
Abstract
Chlamydia trachomatis (CT) is the most common bacterial cause of sexually transmitted infections. CT infections are strongly associated with risk-taking behavior. Recommendations for testing have been implemented in many countries. The effectiveness of the screening programs has been questioned since chlamydia rates have increased. However, the complication rates including pelvic inflammatory disease, tubal factor infertility, and tubal pregnancy have been decreasing, which is good news. The complication rates associated with CT infection have clearly been over-estimated. Genetic predisposition and host immune response play important roles in the pathogenesis of long-term complications. CT plays a co-factor role in the development of cervical neoplasia caused by high-risk human papillomavirus (HPV) types. The evidence linking CT and other adverse pregnancy outcomes is weak. The current nucleic acid amplification tests perform well. A new genetic variant of CT was discovered in Sweden but has only rarely been detected elsewhere. Single-dose azithromycin remains effective against CT. Secondary prevention by screening is still the most important intervention to limit the adverse effects of CT on reproductive health.
Key messages
Health gains and cost-savings obtained by Chlamydia trachomatis screening programs have been over-estimated.
Women with C. trachomatis infection can be reassured that the risk of long-term reproductive health consequences is low after treatment of a single episode.
C. trachomatis may play a co-factor role in cervical carcinogenesis.
Introduction
Chlamydia trachomatis (CT) infections of the genital tract are highly prevalent globally (Citation1–3). CT is the most common bacterial cause of sexually transmitted infections (STI). Chlamydial infections are strikingly common in young populations and strongly associated with sexual risk-taking behavior. CT is a true obligate intracellular pathogen which has a unique growth cycle distinguished from all other micro-organisms. Because of the slow growth cycle chlamydial infections tend to be silent and chronic. The clinical spectrum of CT infections has been well defined. Selected milestones in the evolution of our understanding of CT genital infections are listed in .
Table I. Chlamydia trachomatis revisited: Major discoveries.
Most CT genital infections are silent or asymptomatic and therefore undiagnosed. Therefore, screening for chlamydial infections remains important in the prevention of CT infections. CT vaccine development is difficult because of the complex antigenic structure and limited knowledge of the protective antigens, and also because the nature of protective immune response and correlates of protection are not well known. Primary prevention of chlamydial infections by vaccination is unlikely in any foreseeable future. There are several CT genital strains, but little is known of specific virulence factors of different strains. Besides host genetics, specific chlamydia strains, called serovars, have also been suggested to affect the course of infection (Citation4). CT strains are classified into genovars using PCR restriction fragment length polymorphism (PCR-RFLP) or sequencing of the ompA gene which encodes the major outer membrane protein (MOMP). The most common genovars causing urogenital tract infections are D, E, F, G, H, I, J, and K.
Epidemiology
Genital chlamydial infections are common in young populations and strongly associated with sexual risk-taking behavior. In a systematic review reporting on CT among asymptomatic European women the prevalence ranged from 1.7% to 17% (Citation5). Among young women attending STD clinics rates are well above 10% (Citation6), and in population-based studies among under-30-year-olds prevalence was between 2% and 6% in the Netherlands (Citation7–9). Reported rates of genital chlamydia infections are rising, but it is unclear whether this is due to increased testing or to a true increase in incidence (Citation10). The chlamydia prevalence and test rates reported in European countries vary and depend on the population tested and on the reporting systems (). According to one study, by age 15 already 25% of adolescent urban women acquired their first STI, most often CT (Citation11). In the US, more than 2.8 million new cases occur annually (Citation12,Citation13). In addition to age, other risk factors include history of chlamydial or other STIs, oral contraceptive use, new or multiple sexual partners, inconsistent condom use, just to name a few. In recent years, large population-based prevalence studies have been reported from several countries and continents. Such studies have been adjusted for age, region, race, and other key variables. For instance, the base-line prevalence among 15–26-year-old women was 4%, based on screening of approximately 40,000 women enrolled in human papillomavirus (HPV) vaccination efficacy trials performed in 14 countries and 4 continents (Citation14,Citation15).
Figure 1. Rate of reported chlamydia cases per 100,000 population: 1998–2007.
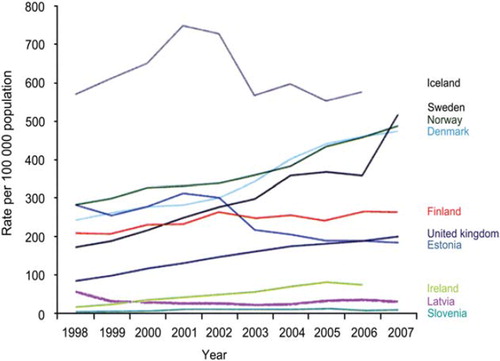
Guidelines or recommendations for annual testing of young sexually active individuals for chlamydial genital infections have been implemented in many countries. The Swedish and the National UK Chlamydia Screening Programme are the best examples of opportunistic screening (Citation2,Citation16,Citation17). Screening can also be provided systematically using registers to identify and invite individuals. Systematic screening is currently used in the Netherlands. The national chlamydia screening program in England offers screening to all sexually active people under the age of 25. Overall, 334,902 screening tests were done in 2007–2008. The positivity rates in women and men were 9.3% and 7.6%, respectively (Citation17). A randomized controlled trial in the general practice (Australian Chlamydia Control Effectiveness Pilot (ACCEPt)) among 16–19-year-old patients presenting for consultation for any reason prefers the word testing rather than screening of asymptomatic individuals. Incentive payments to general practitioners were introduced, and computer alerts increased testing rates by 30% (Citation18).
