Abstract
Asthma is a chronic inflammatory disorder of the airways that requires long-term treatment, the goal of which is to control clinical symptoms for extended periods with the least possible amount of drugs. International guidelines recommend the addition of an inhaled long-acting beta2-agonist (LABA) to a low- to medium-dose inhaled corticosteroid (ICS) when low doses of ICS fail to control asthma symptoms. The fixed combined administration of ICS/LABA improves patient compliance, reducing the risk of therapy discontinuation. The relative deposition pattern of the inhaled drug to the target site is the result of a complex interaction between the device used, the aerosol formulation and the patient’s adherence to therapy. Different inhalation devices have been introduced in clinical practice over time. The new hydrofluoroalkane (HFA) solution aerosols allow for the particle size to be modified, thus leading to deeper penetration of the medication into the lung. The Modulite® technology allows for the manipulation of inhaled HFA-based solution formulations, such as the fixed beclomethasone/formoterol combination, resulting in a uniform treatment of inflammation and bronchoconstriction. The success of any anti-asthmatic treatment depends on the choice of the correct device and the adherence to therapy.
Keywords:
Introduction
Asthma is a chronic inflammatory disorder of the airways characterized by a variable degree of airway obstruction, which can reverse spontaneously or after treatment, and an underlying condition of exaggerated airway narrowing in response to external stimuli. The chronic features of the disease imply a long-term treatment to attain optimal control of the respiratory symptoms. Indeed, the goal of treatment is to achieve and maintain control of clinical symptoms for extended periods with the least possible amount of drugs.
Control of the disease is optimal when the patient presents with no diurnal or night-time symptoms, no limitation of daily activities including exercise, minimum use of beta2-agonists, and no need for hospitalization. According to epidemiological observations, a variable proportion of the asthmatic population does not control the disease because of factors that include inadequate drug treatment, and lack of adherence to the recommended drug therapy or to the device. In addition, physicians and patients tend to underestimate the intensity and frequency of symptoms, and the need to monitor the disease. The occurrence of inadequate physician–patient communication also contributes to the lack of optimal control. As already cited, the lack of adherence to therapy strongly impacts on the control of the disease. Cramer et alCitation1 demonstrated that the frequency of drug administration influences adherence to treatment, decreasing from 87% with one administration per day to 39% when four administrations per day are requested. Long-term treatment as a factor affecting adherence to treatment was shown in a 1-year study conducted in adults and children:Citation2 at the end of the study, only 15% of patients was still receiving inhaled treatment regularly. Above all, it appears pertinent to state that drugs don’t work in patients who don’t take them!
Several epidemiological studies have been conducted in an effort to determine whether asthma control is attainable and in what proportion of patients. The AIRE (Asthma Insights and Reality in Europe) study,Citation3 conducted on a sample of 2803 patients to examine the management of asthma in Europe, showed that despite the existence of highly effective treatments, frequent daytime and nocturnal symptoms and limitations of daily activities are reported by patients, including a high frequency of requests for unscheduled doctor visits, emergency department visits, and hospitalization for serious exacerbations. The ISAYA studyCitation4 confirmed that the inappropriate use of drugs is mainly responsible for failure to control asthma. This study found that 47% of persistent asthmatics that participated in the survey in Italy were using combination therapy that was inadequate for the severity level (too low a dosage of corticosteroids and/or inappropriate treatment), and that 64% of asthmatics were on an irregular treatment that should have been taken daily. The study confirmed that for each degree of severity, regularity of treatment was associated with better control of symptoms.
In evaluating whether optimal asthma control is attainable with current therapeutic options, the GOAL studyCitation5 showed that asthma control can be reached in a high percentage of patients, and this occurs more frequently when a regimen is implemented based on the degree of severity. The study provided evidence that the salmeterol/fluticasone combination is more effective than treatment with fluticasone alone in achieving good asthma control. Of particular importance is the finding that the salmeterol/fluticasone combination was able to control symptoms more quickly and at a lower dose of corticosteroid. The observed improvements in several clinical and functional parameters were clinically relevant and sustained over time, stressing the importance of regular and prolonged treatment.
