation carried forward (LOCF) in the 10 mg and 20 mg vardenafil groups, respectively, compared with an increase from 13.7 to 16.3 for placebo (P < 0.0001).
Hypertension
The number of patients with hypertension has risen considerably in recent years.Citation63 Accordingly, given the close association between ED and hypertension, the need to determine the efficacy and safety of PDE-5 inhibitors for ED therapy in this patient group has assumed greater importance. A 12-week, multicenter, randomized, double-blind, placebo-controlled trial conducted in Germany investigated the efficacy of flexible-dose vardenafil in men with ED and arterial hypertension, which was adequately controlled with at least one antihypertensive medication.Citation64 Compared with placebo, vardenafil significantly improved SEP2 and SEP3 success rates over the study period (P < 0.0001). In vardenafil-treated patients, average SEP2 success rates increased from 50% at baseline to 84% at week 12, compared with a corresponding increase from 49% to 59% in the placebo group. SEP3 rates increased from 18% at baseline to 68% at week 12 in the vardenafil group, compared with an increase from 18% to 35% for placebo. Improved erections (measured by the Global Assessment Question: “Has the treatment you have taken over the past 4 weeks improved your erections?”) were reported by 80% of patients receiving vardenafil versus 40% of those on placebo.
Shabsigh et al conducted a meta-analysis of 8 randomized, double-blind, placebo-controlled, flexible-dose trials of vardenafil in men with ED (n = 2427), where 839 patients (35%) had self-reported hypertension.Citation44 After 12 weeks of vardenafil treatment, statistically significant and clinically meaningful improvements were observed in all primary outcome measures (IIEF-EF, SEP2, SEP3), compared with placebo. IIEF-EF scores increased by an average of 8.9 points, while SEP2 and SEP3 success rates increased by an average of 32.4% and 38.0%, respectively. A comparison of men with and without hypertension showed no significant differences in any of the three outcome measures, suggesting that vardenafil is equally efficacious for the treatment of ED in both patient groups.
Dyslipidemia
Dyslipidemia is believed to be a causal factor in the endothelial damage thought to underlie many cases of organic ED.Citation59 It has been demonstrated that statin therapy to correct lipid levels improves penile rigidity in men with ED and hypercholesterolemia. Citation65 There are few studies evaluating the efficacy of PDE-5 inhibitors in men with ED and dyslipidemia. A 12-week, double-blind, placebo-controlled study investigated the efficacy of flexible-dose vardenafil in men with ED and dyslipidemia on stable statin therapy.Citation28 In addition to dyslipidemia, 61% of subjects had hypertension and 40% had diabetes. Vardenafil treatment was associated with significant improvements in IIEF-EF scores and SEP2 and SEP3 success rates compared with placebo (P < 0.001). After 12 weeks of treatment, least squares (LS) mean IIEF-EF scores using LOCF were 22.0 vs 14.8 for vardenafil vs placebo, while LS adjusted mean success rates for vardenafil vs placebo were: SEP2, 79.1% vs 51.9% and SEP3, 66.7% vs 33.8%.
Efficacy of vardenafil in patients with ED taking concomitant medications
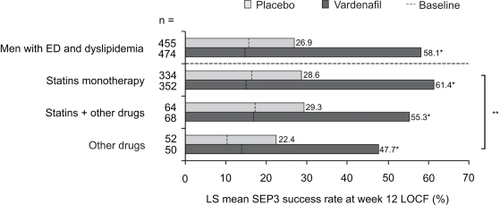
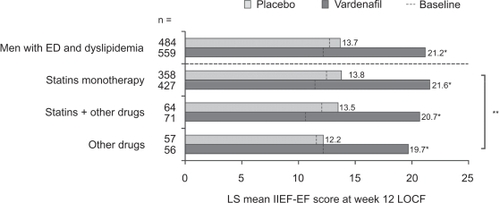
A recent pooled analysis was conducted on individual patient data from 13 randomized, double-blind, placebo-controlled trials of flexible-dose vardenafil of at least 12 weeks’ duration.Citation66 Primary efficacy measures were the IIEF-EF, SEP2 and SEP3. Efficacy was assessed in subgroups of patients with ED and co-existing diabetes, hypertension and dyslipidemia according to type of concomitant medication taken. Consistent with the findings of earlier studies, the concomitant use of medications was not associated with any noteworthy changes in the efficacy of vardenafil. Across all subgroups, vardenafil was statistically superior to placebo over 12 weeks of treatment (P < 0.0001) ( to ). Further, vardenafil treatment resulted in a significant improvement from baseline in IIEF-EF scores and SEP2 and SEP3 success rates, irrespective of the type of medication used (P < 0.0001) ( to ).
