Abstract
Background. Increased rates of coronary heart disease (CHD) and cerebrovascular disease in later life have been repeatedly observed in subjects with low birth-weight. One possible reason for low birth-weight is prenatal stress. Little is known about the influence of prenatal stress on lifelong health outcomes.
Aims. In this study we investigate the influence of prenatal stress on CHD and cerebrovascular disease incidence in adult life.
Methods. We analysed data originating from the Helsinki Birth Cohort Study including hospital data from all men and women born between 1934 and 1944 (n = 13,039) in two hospitals of Helsinki. We estimated the hazard function based on Weibull distribution. We compared those exposed and unexposed to bombings while in utero in terms of lifelong CHD and cerebrovascular disease hazard.
Results. In women exposed to bombings while in utero, we observed higher survival rates of both CHD and cerebrovascular disease than in those unexposed. In men, the results were ambiguous.
Conclusions. Our findings suggest that prenatal exposure to severe stress may be associated with protective effects on the development of CHD in later life.
Introduction
Increased rates of coronary heart disease (CHD) and cerebrovascular disease in later life have been repeatedly observed in subjects with low birth-weight (Citation1–3). One possible reason for low birth-weight is prenatal stress. Prenatal stress has been reported to cause higher prevalence of unfavourable psychological health outcomes in the offspring (Citation4). There is also evidence that major stressful events are associated with a lower birth-weight. For example, studies of the effects on birth outcomes in term deliveries after the World Trade Centre disaster in 2001 showed that birth-weight in the offspring was significantly lower for those who lived close to the event site (Citation5,Citation6). A study of the Belgrade bombings in 1999 showed similar results (Citation7). This could have far-reaching health consequences because of the link to non-optimal growth in utero—which is reflected by low birth-weight in relation to the length of gestation—and the incidence of CHD in adulthood (Citation8–10).
Little is known about the influence of severe prenatal stress on lifelong health outcomes in the offspring. There are some studies focusing upon long-term consequences of malnutrition and stress during the Dutch Hunger Winter, the Leningrad Siege, and the Channel Island famine. The findings regarding the influence on CHD and its risk factors were conflicting (Citation11–14). Interestingly, prenatal exposure to the 1918 influenza pandemic apparently increased the rate of ischemic heart disease (Citation14,Citation15). However, in these extreme conditions it is difficult to differentiate between the effect of stress and that of malnutrition. Animal studies suggest that prenatal stress may cause the offspring to be more sensitive to diseases in later life even in absence of the association with birth outcomes (Citation16).
During the Second World War, Finland fought two wars with the Soviet Union: The ‘Winter War’ between 30 November 1939 and 13 March 1940, and the ‘Continuation War’ from 25 June 1941 to 19 September 1944. During these time periods, Helsinki was bombed several times.
The bombings of Helsinki provide a good basis for assessing the influence of severe prenatal stress on the lifelong health outcome. In this study we investigate the influence of prenatal stress on CHD and cerebrovascular disease incidence in adult life and whether this potential effect is mediated through low birth-weight.
Patients and materials
The study cohort originates from the Helsinki Birth Cohort Study (HBCS), a cohort study with 13,345 men and women, of whom 4,585 were born at the Helsinki City Maternity Hospital and 8,760 at the University Hospital in Helsinki between 1934 and 1944, who attended child welfare clinics in the city and who lived in Finland in 1971 when a unique personal identification number had been allocated to each resident of the country (Citation17). The cohort data include birth characteristics and data on the mothers such as age, parity, height, and date of last menstrual period (Citation10,Citation18). The death registry data contain International Classification of Diseases (ICD) codes of causes of death, and the hospital discharge registry lists ICD codes of the diagnoses made during hospital visits of the individuals. Using the personal identification number, all hospital admissions and deaths could be obtained from the Death Register and the Hospital Discharge Registry maintained by the National Research and Development Centre for Welfare and Health from 1964 onwards (Citation1,Citation19). The following ICD codes were used in this study: CHD: ICD8 and ICD9: 410–414, ICD10: I21-I25; and cerebrovascular disease: ICD8 and ICD9: 430–438, ICD10: I60–I69 (Citation19).