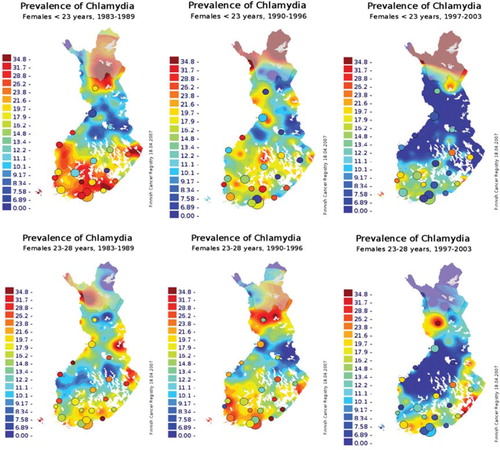
The effectiveness of screening programs has recently been challenged since population studies suggest that screening programs have been strikingly ineffective in lowering CT rates. By contrast, the rates of reported chlamydial infections have recently been increasing in many countries regardless of implementation of screening. This is difficult to explain. One explanation may be that chlamydial infections mostly occur in so-called core groups with risk- taking behavior in which the recurrence rates are strikingly high (Citation19). On the contrary, one seroepidemiologic population-based study from Finland demonstrated that the overall rates of chlamydial antibodies in the population decreased during 1983–2003 () (Citation20). Thus, truly population-based data seem to differ from data based on reported case rates. However, this may also suggest that antibodies are not induced as frequently as earlier due to early detection and antimicrobial treatment known to prevent or delay immune response. Comparative mathematical modeling experiments may be helpful in predicting the population impact of different strategies of chlamydia screening programs (Citation21). In cost-effectiveness analysis, costs, savings and health gains are considered. Only few studies have attempted to quantify health outcomes in terms of quality-adjusted life-years (QALYs), enabling the comparison of chlamydia screening with other health care interventions or with threshold rates for cost- effectiveness. Such exercises have been performed in the USA, the UK, and the Netherlands (Citation22–24).
Reproduced from Chlamydia trachomatis seroprevalence atlas of Finland 1983 – 2003, Lyytikä i nen E, Kaasila M, Koskela P, Lehtinen M, Patama T, Pukkala E, et al. volume 84, pages 19 – 22, Sex Transm Infect, 2008 with permission from BMJ Publishing Ltd.
Figure 2. Chlamydia trachomatis seroprevalence (%) in Finnish women. C. trachomatis IgG antibodies were determined in a random sample of sera from 14–22 and 23–28-year-old women in three consecutive periods (Citation20).
Clinical manifestations
The key clinical manifestations of chlamydial genital infections have been strikingly well described already in the 1970s (Citation25). These include urethritis, mucopurulent cervicitis, plasma cell endometritis, salpingitis, perihepatitis, and periappendicitis. CT infection increases the risk for ectopic pregnancy, tubal factor infertility, chronic abdominal pain, and also increases the risk for hysterectomy. The number of episodes of chlamydial infection progressively increases reproductive tract morbidity. The link between tubal factor infertility and past CT infection is so strong that chlamydial antibody titer is commonly used in clinical practice as a surrogate marker for tubal factor infertility. CT infection has also been linked to other adverse pregnancy outcomes, including chorioamnionitis, placentitis, premature rupture of membranes, and preterm birth. Vertical transmission from the genital tract can cause conjunctivitis and pneumonitis in new-borns.
One recent trend in clinical manifestations has been the rapid decrease in CT-associated upper genital tract infection in women, pelvic inflammatory disease (PID) (Citation26). PID was almost epidemic through the 1980s, and rates followed increasing and high chlamydia rates. Subsequently in-patient PID has become a relatively rare disease (Citation27,Citation28). However, a historical cohort study of almost 25,000 women tested for CT during 1990–2005 still showed a link between prior CT infection and subsequent PID (hazard ratio 1.69; 95% CI 1.21–2.36), although PID was a rare event overall which is reassuring for young women diagnosed with chlamydia (Citation29).
C. trachomatis is still strikingly common in proven PID cases as demonstrated in an on-going study from Malmö University Hospital Sweden (Citation30). Traditional laparoscopic criteria were used for the diagnosis of PID. The overall prevalence of C. trachomatis was approximately 30% of laparoscopically proven cases suggesting that the attributable proportion for C. trachomatis has not much changed during the past 30 years (Citation31). However, only 0.7% of women with positive CT test had PID.
Also the rates of ectopic pregnancy and tubal factor infertility (TFI) have been decreasing in many countries. Recent, revised estimates indicate that the risk of TFI after lower genital tract chlamydial infection is in the range of 4%–5%. This rate is significantly lower than those based on historical case-control studies which were subject to major bias problems. Most previous historical studies were retrospective or cross-sectional, performed in selected patient populations.
The discrepancy between reported chlamydia rates and low or decreasing complication rates remains to be explained. Perhaps increased screening activity and demographic factors such as increasingly common oral contraceptive use among young women explain this to some extent. Thus, from the women's reproductive health point of view the situation at least in developed countries is getting better, which is very good news.
Immunopathogenesis of C. trachomatis infection
The process leading to tubal damage following chlamydial infection has not been well defined, but host genetic factors and individual variation in the immune response are likely to contribute to disease outcome. The T lymphocyte response and a complex network of cytokines are crucial in the resolution of acute infection, and T cells also play an important role in the pathogenesis of C. trachomatis-associated tubal damage. Specifically, a genetic predisposition to low interleukin (IL)-10 and high tumor necrosis factor (TNF)-α expression is associated with a strong inflammatory response and fibrosis of the fallopian tubes, increasing the risk of severe tubal damage. Studies on functional polymorphism in selected cytokine genes seem to contribute to the wide spectrum of disease manifestations and complications (Citation32).
Taken together these data suggest that the etiopathogenesis of chlamydial TFI is related to impaired CMI response caused by chlamydial HSP60-reactive T cells. We found that IL-10 promoter-1082 polymorphism plays an important role in regulating the antigen-specific CMI response during CT infection (Citation33). We also studied functional polymorphism in selected cytokine genes in women with TFI and controls. We found that the IL-10-1082 AA genotype and the TNF-α-308 A allele increased the risk of severe tubal damage (odds ratio 7.3, 95% CI 1.3–42 and 4.0, 95% CI 1.0–16, respectively), suggesting that differences in these genes contribute to the disease spectrum (Citation32).
