Abstract
Usage of the Vibrant Soundbridge (VSB) with round window (RW)-Coupler placement at the RW has been shown to successfully treat mixed hearing loss. Coupling between the VSB's floating mass transducer (FMT) and the RW membrane is difficult in the case of sclerosis in the RW and drilling down the bony lip until the RW membrane can be seen completely can possibly induce a perilymphatic fistula. A 68-year-old woman who had bilateral mixed hearing loss with sclerosis in the RW due to tympanosclerosis underwent a RW-Vibroplasty with a RW-Coupler. Speech discrimination scores in quiet and noise and functional gain with the VSB with RW-Coupler were better than those using a conventional hearing aid. The results of the present case have shown the feasibility of implanting a VSB with RW-Coupler in patients with mixed hearing loss due to tympanosclerosis.
Introduction
Active middle ear implants are an alternative treatment option for various forms of hearing loss. The Vibrant Soundbridge (VSB) comprises an implanted receiver module connected via a conductor link to a floating mass transducer (FMT) and an externally worn audio processor that contains speech-processing circuitry. The classic indication for the use of VSB is sensorineural hearing loss, in which case the FMT is crimped to the long process of the incus with a titanium clip [Citation1]. In 2006, Coletti et al. [Citation2] were the first to describe the application of the VSB on the round window (RW), termed as RW-Vibroplasty, which is emerging as a versatile solution for various causes of conductive or mixed hearing loss. In these patients, conventional hearing aids and/or surgical restoration are either not possible or have failed because of chronic ear disease, extensive otosclerosis, or malformation.
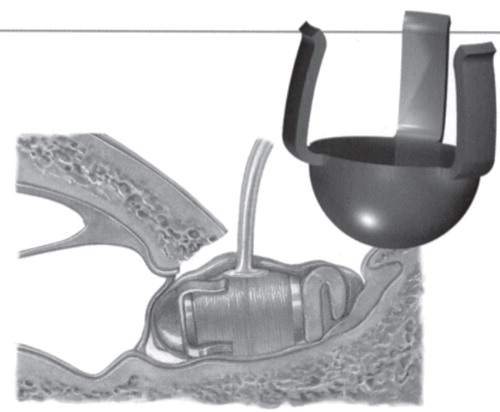
Some surgeons emphasize that the FMT needs to be in complete contact with the round window (RW) membrane for the RW-Vibroplasty to be effective [Citation2]. However, the anatomic mismatch between the diameter of the RW membrane and the FMT diameter does not accommodate complete FMT–RW membrane contact. In cases of sclerosis in the RW, coupling between the FMT and the RW membrane may be difficult because drilling the lesion of sclerosis in the RW can possibly induce a perilymphatic fistula. We report a case of a patient with sclerosis in the RW due to tympanosclerosis who underwent RW-Vibroplasty with a RW-Coupler () used as an alternative coupling aid.
Figure 1. Round window (RW)-Coupler. The RW-Coupler was provided by MED-EL Co.
Case report
The patient was a 68-year-old woman who was diagnosed with bilateral mixed severe hearing loss due to chronic otitis media (right ear, postoperative cholesteatoma plus tympanosclerosis; left ear, tympanosclerosis). She had undergone a tympanoplasty for the right cholesteatoma at the age of 55 years. She had worn a hearing aid on her left ear since she was 57. Revision surgery for cholesteatoma recurrence was conducted at Shinshu University Hospital when she was 66 years old. No ear ossicles were found except for the footplate, which was fixed, and tympanosclerotic lesions were found in the tympanic cavity. Reconstruction surgery was then conducted at the age of 67 years. The ossicular chain was reconstructed using a cartilage and the mastoid cavity was obliterated, with no resulting hearing improvement. She suffered with bilateral hearing loss and was not satisfied with hearing aid usage.