Figure 1 LS mean IIEF-EF scores in patients with ED and diabetes, stratified by type of antidiabetic medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
Figure 6 LS mean SEP3 success rates in patients with ED and dyslipidemia, stratified by type of lipid-lowering medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
*P < 0.0001 for vardenafil vs placebo, **P = 0.3536 for comparison of lipid-lowering medication subgroups.
*P < 0.0001 for vardenafil vs placebo, **P = 0.1972 for comparison of antidiabetic medication subgroups.
Abbreviations: ED, erectile dysfunction; IIEF-EF, erectile function domain of the International Index of Erectile Function; LOCF, last observation carried forward; LS, least squares.
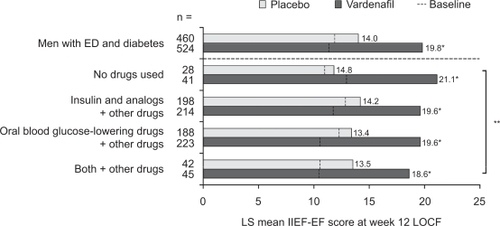
Figure 2 LS mean SEP3 success rates in patients with ED and diabetes, stratified by type of antidiabetic medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
*P < 0.0001 for vardenafil vs placebo, **P = 0.0986 for comparison of antidiabetic medication subgroups.
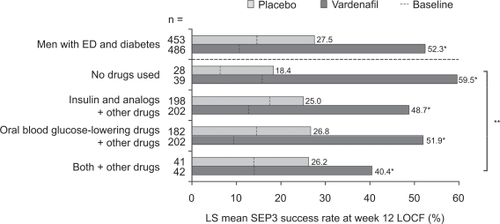
Figure 3 LS mean IIEF-EF scores in patients with ED and hypertension, stratified by type of antihypertensive medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
*P < 0.0001 for vardenafil vs placebo, **P = 0.1651 for comparison of antihypertensive medication subgroups.
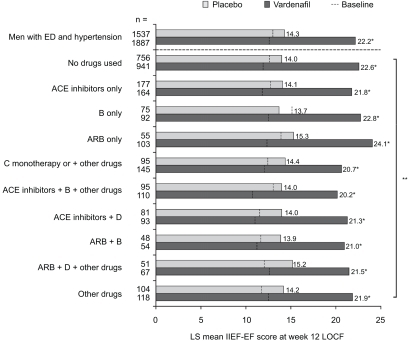
Figure 4 LS mean SEP3 success rates in patients with ED and hypertension, stratified by type of antihypertensive medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
*P < 0.0001 for vardenafil vs placebo, **P = 0.7957 for comparison of antihypertensive medication subgroups.
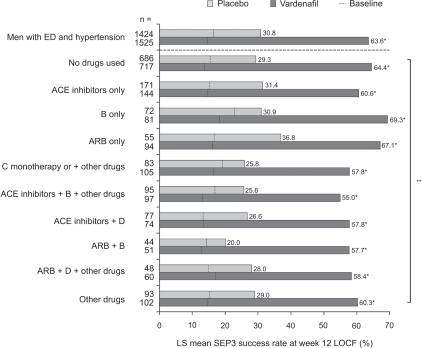
Figure 5 LS mean IIEF-EF scores in patients with ED and dyslipidemia, stratified by type of lipid-lowering medication, at baseline and following 12 weeks of treatment with vardenafil or placebo. Reproduced with permission from Eardley I, Lee Jay C, Shabsigh R, et al. Vardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medications. J Sex Med. 2009.Citation66 In press. Copyright © 2009 Wiley-Blackwell.