Genetic studies of the immunopathogenetic factors will be continued in collaboration with the EpiGenChlamydia Consortium (http://www.epigenchlamydia.eu/) using SNP-Chip approaches. For instance, a single nucleotide polymorphism (SNP) in inflammasome-associated NLRP3 and miRNA-146A genes is associated with the severity of CT infection. The mutant NLRP3 A allele seems to be a risk factor for the development of PID in women with CT (Citation34).
IL-12 produced by monocytes, macrophages, and dendritic cells activates T cells and is required for the production of IFN-γ which is important in host defense against CT. A subunit IL-12p40 gene is polymorphic. We found that one of the six IL-12p40 SNPs (rs2853694) is under-represented in TFI (Citation35). This further supports our line of evidence that genetic factors play a key role in the immune response to CT. In the EpiGenChlamydia Consortium (www.epigenchlamydia.eu), several research groups collaborate on epidemiologic and immunogenetic studies on CT in order to move forward to effective chlamydia control both at the individual and population level.
Interaction between C. trachomatis and human papillomavirus (HPV)
A link between C. trachomatis and cervical atypia was reported already in the 1970s (Citation36,Citation37), and many subsequent studies have confirmed this association. Although human papillomavirus (HPV) is the necessary cause of cervical carcinoma, co-factors also may play an important role in cervical carcinogenesis. Seroepidemiologic studies have linked C. trachomatis and cervical squamous cell carcinoma (Citation38,Citation39). Such studies also suggest that the association is serovar-specific. Serotypes G, I, D, and B showed stronger association to cervical carcinoma than other serotypes. Antibody response to chlamydial HSP60 has been considered as a marker of persistent infection. Accordingly, CHSP-1 antibodies were associated with an increased risk for cervical squamous cell carcinoma, especially among those women with long lag time between chlamydial infection and diagnosis of cervical cancer (Citation40).
New molecular evidence now suggests that C. trachomatis induces centrosome amplification which may better explain the role of C. trachomatis in cervical carcinogenesis (Citation41). Interaction between CT and high-risk HPV types is biologically plausible since CT induces inflammation and metaplasia, and metaplastic cells are potential target cells for HPV. In addition, CT infection may increase access of HPV to the basal epithelium and increases HPV viral load. Also, CT modulates host immune response and inhibits apoptosis.
Although persistent high-risk HPV infection is necessary for the development of cervical cancer, only a small proportion of HPV infections persist, and an even smaller proportion progress to cervical neoplasia (Citation42). Therefore it is likely that co-factors such as CT play significant roles. This is also supported by our meta-analysis of longitudinal studies () (Citation43). This still needs to be demonstrated for high-grade cervical intraepithelial neoplasia (CIN2-3), the immediate precursor of cancer. We estimate that the population-attributable fraction for CT can be high as 20% in cervical neoplasia. This underlines the need to prevent both HPV infection (by vaccination) and CT infection (by screening and health education) in order to reduce or eradicate cervical neoplasia in young women.
Table II. Meta-analysis of longitudinal studies on Chlamydia trachomatis infection and cervical neoplasia (Citation43).
C. trachomatis and other disease conditions
It is certainly tempting to develop a hypothesis of a link between C. trachomatis infection and epithelial ovarian neoplasia or cancer. For instance, CT causes PID, the number of PID episodes increases the risk for epithelial ovarian cancer, PID causes infertility, PID is associated with elevated tumor marker CA-125 levels, and infertility drugs may increase the risk for ovarian cancer (). Although CT has been associated with ovarian cancer in some studies (Citation44), recent seroepidemiological studies do not support this (Citation45), and the organism has not been detected in ovarian tumor tissue, whether benign, border-line, or malignant (Citation46). Similarly, there is no association between CT antibodies and fallopian tube carcinoma (Citation47). One recent serologic case- control study demonstrated an interesting link between CT antibodies and polycystic ovary syndrome (PCOS), suggesting that chronic inflammation associated with chlamydial infection may contribute to the pathogenesis of PCOS (Citation48). However, further studies are needed.
Figure 3. Hypothetical model of an interaction between Chlamydia trachomatis, PID, and epithelial ovarian cancer.
Although CT is a common cause of endometritis, no association between CT and abnormal placentation such as placental abruption has been demonstrated (Citation49). Overall, the existing evidence linking CT to adverse pregnancy outcomes is relatively weak and mostly based on case-control studies. Serology has been often used for case ascertainment, and such studies cannot define the risk attributable to CT.
Large numbers of serologic studies have looked into the role of CT in male infertility, sperm quality, and IVF outcome, and the results have been highly variable (Citation50). There is no consensus about whether chlamydial antibody testing of male partners should be included in the infertility work-up. Chlamydial antibodies in the male partner may simply be a marker of TFI in the female partner. A case-control study of the associations between antichlamydial antibodies and male infertility among couples referred to a university hospital infertility clinic showed that the prevalence of IgG antichlamydial antibodies was higher among men from infertile couples than control men, and men with chlamydial antibodies had lower sperm counts than those without (Citation51). Defining the role of CT infection in male infertility requires further studies using tests measuring both humoral and cell-mediated immunity against CT (Citation52) in subfertile males, in addition to direct detection of apoptosis or DNA fragmentation in sperm.
Diagnosis
Besides identifying chlamydia by culture or by detecting parts of its membrane, C. trachomatis can be identified by detecting the nucleic acids (either DNA or RNA). In the past 25 years nucleic acid amplification tests (NAATs) have been developed. In these amplification tests the original amount of nucleic acid (either DNA or RNA) present in the clinical sample is multiplied. NAATs are far more sensitive than culture, EIA, and DFA. Due to the increased sensitivity NAATs generate 25%–40% more chlamydia-positive results as compared with cell culture (Citation53).