Inhaled therapy in asthma
The cornerstone of the daily control of asthma is inhaled therapy. In this respect, direct delivery of the aerosolized drug in the lower airways is advocated to treat inflammation and to relieve obstruction. In comparison with oral therapy, the inhaled pathway allows the minimization of effective doses and consequently minimization of adverse systemic effects, particularly important for long-term treatments often necessary in asthma. On the other hand, several variables affect the inhaled pathway, mostly related to the drug formulation and delivery device. Pharmacological treatment of asthma requires a stepwise approach based on the severity of the disease, which can be adapted continuously according to the clinical control of the disease. The ultimate goal of treatment is to achieve and maintain control of clinical symptoms for extended periods with the least possible amount of drugs.
Inhaled glucocorticosteroids (ICS) represent first-line treatment for the management of asthma, in that they are the most effective anti-inflammatory medications for the treatment of persistent symptoms (). Most studies have demonstrated their efficacy in controlling airway inflammation,Citation6 reducing symptoms, improving quality of life and lung function, decreasing airway hyper-responsiveness,Citation7 reducing frequency and severity of exacerbations,Citation8 and reducing asthma mortality.Citation9 International guidelines recommend the addition of an inhaled long-acting beta2-agonist (LABA) to a low- to medium-dose ICS when low doses of ICS fail to control asthma symptoms.Citation10 Randomized clinical trials with LABA in combination with corticosteroids have demonstrated that the addition of LABA to ICS is more beneficial in terms of asthma control and pulmonary function than increasing the dose of ICS alone.Citation11–Citation14 When administered as fixed combination, the administration of ICS/LABA has been demonstrated to improve patient compliance, thus reducing the risk of therapy discontinuation,Citation15 compared to the administration of these components separately. There is evidence suggesting that LABA and ICS mutually potentiate their effects when given in combination.Citation16
Table 1 Effects of glucocorticoids on the pathogenic mechanisms of airway inflammation
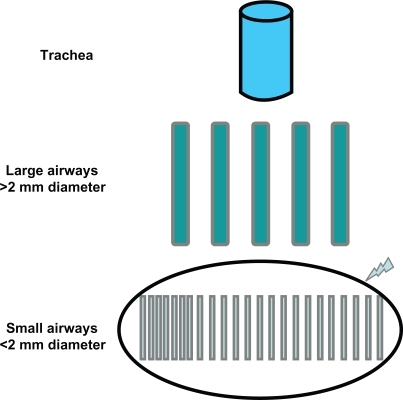
The aim of inhaled therapy is to allow the medication to reach the target site. This can be attained by ensuring the penetration of the aerosolized particles into the lower respiratory tract, and the deposition of the drug along the respiratory tract. Obviously, the deposition of the drug should translate into functional and clinical benefits. Taken together, these conditions also require the right choice of device.Citation17 The relative deposition pattern of the inhaled drug is the result of a complex interaction between the aerosol formulation and the device used. A body of histological and functional evidence has accumulated to confirm that the distal airways are the predominant site of airway inflammation in asthma;Citation18–Citation21 therefore, the distal airways represent the main target of treatment (), and the distribution of the drug along the bronchial tree should translate into higher efficacy of the inhaled therapy and reduced rate of adverse events. Most importantly, similar clinical benefit can be attained with a lower dose of the drug.Citation22
Figure 1 Schematic of the bronchial tree with emphasis on the peripheral district, which is the main target of anti-asthmatic treatment.