*P < 0.0001 for vardenafil vs placebo, **P = 0.9169 for comparison of lipid-lowering medication subgroups.
Efficacy of vardenafil in aging men
Vardenafil improves erectile function in men with ED, including patients over the age of 65 years, the age group in which ED is most prevalent.Citation67 A 12-week multicenter, randomized, double-blind, placebo-controlled, at-home study of vardenafil 5, 10 and 20 mg was conducted in men (n = 580) with mild to severe ED. In a subgroup analysis in which patients were split into 4 age groups (<45 years, 45 to 55 years, 56 to 65 years and >65 years), mean IIEF-EF scores across all age groups were significantly greater for vardenafiltreated patients than those treated with placebo (P < 0.001). No significant differences in the efficacy of vardenafil were observed between age groups.
Duration of erection: a new clinical efficacy measure for vardenafil
Improving penile hardness in men with ED is commonly believed to be the most important factor contributing to successful sexual intercourse. However, there is a body of evidence suggesting that duration of erection, and hence duration of intercourse, may play a role in achieving a satisfactory sexual experience for the man and his partner.Citation68,Citation69
Recent clinical data have demonstrated that vardenafil significantly improves duration of erection in men with ED, including those with underlying conditions. In these studies, a novel efficacy parameter, stopwatch-assessed duration of erection, was employed. A randomized, multicenter, double-blind, placebo-controlled crossover study of fixed-dose vardenafil was conducted in a broad population of men with ED, which included patients with diabetes, hypertension, hyperlipidemia and hypercholesterolemia.Citation29 Over 4 weeks of treatment, vardenafil produced a ∼2.3-fold longer duration of erection than placebo (P < 0.001). Vardenafil also demonstrated a statistically significant superiority over placebo in IIEF-EF scores and SEP2 and SEP3 success rates (all P < 0.001). Duration of erection was also a secondary outcome measure in the study of vardenafil in men with ED and dyslipidemia on stable statin therapy discussed earlier.Citation28 In this study, vardenafil treatment was associated with a ∼3.0-fold longer duration of erection, compared with placebo (P < 0.001).
Efficacy of vardenafil in a real-life observational study
Numerous controlled clinical trials have demonstrated the efficacy of vardenafil in men with ED, including those with associated underlying conditions. These findings were also confirmed in a large observational, open-label study of vardenafil involving over 100,000 participants worldwide. Citation70,Citation71 The Real-Life Safety and Efficacy of vardenafil (REALISE) study recruited patients presenting to their physician with ED and involved a follow-up period of 2 months. An initially prescribed dose of vardenafil could be titrated within the observation period, according to physician recommendation and labeling instructions. Most patients were prescribed vardenafil 10 mg as a starting dose. Treatment outcome was assessed by physician interview; in addition, a voluntary patient questionnaire was used to assess each attempt at sexual intercourse. Although data from REALISE are uncontrolled, they represent real-world experiences with vardenafil, in contrast to rigidly controlled clinical trials.
A pooled analysis of REALISE data from 47 countries in Europe, Asia-Pacific, Latin America and the rest of the world (excluding the United States) has recently been performed (van Ahlen et al in preparation). Data were stratified by the presence of diabetes, hypertension or lipid metabolism disorder. In all subgroups, high numbers of patients reported improvements in erectile function (diabetes, 92.6%; hypertension, 93.6%; lipid metabolism disorder, 94.7%). A large proportion of patients also reported being ‘satisfied’ or ‘very satisfied’ with the efficacy of vardenafil (hypertension 92.0%; diabetes 90.9%; lipid metabolism disorder 93.4%), and stated their intention to continue vardenafil use after the end of the study period.