There has been rapid technical development in diagnostic testing for chlamydial genital infections. For example, urine-based screening tests, vulvar and vaginal swabs, and also self-sampling have proven accurate. Many recent well executed comparative studies of diagnostic tests, sampling procedures, or sampling media tests have been reported (Citation54,Citation55), and new tests have been evaluated (Citation56–58). Clearly gynecologic pelvic examination is not necessary for C. trachomatis screening of women.
A new genetic variant of C. trachomatis was discovered in Sweden in 2006. The variant has a 377-base-pair deletion in the plasmid which was the target for the commonly used NAATs in Sweden. So far the variant has been only occasionally detected outside Sweden or other Scandinavian countries (Citation59–61). In Gothenburg area, Sweden, 17% of positive specimens contained the new variant (Citation62). Many recent studies have focused on the new variant and disease syndromes associated with this variant. Not surprisingly, the clinical manifestations seem not to differ from the clinical manifestations caused by the wild-types (Citation63). Subsequently, NAATs have been modified so that this variant can now be detected by all NAATs commonly used in microbiology laboratories. The proportion of the new variant of CT in different counties in Sweden is getting relatively uniform now when new variant C. trachomatis (nvCT) is detected by all diagnostic tests used in Sweden (Citation64). This nvCT was studied in clinical specimens from four different geographical sites, two counties in Sweden, and Denmark and the Netherlands. The prevalence on nvCT in Sweden was approximately 13%, but only 0%–8% in Denmark, and 0% in the Netherlands (Citation65).
CT serology has been increasingly used in population-based studies and has proven useful in evaluating important on-going megatrends of CT prevalence and incidence rates at population level (Citation66). Therefore, serology has a new role in the evaluation of impact of CT screening programs at population level.
Different serological assays have been developed for the detection of antibodies to CT, including the complement fixation test, micro-immunofluorescence (MIF) assay, EIA, and immunoblotting. Little is known about antibody profiles during acute or chronic genital chlamydia infections. Superficial infections are considered to provide a poor stimulus for antibody formation. However, a correlation between antibody titers and the severity of tubal inflammation has been demonstrated (Citation67,Citation68). IgG antibodies persist for years (Citation69), even after antibiotic treatment (Citation70,Citation71), and are considered as markers of a past CT infection. IgM production is transient, and rises in IgM titers are infrequently found. Therefore, IgM titers are of no significance in diagnosing current or previous disease. Chlamydia IgG antibody testing in serum is applied in reproductive medicine in the fertility work-up (Citation68) but has no place in early diagnosis of chlamydia infection.
Treatment
Chlamydial infection is easily treated (). A single dose of azithromycin (1 g orally) is highly effective—more than 95% of those treated are negative for chlamydia after 2 weeks (Citation72). The single-dose option increases compliance. It is important to advise patients to avoid sexual contact during treatment and for 7 days afterwards to prevent reinfection before the treatment has been effective (). No test of cure is needed if treatment has been taken correctly and the advice to prevent reinfection has been followed. The exception is pregnant women who have a reduced cure rate because increased hepatic clearance results in lower plasma concentrations of erythromycin. Reinfection is 20–23 per 100 person years (Citation73), and the CDC recommends retesting after 3–4 months, although the English program does not (Citation74).
Figure 4. Chlamydia trachomatis screening program flow chart (modified from (Citation2)).
Table III. Treatment for Chlamydia trachomatis: current recommendations.
Partner notification is the process of informing sexual partners of people diagnosed with an STI about their potential exposure to infection. It aims to increase testing and treatment among partners who are at high risk, to prevent reinfection of the index case, and to prevent transmission in the community. This is an important part of the management of any STI.
Prevention
Any public health approach to preventing and controlling sexually transmitted infections must promote safer sexual behavior, encourage early health care-seeking behavior, and introduce prevention and care activities across all primary health care providers.
Screening remains important in limiting the reproductive rate and complications of chlamydial genital infection. Early antimicrobial treatment of infected individuals reduces transmission by shortening the average duration of infection. Prevention efforts can be primary, secondary, or tertiary. Primary prevention by education and behavior change has not proved very effective. Primary prevention by vaccination is problematic since the development of a C. trachomatis vaccine still is a major challenge (Citation75,Citation76). Search for a vaccine with protective and not harmful effects is a complex task for the future. More basic research is needed on immune correlates of protection against CT and the disease pathogenesis.
Internationally a variety of control approaches have been used. Few organized programs exist nationally (Citation10), and those that do range from opportunistic screening, such as the English national chlamydia screening program and the US infertility prevention program, to an internet-based register that is being piloted in the Netherlands.
According to European Centre for Disease Prevention and Control (ECDC), six other European countries offer opportunistic testing—Denmark, Estonia, Iceland, Latvia, Norway, and Sweden (Citation77). The US Centers for Disease Control and prevention (CDC) recommends that all sexually active women aged 25 years and younger should be screened for chlamydia ().
It is extremely disturbing that despite emerging screening recommendations and increasing screening activity CT case rates reported are on the rise again. For instance, in Finland there has been a 60% increase of CT infections during the past 10 years. Thus, there is major frustration with opportunistic or organized screening programs, implementation of management guidelines, and contact-tracing efforts. Core group hypothesis and high reinfection rates (Citation19,Citation78,Citation79) have been proposed to explain the discrepancy. Also so-called arrested immunity (Citation80) associated with early therapy may leave individuals susceptible to reinfection by preventing the development of protective immunity. Indeed reinfection rates have been rapidly increasing in some countries, for instance Canada, the United States, and England. One study showed that of repeat infections among adolescent women tested every 3 months, 84% were definite, probable, or possible reinfections, 14% were probable or possible treatment failures, and 2% persisted without documented treatment (Citation19). Although CT seroprevalence rates have decreased, the incidence rates based on seroconversions or reported laboratory notifications of diagnosed CT infections have increased (Citation81). The discrepancy between the CT incidence and seroprevalence trends warrants further study.
