Abstract
Purpose. To examine cancer patients’ needs for rehabilitation services and factors associated with such needs, and secondly identify unmet needs for rehabilitation services and related factors. Material and methods. In 2008 persons aged 25–60 years, diagnosed in 2005/2006 with the ten most prevalent cancers in Norway were identified through the Cancer Registry of Norway. These patients were contacted by their treating hospital receiving a mailed questionnaire. Main outcomes for the present study were measured by two questions assessing a) needs for rehabilitation services and b) rehabilitation services offered/used. For each question seven services were listed; physical therapy, physical training, psychological counseling, consultations with social worker, occupational therapy, supportive group sessions and admittance to a convalescent home. The respondents then rated to what extent they had experienced needs and if they had been offered and used each service. Those who reported need for a service that not had been offered were defined as having unmet need. Associations between demographic, health-related and outcome variables were analyzed by multivariate logistic and linear regression analyses. Results. Among the 1 325 respondents, the mean age was 52 years and 70% were women. Sixty-three percent reported need for at least one rehabilitation service. Need for physical therapy was most frequently reported (43%), followed by physical training (34%), psychological counseling (27%), supportive group sessions (24%), admittance to a convalescent home (24%), consultation with social worker (19%) and occupational therapy (6%). Changes in employment status and ongoing or previous chemotherapy were associated with reporting needs for all rehabilitation services. Forty percent reported unmet needs, which most frequently was reported among persons living alone, who had changed their employment status, receiving or had received chemotherapy or reported comorbidities. Conclusions. The majority reported need for at least one rehabilitation service, and 40% reported unmet needs. Prospective studies are recommended in order to better understand needs for rehabilitation services, such as needs in relation to time since treatment, extent of disease and treatment intensity.
The number of cancer survivors in the Western world has been steadily increasing during the last decades. Estimates from The Association of the Nordic Cancer Registries show that currently about 900 000 persons previously diagnosed with cancer are alive in the Nordic countries [Citation1]. Approximately 65% of cancer patients live for more than five years after diagnosis [Citation2]. However, cancer treatment, i.e. chemotherapy, radiotherapy, hormone therapy and surgery, alone or in combinations, are accompanied by adverse health effects, which may lead to impaired physical and/or psychosocial functioning [Citation3–6]. All these factors point to an increasing need for rehabilitation after cancer treatment.
The World Health Organization (WHO) has defined rehabilitation as: ‘processes intended to enable people with disabilities to reach and maintain optimal physical, sensory, intellectual, psychological and/or social function’ [Citation7]. Rehabilitation encompasses a wide range of services including rehabilitative medical care, physical, psychological, and occupational therapies and support services.
From the perspective of the health care system, needs for specific rehabilitation services are of relevance in relation to service development, costs and resource allocation. Due to the variability of impaired function after cancer treatment, cancer survivors may be in need of different rehabilitation services at different times and of different complexity in order to (re)gain as optimal function as possible. Some cancer patients will need professional assistance for a specific problem which can be delivered by one type of health care professional such as physical therapy for lymphedema (single rehabilitation). Other patients will need multiple rehabilitation services including assistance from different health care professionals such as physical therapists, social workers and psychologists (complex rehabilitation).
Among the different elements within cancer rehabilitation the need for physical activity counseling has been explored rather extensively with studies showing that 75–85% of cancer patients are interested in such counseling [Citation8–10]. In a study investigating need for psychosocial support, 19% of cancer survivors (n = 351) reported unmet needs for this kind of service 22 months (mean) after time of diagnosis, but only 10% were actually using psychosocial services [Citation11]. As far as we know, no studies have examined the needs for complex rehabilitation and factors associated with such need.
Needs for rehabilitation services may vary with cancer diagnosis, because different treatment modalities and intensities might lead to different physical and psychological impairments. We believe, for example, that breast cancer patients more often than patients with other diagnoses will report need for physical therapy due to limitations in arm mobility and lymphedema. Intensive cancer treatment can increase the need for complex rehabilitation, due to the high prevalence of multiple late effects after such treatment. Reduced somatic health, due to comorbidities might also increase the need for rehabilitation services beyond the need emerging as a result of the cancer and its treatment per se. Socio-demographic factors such as education level, increasing age and living alone might also increase the need for one or more rehabilitation services. Still, we lack systematic data on how these factors influence the patients’ self-reported needs for rehabilitation services.
This cross-sectional study was therefore launched with the primary aim to assess the needs for rehabilitation services among cancer survivors and to explore factors associated with these needs. Secondary aims were to estimate the need for complex rehabilitation and factors associated with such need and finally to assess unmet needs for rehabilitation services and explore factors associated with these unmet needs.
