To the Editor,
Adult T-cell leukaemia/lymphoma (ATLL) is an aggressive type of leukaemia/ lymphoma associated with human T-cell lymphotropic virus type I (HTLV-1). Patients with ATLL usually have short survival and poor response to treatment. ATLL is classically divided into four clinical types: acute, chronic, lymphoma and smoldering. We report two occult cases of ATLL which indicated that clinical awareness is important to avoid missing the diagnosis.
Case 1
The first patient was a 57-year-old Hong Kong Chinese male with a history of hypertension and diabetes mellitus presented with multiple cervical lymph nodes for one month. He also had fever, decreased appetite and weight loss. Physical examination showed bilateral cervical lymphadenopathy and hepatomegaly. Laboratory investigations showed lymphocytosis with lymphocyte count of 4.67 × 109/L. Flow cytometry revealed the lymphocytes to be positive for CD3, CD4 and CD5 and negative for CD7, CD8, CD19, CD20, CD22 and CD56. The immunophenotype was suggestive of T-lymphoproliferative disease. There was raised serum globulin and the serum calcium level was mildly elevated at 2.61 mmol/L. Lactate dehydrogenase level was 628 u/L. Cervical lymph node biopsy was performed and showed proliferation of mostly small and some medium sized lymphoid cells with irregular nuclear outline. There were readily noted arborising and branching vessels. There were also frequent mitotic figures and the tumour cells were immunoreactive to CD3, CD5 and negative to L26, cyclin D1, ALK and CD 30. The features were interpreted as angioimmunoblastic T-cell lymphoma. Bone marrow examination confirmed lymphomatous involvement at the marrow. He was given eight courses of CHOP chemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisolone), but there was still residual disease at the marrow. He also had a rash involving his forearm and legs and skin biopsy confirmed lymphomatous involvement at the skin ().
Figure 1A. Patient has skin involvement by the lymphoma. B. Flower cell (centre) in peripheral blood of the patient.
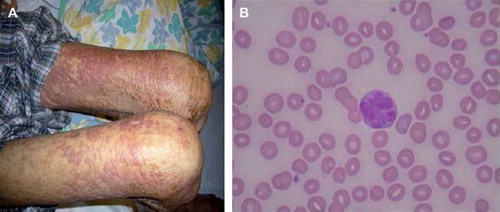
Further review of the peripheral blood films showed flower cells which were typical of ATLL (). Serology for human T- cell lymphotropic virus 1 (HTLV-1) was positive for the patient. The overall features were consistent with ATLL. The patient was refractory to further chemotherapy (SMILE regimen, dexamethasone, methotrexate, ifosphamide, L-asparaginase and ectoposide). Zidovudine was also added but there was still no improvement and palliative care was then given. He finally died of pneumonia.
Case 2
This was a 50-year-old Chinese female with a history of pulmonary tuberculosis given anti-TB drugs. She presented with shortness of breath, fever and cough. CXR showed diffuse patchy infiltrates. She had desaturation and was intubated. HRCT thorax showed patchy ground glass opacity over bilateral lung fields. Bronchoscopy did not show any endobronchial lesion. Transbronchial biopsy showed interstitial pneumonia and transbronchial aspirate grew pseudomonas and nocardia. Patient was given broad-spectrum antibiotics, condition gradually improved and she was later extubated.
She was then noted to have lymphocytosis in peripheral blood with lymphocyte count of 5.3 × 109/L. Flow cytometry revealed the lymphocytes to be positive for CD4, CD7 but negative for B-cell markers. It was suspicious of T-cell lymphoproliferative disease. Serology for HTLV-1 was checked and turned out to be positive for this patient. Bone marrow exam showed evidence of clonal T-cell proliferation. There was generalised increase in lymphocytes with some disruption of the normal marrow architecture. Immunohistochemical study showed that these are CD3 positive T-cells. The bone marrow morphology, leukaemic involvement and the positive anti HTLV-1 antibody were consistent with ATLL, chronic variant. Patient was given interferon-alpha and zidovudine for ATLL. Bone marrow exam repeated four months after treatment and showed no evidence of residual lymphoma.
Discussion
Adult T-cell leukaemia/lymphoma (ATLL) is caused by HTLV1 which is endemic in Japan, Africa, South America and Caribbean. HTLV-1 infection affects 15–20 million people worldwide, although 95% of individuals infected remain asymptomatic [Citation1]. The estimated population carriage rate of HTLV-1 in Hong Kong Chinese is 0.0041% [Citation2]. Several clinical variants are recognised: acute, lymphomatous, chronic and smoldering. The acute form is characterised by increasing WBC, lymphadenopathy, hepatosplenomegaly, skin lesion and hypercalcaemia. ATLL cells are variable in size and have a flower-shaped nucleus. The mature T-cells are almost invariably CD4+ and CD25+ , but are usually negative for CD7 and CD8.
