To the Editor,
A 48-year-old man originally from Asia presented to clinic with a six month history of diarrhea. He reported two to four loose stools per day which was watery in nature and consisting of food particles. It was associated with vague abdominal pain. He also complained of involuntary weight loss of 9 kg over a six month period. He denied nausea, vomiting, malena, hematuria and fever. His past medical history included hypertension well controlled with nifedipine. There was no history of other medication use or drug abuse. He is a non-smoker and consumed no alcohol. Family history was non-contributory. On physical examination, his vitals were within normal limits. There was no lymphadenopathy. Systemic examinations including abdominal examination were unremarkable and without any organomegaly.
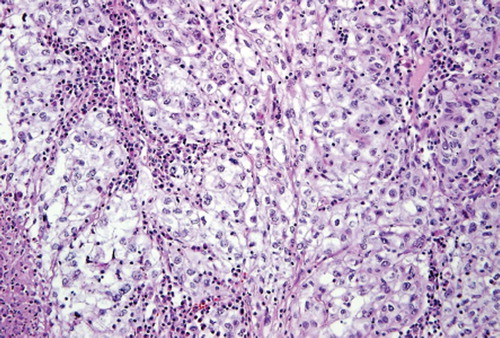
Initial stool tests for ova, parasites, WBCs, culture, fecal occult blood test and clostridium difficile toxin were all negative. Complete blood count, blood chemistries, urinalysis, liver function tests, erythrocyte sedimentation rate, C-reactive protein, TSH, and celiac profile (anti transglutaminase IgA antibody test) did not reveal any abnormality. Patient underwent esophago-gastro-dudenoscopy with biopsy and colonoscopy which were non-diagnostic. CT scan of abdomen and pelvis showed a left renal mass, the largest measured dimension being 10 × 3 × 12 cm (). Mass was heterogeneous, partially necrotic with mild stranding in the perinephric fat with normal left renal vein and enlarged left peri-aortic lymph node of 17 mm. His CT scan of the chest and bone scan were normal. Patient underwent left radical nephrectomy. Following surgery, diarrhea resolved completely. The histopathological examination revealed grade III, renal cell carcinoma (RCC), with extension into perinephric soft tissue. Picture shows RCC cells in an alveolar arrangement with clear cytoplasm and distinct cell membranes consistent with RCC clear cell variant ().
Figure 1. CT scan showing left renal mass.
Figure 2. Histopathology showing RCC cells in an alveolar arrangement with clear cytoplasm.
Discussion
Renal cell carcinoma, so called one of the “great mimics” of medicine, is associated with a multitude of paraneoplastic syndromes, vascular syndromes and metastases to unusual sites [Citation1]. The incidence of paraneoplastic syndromes in RCC is found in about 10–40% of cases [Citation2]. Paraneoplastic syndromes associated with RCC include hypercalcemia, hypertension, polycythemia, non-metastatic hepatocellular enzyme elevation (Stauffer syndrome), fever, weight loss, cachexia, Cushing's syndrome, abnormalities in glucose metabolism, neuromyopathies, amyloidosis, anemia, dermatomyositis, galactorrhea, and glomerulopathies [Citation1,Citation3,Citation4]. These may be the initial manifestations of the disease or indicate the recurrence of the treated disease [Citation3].
RCC was found during work up for diarrhea in our patient. Diarrhea completely resolved following nephrectomy. We suggest diarrhea as a paraneoplastic syndrome of RCC in our patient. To the best of our knowledge, this is the second reported case of RCC presenting with diarrhea. Roldán et al. [Citation5] reported a case of RCC with diarrhea and weight loss where diarrhea resolved following surgery. Diarrhea syndrome in tumors may be due to the production of prostaglandins, vasoactive intestinal peptide [Citation6,Citation7].
In conclusion, the initial presentation of RCC may be diarrhea, as a paraneoplastic manifestation. Although rare, physicians should consider this possibility once common causes of diarrhea are ruled out.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Papac RJ, Poo-Hwu WJ. Renal cell carcinoma: A paradigm of lanthanic disease. Am J Clin Oncol 1999;22:223–31.
- Sacco E, Pinto F, Sasso F, Racioppi M, Gulino G, Volpe A, . Paraneoplastic syndromes in patients with urological malignancies. Urol Int 2009;83:1–11.
- Palapattu GS, Kristo B, Rajfer J. Paraneoplastic syndromes in urologic malignancy: The many faces of renal cell carcinoma. Rev Urol 2002;4:163–70.
- Curti BD. Renal cell carcinoma. JAMA 2004;292:97–100.
- Roldán AB, López CG, Olivera FT, Benítez AV, Bautista FP, Gutiérrez JMH. Diarrhea syndrome and renal cell carcinoma. Rev Esp Enferm Dig 2008;100:505–6.
- Metz SA, McRae JR, Robertson RP. Prostaglandins as mediators of paraneoplastic syndromes: review and up-date. Metabolism 1981;30:299–316.
- Ebeid AM, Murray PD, Fischer JE. Vasoactive intestinal peptide and the watery diarrhea syndrome. Ann Surg 1978;187:411–6.