Safety and tolerability of vardenafil in men with ED and underlying conditions
Interactions between food/alcohol and vardenafil
Vardenafil is rapidly absorbed after the administration of a single oral dose. Absorption is unaffected when taken in conjunction with a meal containing a moderate amount of fat; however, very high fat meals (ie, meals in which more than 57% of the calories come from fat) can affect the rate, but not the extent, of absorption.Citation72 The simultaneous administration of vardenafil and alcohol does not result in any clinically relevant pharmacokinetic or pharmacodynamic interactions.Citation73
Adverse events
The side-effect profile of vardenafil is typical of PDE-5 inhibitors. Commonly reported adverse events in patients receiving vardenafil include headache, rhinitis, flushing and dyspepsia. Citation74,Citation75 Most men with concomitant cardiovascular disease, including heart failure and stable arrhythmias, can be safely treated for ED with vardenafil or other PDE-5 inhibitors.Citation76 Eardley et al’s previously described analysis,Citation66 conducted upon data from a large pool of patients with ED and underlying conditions, showed that the use of concomitant medications did not affect the safety or tolerability of vardenafil in patients with diabetes, hypertension or dyslipidemia. The number and type of the most frequent treatment-emergent adverse events were comparable with those of other studies of PDE-5 inhibitors in these patient groups.
Contraindications
Like other PDE-5 inhibitors, vardenafil is contraindicated in patients taking organic nitrates (eg, nitroglycerin, isosorbide mono- or dinitrate), nitrate preparations used to treat angina, amyl nitrate or amyl nitrite.Citation21,Citation77 This is thought to be due to a stimulation of soluble guanylate cyclase by nitric oxide, resulting in a large cGMP accumulation which in turn and through a cascade of events leads to smooth muscle relaxation, and thus to a decrease in blood pressure. In patients taking alpha blockers (for the treatment of hypertension and/or benign prostatic hyperplasia), vardenafil should be used with caution and patients’ blood pressure carefully monitored. Caution is also recommended with the use of vardenafil in the presence of cytochrome P450, family 3, subfamily A (CYP3A) inhibitors, such as azole antifungal agents, antiretroviral protease inhibitors, macrolid antibiotics, or grapefruit juice.Citation78
Expert opinion
The introduction onto the market of the first PDE-5 inhibitor more than a decade ago profoundly revolutionized medical perceptions of ED, and opened the way to oral pharmacological therapy for this condition. For a long time, experts had denied that there was an underlying organic cause of ED, and almost invariably, patients suffering from ED were referred for counselling to address psychological issues. Improvements in our knowledge and understanding of erectile function were triggered in the late 1980s, with the introduction of intracavernosal injections of vasoactive drugs, followed by therapy with oral agents to safely and effectively treat ED. Risk factors for ED and associated underlying conditions have now been identified, and it is widely accepted that a man presenting with ED in the physician’s office warrants a thorough evaluation of his metabolic and cardiovascular status, in addition to a comprehensive psycho-social-sexual history.
PDE-5 inhibitors constitute the first-line treatment option for men affected by ED, to be combined with counseling on lifestyle, diet, exercise and weight control, if required. A major concern when using PDE-5 inhibitors in men presenting with ED and associated underlying conditions has been cardiovascular safety and potential drug interactions. Apart from the well established absolute contraindication of concomitant use with nitrates or nitric oxide donors, PDE-5 inhibitors have demonstrated excellent safety and efficacy profiles over time.