The devices differ in terms of technical design (required inspiratory flow rate, actuation), composition (characteristics of the propellant, carrier substances), dose per inhalation, and costs. In addition, producers have made major efforts to make devices more user-friendly. The pressurized metered dose inhaler (pMDI) is the most widely used device.Citation23 The major issue with the use of pMDIs is that the aerosol is fast-moving, which increases the risk of drug deposition in the pharynx, and therefore occurrence of local side-effects with limited clinical efficacy. The drug contained in the MDI canister is formulated as a suspension or solution, formulations which have different properties in terms of particle size, plume velocity and duration, as well as user friendliness, which affect drug delivery to the appropriate site. In the suspension formulation, the active drug is insoluble in the propellant and remains as solid powder; therefore, suspension formulations need to be shaken before inhalation to allow uniform distribution of solid powder particles of the drug. It has been demonstrated that a significant proportion of patients do not shake the device properly or present with coordination problems,Citation24 resulting in variable amounts of drug emitted in each aerosol puff. The occurrence of mistakes associated with the inhalation procedures can be reduced by regular training and follow-up. Other devices include breath-actuated pMDIs (BA-pMDI), such as Autohaler® and Easi-Breathe®, which incorporate a mechanism activated during inhalation that triggers the metered-dose inhaler. Dry powder inhalers (DPIs) do not need coordination, as the drug is not driven by the propellant but is delivered by the inhalation effort. However, the actuation of the device needs high inspiratory flow to assure optimal drug delivery,Citation25 which is crucial in the elderly. Indeed, Janssens and colleaguesCitation26 recently demonstrated that, in elderly patients, the ability to generate sufficient inspiratory flow across a dry powder inhaler is compromised, irrespective of the presence of chronic obstructive pulmonary disease (COPD). Three types of DPIs are available with different handling instructions: single dose (Handihaler®, Aerolizer®), multiple doses (Diskus®) and reservoir (Turbohaler®). An official document on device selection and outcomes of aerosol therapy based on current literature reported that, when selecting a device for patients with asthma and COPD, the following should be considered: device/drug availability, patient age and the ability to use the selected device correctly, device use with multiple medications, and physician and patient preference.Citation27 Evidence-based guidelines for the device selection conclude that no difference between devices in any efficacy outcome has been recorded, provided that patients use the correct technique for inhalation. Therefore, the selection criteria should be related mainly to patient age, preference and ability to use the selected device correctly. describes the main properties of each device.
Table 2 Description of the main properties of different devices
The Modulite® technology and the beclomethasone dipropionate/formoterol combination
Since the 1987 Montreal Protocol that abolished chlorofluorocarbon (CFC) use in inhalers investigated, a hydrofluoroalkane propellant (HFA-134a) was developed as a nonozone-depleting CFC-free alternative for use in pMDI. The limits of the pMDI (difficulty to coordinate, low lung deposition, high oral deposition, need of a spacer) are not present in HFA inhalers, which are largely accepted by patients.Citation28 Studies comparing beclometasone HFA with CFC inhalers showed no difference in terms of adverse events (oral thrush and hoarse voice).Citation28 The new HFA solution aerosols allow for the particle size to be modified, thus leading to deeper penetration of the medication into the lung.Citation29 Recently, a new technology of the HFA solution pMDI has been developed:Citation30 the Modulite® (Chiesi Ltd) platform technology allows for the manipulation of inhaled HFA-based solution formulations. This technology offers the advantage of matching the CFC-based pMDIs with the HFA-MDIs on a 1:1 nominal dose ratio basis, thus favoring the transition to CFC-free formulations. Switching from CFC-MDI to HFA-MDI has been achieved successfully for corticosteroidsCitation31 and bronchodilators.Citation32 Recently, the HFA-propelled extra-fine fixed combination formulation of beclometasone dipropionate/formoterol (BDP/F) 100/6 μg (Foster®) delivered via pMDI has been developed with the Modulite® technology. The BDP/F HFA pMDI combination is an extra-fine formulation, in which BDP dose is 2.5-fold lower than the conventional BDP CFC product (100 μg of BDP per actuation instead of 250 μg of nonextra-fine BDP). Furthermore, because of the small particle size of BDP/F, the two active drugs are delivered to both central and peripheral airways, resulting in a uniform treatment of inflammation and bronchoconstriction. The reduction in BDP dose lowers the amount of drug deposited in the upper airway, potentially improving the efficacy/safety ratio. Therefore, the optimized drug deposition that results from reduced particle size may lead to improved clinical benefit, as shown by Huchon et al.Citation33 The slower velocity and the longer duration of the plume reduce the throat deposition and improve the lung deposition of the drug.