Data on bombings have been gathered from historical sources and conserved records of the exact dates and times of the bombing raids from the military archive in Helsinki. Damage and destruction of buildings, loss of human lives, and number of injured persons have been brought together from historical sources (Citation20,Citation21).
During the Winter War and the Continuation War, Helsinki was bombed several times. The first raids initiated the Winter War in November 1939 (Citation20). During these raids 97 people died and 60 were wounded. The second wave of raids happened during 2 days in January 1940, with no further raids during that war. In the Continuation War, Finland was frequently bombed but generally with lower intensity than in the Winter War (Citation21). There were 9 raids in 1941, 17 in 1942, and 13 in 1943, with a total of 104 dead and 398 wounded (Citation20). Three very intensive raids took place within a short time period in February 1944; due to the successful air defence of the city, the extent of damage and number of dead and wounded could be kept to a minimum. Nevertheless, there were 146 fatal casualties and 364 wounded (Citation20). At the time of the Second World War, Helsinki was concentrated on a peninsula surrounded by the sea and was relatively compact with about 275,000 inhabitants (Citation22). Therefore we can assume that the threat of losing one's life, friends, family, or property to have been equally present for everyone living in the city during that time.
Methods
The incidence of both CHD and cerebrovascular disease was assumed to follow a Weibull hazard model (Citation23). A Bayesian conditional autoregressive model (CAR) (Citation24) was fitted to the Weibull median with time of birth as a spatial co-ordinate. The model assumes that people born closer in time to each other would have a more similar hazard than people born further apart. This conditioning also allows to ‘borrow strength’ from the neighbouring observations, making the analysis more powerful than, for example, comparison of individual months of birth. The model was estimated using an MCMC algorithm run on C. A total of 500,000 iterations were run after an initial burn-in of 100,000, which was deemed to be sufficient to achieve convergence.
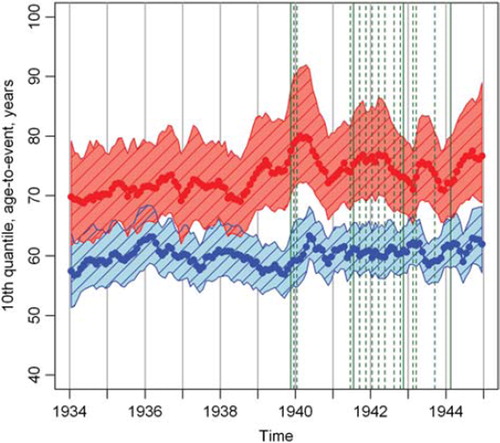
The study subjects were divided into groups based upon the exposure to bombings while in utero. The time in utero was assessed to be 2 weeks after the last menstrual period of the mother and ending with the birth date. During the study period from 1934 to 1944, there were 48 days when bombings occurred. These are grouped into ‘all bombings’, including all 48 days. This is illustrated in . We also divided the bombings into ‘major bombings’, based upon dates with high numbers of causalities (deaths and injuries) compared to the other bombings. These major bombings took place on the following days during the study period: 30 November 1939, 9 July 1941, and 6, 7, 16, and 17 February 1944.
Figure 1. The mean posterior 10th quantile of the age-to-event for coronary heart disease based on CAR Weibull distribution fitted separately for men (below) and women (above) with a 95% envelope. The vertical dashed lines indicate “all bombing” dates, including the non-dashed “major bombing” dates.
The Weibull model was estimated for each group separately by gender. The survival curves adjusted for birth-weight, socio-economic status (SES) characterized by father's occupation, and parity were then evaluated together with the corresponding pointwise age-specific 95% credible intervals (Bayesian version of confidence intervals). Birth-weight, gestational age, birth-weight adjusted for gestational age, ponderal index, length at birth, and socio-economic status according to the father's occupation were also compared between the groups.