The data provided in this review demonstrate the efficacy, safety, effectiveness and satisfaction of vardenafil in two different sample populations: men presenting with ED and associated underlying conditions enrolled in clinical trials, and men presenting with ED without contraindications for vardenafil use, enrolled in a large observational study. Efficacy data are derived from clinical trials, effectiveness and satisfaction data are derived from real-life scenarios, and safety data are derived from all the studies reviewed. Physicians should be confident about safety when prescribing vardenafil to patients with ED and associated underlying conditions. Men with underlying conditions are more likely to suffer from ED, which is generally of greater severity. Taking into consideration overall efficacy, patients’ responses to vardenafil treatment are significantly superior compared with placebo, regardless of underlying clinical condition or outcome measure/instrument used (ie, the conventional SEP2, SEP3 and IIEF parameters, or the newly proposed duration of erection measure). This response is also consistent with data obtained from real-life situations, where a high patient satisfaction rate was also demonstrated. Together, this evidence supports the use of vardenafil as a first-line efficacious treatment option for men presenting with ED and underlying conditions.
Conclusion
In light of the evidence that many men with ED also have associated underlying cardiovascular and metabolic conditions, it is important to evaluate the efficacy and safety of PDE-5 inhibitors for ED therapy in these patient groups. There is a significant body of evidence demonstrating the favorable efficacy and safety profile of vardenafil in men with ED and associated underlying conditions including diabetes, hypertension and dyslipidemia. Importantly, the concomitant use of medications, including antihypertensive agents, is not associated with any decreases in efficacy or safety.
Author contributions
Drafting of the article: AMM, VM, JD, PC.
Revision of the intellectual content of the article: AMM, VM, JD, PC.
Final approval of the version for publication: AMM, VM, JD, PC.
Acknowledgements
Writing assistance was provided by Fishawack Communications Ltd. A number of the studies discussed in the manuscript were funded by Bayer Schering Pharma.
Disclosures
All of the authors have acted as speakers, investigators and/or paid consultants for Bayer Schering Pharma.
References
- AytaçIAMcKinlayJBKraneRJThe likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequencesBJU Int199984505610444124
- McKinlayJBThe worldwide prevalence and epidemiology of erectile dysfunctionInt J Impot Res200012Suppl 4S6S1111035380
- GuestJFDas GuptaRHealth-related quality of life in a UK-based population of men with erectile dysfunctionPharmacoeconomics20022010911711888363
- HawtonKIntegration of treatments for male erectile dysfunctionLancet1998351789433420
- Fugl-MeyerARLodnertGBränholmIBFugl-MeyerKSOn life satisfaction in male erectile dysfunctionInt J Impot Res199791411489315491
- MironeVFuscoFRossiASicuteriRMontorsiFTadalafil and vardenafil vs sildenafil: a review of patient-preference studiesBJU Int200910391212121719154480
- FeldmanHAJohannesCBDerbyCAErectile dysfunction and coronary risk factors: prospective results from the Massachusetts Male Aging StudyPrev Med20003032833810731462
- GuayATED2: erectile dysfunction = endothelial dysfunctionEndocrinol Metab Clin North Am20073645346317543729
- NehraAErectile dysfunction and cardiovascular disease: efficacy and safety of phosphodiesterase type 5 inhibitors in men with both conditionsMayo Clin Proc20098413914819181648
- VlachopoulosCIoakeimidisNStefanadisCErectile dysfunction and coronary artery disease: a relationship for disclosureHellenic J Cardiol2008481618350775