Tertiary prevention means more effective management and antimicrobial therapy. This is currently not a problem since CT remains susceptible to azithromycin, which has excellent intracellular tissue penetration and is the best single-dose agent for treatment of chlamydial infection in men and women. Single-dose therapy is particularly important in adolescents and asymptomatic individuals in general. There have been surprisingly few reports of azithromycin resistance in CT.
Another innovation is so-called expedited treatment of sex partners through patient-delivered partner therapy which certainly reduces rates of persistent or recurrent chlamydial infection (Citation82). Novel interventions such as postal testing kits and patient- delivered partner therapy also offer other advantages including simplicity and lower cost (Citation83).
The internet is becoming a platform that is used more frequently for testing of STI (Citation84). STI-testing services are available from the internet, and several sites offer kits for at-home testing. However, it is still difficult for consumers to contact these sites. Often internet-solicited STI results are not accurate. FDA clearance of self-collected urogenital swab specimens at home is required. Regulatory control is needed to protect internet consumers from receiving inaccurate results. With regulation, internet services could provide accurate results in a confidential manner for those who are reluctant to use clinics for routine STI testing.
Key messages
Many lessons have been learnt since the 1970s when the wide spectrum of clinical manifestations of C. trachomatis infections was described. However, there are still many unanswered questions and major defects in our understanding of the biology of this intracellular micro-organism. Undoubtedly, secondary prevention and current screening programs are important steps toward limiting the complications of chlamydial genital infection, although these program efforts are likely to have more individual than public health impact. More research on the effectiveness of C. trachomatis screening programs is needed, and the question still remains: Are we doing enough? Nonetheless, the benefit to individual patients of testing and appropriate treatment is indisputable, and we recommend that chlamydia testing be offered routinely to young people as part of an approach to sexual health in primary care.
Declaration of interest: The author's work is in part supported by Helsinki University Hospital Research Grants and the European Commission within the Sixth Framework Programme through the EpiGenChlamydia project (contract no. LSHG-CT-2007-037637). See www.EpiGenChlamydia.eu for more details.
References
- Land JA, Van Bergen JEAM, Morre SA, Postma MJ. Epidemiology of Chlamydia trachomatis infection in women and the cost-effectiveness of screening. Hum Reprod Update. 2010:16:189–204.
- Kalwij S, Macintosh M, Baraitser P. Screening and treatment of Chlamydia trachomatis infections. BMJ. 2010;340:912–7.
- ECDC Guidance: Chlamydia control in Europe, 2009. Available at: www.ecdc.europa.eu. (Accessed date: 29 December 2010).
- Morre SA, Rozendaal L, Van Valkengoed IG, Boeke AJ, Van Voorst Vader PC, Schirm J, . Urogenital Chlamydia trachomatis serovars in men and women with a symptomatic or asymptomatic infection: an association with clinical manifestations? J Clin Microbiol. 2000;38:2292–6.
- Wilson JS, Honey E, Templeton A, Paavonen J, Mårdh PA, Stary A, .; EU Biomed Concerted Action Group. A systematic review of the prevalence of Chlamydia trachomatis among European women. Hum Reprod Update. 2002;28: 385–94.
- van Bergen J, Spaargaren J, Götz HM, Veldhuijzen IK, Bindels PJE, Coenen TJ, .; the PILOT CT study-group. Population prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae in the Netherlands. BMC Infect Dis. 2006;6:42.
- van Bergen J, Gotz HM, Richardus JH, Hoebe CJ, Broer J, Coenen AJ. Prevalence of urogenital Chlamydia trachomatis increases significantly with level of urbanisation and suggests targeted screening approaches: results from the first national population based study in the Netherlands. Sex Transm Infect. 2005;81:17–23.
- Andersen B, Olesen F, Moller JK, Ostergaard L. Population-based strategies for outreach screening of urogenital Chlamydia trachomatis infections: a randomized, controlled trial. J Infect Dis. 2002;185:252–8.
- Macleod J, Salisbury C, Low N, McCarthy A, Sterne JA, Holloway A, . Coverage and uptake of systematic postal screening for Chlamydia trachomatis and prevalence of infection in the United Kingdom general population: cross sectional study. BMJ. 2005;330:940–2.
- Low N; the SCREen project team. Publication report on chlamydia control activities in Europe. Euro Surveill. 2008; 13: pii: 18924.
- Tu W, Batteiger B, Wiehe S, Ofner S, Van Der Pol B, Katz BP, . Time from first intercourse to first sexually transmitted infection diagnosis among adolescent women. Arch Pediatr Adolesc Med. 2009;163:1106–11.
- Centers for Disease Control and Prevention (CDC). Chlamydia screening among sexually active young female enrollees of health plans—United States, 2000–2007. MMWR Morb Mortal Wkly Rep. 2009;58:362–5.
- Aral SO, Fenton KA, Holmes KK. Sexually transmitted disease in the USA. Temporal trends. Sex Transm Infect. 2007;83:257–66.
- Paavonen J; FUTURE II Study Group. Baseline demographic characteristics of subjects enrolled in international quadrivalent HPV (types 6/11/16718) vaccine trials. Curr Med Res Opin. 2008;24:1–12.
- Paavonen J, Naud P, Salmerón J, Wheeler CM, Chow SN, Apter D, . Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA). Final analysis of a double-blind, randomised study in young women. Lancet. 2009;374:301–14.
- Egger M, Low N, Smith GD, Lindblom B, Hermann B. Screening for chlamydial infections and the risk of ectopic pregnancy in a county in Sweden: ecological analysis. BMJ. 1998;316:1776–80.
- Simms I, Talebi A, Rhia J, Horner P, French RS, Sarah R, . The English National Screening Programme: variation in positivity in 2007/2008. Sex Transm Dis. 2009;36: 522–7.