Clinical efficacy and safety of beclomethasone/formoterol combination
A body of literature has demonstrated the efficacy and safety of both beclomethasone and formoterol separately and as fixed combination treatment, as reviewed by Nicolini et al,Citation34 and by Fabbri et al.Citation35 The efficacy of the BDP/F fixed combination was evaluated in a 3-month randomized controlled trial conducted in patients with moderate asthma who were still symptomatic despite receiving low-dose ICS.Citation36 BDP/F given as one inhalation twice daily improved lung function by more than a double equipotent dosage of BDP nonextra-fine. In patients with severe asthma,Citation36 BDP/F given as two inhalations twice daily for 6 months showed improvement in peak expiratory flow and forced expiratory volume in 1 second comparable to that of an equipotent nonextra-fine regimen of BDP and formoterol administered via separate inhalers, and was more effective than 1000 μg/day BDP nonextra-fine. Importantly, the BDP/F fixed combination was superior to both BDP plus formoterol in separate inhalers and BDP monotherapy in terms of clinical measures of asthma control, suggesting that patients receiving extra-fine BDP/F may experience additional benefits to functional improvements.
Two studies with similar resultsCitation37,Citation38 were conducted to assess the efficacy and tolerability of BDP/F vs budesonide/formoterol (BUD/F) and fluticasone propionate/salmeterol (FP/S), respectively. In the first study,Citation38 patients who were taking BDP/F as two inhalations twice daily showed similar improvement in lung function, asthma symptoms and percentage of days without the use of rescue medication to that obtained with an equipotent regimen of BUD/F 200/6 μg administered as two puffs twice daily. Interestingly, BDP/F demonstrated similar onset of action to that of BUD/F. In the second study,Citation37 BDP/F was compared with fluticasone propionate/salmeterol (FP/S) pMDI 125/25 μg, both administered as two puffs twice daily, and lung function improved similarly in both arms. In this study, the BDP/F group had a faster onset of bronchodilation as opposed to the FP/S group. This is of great importance, based on the fact that patients ask for immediate relief of symptoms, and this can drastically improve adherence to treatment and, consequently, asthma control. Of note, a greater improvement in forced vital capacity was shown in the BDP/F group, suggesting a greater effect on peripheral airways.
Patient perspectives and outcomes
Asthmatic patients are worried about three different aspects of the disease: asthmatic exacerbations, management of symptoms, and management of the disease during an exacerbation-free period. Even if asthmatic exacerbations could be the most important event in a patient’s life, the impact of asthma on everyday life could be an important factor also when asthma is asymptomatic. For the patient, the way of approaching emerging health-related problems depends on the severity of the clinical manifestations as well as on the strategies that are used to solve them (coping strategies) and on previous experiences. Different studies have clearly confirmed a weak correlation between the magnitude of airway obstruction and the severity of asthmatic symptoms.Citation39
It is therefore important to understand needs and expectations of asthmatic patients in order to obtain optimal disease management. Several surveysCitation40,Citation41 note that these patients have little information about their asthma and they live with diurnal and nocturnal symptoms. Moreover, these studies emphasize that patients are not completely satisfied with physician behavior. Moreover, patients often do not trust pharmacological treatment, and they are not convinced that therapy can completely control asthmatic symptoms.
Nowadays, effective diagnostic and therapeutic tools are widely available. In chronic diseases such as asthma, diagnosis and therapy are not sufficient to obtain the improvement of health status. In fact, adherence to therapy, although often underestimated, is necessary to obtain optimal control of asthma; proper management of therapy is probably more useful then expensive investments to improve current therapies. Nonadherence may involve up to 20% of patients who need treatment for a short period (10 days) because of an acute disease, up to 50% of patients affected by a chronic symptomatic disease, and up to 70% of those affected by a chronic asymptomatic disease. Coping strategies, which represent the way patients face the disease, determine individual differences in the psychological reactions towards asthma,Citation42–Citation45 which in turn influence the adherence to treatment and quality of life.