- KapurVChienCVFuessJESchwarzERThe relationship between erectile dysfunction and cardiovascular disease. Part II: The role of PDE-5 inhibition in sexual dysfunction and cardiovascular diseaseRev Cardiovasc Med2008918719518953278
- MinerMMErectile dysfunction and the “window of curability”: a harbinger of cardiovascular eventsMayo Clin Proc20098410210419181641
- ShabsighRShahMSandMErectile dysfunction and men’s health: developing a comorbidity risk calculatorJ Sex Med200851237124318439154
- InmanBASt SauverJLJacobsonDJA population-based, longitudinal study of erectile dysfunction and future coronary artery diseaseMayo Clin Proc20098410811319181643
- GazzarusoCSolerteSBPujiaAErectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with angiographically proven asymptomatic coronary artery disease: a potential protective role for statins and 5-phosphodiesterase inhibitorsJ Am Coll Cardiol2008512040204418498958
- MontorsiPRavagnaniPMGalliSAssociation between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trialEur Heart J2006272632263916854949
- HodgesLDKirbyMSolankiJO’DonnellJBrodieDAThe temporal relationship between erectile dysfunction and cardiovascular diseaseInt J Clin Pract200761122019202517997808
- FeldmanHAGoldsteinIHatzichristouDGKraneRJMcKinlayJBImpotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging StudyJ Urol199415154618254833
- TanHMLowWYNgCJPrevalence and correlates of erectile dysfunction (ED) and treatment seeking for ED in Asian Men: the Asian Men’s Attitudes to Life Events and Sexuality (MALES) studyJ Sex Med200741582159217908233
- RosenRCFisherWAEardleyINiederbergerCNadelASandMThe multinational Men’s Attitudes to Life Events and Sexuality (MALES) study: I. Prevalence of erectile dysfunction and related health concerns in the general populationCurr Med Res Opin20042060761715171225
- WespesEAmarEHatzichristouDEAU Guidelines on erectile dysfunction: an updateEur Urol20064980681516530932
- MontagueDKJarowJPBroderickGAChapter 1: The management of erectile dysfunction: an AUA updateJ Urol200517423023915947645
- EardleyIVardenafil: a new oral treatment for erectile dysfunctionInt J Clin Pract20045880180615372854
- MontorsiFPadma-NathanHBuvatJEarliest time to onset of action leading to successful intercourse with vardenafil determined in an at-home setting: a randomized, double-blind, placebo-controlled trialJ Sex Med2004116817816422971
- PorstHSharlipIDHatzichristouDExtended duration of efficacy of vardenafil when taken 8 hours before intercourse: a randomized, double-blind, placebo-controlled studyEur Urol20065010861094 discussion 1094–1095.16820261
- MontorsiFHellstromWJValiquetteLVardenafil provides reliable efficacy over time in men with erectile dysfunctionUrology2004641187119515596195
- ValiquetteLMontorsiFAuerbachSVardenafil demonstrates first-dose success and reliability of penetration and maintenance of erection in men with erectile dysfunction – RELY-IICan Urol Assoc J2008218719518682779
- MinerMGildermanLBailenJVardenafil in men with stable statin therapy and dyslipidemiaJ Sex Med200851455146718373526
- RosenbergMTAdamsPLMcBrideTARobertsJNMcCallumSWImprovement in duration of erection following phosphodiesterase type 5 inhibitor therapy with vardenafil in men with erectile dysfunction: the ENDURANCE studyInt J Clin Pract200963273419125990
- KendirciMBivalacquaTJHellstromWJVardenafil: a novel type 5 phosphodiesterase inhibitor for the treatment of erectile dysfunctionExpert Opin Pharmacother2004592393215102574
- MontorsiFSaloniaABrigantiAVardenafil for the treatment of erectile dysfunction: a critical review of the literature based on personal clinical experienceEur Urol20054761262115826752
- LaumannEOPaikARosenRCSexual dysfunction in the United States: prevalence and predictorsJAMA199928153754410022110