Results
We used a total number of 13,039 individual records of which 52% were male for the unadjusted autoregressive analysis. Of the study subjects, 7,493 (57%) were exposed to at least one bombing while in utero, and 5,198 (40%) were exposed to at least one major bombing while in utero. Of these, 12,209 had information on both SES and parity. There was no statistically significant difference in birth-weight, gestational age, birth-weight adjusted for gestational age, ponderal index, length at birth, or socio-economic status according to the father's occupation between exposed and unexposed subjects, in either the major or all-bombing group (). The distributions of SES and parity were somewhat different. However, the Weibull regression modelling has shown no effect of parity on the risk of either CHD or cerebrovascular disease. The male children of labourers appeared to have, on average, a higher risk of both CHD and cerebrovascular disease than do the male children of higher office workers. No such effect was found for women. The birth-weight only had an effect on CHD risk for men (posterior P = 0.0013).
Table I. Birth characteristics of exposed and unexposed individuals.
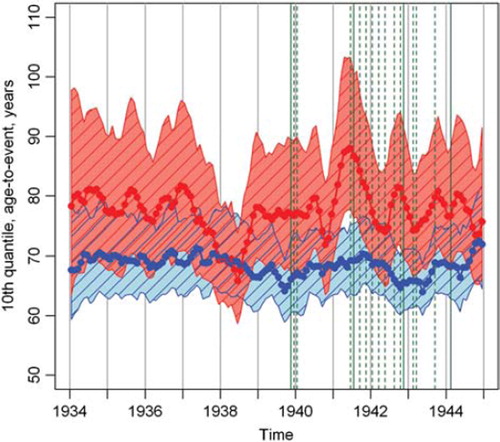
and illustrate the mean posterior 10th quintile of the age-to-event for CHD and cerebrovascular disease, respectively. This means that in the absence of competing risks, an average 10% of the individuals will get the disease by the age shown on the y-axis, provided they survived until then. Higher quintile value thus corresponds to longer disease-free survival and lower age-specific risk for all ages. If there was an adverse effect of bombings on the CHD lifelong outcome, we would expect the curve to go upwards after a bombing event, which is not the case. The 95% credible intervals show that there are no exceptional tendencies; therefore we can conclude that the disease risk has stayed level over the years. The higher values for women correspond to fewer CHD and cerebrovascular disease cases.
Figure 2. The mean posterior 10th quantile of the age-to-event for cerebrovascular disease based on CAR Weibull distribution fitted separately for men (below) and women (above) with a 95% envelope.
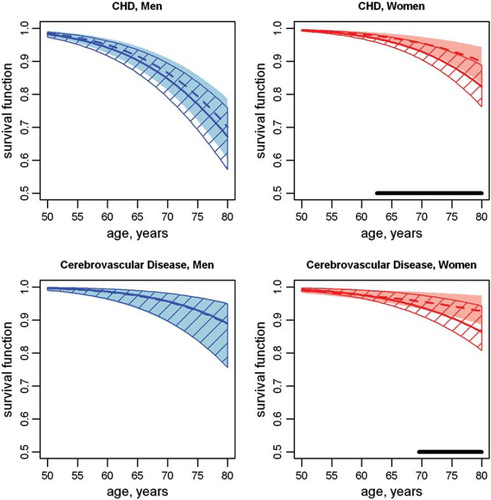
Fitting survival curves for CHD and cerebrovascular disease separately by sex and exposure to all and major bombings, we detected better survival rates for CHD in both exposed women and men ( and ). In the all-bombings group, the survival rates were significantly higher in women between 63 and 80, for men between 50 and 54 years of age. In the major bombing group, the rates for CHD were significantly higher only in women between 62 and 80, and for cerebrovascular disease also only in women between 70 and 80 years of age. Subdivision into pregnancy trimesters did not show differences in the result by trimester (data not shown).
Figure 3. Posterior 95% envelopes and mean survival curves of coronary heart disease and cerebrovascular disease adjusted for birth weight, parity and father's occupation, and fitted separately for individuals unexposed (solid line) and exposed (dashed line) to all bombing events. The thick horizontal lines indicate significant differences in survival.