Nonadherence can occur in only one phase of the treatment (eg, a patient takes drugs regularly but does not change their life-style, for example, they do not quit smoking); or it can occur in different phases of treatment (eg, some patients are more adherent to therapy during weekends than weekdays). Moreover, patients may spontaneously stop therapy to verify their recovery and efficacy of treatment. Nonadherence has some consequences for patients and their relatives, for the health system and for society. The consequences of nonadherence are shown in .
Table 3 Consequences of nonadherence
Several different factors reduce adherence to therapy
Factors related to treatment:Citation46,Citation47 complex medical treatment that requires the use of different drugs; the complexity of dosage and the different devices used for inhalation therapy; the side effects of medications.
Factors related to the patient: age; low perception of the disease; personal ideas about treatment; cognitive or physical impairments; psychological or psychiatric disorders; absence of family or social support; financial difficulties; the refusal to accept the disease.
Factors related to the health system organization: difficult admission to medical facilities; health welfare discontinuation; high costs for patients.
Factors related to the relationship between physicians and patients:Citation48 ineffective communication; inadequate patient or doctor behavior; inability to understand the patient perspectives on disease and treatment.
Different strategies can improve adherence to therapy.Citation49 These can be summarized as follows: improve patient–physician communication, simplify the therapeutic plan (if possible reduce the number of daily doses, using the simplest and most effective inhalator devices), and reduce the waiting lists. As stated by Juniper,Citation50 both the clinician and the patient decide on the patient’s management plan, by negotiating a plan that the patient is willing to follow. A contractual agreement between patient and clinician may improve both clinical asthma control and patient health-related quality of life.
Conclusions
Treatment of asthma aims at achieving and maintaining control of symptoms by using inhaled LABA and ICS. The fixed combined administration of ICS/LABA improves patient compliance, thus reducing the risk of therapy discontinuation. The optimal control of asthma depends on the drug selected, the device used, and the elimination of factors that reduce patient adherence to therapy. Inhalers differs in their delivery technique, their efficiency, and their ease of use. The new aerosol technologies allow for the particle size to be modified, thus leading to deeper penetration of the medication into the lung. How a patient approaches the different components of the disease depends on the strategies they use to cope with them, which is why international asthma guidelines stress that before making changes to a patient’s therapy their compliance and inhaler technique should be checked. Adherence to treatment can be considered as the final result of interactions among the patient, the disease, the treatment, and the health system organization.
Disclosures
The authors declare no conflicts of interest.
References
- CramerJAMattsonRHPreveyMLScheyerRDOuelletteVLHow often is medication taken as prescribed? A novel assessment techniqueJAMA1989 926122327332772716163
- Breekveldt-PostmaNSKoerselmanJErkensJAvan der MolenTLammersJWHeringsRMTreatment with inhaled corticosteroids in asthma is too often discontinuedPharmacoepidemiol Drug Saf200817441142218205251
- VermeirePARabeKFSorianoJBMaierWCAsthma control and differences in management practices across seven European countriesRespir Med200296314214911905548
- De MarcoRCazzolettiLCerveriICorsicoABugianiMAccordiniSAre the asthma guideline goals achieved in daily practice? A population-based study on treatment adequacy and the control of asthmaInt Arch Allergy Immunol2005138322523416210861
- BatemanEDBousheyHABousquetJBusseWWClarkTJPauwelsRACan guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL studyAm J Respir Crit Care Med2004170883684415256389
