Abstract
Background. In modern radiotherapy accelerators are equipped with 3D cone-beam CT (CBCT) which is used to verify patient position before treatment. The verification is based on an image registration between the CBCT acquired just before treatment and the CT scan made for the treatment planning. The purpose of this study is to minimise the scan time of the CBCT without compromising the accuracy of the image registration in IGRT. Material and methods. Fast scans were simulated by reducing the number of acquired projection images, i.e. new reconstructions based on a subset of the original projections were made. The deviation between the registrations of these new reconstructions and the original registration was measured as function of the amount of reduction. Results and Discussion. Twenty nine head and neck (H&N) and 11 stereotactic lung patients were included in the study. The mean of the registration deviation did not differ significantly from zero independently of the number of projections included in the reconstruction. Except for the smallest subset of reconstructions (10% and 25% of the original projection for the lung and H&N patients, respectively) the standard deviation of the registration differences was constant. The standard deviations were approximately 0.1 mm and 0.2 mm for the H&N and lung group, respectively. Based on these results an in-house developed solution, able to reduce the Cone-Beam CT scan time, has been implemented clinically.
In modern radiotherapy the patient is scanned in the accelerator using CBCT before treatment to verify the position of the patient [Citation1–4]. The CBCT is compared with the therapy planning CT, and the displacement is calculated using rigid image registration, which can be used to correct the patient position before treatment.
At an Elekta accelerator the images are acquired at a constant frequency (∼ 5 s–1) as the gantry rotates continuously with no pause during acquisition. The standard rotation speed during a CBCT scan is only half of the speed used clinically when the gantry is changing position from one treatment field to another. All utilised software and hardware are the latest released from the vendor, thus currently image acquisition time is mainly limited by the speed of the gantry rotation. A full standard 360° CBCT consists of approximately 630 projections and takes about 130 seconds to acquire. The dose to the patient during such a scan is ∼ 2 cGy [Citation5], measured with PTW T40016 body phantom in 1 cm depth (AAPM TG66). Due to the constant frequency of image acquisition, an increase of the rotation speed would result in less projection images but also decrease the acquisition and reconstruction time. If the rotation speed can be doubled, the acquisition time can be reduced by one minute, which is to be compared to standard treatment slots of 10–15 minutes. Thus, for institutions using daily CBCT for all patients, the increased rotation speed could potentially increase the patient throughput by 5–10% which can be important [Citation6]. As an added benefit the less number of projection images reduces the imaging dose to the patient.
Reducing the number of projections will evidently have an impact on the image quality of the reconstruction [Citation7]. The question is; how much it is possible to reduce the number of projections in a CBCT while still maintaining the precision of the image registration?
Material and methods
In this study the X-ray Volume Imaging (XVI) software v.3.5 (Elekta SynergyTM, Elekta Oncology Systems Ltd., Crawley, West Sussex, United Kingdom) is used for reconstruction of the CBCT and image registration on an Elekta Synergy accelerator.
All patients were scanned according to standard clinical procedure as listed in . The registration from the clinical scan was used as the reference – the golden standard. XVI provides a feature to select which projections to include in the reconstruction. This feature was utilised to activate only a subset of the projections to simulate a fast scan with less projections.
Table I. Settings for the CBCT scan.
Fast scans were created which included 90%, 75%, 50%, 33%, 25%, and 10% of the original projections. The excluded projections were evenly distributed over the initial set of projections.
The CBCTs were reconstructed using the High Resolution preset. XVI provides two algorithms for image registration; one based on bone density values and the other on all density values (named grey values) [Citation8]. Only the grey value algorithm was used in this study as this is the standard clinical procedure in our institution. Image registration in XVI is based on selected volumes of interest (VOI), called clip-boxes, defining the region used for registration of the two image sets. All clipboxes were also made according to a local protocol. The edges of the clipbox are defined in .
Table II. Definition of edges of the clipbox used for the image registration.
The registrations made on the fast scans were compared to the result obtained from the full standard scan (golden standard), and the difference in translation displacement between the two registrations is denoted ΔT Thus, this study does not focus on whether the registration is correct but only on the reproducibility as the number of projections is reduced.
The standard deviations of the rotations are typically 1° [Citation4,Citation9]. A rotation of 1° has limited impact on a target located close to the isocenter. Furthermore, only few treatment couches supports rotational corrections, thus in this IGRT study only the translational displacement is included.