- RosenRCWingRSchneiderSGendranoNEpidemiology of erectile dysfunction: the role of medical comorbidities and lifestyle factorsUrol Clin North Am20053240341716291033
- Martín-MoralesASanchez-CruzJJSaenz de TejadaIRodriguez-VelaLJiminez-CruzJFBurgos-RodriguezRPrevalence and independent risk factors for erectile dysfunction in Spain: results of the Epidemiologia de la Disfuncion Erectil Masculina StudyJ Urol200116656957411458070
- TelesAGCarreiraMAlarcãoVPrevalence, severity, and risk factors for erectile dysfunction in a representative sample of 3,548 Portuguese men aged 40 to 69 years attending primary healthcare centers: results of the Portuguese erectile dysfunction studyJ Sex Med200851317132418194181
- SaigalCSWessellsHPaceJSchonlauMWiltTJPredictors and prevalence of erectile dysfunction in a racially diverse populationArch Intern Med200616620721216432090
- SunPSwindleRAre men with erectile dysfunction more likely to have hypertension than men without erectile dysfunction? A naturalistic national cohort studyJ Urol200517424424815947647
- KlonerRAMullinSHShookTErectile dysfunction in the cardiac patient: how common and should we treatJ Urol2003170S46S50 discussion S50.12853773
- MontorsiFBrigantiASaloniaAErectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery diseaseEur Urol200344360364 discussion 364–365.12932937
- McCullochDKCampbellIWWuFCPrescottRJClarkeBFThe prevalence of diabetic impotenceDiabetologia1980182792837418954
- GiulianoFALericheAJaudinotEOSolesse de GendreAPrevalence of erectile dysfunction among 7689 patients with diabetes or hypertension, or bothUrology2004641196120115596196
- SasakiHYamasakiHOgawaKPrevalence and risk factors for erectile dysfunction in Japanese diabeticsDiabetes Res Clin Pract200570818916126126
- PensonDFLatiniDMLubeckDPWallaceKLHenningJMLueTFDo impotent men with diabetes have more severe erectile dysfunction and worse quality of life than the general population of impotent patients? Results from the Exploratory Comprehensive Evaluation of Erectile Dysfunction (ExCEED) databaseDiabetes Care2003261093109912663579
- ShabsighRDuvalSShahMReganTSJuhaszMVeltryLGEfficacy of vardenafil for the treatment of erectile dysfunction in men with hypertension: a meta-analysis of clinical trial dataCurr Med Res Opin2007232453246017727740
- SeftelADSunPSwindleRThe prevalence of hypertension, hyperlipidemia, diabetes mellitus and depression in men with erectile dysfunctionJ Urol20041712341234515126817
- RoumeguèreTWespesECarpentierYHoffmannPSchulmanCCErectile dysfunction is associated with a high prevalence of hyperlipidemia and coronary heart disease riskEur Urol20034435535912932936
- RaoKDuGHYangWMHyperlipidemia and erectile dysfunctionZhonghua Nan Ke Xue20061264364616894947
- WeiMMaceraCADavisDRHornungCANankinHRBlairSNTotal cholesterol and high density lipoprotein cholesterol as important predictors of erectile dysfunctionAm J Epidemiol19941409309377977280
- CoronaGFortiGMaggiMWhy can patients with erectile dysfunction be considered lucky? The association with testosterone deficiency and metabolic syndromeAging Male20081119319919172551
- CoronaGMannucciEPetroneLA comparison of NCEP-ATPIII and IDF metabolic syndrome definitions with relation to metabolic syndrome-associated sexual dysfunctionJ Sex Med2007478979617498109
- KahnRBuseJFerranniniESternMThe metabolic syndrome: time for a critical appraisal: joint statement from the American Diabetes Association and the European Association for the Study of DiabetesDiabetes Care2005282289230416123508
- TraishAMGuayAFeeleyRSaadFThe dark side of testosterone deficiency: I. Metabolic syndrome and erectile dysfunctionJ Androl200930102218641413
- CoronaGMannucciEFortiGMaggiMHypogonadism, ED, metabolic syndrome and obesity: a pathological link supporting cardiovascular diseasesInt J Androl2009 Epub 2009 Feb 16.