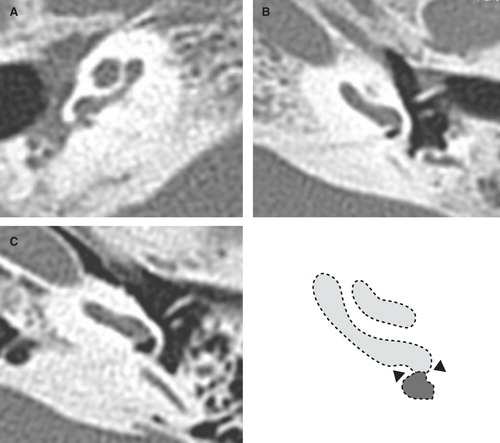
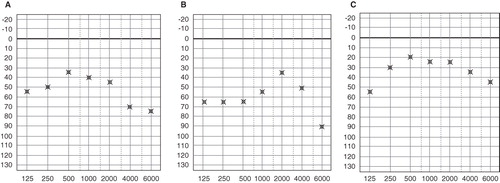
Otoscopic examination revealed an expansion of the right external auditory canal and a sclerotic lesion on her left tympanic membrane (). A pure-tone audiometric examination showed bilateral mixed hearing loss (). Average air conduction hearing loss was 73.8 dBHL in the right ear and 68.8 dBHL in the left ear. The average air–bone gap was 41.3 dB in the right ear and 36.3 dB in the left ear. Her maximum speech discrimination score with monosyllables was 55% (100 dB) in the right ear and 85% (100 dB) in the left ear. We evaluated the effect of her conventional hearing aids as follows. (1) Speech discrimination scores with and without the hearing aids. (2) Questionnaire regarding background noise with the hearing aids. (3) Warble tone threshold level with and without the hearing aids. (4) Speech discrimination scores with the hearing aids in quiet and in noise. (5) Questionnaire with and without the hearing aids. She did not pass items number 2–5, according to the guideline for adaptation tests of conventional hearing aids (2010) in Japan. Computed tomography (CT) of the temporal bone showed poor development of both mastoid cavities, sclerotic lesions in both tympanic cavities, and sclerosis in both RWs ().
Figure 2. Otoscopic findings of tympanic membrane. The right external auditory canal was expanded (A) and sclerotic lesion was found in the left tympanic membrane (B).
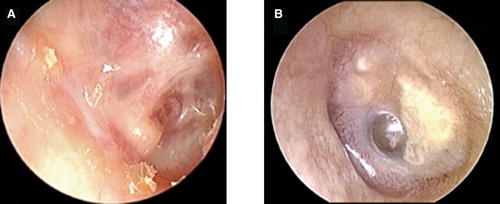
Figure 3. Pure-tone audiogram. (A) Bilateral mixed hearing loss was present. (B) Left hearing level was not changed after the VSB surgery.
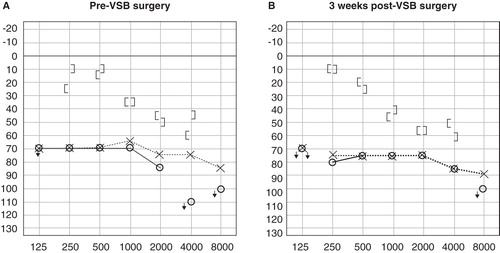
Figure 4. CT scan of region of the round window (RW) in our case. (A) Right ear, (B) left ear, and (C) control case. The RW in our case was remarkably small compared with the control case. The diameter of the RW is shown as arrowheads in the schematic representation.
We judged that it was difficult to improve the hearing loss in the patient's left ear by tympanoplasty, because her left conductive hearing impairment was also caused by tympanosclerosis, as in the right ear. The hearing aid evaluation tests revealed that the hearing aid's effect had been inadequate ( and ). The maximum speech discrimination score in the right ear was much worse than that in the left ear. We performed a RW-Vibroplasty with VSB in her left ear.
Table I. Outcomes of audiological tests in open field.
Figure 5. Warble tone threshold level. Compared with the threshold level of the conventional hearing aid (A), the threshold level of the VSB at the first fitting was improved at the high frequencies (B). After refitting, amplification at the low frequencies was elevated (C).