This study includes 29 H&N patients and 11 stereotactic non-small cell lung cancer (NSCLC) patients. All patients had a body mass index (BMI) below 30.
Results
Due to the low number of projections in the original H&N data, XVI was not able to reconstruct the CBCT based on only 10% of the projections. shows the sagital plan of the reconstructions, as the number of projections is reduced to 25% for the H&N patients and 10% for the lung patients. Visually only a vague change in the image quality is seen when the number of projections is reduced to 50%. Reconstructions for the 90% and 75% cases are very similar to the original reconstruction and are therefore omitted in the figure. As the number of projections is reduced to 25% of the original data artefacts become more visible.
Figure 1. The visual differences when reducing the number of projections. Slices from the reconstruction using 90% and 75% are omitted because of the very little visual changes. There were too few projection images to reconstruct the CBCT in the 10% case for the H&N patients.
The average and the standard deviation of ΔT in the three spatial directions are shown in . It is seen that the average error and the standard deviations (STD) are small. The standard deviation shown in is almost constant (∼0.1 mm and ∼0.2 mm for the H&N and lung patients, respectively). However, there might be an indication of an increased STD for the fast scan based on the lowest number of projections (25% and 10%).
Figure 2. The components of ΔT for the lung and H&N patients. The average translation in each direction left-right (LR), anterior-posterior (AP) and cranio-caudal (CC) are marked with the asterisk symbol, and the error bars shows ± 1 standard deviation.
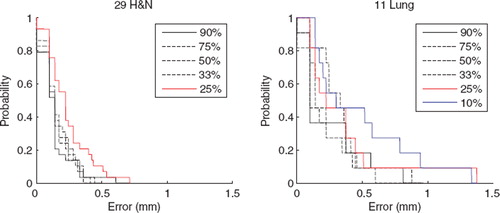
The euclidean length of the deviation between the registrations of the fast scan and the original registration is visualised in , which shows the probability of having translational errors above a certain level. For example, it is seen in that for the lung patients using only 10% of the original projections, the probability of having a translational difference of more than 0.5 mm is about 45%. As can be seen in no differences larger than 0.7 mm for the H&N group were observed. Likewise, in the lung group except for two measurements of about 1.4 mm the rest were below 0.9 mm.
Figure 3. Probability histogram showing the probability of having a translational error of length larger than a given length. It is seen that no deviation larger than 0.7 mm is seen in the H&N group. Likewise, it is seen for the lung group that there is a small probability of deviations above 1 mm, however deviation above 1.4 mm is not observed in any of the reduced data sets.
The clinically measured scan time for a full standard CBCT used for the lung patients takes ∼130 seconds. For the double rotation speed this is reduced to ∼70 seconds. Only a few seconds pass to complete the reconstruction after the acquisition in both cases. For the H&N patients it takes ∼80 seconds and is reduced to ∼44 seconds for the double rotation speed.
Discussion
The almost constant STD displayed in shows that the STD is mainly defined by the intrinsic uncertainty of the XVI system for the selected patient group and only to a lesser extent by the number of projection images.
It should be noticed that the largest deviation found in this study was 1.4 mm which is small compared to clinical acceptance level of 3–5 mm, typically. The small indication of the increasing uncertainty in for data reduced to 10% (lung) and 25% (H&N) is more evident in . It is especially seen that the 10% line for the lung patients deviates from the others. Although not as pronounced, this also seems to be the case for the 25% reduced data for the H&N. Thus at these levels of reductions the uncertainty is no longer defined only by the intrinsic uncertainty of the XVI system but also by the number of projections.
The most noticeable disadvantage of reducing the number of projections is the reduction of the visual image quality, which can be a disadvantage in the validation of the automatic registration. It could also be a problem in those seldom cases where the registration has to be performed manually. All registrations in this study were performed automatically – no manual registration was needed. X-ray images of obese patients can result in reduced image quality because of the attenuation of the x-rays in the extra tissue. The lack of contrast in soft tissue regions in a CBCT can make it difficult to perform registrations of such regions. In these cases a reduced scan might not be an optimal choice.