- JefferyPKGodfreyRWAdelrothENelsonFRogersAJohanssonSAEffects of treatment on airway inflammation and thickening of basement membrane reticular collagen in asthma. A quantitative light and electron microscopic studyAm Rev Respir Dis1992145(4 Pt 1):8908991554218
- JuniperEFKlinePAVanzieleghemMARamsdaleEHO’ByrnePMHargreaveFEEffect of long-term treatment with an inhaled corticosteroid (budesonide) on airway hyperresponsiveness and clinical asthma in nonsteroid-dependent asthmaticsAm Rev Respir Dis199014248328362221590
- PauwelsRALofdahlCGPostmaDSTattersfieldAEO’ByrnePBarnesPJEffect of inhaled formoterol and budesonide on exacerbations of asthma. Formoterol and Corticosteroids Establishing Therapy (FACET) International Study GroupN Engl J Med199733720140514119358137
- SuissaSErnstPBenayounSBaltzanMCaiBLow-dose inhaled corticosteroids and the prevention of death from asthmaN Engl J Med2000343533233610922423
- Global INitiative for Asthma (GINA)Global strategy for asthma management and prevention: NHLBI/WHO workshop reportNational Heart, Lung and Blood InstituteBethesda, MD Updated2006
- BatemanEDBantjeTAJoao GomesMToumbisMGHuberRMNayaICombination therapy with single inhaler budesonide/formoterol compared with high dose of fluticasone propionate alone in patients with moderate persistent asthmaAm J Respir Med20032327528114720008
- LallooUGMalolepszyJKozmaDKroftaKAnkerstJJohansenBBudesonide and formoterol in a single inhaler improves asthma control compared with increasing the dose of corticosteroid in adults with mild-to-moderate asthmaChest200312351480148712740264
- RingdalNElirazAPruzinecRWeberHHMulderPGAkveldMThe salmeterol/fluticasone combination is more effective than fluticasone plus oral montelukast in asthmaRespir Med200397323424112645830
- TalASimonGVermeulenJHPetruVCobosNEverardMLBudesonide/formoterol in a single inhaler versus inhaled corticosteroids alone in the treatment of asthmaPediatr Pulmonol200234534235012357478
- RosenhallLBorgSAnderssonFEricssonKBudesonide/formoterol in a single inhaler (Symbicort) reduces healthcare costs compared with separate inhalers in the treatment of asthma over 12 monthsInt J Clin Pract200357866266714627174
- BarnesPJAsthma. New therapeutic approachesBr Med Bull19924812312471352169
- BrocklebankDWrightJCatesCSystematic review of clinical effectiveness of pressurised metered dose inhalers versus other hand held inhaler devices for delivering corticosteroids in asthmaBMJ2001323731889690011668133
- BattagliaSden HertogHTimmersMCLazeromsSPVignolaAMRabeKFSmall airways function and molecular markers in exhaled air in mild asthmaThorax200560863964416061704
- BourdinAPaganinFPrefautCKieselerDGodardPChanezPNitrogen washout slope in poorly controlled asthmaAllergy2006611858916364161
- in ’t VeenJCBeekmanAJBelEHSterkPJRecurrent exacerbations in severe asthma are associated with enhanced airway closure during stable episodesAm J Respir Crit Care Med200016161902190610852764
- WagnerEMLiuMCWeinmannGGPermuttSBleeckerERPeripheral lung resistance in normal and asthmatic subjectsAm Rev Respir Dis199014135845882178524
- PritchardJNThe influence of lung deposition on clinical responseJ Aerosol Med200114Suppl 1S19S2611424889
- VirchowJCCromptonGKDal NegroRPedersenSMagnanASeidenbergJImportance of inhaler devices in the management of airway diseaseRespir Med20081021101917923402
- GiraudVRocheNMisuse of corticosteroid metered-dose inhaler is associated with decreased asthma stabilityEur Respir J2002192246245111866004
- TarsinWYPearsonSBAssiKHChrystynHEmitted dose estimates from Seretide Diskus and Symbicort Turbuhaler following inhalation by severe asthmaticsInt J Pharm20063161–213113716584855
- JanssensWVandenBrandePHardemanEDe LangheEPhilpsTTroostersTInspiratory flow rates at different levels of resistance in elderly COPD patientsEur Respir J2008311788317898020
- DolovichMBAhrensRCHessDRAndersonPDhandRRauJLDevice selection and outcomes of aerosol therapy: Evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and ImmunologyChest2005127133537115654001