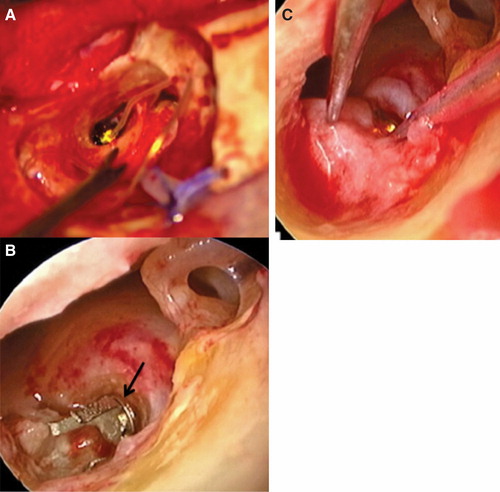
The surgical procedure consisted of a VSB implantation using a retroauricular approach. We found sclerotic lesions in the middle ear cavity and the RW and fixation of the stapes. The bony lip of the RW was drilled down until the RW membrane could be seen. However, drilling down the bony lip until the FMT could be placed completely on the RW membrane meant that a perilymphatic fistula might possibly be induced because of injury to the RW membrane. Therefore, to prevent the occurrence of a fistula, we decided to use the RW-Coupler, which is designed to fit smaller RW diameters, and were able to confirm good coupling (). Perichondrium was placed in contact with the RW membrane, with the FMT interposed and wrapped with the perichondrium.
Figure 6. Floating mass transducer (FMT) with round window (RW)-Coupler placement in the RW. The FMT attached with RW-Coupler was placed in the RW (A) after good fitting of the RW-Coupler (arrow) was confirmed (B). The FMT was wrapped in perichondrium (C).
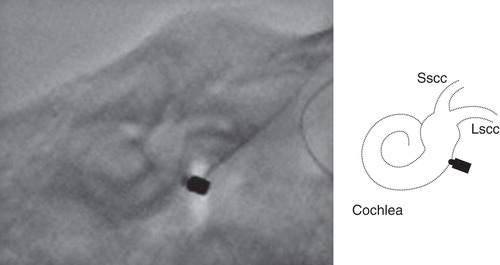
Fitting of the VSB's audio processor (Amadė®) was performed at 2 months following implantation. Warble tone threshold level at the first fitting according to the postoperative audiogram () showed that functional gain at low frequencies (0.25–1 kHz) was low (). Amplification was elevated at the low frequencies and the final threshold level was calculated in . The audiologic outcomes 3 month after VSB fitting are shown in . The evaluation tests consisted of the following. (1) Speech discrimination test for monosyllables at 60, 70, and 80 dBSPL. (2) Questionnaire for environmental noise (sentences 65 dBSPL and noise 60 dBSPL in the following conditions: a train station platform, a major intersection, a rub sound with a plastic bag, the sound of dishes being washed). (3) Speech discrimination tests for monosyllables in noise (noise at 60 dBSPL and monosyllables at S/N + 0, 5, 10 dB). Speech and noise signals were delivered by two speakers frontally placed at a distance of 1 m from the center of the subject's head. Speech discrimination scores in quiet and noise and functional gain with the VSB were better than those with the conventional hearing aid. Good placement of the FMT with RW-Coupler at the RW was confirmed 3 months after implantation ().
Figure 7. X-P finding of floating mass transducer (FMT) placement after VSB surgery. Good placement of the FMT with the round window (RW)-Coupler was confirmed. Scheme of X-P is shown. Lscc, lateral semicircular canal; Sscc, superior semicircular canal.
This study was approved by the Ethics Committee of Shinshu University School of Medicine and written consent was obtained from the patient.