- Franklin N, O’Connor CC, Shaw M, Guy R, Grulich A, Fairley CK, . Chlamydia at an inner metropolitan sexual health clinic Sydney, NSW; the Australain collaboration for chlamydia enhanced sentinal surveillance (ACCESS) Project. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Hof bei Salzburg, Austria, 20–25 June 2010. 413.
- Batteiger BE, Tu W, Ofner S, Van Der Pol B, Stothard D, Orr DP, . Repeated Chlamydia trachomatis genital infections in adolescent women. J Infect Dis. 2010;201:42–51.
- Lyytikäinen E, Kaasila M, Koskela P, Lehtinen M, Patama T, Pukkala E, . Chlamydia trachomatis seroprevalence atlas of Finland 1983–2003. Sex Transm Infect. 2008; 84: 19–22.
- Kretzshmar M, Turner KME, Barton PM, Edmunds WJ, Low N. Predicting the population impact of chlamydia screening programmes: comparative mathematical modelling study. Sex Transm Infect. 2009;85:359–66.
- Hu D, Hook EW III, Goldie SJ. Screening for Chlamydia trachoamatis in women 15 to 29 years of age: a cost- effectiveness analysis. Ann intern Med. 2004;141:501–14.
- Adams EJ, Tirner KME, Edmonds WJ. The cost effective ness of opportunistic Chlamydia screening in England. Sex Transm Inf. 2007;83:267–75.
- De Vries R, Van Bergen JEAM, De Jong-van den Berg LTW, Postma PJ; the PILOT-CT study Group. Cost-utility of repeated screening for Chlamydia trachomatis. Value Health. 2008;11:272–4.
- Paavonen J. Memorable Chlamydia trachomatis papers. Sex Transm Infect. 2000;76:S30–2.
- Wiesenfeld H, Paavonen J. Pelvic inflammatory disease. Morse SA, Ballard RC, Holmes KK, Moreland A. Atlas of sexually transmitted disease and AIDS. 4th. London, UK: Elsevier Ltd. 2010, 94–110. In press.
- van Valkengoed I, Morré S, van den Brule A, Meijer CJ, Bouter LM, Boeke AJ. Overestimation of complication rates in evaluations of Chlamydia trachomatis screening programmes—implications for cost-effectiveness analyses. Int J Epidemiol. 2004;33:416–25.
- Low N, Egger M, Sterne JA, Harbord RM, Ibrahim F, Lindblom B, . Incidence of severe reproductive tract complications associated with diagnosed genital chlamydial infection: the Uppsala Women's Cohort Study. Sex Transm Infect. 2006;82:212–8.
- Bakken IJ, Ghaderi S. Incidence of pelvic inflammatory disease in a large cohort of women tested for Chlamydia trachomatis: a historical follow-up study. BMC Infect Dis. 2009;9:130–4.
- Bjartling C, Osser S, Persson K. Chlamydia trachomatis is still in common in pelvic inflammatory disease in the south of Sweden. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Hof bei Salzburg, Austria, 20–25 June 2010. 389.
- Mårdh P-A, Ripa T, Svensson L, Weström L. Chlamydia trachomatis infection in patients with acute salpingitis. N Engl J Med. 1977;296:1377–9.
- Öhman H, Tiitinen A, Halttunen M, Lehtinen M, Paavonen J, Surcel HM. Cytokine polymorphisms and severity of tubal damage in women with chlamydia-associated infertility. J Infect Dis. 2009;199:1353–9.
- Öhman H, Tiitinen A, Halttunen M, Birgelund S, Christiansen G, Koskela P, . IL-10 polymorphism and cell mediated immune response to chlamydia trachomatis. Genes Immun. 2006;7:243–9.
- Wang W, Stassen FR, Surcel H-M, Öhman H, Tiitinen A, Paavonen J, . Analyses of polymorphism in inflammasome-associated NLRP3 and miRNA-146A genes in the susceptibility to and tubal pathology of Chlamydia trachomatis infection. Drugs Today (Barc). 2009;45, Suppl B: 95–103.
- Öhman H, Bailey R, Natividad A, Tiitinen A, Halttunen M, Paavonen J, . Il-12p40 polymorphisms and C. trachomatis specific lymphocyte proliferative responses. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Salzburg, Austria, 20–25 June 2010. Abstract. 169–72.
- Schachter J, Hill EC, King EB, Coleman VR, Jones P, Meyer KF. Chlamydia infection in women with cervical dysplasia. Am J Obstet Gynecol. 1975;123:753–7.
- Paavonen J, Vesterinen E, Meyer B, Saikku P, Suni J, Purola E, . Genital Chlamydia trachomatis infections in patients with cervical atypia. Obstet Gynecol. 1979;54:289–91.
- Koskela P, Anttila T, Björge T, Brunsvig A, Dillner J, Hakama M, . Chlamydia trachomatis infection and invasive cervical cancer. Int J Cancer. 2000;85:35–9.
- Anttila T, Saikku P, Koskela P, Bloigu A, Dillner J, Ikäheimo I, . Serotypes of Chlamydia trachomatis and risk for cervical squamous cell carcinoma. JAMA. 2001;285: 47–51.
- Paavonen J, Karunakaran KP, Noguchi Y, Anttila T, Bloigu A, Dillner J, . Serum antibody response to the heat shock protein 60 of Chlamydia trachomatis in women with developing cervical cancer. Am J Obstet Gynecol. 2003; 189:1287–92.
- Johanson KA, Chen AL, Tan M, Sütterlin C. The role of the protease CPAF in chlamydia-induced centronome amplification. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, Hof bei Salzburg, Austria, 20–25 June 2010. Oral presentation.
- Schiffman M, Castle PE, Jeronimo J, Rodriguez A, Wacholder S. Human papillomavirus and cervical cancer. Lancet. 2007;370:890–907.