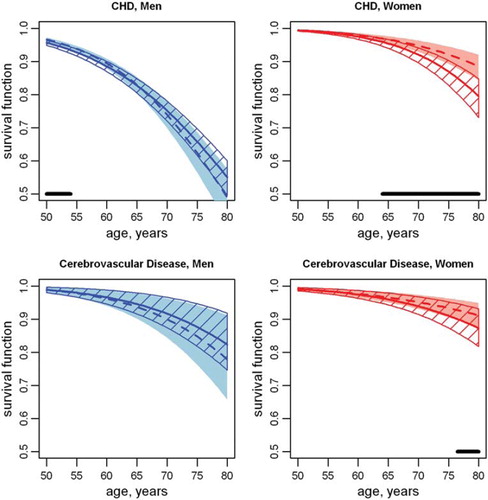
Figure 4. Posterior 95% envelopes and mean survival curves of coronary heart disease and cerebrovascular disease adjusted for birth weight, parity and father's occupation, and fitted separately for individuals unexposed (solid line) and exposed (dashed line) to major bombing events. The thick horizontal lines indicate significant differences in survival.
Discussion
Among subjects exposed to bombings while in utero, we observed higher CHD survival rates from the age of 64 and above in women, and between 50 and 54 in men, when all bombing dates were taken into account. If we take only the major bombing days—with considerably higher numbers of causalities and more damage to buildings than other bombings—into account, the figures for women do not change markedly, while the significant effect on men disappears. However, an additional significant effect on cerebrovascular disease in women was found. There were no significant differences in birth-weight, gestational age, birth-weight adjusted for gestational age, ponderal index, and length at birth between the exposed and unexposed groups.
We observed a difference in the ages at which women and men have higher survival rates for CHD. Women start to have health problems due to CHD at a later age than do men, which explains the gender-specific shift in the age range of the significant higher survival rates for exposed subjects.
In the present study we divided the bombings into two categories. Major bombings include bombings that caused a considerably higher number of causalities and more damage to buildings than the other bombings. We expect major bombings to be more stressful and therefore to show a potential effect more clearly. Several studies on the effect of birth outcome in term deliveries have shown decreased birth-weights, for example, after the terrorist attack on the World Trade Centre in 2001 and the Belgrade bombings in 1999 (Citation5–7). However, we did not observe any effect of prenatal exposure to the bombings on birth-weight adjusted for gestational age. This indicates that there was no detectable restriction of growth in utero associated with the bombings.
In opposition to our original hypothesis we observed higher CHD survival rates among both men and women exposed to bombings while in utero. Previous studies, such as the Dutch Hunger Winter study, the Channel Island famine study, and the Leningrad Siege study focused upon the long-term health effects of malnutrition (Citation11–14). In these studies the severe malnutrition was also found to be a stress factor for pregnant women. However, the findings with regard to influence of prenatal stress on coronary heart disease and its risk factors varied between the studies. In the Leningrad Siege study and the Channel Island famine study, little effect of prenatal stress and malnutrition was seen on later coronary heart disease and cardiovascular diseases in general, respectively. In contrast, findings from the Dutch Hunger Winter suggest that malnutrition during prenatal life would have a long-term effect by increasing the risk of coronary heart disease and type 2 diabetes in later life. This effect was not always mediated by a small body size at birth (Citation25). A paper on the impact of the economic crises due to the US embargo in Cuba on health indicates that despite food and medicine restrictions, Cuba showed health gains through lowered infant and maternal mortality, and reduction of other diseases (Citation26). This indicates that milder food shortages, possibly similar to those that occurred in Finland during the Second World War, may also be protective regarding the long-term health outcome.
Miscarriages caused by stress may affect ‘genetically weaker’ embryos (Citation27). Due to the severe stress of the bombings, miscarriages could have been more frequent and therefore lead to a selection bias of our sample of the exposed group. Stronger and therefore healthier embryos in later life—also regarding CHD—could have been more likely to survive. However, since we have no data on miscarriages, we cannot test this hypothesis.