Discussion
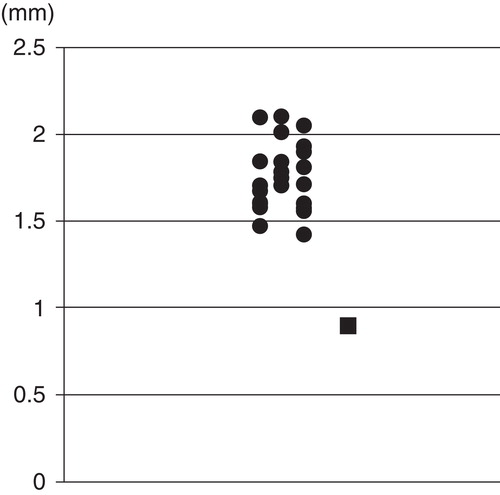
The rate of tympanosclerosis is reported to be 9–38% in chronic otitis media cases, with bilateral tympanosclerosis seen in about 50% of the patients [Citation3]. Tympanosclerotic plaques are found in the attic and around the stapes, oval window, RW, and promontorium [Citation3]. The second most common site for sclerosis occurrence is the RW region, which is involved in 30% of clinical cases in histologic studies [Citation4]. In radiologic studies, the prevalence of sclerosis in the RW is 3.2–13% [Citation4]. Half of the patients with tympanosclerosis have required second sessions or revision procedures if ossicle fixation was present [Citation5]. The present case involved bilateral mixed hearing loss and sclerotic lesions in both middle ears, which does not seem to be very rare. shows the diameters of the left RW membrane in our case and in 24 patients with sensorineural hearing loss as controls by radiologic evaluation of CT scan, which was measured on the inferior edge of the RW (arrowheads in the diagram in ) in the transverse slice. The diameter of the left RW in our case (0.9 mm) was remarkably small compared with control cases (1.78 mm on average) because of sclerosis of the inferior edge of the RW. An air–bone gap of 41.3 dB was found, which tympanoplasty in the right ear was unable to improve. We therefore decided that it would also be difficult to improve the hearing loss by tympanoplasty in the left ear. The maximum speech discrimination score in the right ear was much worse than that in the left ear. We decided to perform the RW-Vibroplasty in the left ear.
Figure 8. Diameter of the round window (RW) by radiologic evaluation of CT scan. The diameter was measured on the inferior edge of the RW in the transverse slice in the left ear. This case (black square) was remarkably small compared with control cases (black circles). Patients with sensorineural hearing loss were measured as control cases.
The VSB was developed as an active middle ear implant to transmit vibration into the inner ear. It was originally coupled to the long process of the incus in patients with a sensorineural hearing loss and an intact ossicular chain. Recently, application of the middle ear implant has become an efficient procedure to restore mixed hearing loss in selected patients [Citation2]. In these cases, the attachment point of the VSB's FMT has been modified. Different authors have described various modifications, including coupling the FMT to the stapes suprastructure, a total ossicular replacement prosthesis (TORP), a partial ossicular replacement prosthesis (PORP), the oval window membrane, and the RW membrane [Citation6-10]. In tympanosclerosis including sclerosis in the oval and round windows with mixed hearing loss, stapes surgery allows one to restore the conductive part of the hearing. However, air–bone gap closure does not systemically improve the auditory threshold enough to avoid use of conventional hearing aids. We considered the present case with mixed hearing loss induced by tympanosclerosis to have an indication for VSB, because the patient was unable to use a conventional hearing aid. We considered that an attachment technique of the FMT to a PORP or the RW membrane could be selected in the present case, because other attachment techniques require a mobile stapes footplate. However, there is no permission to use a PORP in Japan. Therefore, we had concluded that placing the FMT at the RW would improve the mixed hearing loss in the present patient with tympanosclerosis.
The attachment of the FMT on the RW was first described by Colletti et al. [Citation2] and is now becoming more frequently used because of its effectiveness and wide range of applications in difficult to treat otologic cases. Clinical data reported by Rajan et al. [Citation11] showed that either partial or complete direct contact of the FMT with the RW membrane increases relative coupling efficiency between the FMT and the RW membrane. The experimental findings in the cadaveric human temporal bone supported the assertion that no acoustic response was measured when the FMT was placed onto the promontory [Citation12]. The postoperative migration of the FMT seems to occur within the first 6 months after surgery [Citation11]. The obliteration of any dead space around the FMT minimizes the chance of FMT migration. Wrapping the FMT with the perichondrium has helped to prevent the migration. It is sometimes not possible to achieve FMT–RW membrane contact because of the depth of the RW niche and the mismatch between the diameter of the FMT and that of the RW membrane. Especially in cases of sclerosis in the RW, the sclerotic lesion should be drilled out to put the FMT in contact with RW membrane, but by so doing, the possibility of inducing a perilymphatic fistula increases. To make sure the FMT contacts the RW membrane while reducing the possibility of perilymphatic fistula, soft tissue such as fascia or perichondrium [Citation7] and cartilage [Citation11] as well as the RW-Coupler can be placed as a coupler between the FMT and RW membrane. However, soft tissue couplers seem to reduce the relative coupling efficiency when compared with direct placement of the FMT onto the RW membrane [Citation11]. Recently, the RW-Coupler has been used as an alternative coupling aid to fit smaller RW diameters and incur less drilling in the RW niche. It is unclear how the RW-Coupler will affect the outcomes, and the present case may be the first report to show these clinical results. Direct coupling with the RW membrane would be expected to achieve complete closure of the air–bone gap, but a large fraction of the gain is required to overcome the soft tissue-related reduction of coupling efficiency [Citation13,14]. In the present case, the perichondrium was placed between the RW membrane and the RW-Coupler attached to the FMT. The functional gain at low frequencies (0.25–1 kHz) after the first fitting according to the postoperative audiogram was less than the predicted ideal acoustic gain. Good functional gain was found at high frequencies compared with conventional hearing aids. Therefore, we increased the gain offered by the audio processor at low frequencies, resulting in good speech discrimination scores. Beltrame et al. [Citation13] described functional gain in VSB patients with a fixed stapes to be smaller than that in other patients. Consequently, the RW-Coupler has been available for patients with tympanosclerosis involving sclerosis in the RW, and more amplification from the VSB audio processor at low frequencies might be required to provide enough functional gain.