Our first patient was initially suspected to have angioimmunoblastic T-cell lymphoma and he was refractory to chemotherapy. The diagnosis was reviewed and then serology for HTLV-1 was checked and turned out to be positive. Blood film was also reviewed and cells with flower-shaped nucleus typical of ATLL were seen. There was case report of patients with morphologic variant of ATLL, angioimmunoblastic T-cell lymphoma [Citation3]. In that study, the examined lymph node showed features of angioimmunoblastic T-cell lymphoma. However, the immunohistochemical features were suggestive of ATLL and the serology for HTLV-1 was positive for all the patients. Our patient may have this morphologic variant of ATLL and the HTLV-1 antibody status and flower cell in blood film both were compatible with the diagnosis of ATLL.
The second patient was admitted for pneumonia requiring intubation and underlying cause of impaired immunity was searched. Lymphocytosis in peripheral blood was noted and then flow cytometry was suggestive of T-cell lymphoproliferative disease. She was finally diagnosed to have ATLL from the bone marrow exam and the HTLV-1 serology. The interstitial pneumonia found in this patient can be secondary to the ATLL since ATLL is an immunodeficient condition which can lead to various types of pulmonary diseases [Citation4]. Some patients were diagnosed to have “chronic lung diseases” before the diagnosis of ATLL [Citation5]. Hence, when we encounter patients with unexplained pulmonary diseases, we may need to consider any underlying immunodeficient condition like lymphoma as in our patient. She was treated with interferon-alpha and zidovudine for the ATLL and there was good response with the treatment.
The prognosis for ATLL is generally poor with median survival ranging from 7 to 13 months [Citation6]. The overall treatment for ATLL has remained unsatisfactory. There are two major difficulties. One is a highly immunocompromised state leading to development of lethal opportunistic infections. The other is intrinsic tumour cell resistance to conventional chemotherapy by expressing p-glycoprotein and antiapoptotic proteins.
Various therapies have been used, including combinations of standard chemotherapy with antiretroviral agents like zidovudine, arsenic trioxide [Citation7] and monoclonal antibodies. Response to conventional treatments is generally less than 50% and of short duration. There was case report of using aleutuzumab (anti-CD52) in a patient with refractory disease and could achieve a prolonged remission (more than a year) following 12 weeks of treatment with subcutaneous alemtuzumab [Citation8].
Zidovudine in combination with interferon-alpha, with or without concomitant chemotherapy, has shown improvement in response rate and survival. The overall response rate is 67% and median survival is 18 months [Citation9]. Allogenic stem cell transplant may play a role in the treatment of ATLL. A study of 40 ATLL patients showed three-year overall survival was 45% after transplant [Citation10].
In summary, ATLL is a relatively rare and aggressive lymphoma. Clinical awareness is important to avoid missing the diagnosis. Response to treatment is usually fair and of short duration.
Acknowledgements
The authors would like to thank Dr L. G. Wong for review of the slides. The authors declare no conflict of interest.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Mahieux R, Gessain A. HTLV-1 and associated adult T-cell leukaemia/lymphoma. Rev Clin Experiment Hematol 2003; 7:336–61.
- Au WY, Lo JYC. HTLV-1 related lymphoma in Hong Kong Chinese. Am J Hematol 2005;78:80–4.
- Karube K, Suzumiya J, Okamoto M, Takeshita M, Maeda K, Sakaguchi M, . Adult T-cell lymphoma/ leukemia with angioimmunoblastic T-cell lymphomalike features: Report of 11 cases. Am J Surg Pathol 2007;31:216–23.
- Tamura K, Yokota T, Mashita R, Tamura S. Pulmonary manifestations in adult T-cell leukemia at the time of diagnosis. Respiration 1993;60:115–9.
- Yoshioka R, Yamaguchi K, Yoshinaga T, Takatsuki K. Pulmonary complications in patients with adult T-cell leukemia. Cancer 1985;15:2491–4.
- Plumelle Y, Pascaline N, Nguyen D, Panelatti G, Jouannelle A, Jouault H, Imbert M. Adult T-cell leukaemia/lymphoma: A clinico-pathologic study of 26 patients from Martinique. Hematol Pathol 1993;7:251–62.
- Hermine O, Dombret H, Poupon J, Arnulf B, Lefr re F, Rousselot P, . Phase II trial of arsenic trioxide and alpha interferon in patients with relapsed /refractory adult T-cell leukaemia/lymphoma. Hematol J 2004;5:130–4.
- Mone A, Puhalla S, Whitman S, Baiocchi R, Cruz J, Vukosavljevic T, . Durable haematologic complete response and suppression of HTLV-1 viral load following alemtuzumab in zidovudine/IFN-alpha refractory adult T-cell leukaemia. Blood 2005;106:3380–2.
- Matutes E, Taylor G P, Cavenagh J, Pagliuca A, Bareford D, Domingo A, . Interferon alpha and zidovudine therapy in adult T-cell leukaemia/ lymphoma: Response and outcome in 15 patients. Br J Haematol 2001;113:779–84.
- Fukushima T, Miyazaki Y, Honda S, Kawano F, Moriuchi Y, Masuda M, . Allogenic haematopoietic stem cell transplantation provides sustained long-term survival for patients with adult T-cell leukaemia/lymphoma. Leukaemia 2005;19: 829–34.