During the Continuation War of 1941–1944, bombing raids were more frequent but with lower intensity than in the Winter War. This could induce some degree of adaptation to the alarms and to the raids so that the actual threat is not big enough any more to have an effect in utero. This adaptation could also influence the hormonal axis. However, even if this were the reason, we should still see an effect when concentrating only on major bombings. This was not the case; the effects of stress at a specific point in pregnancy may, however, not be visible due to limited statistical power.
We focused our study on CHD and cerebrovascular disease. Both diseases occur during later adult life. Our study cohort consists of individuals who were mostly between 60 and 70 years of age when these outcomes were assessed. A longer follow-up period would increase the statistical power of the study. On the other hand, already at this age morbidity is fairly common especially among men.
Both exposed and unexposed subjects while in utero to bombings experienced many other stressors during that time such as food shortages, concern for family members at the front, threat of invasion by the enemy, and related war strains, which could mask and hide a potential effect of the bombings. Compared to the World Trade Centre disaster and the health outcomes, in our study there is not just a single extreme event. Furthermore, the bombing events in Helsinki might not have been always comparable in intensity. We tried to solve this problem by introducing exposed groups only for major bombings, which included only bombings where there were a lot of casualties and a high number of destroyed buildings. However, the results for major and all bombings were not different from each other. A more optimal way to study this would be to compare a wartime group with a post-war control group. Unfortunately, there is no such data available in the Helsinki Birth Cohort Study. One reason for not finding a positive association between prenatal stress and later CHD could be that only stress severe enough to lower birth-weight would have adverse effects on the development of CHD.
Findings from the Dutch Hunger Winter suggested that the trimester during which the individual was exposed matters (Citation28). We investigated this in our cohort but did not find any support of this hypothesis in relation to the bombings and later health outcomes.
In conclusion, our findings suggest that prenatal exposure to severe stress may be associated with protective effects on the development of CHD in later life.
Ethical considerations and data confidentiality
The Ethical committees at Helsinki University Central Hospital and at the National Public Health Institute have approved the Helsinki Birth Cohort Study.
Acknowledgements
We thank Tom Forsén for the inspiration to that study and the collection of the bombing dates.
Declaration of interest: The authors state no conflict of interest and have received no payment in preparation of this manuscript.
References
- Eriksson JG. Early growth, and coronary heart disease and type 2 diabetes: experiences from the Helsinki Birth Cohort Studies. Int J Obes (Lond). 2006;30 Suppl 4: S18–22.
- Frankel S, Elwood P, Sweetnam P, Yarnell J, Smith GD. Birthweight, body-mass index in middle age, and incident coronary heart disease. Lancet. 1996;348:1478–80.
- Leon DA, Lithell HO, Vagero D, Koupilova I, Mohsen R, Berglund L, . Reduced fetal growth rate and increased risk of death from ischaemic heart disease: cohort study of 15 000 Swedish men and women born 1915–29. BMJ. 1998;317:241–5.
- Bowler RM, Mergler D, Huel G, Cone JE. Psychological, psychosocial, and psychophysiological sequelae in a community affected by a railroad chemical disaster. J Trauma Stress. 1994;7:601–24.
- Lederman SA, Rauh V, Weiss L, Stein JL, Hoepner LA, Becker M, . The effects of the World Trade Center event on birth outcomes among term deliveries at three lower Manhattan hospitals. Environ Health Perspect. 2004;112: 1772–8.
- Berkowitz GS, Wolff MS, Janevic TM, Holzman IR, Yehuda R, Landrigan PJ. The World Trade Center disaster and intrauterine growth restriction. JAMA. 2003;290:595–6.
- Maric NP, Dunjic B, Stojiljkovic DJ, Britvic D, Jasovic-Gasic M. Prenatal stress during the 1999 bombing associated with lower birth weight—a study of 3,815 births from Belgrade. Arch Womens Ment Health. 2010;13:83–9.
- Eriksson JG. Epidemiology, genes and the environment: lessons learned from the Helsinki Birth Cohort Study. J Intern Med. 2007;261:418–25.