Acknowledgments
We thank Prof. Mueller Joachim for supporting the VSB surgery.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Luetje CM, Brackman D, Balkany TJ, Maw J, Baker RS, Kelsall D, Phase III clinical trial results with the Vibrant Soundbridge implantable middle ear hearing device: a prospective controlled multicenter study. Otolaryngol Head Neck Surg 2002;126:97–107.
- Colletti V, Soli SD, Carner M, Colletti L. Treatment of mixed hearing losses via implantation of a vibratory transducer on the round window. Int J Audiol 2006;45:600–8.
- Aslan H, Katilmis H, Öztürkcan S, İlknur AE, Başoğlu S. Tympanosclerosis and our surgical results. Eur Arch Otorhinolaryngol 2010;267:673–7.
- Mansour S, Nicolas K, Ahmad HH. Round window otosclerosis: radiologic classification and clinical correlations. Otol Neurotol 2011;32:384–92.
- Teufert KB, De la Cruz A. Tympanosclerosis: long term hearing results after ossicular reconstruction. Otolaryngol Head Neck Surg 2002;126:264–72.
- Venail F, Lavieille JP, Meller R, Deveze A, Tardivet L, Magnan J. New perspectives for middle ear implants: first results in otosclerosis with mixed hearing loss. Laryngoscope 2007;117:552–5.
- Mlynski R, Mueller J, Hagen R. Surgical approaches to position the Vibrant Soundbridge in conductive and mixed hearing loss. Oper Tech Otolaryngol 2010;21:272–7.
- Zehlicke T, Dahl R, Just T, Pau HW. Vibroplasty involving direct coupling of the floating mass transducer to the oval window niche. J Laryngol Otol 2010;124:716–19.
- Service GJ, Roberson JB. Alternative placement of the floating mass transducer in implanting the MED-EL Vibrant Soundbridge. Oper Tech Otolaryngol 2010;21:194–6.
- Shimizu Y, Puria S, Goode RL. The floating mass transducer on the round window versus attachment to an ossicular replacement prosthesis. Otol Neurotol 2010;32:98–103.
- Rajan GP, Lampacher P, Ambett R, Dittrich G, Kuthubutheen J, Wood B, Impact of floating mass transducer coupling and positioning in round window vibroplasty. Otol Neurotol 2011;32:271–7.
- Arnold A, Kompis M, Candreia C, Pfiffner F, Häusler R, Stieger C. The floating mass transducer at the round window: direct transmission or bone conduction? Hear Res 2010;263:120–7.
- Beltrame AM, Martini A, Prosser S, Giarbini N, Streitberger C. Coupling the Vibrant Soundbridge to cochlea round window: auditory results with mixed hearing loss. Otol Neurotol 2009;30:194–201.
- Nakajima HH, Dong W, Olson ES, Rosowski JJ, Ravicz M, Merchant SN. Evaluation of round window stimulation using the floating mass transducer by intracochlear sound pressure measurements in human temporal bones. Otol Neurotol 2010;31:506–11.