Based on the above mentioned advantages and disadvantages we have decided to increase the rotation speed of the CBCT scan by a factor of two. Change of the scan speed is not a commercially available feature in the XVI system, but it can be achieved by a relatively simple hardware modification on the Elekta accelerator. Our current in-house developed solution makes it possible to change the rotation speed on a switch in the control room. Having used the increased speed for almost half a year, no complaints about image quality has been reported by the treatment technicians, but they are fully satisfied about the reduced amount of time spent on the individual CBCT.
The time saved can be used to increase the treatment quality or patient throughput. In our institution it has enabled us to increase the number of CBCT scans during the treatment course and thereby obtaining a better validation of the patient positioning.
The study shows that it is possible to increase the scan speed by almost another factor of two without increasing the uncertainty of the registration. For the safety of the patient the gantry should be able to stop within 3° in case of collision. Thus due to the patient safety and the even further reduced visual quality of the images, no attempt has been made to increase the scan speed further at this stage.
The results in this study are also of interest for 4D-CBCT. 4D-CBCT is a time resolved version of standard CBCT, which can be used to image the patient as function of respiration phase. In 4D-CBCT a standard CBCT is divided in 10 respiration phases, and each of them are reconstructed containing only one tenth of the projection images, and finally composed to a 4D-CBCT. If the speed of the gantry is not reduced the projection for each respiration phase corresponds to the 10% case in this study. Thus this study shows that the uncertainty of a registration in a 4D-CBCT scan, is only slightly larger than the registration uncertainty in a standard 3D-CBCT.
The purpose of this study was to reduce the scan time. The decrease in dose to the patient is therefore just an added benefit. If dose to the patient was the only concern it would probably be better to reduce the x-ray current instead of reducing the number of projections in terms of registration uncertainty.
The present study is based on lung and H&N patients treated on Elekta Synergy accelerators, and the results might not be reproducible for other treatment sites or types of accelerators.
Conclusion
The reconstructions with reduced number of projections does have an impact on the visual image quality as expected, but sufficient information for accurate image registration is still preserved using only 33% of the initial number of projection images. Thus, both time and dose can quite easily be reduced by a factor of two with no significant impact on the registration, and almost no visual reduction of the image quality. A further reduction results in a noticeably decreased visual image quality, however the registration accuracy is only reduced slightly.
Changing the scan speed is not a commercially available feature in the XVI system, but it can be achieved by a relatively simple hardware modification on the Elekta accelerator.
Based on these results an in-house developed solution, able to reduce the Cone-Beam CT scan time, has been implemented clinically.
Acknowledgements
This work is supported by CIRRO – The Lundbeck Foundation Center for Interventional Research in Radiation Oncology and The Danish Council for Strategic Research (CIRRO number WP05-02-2009).
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Jaffray DA, Siewerdsen JH. Cone-beam computed tomography with a flat-panel imager: Initial performance characterization. Med Phys 2000;27:1311–23.
- Jaffray DA, Siewerdsen JH, Wong JW, Martinez AA. Flat-panel cone-beam computed tomography for image-guided radiation therapy. Int J Radiat Oncol Biol Phys 2002;53:1337–49.
- Bertelsen A, Nielsen M, Westberg J, Jensen HR, Brink C. The representitativeness of patient position during the first treatment fractions. Acta Oncol 2009;48:259–66.
- Nielsen M, Bertelsen A, Westberg J, Jensen HR, Brink C. Cone beam CT evaluation of patient set-up accuracy as a QA tool. Acta Oncol 2009;48:271–6.
- Song WY, Kamath S, Ozawa S, Ani SA, Chvetsov A, Bhandare N, . A dose comparison study between XVI and OBI CBCT systems. Med Phys 2008;35:480–6.
- Thomas SJ. Capacity and demand models for radiotherapy treatment machines. Clin Oncol (R Coll Radiol) 2003;15:353–8.
- Sonke JJ, Zijp L, Remeijer P, van Herk M. Respiratory correlated cone beam CT. Med Phys 2005;32:1176–86.
- Smitsmans MHP, Wolthaus JWH, Artignan X, de Bois J, Jaffray DA, Lebesque JV, . Automatic localization of the prostate for on-line or off-line image-guided radiotherapy. Int J Radiat Oncol Biol Phys 2004;60:623–35.
- Kaiser A, Schultheiss TE, Wong JYC, Smith DD, Han C, Vora NL, . Pitch, roll, and yaw variations in patient positioning. Int J Radiat Oncol Biol Phys 2006;66:949–55.