- Barker DJ, Osmond C, Simmonds SJ, Wield GA. The relation of small head circumference and thinness at birth to death from cardiovascular disease in adult life. BMJ. 1993; 306:422–6.
- Eriksson JG, Forsen T, Tuomilehto J, Osmond C, Barker DJ. Early growth and coronary heart disease in later life: longitudinal study. BMJ. 2001;322:949–53.
- Roseboom TJ, van der Meulen JH, Osmond C, Barker DJ, Ravelli AC, Schroeder-Tanka JM, . Coronary heart disease after prenatal exposure to the Dutch famine, 1944–45. Heart. 2000;84:595–8.
- Stanner SA, Yudkin JS. Fetal programming and the Leningrad Siege study. Twin Res. 2001;4:287–92.
- Stanner SA, Bulmer K, Andres C, Lantseva OE, Borodina V, Poteen VV, . Does malnutrition in utero determine diabetes and coronary heart disease in adulthood? Results from the Leningrad siege study, a cross sectional study. BMJ. 1997;315:1342–8.
- Head RF, Gilthorpe MS, Byrom A, Ellison GT. Cardiovascular disease in a cohort exposed to the 1940–45 Channel Islands occupation. BMC Public Health. 2008;8:303.
- Mazumder B, Almond D, Park K, Crimmins EM, Finch CE. Lingering prenatal effects of the 1918 influenza pandemic on cardiovascular disease. J Dev Orig Health Dis. 2010;1: 26–34.
- Mastorci F, Vicentini M, Viltart O, Manghi M, Graiani G, Quaini F, . Long-term effects of prenatal stress: changes in adult cardiovascular regulation and sensitivity to stress. Neurosci Biobehav Rev. 2009;33:191–203.
- Eriksson JG, Forsen T, Tuomilehto J, Winter PD, Osmond C, Barker DJ. Catch-up growth in childhood and death from coronary heart disease: longitudinal study. BMJ. 1999;318: 427–31.
- Forsen T, Eriksson JG, Tuomilehto J, Teramo K, Osmond C, Barker DJ. Mother's weight in pregnancy and coronary heart disease in a cohort of Finnish men: follow up study. BMJ. 1997;315:837–40.
- Tolonen H, Salomaa V, Torppa J, Sivenius J, Immonen-Raiha P, Lehtonen A. The validation of the Finnish Hospital Discharge Register and Causes of Death Register data on cerebrovascular disease diagnoses. Eur J Cardiovasc Prev Rehabil. 2007;14:380–5.
- Helminen M, Lukander A. Helsingin Suurpommitukset Helmikuussa 1944. Helsinki: WSOY; 2004.
- Jatkosodan historia 1. Talvisodasta jatkosotaan. Sota alkaa. Porvoo, Helsinki, Juva: WSOY; 1988.
- Helsingin historia 2010. Available from: http://www.hel.fi/wps/portal/Helsinki/Artikkeli?WCM_GLOBAL_CONTEXT=/helsinki/fi/Helsinki-tietoa+ja+linkkej_/Helsingin+historia (accessed 2010).
- Cox DR, Oakes D. Analysis of survival data. New York & London: Chapman and Hall; 1984. 19.
- Besag J, York J, Mollie A. Bayesian image restoration with two applications in spatial statistics. Ann Inst Stat Math. 1991;43:1–59.
- Painter RC, Roseboom TJ, Bleker OP. Prenatal exposure to the Dutch famine and disease in later life: an overview. Reprod Toxicol. 2005;20:345–52.
- Garfield R, Santana S. The impact of the economic crisis and the US embargo on health in Cuba. Am J Public Health. 1997;87:15–20.
- Clark DA, Chaouat G, Gorczynski RM. Thinking outside the box: mechanisms of environmental selective pressures on the outcome of the materno-fetal relationship. Am J Reprod Immunol. 2002;47:275–82.
- Glynn LM, Wadhwa PD, Dunkel-Schetter C, Chicz-Demet A, Sandman CA. When stress happens matters: effects of earthquake timing on stress responsivity in pregnancy. Am J Obstet Gynecol. 2001;184:637–42.