Patients and methods
Patients and study design
Patients included in this cross-sectional survey participated in an extensive investigation of cancer patients’ work- and economic situation [Citation12]. Eligible patients were identified through the Cancer Registry of Norway (CRN) in 2008. The inclusion criteria were cancer patients aged 25–60 years, diagnosed for the first time in 2005/2006 with one of the ten most frequent types of cancer within each gender in Norway (breast-, prostate-, colorectal/anal-, cervix/corpus-, uteri/ovarian-, lung- and testicular cancer, melanoma, non-Hodgkin lymphoma, leukemia, tumor in bladder/urethra, nerve system and thyroid) and having current address in Norway. Active disease or currently receiving cancer treatment was not exclusion criteria. To ensure geographical representativeness, the patients should have had their initial treatment at one of four hospitals located in different health regions of the country. After identification at the CRN, each hospital received a list of patients who had been treated at that particular hospital. Patients were excluded if one or more of the following criteria were present: 1) being unaware of having a cancer diagnosis, 2) being in such a medical condition that it was considered unethical to ask the patients to complete the questionnaire (i.e. very advanced or terminal disease), 3) mental retardation, reduced cognitive function or a diagnosis of major psychiatric disorder. The eligible patients received a questionnaire together with the invitation letter. By returning the questionnaire the patient agreed to participate. All answers were anonymous and reminders were therefore not sent.
Outcome variables
The outcome variables for the present study were the items covering needs for rehabilitation services and rehabilitation services offered/used. These variables were assessed by two questions:
To what extent have you experienced need for the following rehabilitation services in relation to your cancer?
To what extent have you been offered and used the following rehabilitation services in relation to your cancer?
Under each question the following seven rehabilitation services were listed; physical therapy, physical training, psychological counseling, consultation with social worker, occupational therapy, supportive group sessions and admittance to a convalescent home.
When responding to question 1 (needs for services) the respondent was asked to rate his/her need for each rehabilitation service on a 3-point verbal rating scale (“No need”, “Some need” and “Large need”). The responses were subsequently dichotomized into “no need” and “need” (the latter combining “some need” and “large need”) in the analyses of variables associated with the need for each rehabilitation service. To explore the need for complex rehabilitation (more than one service needed), a variable was constructed by adding the number of rehabilitation services the responders reported need for (response range: 0–7, continuous variable). Thus, a higher number represented need for more complex rehabilitation.
The response alternatives to question 2 (services offered/used) included four alternatives for each service (“Have not been offered this program”, “Have been offered this program but did not use it”, “Have been offered and used to little extent” and “Have been offered and used to large extent”).
A participant was categorized as having unmet need, if he/she reported need for a specific rehabilitation service (question 1), but was not offered this service (question 2). This categorization was done for all seven rehabilitation services separately. The number of services unmet was summarized (response: 1–7 unmet needs).
The outcome variables are not validated, however pilot-tested for clarity and understandability and subsequently adjusted.
Explanatory variables
Self-reported demographic explanatory variables included gender, age, living with a partner or not, children below 18 years living at home or not, level of education, employment status, changes in employment status due to cancer and health-region.
All cancer-related explanatory variables were also self-reported and included months since diagnosis, type of cancer diagnosis [breast-, prostate-, colorectal/anal-, cervix/corpus-, uteri/ovarian cancer, melanoma, non-Hodgkin lymphoma, other cancer sites (defined as diagnostic groups reported by n<50 or if the responders reported more than one cancer diagnosis)]. Other explanatory variables included recurrence, being under current treatment and type of treatment received. All categories of the explanatory variables are shown in .
Table I. Demographic and medical characteristics, number of needs and unmet needs.
Non-cancer health-related explanatory variables were also self-reported and included comorbidities (defined as presence of at least one of the following medical conditions: cardiovascular- or respiratory disease, psychological disorders, thyroid dysfunction, trauma or neurological disorders) and general health (very good, quite good, neither good or bad, quite bad or very bad).
