
We read with interest the case report by Li et al. (Citation2013), describing a case of spontaneous splenic rupture in ectopic pregnancy. We would like to add our experience of spontaneous splenic rupture occurring in 3rd trimester of pregnancy, wherein another acute presentation was in the form of a massive haemoperitoneum.
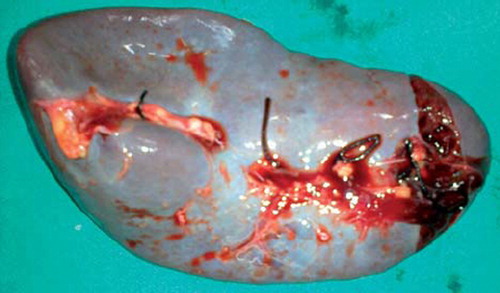
A 26-year-old multigravida, at 8 months’ gestation, presented with sudden onset pain in the abdomen, breathlessness and loss of fetal movements. There was a history of five sudden episodes of vomiting prior to her presentation. However, there was no history of bleeding or leaking per vaginum. She had no bladder or bowel complaints. There was no evidence of trauma and her past history was unremarkable. Examination revealed severe pallor with signs of hypovolaemic shock. The abdomen was grossly distended with a positive fluid thrill. The uterine contour could not be made out and fetal heart sounds were absent. Emergency laparotomy was done with a provisional diagnosis of uterine rupture. Peroperatively, two litres of haemoperitoneum were present; the uterus was intact and a pre-term stillborn fetus was delivered by lower segment caesarean section. Abdominal exploration revealed a 6 cm laceration on the lower pole of the ventral surface of the spleen, which was bleeding actively (). The spleen was otherwise grossly normal in morphology and size. A total splenectomy was performed. The patient made an uneventful recovery. Histopathology reported a normal spleen with congestion and haemorrhage.
Figure 1. Lacerated spleen with haemorrhages.
In the 3rd trimester, the most important causes of acute massive haemoperitoneum are antepartum haemorrhage, uterine rupture and less commonly, endometriosis, splenic and renal artery aneurysm rupture. They have a high maternal and fetal mortality rate (Grunewald and Jördens Citation2010). Spontaneous splenic rupture, being rare, is often not suspected and the diagnosis is made during laparotomy. In the absence of other findings, as mentioned by Li et al. (Citation2013), spontaneous rupture appears as the most probable aetiology in our case. An episode of excessive vomiting might be a possible cause (Sakhel et al. Citation2003).
The treatment of choice depends on the grade of splenic rupture, haemodynamic instability and availability of endovascular treatment. Splenectomy remains the treatment of choice in patients with severe hypovolaemic shock. Other options are splenic repair, tamponade using an absorbable mesh or transcatheter arterial embolisation. These two reports create awareness regarding a differential diagnosis, while dealing with acute massive haemoperitoneum in pregnancy.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Grunewald C, Jördens A. 2010. Intra-abdominal hemorrhage due to previously unknown endometriosis in the third trimester of pregnancy with uneventful neonatal outcome: a case report. European Journal of Obstetrics, Gynecology, and Reproductive Biology 148:204–205.
- Li W, Yin D, Huo NC, et al. 2013. A case of spontaneous splenic rupture in an ectopic pregnancy. Journal of Obstetrics and Gynaecology 33:93–94.
- Sakhel K, Aswad N, Usta I, et al. 2003. Postpartum splenic rupture. Obstetrics and Gynecology 102:1207–1210.