- Lehtinen M, Lyytikäinen E, Koskela P, Surcel H-M, Paavonen J. Chlamydia trachomatis and risk for cervical neoplasia—a meta-analysis of longitudinal studies. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Salzburg, Austria, 20–25 June 2010. Abstract. 445–8.
- Risch HA, Howe GR. Pelvic inflammatory disease and the risk of epithelial ovarian cancer. Cancer Epidemiol Biomarkers Prevent. 1995;4:447–51.
- Ness RB, Shen C, Bass, Jackson C, Moysich K, Edwards R, . Chlamydia trachomatis serology in women with and without ovarian cancer. Infect Dis Obstet Gynecol. 2008; 16:1–5.
- Idahl A, Lundin E, Elgh F, Jurstrand M, Møller JK, Marklund I, . Chlamydia trachomatis, Mycoplasma genitalium, Neisseria gonorrhoeae, human papillomavirus, and polyomavirus are not detectable in human tissue with epithelial ovarian cancer, borderline tumor, or benign conditions. Am J Obstet Gynecol. 2010;202:71.e1–6.
- Riska A, Finne P, Alfthan H, Anttila T, Jalkanen J, Sorvari T, . Past chlamydial infection is not associated with primary fallopian tube carcinoma. Eur J Cancer. 2006;42:1835–8.
- Morin-Papunen L, Duleba A, Bloigu A, Järvelin MR, Saikku P, Pouta A. Chlamydia antibodies and self-reported symptoms of oligo-amenorrhea and hirsutism: a new etiologic factor in polycystic ovary syndrome. Fertil Steril. 2010;94: 1799–804.
- Tikkanen M, Surcel H-M, Boigu A, Nuutila M, Hiilesmaa V, Ylikorkala O, . Prediction of placental abruption by testing for C-reactive protein and chlamydial antoibody levels in early pregnancy. BJOG. 2008;115:486–91.
- Paavonen J, Eggert-Kruse W. Chlamydia trachomatis infection—impact on human reproduction. Hum Reprod Update. 1999;5:433–47.
- Joki-Korpela P, Sahrakorpi N, Halttunen M, Surcel HM, Paavonen J, Tiitinen A. The role of Chlamydia trachomatis in male infertity. Fertil Steril. 2009;91:S1448–50.
- Tiitinen A, Surcel H-M, Halttunen M, Birkelund S, Bloigu A, Christiansen G, . Chlamydia trachomatis and chlamydial heat shock protein 60-specific antibody and cell-mediated responses predict tubal factor infertility. Hum Reprod. 2006;21:1533–8.
- Jespersen DJ, Flatten KS, Jones MF, Smith TF. Prospective comparison of cell culture and nucleic acid amplification tests for laboratory diagnosis of Chlamydia trachomatis infections. J Clin Microbiol. 2005;43:5324–6.
- Chernesky M, Jang D, Smieja M, Portillo E, Ewert R, Pritchard C, . Validation of the APTIMA Combo 2 assay for the detection of Chlamydia trachomatis and Neisseria gonorrhoeae in SurePath liquid-based pap test samples taken with different collection devices. Sex Transm Dis. 2009;36:581–3.
- Masek BJ, Arora N, Quinn N, . Performance of three nucleic acid amplification tests for detection of Chlamydia trachomatis and Neisseria gonorrhoeae by use of self- collected vaginal swabs obtained via an internet-based screening program. J Clin Microbiol. 2009;47:1663–7.
- Quint K, Porras C, Safaeian M, González P, Hildesheim A, Quint W, . Evaluation of a novel PCR-based assay for detection and identification of Chlamydia trachomatis serovars in cervical specimens. J Clin Microbiol. 2007;45:3986–91.
- Quint K, van Doorn L-J, Kleter B, de Koning MN, van den Munckhof HA, Morre SA . A highly sensitive, multiplex broad-spectrum PCR-DNA-enzyme immunoassay and reverse hybridization assay for rapid detection and identification of Chlamydia trachomatis serovars. J Mol Diagn. 2007;9:631–8.
- Mahilum-Tapay L, Laitila V, Wawrzyniak JJ, Lee HH, Alexander S, Ison C, . New point of care Chlamydia Rapid Test—bridging the gap between diagnosis and treatment: performance evaluation study. BMJ. 2007;335: 1190–4.
- Morré SA, Catsburg A, de Boer M, Spaargaren J, de Vries HJ, Schirm J, . Monitoring the potential introduction of the Swedish Chlamydia trachomatis variant (swCT) in the Netherlands. Euro Surveill. 2007;12:318–20.
- de Barbeyrac B, Raherison S, Cado S, Normandin F, Clerc M, Clairet V, . French situation concerning the Swedish Chlamydia trachomatis variant. Euro Surveill. 2007;12:321–2.
- Reischl U, Straube E, Unemo M. The Swedish new variant of Chlamydia trachomatis (nvCT) remains undetected by many European laboratories as revealed in the recent PCR/NAT ring trial organised by INSTAND e.V., Germany. Euro Surveill. 2009; 14; pii: 19302.
- Lagergård T, Hadad R, Tunbäck P, Lindholm L, Löwhagen GB, Unemo M. Distribution of Chlamydia trachomatis ompA genovars and the new variant of C. trachomatis in the Göteborg area, Sweden. Eur J Clin Microbiol Infect Dis. 2010;29:609–11.
- Bjartling C, Osser S, Johnsson A, Persson K. Clinical manifestation and epidemiology of the new genetic variant of chlamydia trachomatis. Sex Transm Dis. 2009;36:529–35.
- Christerson L, Klint M, Hadad R, Lor B, Anagrius C, Österlund A, . The proportion of the new variant of Chlamydia trachomatis is converging in Sweden counties over time. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Hof bei Salzburg, Austria, 20–25 June 2010. 401.
- Clarke IN, Hammas B, Beerens AMJ, Luijt DS, Westh H, Nilsson P, . Detection and spread of new variant Chlamydia trachomatis in northern European countries. Proceedings of the Twelfth International Symposium on Human Chlamydial Infections, International Chlamydia Symposium, Hof bei Salzburg, Austria, 20–25 June 2010. 397.