Statistical analyses
Logistic regression analyses were used to explore the associations between the need for each rehabilitation service separately and demographic and medical explanatory variables. Explanatory variables statistically significantly associated with the dependent variable in the univariate analyses were included as explanatory variables in the multivariate analyses. Explanatory variables not statistically significantly associated with the dependent variable in the multivariate logistic regression model were subsequently excluded step by step until the model included statistically significantly variables only. The same procedure was used to explore the association between unmet needs for rehabilitation services and demographic and medical explanatory variables. Univariate and multivariate linear regression analyses were performed to explore factors associated with need for increasing number of services (complex rehabilitation) (response range: 0–7 services) controlled for self-reported demographic, cancer related and non-cancer health-related explanatory variables. As in the multivariate logistic regression model, the multivariate linear model was reduced to include statistically significant variables only. Gender was not included as an explanatory variable in any of the analyses because several of the diagnoses were gender specific, which made it difficult to separate diagnosis and gender in the overall analyses. The data set included also patients with missing data on one or more items. Therefore, due to missing data for the explanatory variables the numbers of patients vary in the statistical analyses. All tests were two-sided and p< 0.05 was considered statistically significant. Adjusted odds ratios (aOR) are presented with 95% Confidence Intervals (95% CI). All analyses were performed using SPSS 16.
Ethics
The Data inspectorate and the Regional committee for ethics, Health region south-east, Norway, approved the study.
Results
Attrition
The CRN identified 2 848 eligible patients. From this cohort, 346 were excluded according to the exclusion criteria. The questionnaire was thus sent to 2 502 patients. Twenty-nine questionnaires were returned due to invalid address and seven were returned because of death or by individuals reporting not to have had cancer. From the remaining 2 466 eligible patients 1 325 completed questionnaires were returned, yielding a response rate of 54%. Demographic and medical characteristics of the participants are presented in .
Need for rehabilitation services
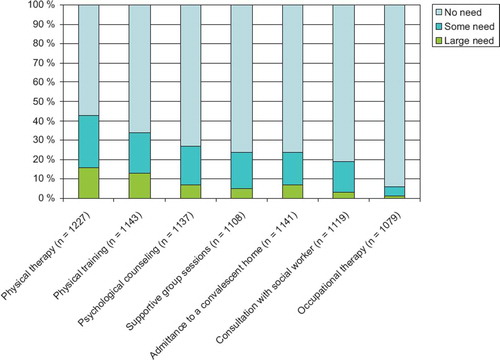
Overall, 37% reported no need for any rehabilitation services, whereas 63% reported need for at least one rehabilitation service (). Need for physical therapy was reported most frequently (43%), followed by physical training (34%), psychological counseling (27%), supportive group sessions (24%), admittance to a convalescent home (24%), consultation with social worker (19%) and occupational therapy (6%) ().
Figure 1. Proportions of cancer patients reporting need for seven rehabilitation services.
Factors associated with need for rehabilitation services
Estimates from the multivariate logistic regression analysis are shown in . Patients who changed their employment status due to the cancer diagnosis, and those who had received chemotherapy (with or without radiotherapy and/or other treatment modalities) were more likely to report need for all rehabilitation services than those who did not change their employment status and those who had not received chemotherapy.
Table II. Factors associated with need for each rehabilitation service in multivariate logistic regression analyses.
Higher age and living with a partner were negatively associated with needs for some types of rehabilitation services. For example, need for psychological counseling, consultation with a social worker and admittance to a convalescent home decreased by increasing age. Those living with a partner were less likely to need physical training, psychological counselling, consultation with a social worker, occupational therapy or admittance to a convalescent home than those living alone.
Need for physical training was higher among patients with children below 18 years living at home. Those with high educational level (university/college) were more likely to report need for physical training, psychological counseling, supportive group sessions or admittance to a convalescent home than those with a low educational level. Patients not working or studying more frequently reported need for psychological counseling, consultation with a social worker and admittance to a convalescent home than those working or studying.
Breast cancer patients were more likely to report need for physical therapy and supportive group sessions than patients with other diagnoses. Compared to breast cancer patients those with melanoma reported less often need for physical training and admittance to a convalescent home. Patients who had experienced recurrence were more likely to need physical therapy compared to those who had not experienced recurrence. The need for consultation with a social worker was more frequently reported among those patients currently receiving cancer treatment as compared to those who had completed treatment.
Need for complex rehabilitation and associated factors
Forty percent of the patients needed two or more rehabilitation services (complex rehabilitation) (). On average each patient reported need of 1.58 rehabilitation services [median 1.0, (range 0–7) data not shown]. Variables associated with need of complex rehabilitation are shown in . Factors that remained significantly associated with need for complex rehabilitation in the multivariate analysis were young age, living alone, high education, not working, changes in employment status due to the cancer diagnosis, presence of comorbidities, having breast cancer and treatment with chemotherapy and radiotherapy together with or without other treatment modalities.
Table III. Factors associated with increasing need for rehabilitation (complex rehabilitation) (range 0–7).
Unmet need for rehabilitation and associated factors
Among all patients, 40% reported unmet needs (), 20% reported to have one unmet need, 10% reported to have two unmet needs, whereas only 1% reported to have seven unmet needs (). Nine percent of all patients were not offered physical therapy even though they reported to need this service, whereas 22% of those in need of physical training and 17% of those in need of psychological counseling were not offered these services ().