- YassinAASaadFGoorenLJMetabolic syndrome, testosterone deficiency and erectile dysfunction never come aloneAndrologia20084025926418727737
- ShabsighRRajferJAversaAThe evolving role of testosterone in the treatment of erectile dysfunctionInt J Clin Pract2006601087109216939550
- MorelliACoronaGFilippiSWhich patients with sexual dysfunction are suitable for testosterone replacement therapyJ Endocrinol Invest20073088088818075293
- BuvatJBou JaoudeGSignificance of hypogonadism in erectile dysfunctionWorld J Urol20062465766717082935
- MalavigeLSLevyJCErectile dysfunction in diabetes mellitusJ Sex Med200961232124719210706
- EardleyILeeJCGuayATGlobal experiences with vardenafil in men with erectile dysfunction and underlying conditionsInt J Clin Pract2008621594160318822030
- RhodenELRibeiroEPRiednerCETelokenCSoutoCAVGlycosylated haemoglobin levels and the severity of erectile function in diabetic menBJU Int20059561561715705090
- GoldsteinIYoungJMFischerJBangerterKSegersonTTaylorTVardenafil, a new phosphodiesterase type 5 inhibitor, in the treatment of erectile dysfunction in men with diabetes: a multicenter double-blind placebo-controlled fixed-dose studyDiabetes Care20032677778312610037
- IshiiNNagaoKFujikawaKTachibanaTIwamotoYKamidonoSVardenafil 20-mg demonstrated superior efficacy to 10-mg in Japanese men with diabetes mellitus suffering from erectile dysfunctionInt J Urol2006131066107216903931
- FieldsLEBurtVLCutlerJAHughesJRoccellaEJSorliePThe burden of adult hypertension in the United States 1999 to 2000: a rising tideHypertension20044439840415326093
- van AhlenHWahleKKupperWYassinAReblinTNeureitherMSafety and efficacy of vardenafil, a selective phosphodiesterase 5 inhibitor, in patients with erectile dysfunction and arterial hypertension treated with multiple antihypertensivesJ Sex Med2005285686416422810
- SaltzmanEAGuayATJacobsonJImprovement in erectile function in men with organic erectile dysfunction by correction of elevated cholesterol levels: a clinical observationJ Urol200417225525815201788
- EardleyILee JayCShabsighRVardenafil improves erectile function in men with erectile dysfunction and associated underlying conditions, irrespective of the use of concomitant medicationsJ Sex Med2009 In press.
- PorstHYoungJMSchmidtACBuvatJEfficacy and tolerability of vardenafil for treatment of erectile dysfunction in patient subgroupsUrology20036251952412946758
- SchnablSCorrelations and Determinants of Functional Sexual DisturbancesLittleton, MAPSG Publishing1980
- WeissPBrodySWomen’s partnered orgasm consistency is associated with greater duration of penile-vaginal intercourse but not of foreplayJ Sex Med2009613514119170844
- KamelAKhaouliRSabhaMAl MitwallyKFouadWLandenHThe real-life efficacy and safety of vardenafil: an international post-marketing surveillance study of 2824 patients from the Middle EastClin Drug Investig2007275339346
- TobingNLArsyadKMManuputtyDLandenHSyarifHThe real-life safety and efficacy of vardenafil: an international post-marketing surveillance study from 1171 Indonesian patientsMaj Kedokt Indon2006568468473
- RajagopalanPMazzuAXiaCEffect of high-fat breakfast and moderate-fat evening meal on the pharmacokinetics of vardenafil, an oral phosphodiesterase-5 inhibitor for the treatment of erectile dysfunctionJ Clin Pharmacol200343326026712638394
- WensingGBauerRUngerSRohdeGHeinigRSimultaneous administration of vardenafil and alcohol does not result in a pharmacodynamic or pharmacokinetic interaction in healthy male subjectsInt J Clin Pharmacol Ther200644521622416724576
- HellstromWJGittelmanMKarlinGVardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trialJ Androl20022376377112399521
- KeatingGScottLVardenafil: a review of its use in erectile dysfunctionDrugs200363232673270314636086
- RosenRCJacksonGKostisJBErectile dysfunction and cardiac disease: recommendations of the Second Princeton ConferenceCurr Urol Rep2006749049617052447
- KostisJBJacksonGRosenRSexual dysfunction and cardiac risk (the Second Princeton Consensus Conference)Am J Cardiol20059685M93M
- CoronaGRazzoliEFortiGMaggiMThe use of phosphodiesterase 5 inhibitors with concomitant medicationsJ Endocrinol Invest20083179980818997493