- Johnson AM, Horner P. A new role for Chlamydia trachomatis serology. Sex Transm Infect. 2008;84:79–80.
- Traharne JD, Ripa KT, Mårdh PA, Svensson L, Weström L, Darougar S. Antibodies to Chlamydia trachomatis in acute salpingitis. Br J Vener Dis. 1979;55:26–9.
- Akande VA, Hunt LP, Cahill DJ, Caul EO, Ford WCL, Jenkins JM. Tubal damage in infertile women: prediction using chlamydia serology. Hum Reprod. 2003;18:1841–7.
- Gijsen AP, Land JA, Goossens VJ, Slobbe MEP, Bruggeman CA. Chlamydia antibody testing in screening for tubal factor subfertility: the significance of IgG antibody decline over time. Hum Reprod. 2002;17:699–703.
- Piura B, Sarov B, Sarov I. Persistance of antichlamydial antibodies after treatment of acute salpingitis with doxycycline. Eur J Obstet Gynecol Reprod Biol. 1993;48:117–21.
- Henry-Suchet J, Askienay-Elbhar M, Thibon M, Revol C, Akue BA. The post-therapeutic course of serum antibody titres in women with acute salpingitis and tubal infertility. Fertil Steril. 1994;62:296–304.
- Tobin JM, Harinda V, Mani R. Which treatment for genital tract Chlamydia trachomatis infection? Int J STD AIDS. 2004;15:737–9.
- Lamontagne S, Baster K, Emmett L, Nichols T, Randell S, McLean L, . Incidence and reinfection rates of genital chlamydial infection among women aged 16–24 years attending general practice, family planning and genitourinary medicine clinics in England: a prospective cohort study by the Chlamydia Recall Study Advisory Group. Sex Transm Infect. 2007;83:292–303.
- Centers for Disease Control and Prevention. Chlam ydia screening fact sheet. Available at: www.cdc.gov/std/Chlamydia/STDFact-Chlamydia.htm.
- Igietseme JU, He Q, Joseph K, Eko FO, Lyn D, Ananaba G, . Role of T lymphocytes in the pathogenesis of chlamydia disease. J Infect Dis. 2009;200:926–34.
- Brunham RC, Rey-Ladino J. Immunology of Chlamydia infection: implications for a Chlamydia trachomatis vaccine. Nature. 2005;5:149–61.
- European Centre for Disease Prevention and Control. Chlamydia control in Europe. Available at: 2009. wwwecdc.europa.eu/en/publications/Publications(0906_GUI_Chlamydia_Control_in_Europe.pdf.
- Gaydos CA, Wright C, Wood B, Waterfield G, Hobson S, Quinn TC. Chlamydia trachomatis reinfection rates among female adolescents seeking rescreening in school-based health centers. Sex Transm Dis. 2008;35:233–7.
- Fung M, Scott K, Kent C, Klausner JD. Chlamydial and gonococcal reinfection among men: a systematic review of data to evaluate the need for retesting. Sex Transm Infect. 2007;83:304–9.
- Brunham R, Rekart M. The arrested immunity hypothesis and the epidemiology of chlamydia control. Sex Transm Dis. 2008;35:53–4.
- Lyytikäinen E, Kaasila M, Hiltunen-Back E, Lehtinen M, Tasanen K, Surcel HM, . A discrepancy of Chlamydia trachomatis incidence and prevalence trends in Finland 1983–2003. BMC Infect Dis. 2008;8:169–74.
- Golden MR, Whittington WL, Handsfield HH, Hughes JP, Stamm WE, Hogben M, . Effect of expedited treatment of sex partners on recurrent or persistent gonorrhea or chlamydial infection. N Engl J Med. 2005;352:676–85.
- Cameron ST, Glasier A, Scott G, Young H, Melvin L, Johnstone A, . Novel interventions to reduce re-infection in women with chlamydia: a randomized controlled trial. Hum Reprod. 2009;24:888–95.
- Owens SL, Arora N, Quinn N, Peeling RW, Holmes KK, Gaydos CA. Utilising the internet to test for sexually transmitted infections: results of a survey and accuracy testing. Sex Transm Infect. 2010;86:112–6.
- Arnheim L. Immunological responses in genital HPV infections and etiology of cervical cancer. Thesis. Stockholm: Karolinska Institute; 2005.
- Lehtinen M, Dillner J, Knekt P, Luostarinen T, Aromaa A, Kirnbauer R, . Serologically diagnosed infection with human papillomavirus type 16 and risk for subsequent development of cervical carcinoma: nested case-control study. BMJ. 1996;312:537–9.
- Naucler P, Chen H-C, Persson K, You SL, Hsieh CY, Sun CA, . Seroprevalence of human papillomavirus and Chlamydia trachomatis and cervical cancer risk: nested case-control study. J Gen Virol. 2007;88:814–22.
- Koutsky LA, Holmes KK, Critchlow CW, Stevens CE, Paavonen J, Beckmann AM, . A cohort study of the risk of cervical intraepithelial neoplasia grade 2 or 3 in relation to papillomavirus infection. N Engl J Med. 1992;327:1272–8.
- Lehtinen M, Ault K, Lyytikäinen E, Dillner J, Garland SM, Ferris DG, . Chlamydia trachomatis infection and risk of cervical intraepithelial neoplasia. Sex Transm Infect. In press.
- Samoff E, Koumans EH, Markowitz LE, Sternberg M, Sawyer MK, Swan D, . Association of Chlamydia trachomatis with persistence of high-risk of human papillomavirus in a cohort of female adolescents. Am J Epidemiol. 2005;162:668–75.
- Silins I, Ryd W, Strand A, Törnberg S, Hansson BG, Wang X, . Chlamydia trachomatis infection and persistence of human papillomavirus. Int J Cancer. 2005;116:110–5.