Figure 2. Rehabilitation services – needed and offered.
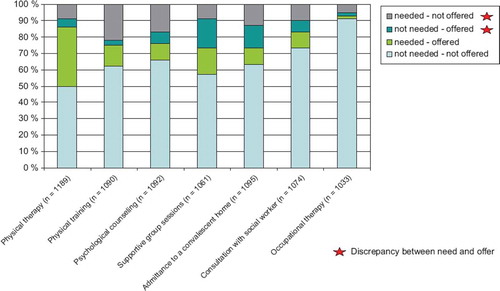
Table IV. Factors associated with unmet need for rehabilitation.
Those living alone, those who had changed their employment status due to cancer diagnosis or those having comorbidities were more likely to report unmet needs for rehabilitation. Compared to those receiving chemotherapy and radiotherapy together with or without other treatment modalities, those not receiving chemotherapy were less likely to report unmet need for rehabilitation ().
Discussion
The majority of the cancer patients in the present study reported need for at least one rehabilitation service and two thirds of the patients that needed rehabilitation services reported needs for two or more services. By far, physical therapy was most frequently needed among the seven rehabilitation services studied. Changes in employment status due to the cancer diagnosis and more intensive treatment increased the likelihood for need for all rehabilitation services. Forty percent of the patients reported unmet needs for rehabilitation services.
As expected breast cancer patients were more likely to report need for physiotherapy than patients with all the other diagnoses. Breast cancer patients also reported need for admittance to a convalescent home more frequently than the other diagnostic groups. This result is in line with our clinical experience observing that the majority of cancer patients participating at in-patient rehabilitation centers have breast cancer [Citation13]. In line with our hypothesis those receiving intensive treatment and those having comorbidities were more likely to need several rehabilitation services.
Treatment status (during or after treatment) did not influence the need for any rehabilitation service expect for consultation with a social worker, which was more frequently needed during treatment than after treatment. These results demonstrate that patients need rehabilitation services in all phases of cancer treatment. In several clinical settings rehabilitation is offered shortly after completion of treatment, whereas our results indicate that needs for rehabilitation services seems relatively constant the first two to three years after diagnosis and are not influenced upon by treatment status.
Contrasting our findings, a study of 103 females treated for gynaecological cancer showed a greater need for emotional than physical help during and after treatment [Citation14]. Our finding of less than one third of the patients reporting need for psychological counseling is similar to the findings of Ernstmann et al. [Citation11]. Comparisons with other studies are limited by different assessment methods and/or different samples.
Forty percent of the participants reported unmet needs for rehabilitation services. The unmet need was highest for physical training and lowest for occupational therapy. In contrast, the supportive group session was the service that was most frequently offered but not needed. These findings are important for health authorities in future planning of cancer rehabilitation. Previous studies have reported different proportions of unmet needs for various rehabilitation programs [Citation11,Citation15]. Zebrack et al. reported that more than half of the respondents indicated that their needs for information and services have been unmet [Citation15], whereas the results from the study of Ernstmann et al. showed that less than 20% had an unmet need for psychosocial support [Citation11]. In addition to differences between samples, local, regional and national differences might effect upon the number of patients reporting unmet needs. There are also reasons to believe that rehabilitation services offered to cancer patients may differ across Europe and even within European regions such as within Scandinavia. Further, patients’ needs for rehabilitation services are also probably influenced by expectations within the population. For example, absence of rehabilitation services might lower expectations and thereby reduce the number reporting unmet needs.
One limitation of this study is that the questionnaire was not fully validated. However, the items have a concrete content thus limiting the need for psychometric testing and most of them have been used in previous surveys of other populations. Further, the test-retest reliability of the questionnaire and its sensitivity to detect between-patient differences have not been established. Thus, the questionnaire's discriminative properties are not documented. However, the questionnaire was pilot-tested for clarity and understandability and subsequently adjusted. Another limitation is that the rehabilitation services asked for are not complete since, for example, nutritional counseling was not included.
The needs for rehabilitation services among those 60 years or older was not assessed due to the inclusion criteria. The cancer incidence is higher and increasing among the elderly, and theoretically elderly patients could need rehabilitation services to a higher extent than younger patients due to their higher prevalence of comorbidities and generally poorer health status. However, we found that the needs for some types of rehabilitation services were less frequently reported among the oldest in the present sample. This might indicate that patients aged > 60 years not necessarily report needs for rehabilitation services more frequently than patients aged < 60 years or less.