- Vanden BurgtJABusseWWMartinRJSzeflerSJDonnellDEfficacy and safety overview of a new inhaled corticosteroid, QVAR (hydrofluoroalkane-beclomethasone extrafine inhalation aerosol), in asthmaJ Allergy Clin Immunol200010661209122611112914
- GoldinJGTashkinDPKleerupECGreaserLEHaywoodUMSayreJWComparative effects of hydrofluoroalkane and chlorofluorocarbon beclomethasone dipropionate inhalation on small airways: assessment with functional helical thin-section computed tomographyJ Allergy Clin Immunol19991046S258S26710588987
- AcerbiDBrambillaGKottakisIAdvances in asthma and COPD management: delivering CFC-free inhaled therapy using Modulite technologyPulm Pharmacol Ther200720329030316890465
- ThongngarmTSilkoffPEKossackWSNelsonHSHydrofluoroalkane-134A beclomethasone or chlorofluorocarbon fluticasone: effect on small airways in poorly controlled asthmaJ Asthma200542425726316032934
- HoughtonCMLangleySJSinghSDHoldenJMonici PretiAPAcerbiDComparison of bronchoprotective and bronchodilator effects of a single dose of formoterol delivered by hydrofluoroalkane and chlorofluorocarbon aerosols and dry powder in a double blind, placebo-controlled, crossover studyBr J Clin Pharmacol200458435936615373928
- HuchonGMagnussenHChuchalinADymekLGonodFBBousquetJLung function and asthma control with beclomethasone and formoterol in a single inhalerRespir Med20091031414918977646
- NicoliniGScichiloneNBizziAPapiAFabbriLMBeclomethasone/formoterol fixed combination for the management of asthma: patient considerationsTher Clin Risk Manag20084585586419209268
- FabbriLMNicoliniGOlivieriDPapiAInhaled beclometasone dipropionate/formoterol extra-fine fixed combination in the treatment of asthma: evidence and future perspectivesExp Opin Pharmacother200893479490
- DhillonSKeatingGMBeclometasone dipropionate/formoterol: in an HFA-propelled pressurised metered-dose inhalerDrugs2006661114751483 discussion 84–8516906779
- PapiAPaggiaroPNicoliniGVignolaAMFabbriLMBeclomethasone/formoterol vs fluticasone/salmeterol inhaled combination in moderate to severe asthmaAllergy200762101182118817845589
- PapiAPaggiaroPLNicoliniGVignolaAMFabbriLMBeclomethasone/formoterol versus budesonide/formoterol combination therapy in asthmaEur Respir J200729468268917107988
- ApterAJAffleckGReisineSTTennenHABarrowsEWellsMPerception of airway obstruction in asthma: sequential daily analyses of symptoms, peak expiratory flow rate, and moodJ Allergy Clin Immunol19979956056129155825
- HolgateSTPriceDValovirtaEAsthma out of control? A structured review of recent patient surveysBMC Pulm Med20066Suppl 1S217140420
- KoningsEDubois-ArberFNarringFMichaudPAIdentifying adolescent drug users: results of a national survey on adolescent health in SwitzerlandJ Adolesc Health19951632402477779836
- MilesJFGardenGMTunnicliffeWSCaytonRMAyresJGPsychological morbidity and coping skills in patients with brittle and non-brittle asthma: a case-control studyClin Exp Allergy19972710115111599383255
- AaltoAMHarkapaaKAroARRissanenPWays of coping with asthma in everyday life: validation of the Asthma Specific Coping ScaleJ Psychosom Res20025361061106912479987
- AdamsRJSmithBJRuffinREFactors associated with hospital admissions and repeat emergency department visits for adults with asthmaThorax200055756657310856316
- AdamsSPillRJonesAMedication, chronic illness and identity: the perspective of people with asthmaSoc Sci Med19974521892019225407
- BarberNParsonsJCliffordSDarracottRHorneRPatients’ problems with new medication for chronic conditionsQual Saf Health Care200413317217515175485
- ClaxtonAJCramerJPierceCA systematic review of the associations between dose regimens and medication complianceClin Ther20012381296131011558866
- FuertesJNMislowackABennettJPaulLGilbertTCFontanGThe physician-patient working alliancePatient Educ Couns2007661293617188453
- CorsicoAGCazzolettiLde MarcoRJansonCJarvisDZoiaMCFactors affecting adherence to asthma treatment in an international cohort of young and middle-aged adultsRespir Med200710161363136717188854
- JuniperEFThe impact of patient compliance on effective asthma managementCurr Opin Pulm Med20039Suppl 1S8S1012974536