The CRN has a complete list of all new cancer cases in Norway. Patients treated at four hospitals from different health regions were eligible for this survey in order to reflect the total population of Norwegian cancer patients. All eligible patients from these hospitals were included, and the sample is therefore assumed to be fairly representative for Norwegian cancer patients aged between 25–60 years. However, a relatively low response rate of 54% may result in a biased sample. Compared to the general population, women were overrepresented and the educational level was higher in our sample (www.ssb.no/utniv/tab-2008-08-21-03.html). In sum these considerations and the assumption that patients not interested in rehabilitation probably will not respond to such a survey makes us conclude that an overestimation of the needs is more probable than an underestimation.
In order not to complicate data collection and increase costs, permissions from the patients to collect and link data from their medical journal with the survey data were not obtained. Thus, all medical information is self-reported which presupposes that the patients have adequate knowledge of their medical history and treatment. Possible sources of errors associated to the self-reported medical data are considered acceptable due to the relatively broad categories being asked for (diagnosis, type of treatment and recurrence). Further, “needs for rehabilitation” were assessed by the patients’ self-report and not by any functional assessment. The agreement between self-reported need and the actual use of the services offered is unknown. Still, we believe that an objectively assessed need to a large extent will also be perceived as a need subjectively.
The large patient sample has made it possible to investigate the influence of medical and demographical background variables. Thus, we have been able to examine how the needs for different rehabilitation services differ among different subgroups of cancer patients. These results should in our opinion therefore be of interest to both clinicians working with cancer rehabilitation and health authorities.
Conclusions
The majority of cancer patients report needs for one type of rehabilitation service, two thirds of those also report need for two or more services, and 40% had an unmet need for rehabilitation services. Future focus should in our opinion be more directed towards content of the services and their effects, and prospective studies are needed in order to investigate the optimal content of the rehabilitation services for cancer patients and at what time they are mostly needed, as well as to identify patients that will benefit from the different services.
Acknowledgements
This project was requested and financed by The Norwegian Cancer Society which however had no influence over the data collection or the statistical analyses presented in this study.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML, Klint A, . NORDCAN – a Nordic tool for cancer information, planning, quality control and research. Acta Oncol 2010;49:725–36.
- Cancer Registry of Norway Ioocr. Cancer in Norway 2008 – Cancer incidence, mortality, survival and prevalence in Norway. 2009.
- Fossa SD, Vassilopoulou-Sellin R, Dahl AA. Long term physical sequelae after adult-onset cancer. J Cancer Surviv 2008;2:3–11.
- Fossa SD, Loge JH, Dahl AA. Long-term survivorship after cancer: How far have we come? Ann Oncol 2008;19(Suppl 5):v25–v29.
- Alfano CM, Rowland JH. Recovery issues in cancer survivorship: A new challenge for supportive care. Cancer J 2006;12:432–43.
- Aziz NM. Cancer survivorship research: Challenge and opportunity. J Nutr 2002;132(11 Suppl):3494S–503S.
- World Health Organization [Internet]. Geneva: World Health Organization, Disability and Rehabilitation Team; 2009.
- Vallance JK, Courneya KS, Jones LW, Reiman T. Exercise preferences among a population-based sample of non-Hodgkin's lymphoma survivors. Eur J Cancer Care (Engl) 2006;15:34–43.
- Jones LW, Courneya KS. Exercise counseling and programming preferences of cancer survivors. Cancer Pract 2002; 10:208–15.
- Stevinson C, Capstick V, Schepansky A, Tonkin K, Vallance JK, Ladha AB, . Physical activity preferences of ovarian cancer survivors. Psychooncology 2009;18:422–8.
- Ernstmann N, Neumann M, Ommen O, Galushko M, Wirtz M, Voltz R, . Determinants and implications of cancer patients’ psychosocial needs. Support Care Cancer 2009;17: 1417–23.
- Fløtten T, Torp S, Kavli H, Nielsen R, Syse J, Grønningsæter AB, . Kreftrammedes levekår Om arbeid, økonomi, rehabilitering og sosial støtte. FAFO-rapport 2008. 2008;47. Norwegian.
- Fossa SD, Kvaloy J, Kvaloy S, Loge JH, Dahl AA. Courses for cancer patients–15 years’ experience at The Montebello Centre in Norway. Tidsskr Nor Laegeforen 2008;128:2554–7. Norwegian.
- Steele R, Fitch MI. Supportive care needs of women with gynecologic cancer. Cancer Nurs 2008;31:284–91.
- Zebrack B. Information and service needs for young adult cancer survivors. Support Care Cancer 2009;17:349–57.