
Abstract
A key function of human skin is the formation of a structural barrier against the external environment. In part, this is achieved through the formation of a cornified cell envelope derived from a stratified squamous epithelium attached to an epithelial basement membrane. Resilient in health, the structural integrity of skin can become impaired or break down in a collection of inherited skin diseases, referred to as the blistering genodermatoses. These disorders arise from inherited gene mutations in a variety of structural and signalling proteins and manifest clinically as blisters or erosions following minor skin trauma. In some patients, blistering can be severe resulting in significant morbidity. Furthermore, a number of these conditions are associated with debilitating extra-cutaneous manifestations including gastro-intestinal, cardiac, and ocular complications. In recent years, an improved understanding of the molecular basis of the blistering genodermatoses has led to better disease classification and genetic counselling. For patients, this has also advanced translational research with the advent of new clinical trials of gene, protein, cell, drug, and small molecule therapies. Although curing inherited blistering skin diseases still remains elusive, significant improvements in patients’ quality of life are already being achieved.
Key words::
Key messages
Skin blisters can develop as a consequence of trauma, infection, autoimmune disease, or gene mutations that target a variety of proteins involved in maintaining the structural integrity and resilience of human skin. With regard to the genetic pathologies, molecular dissection of the inherited blistering skin diseases has identified at least 18 candidate genes that encode key structural and signalling proteins involved in cell-cell and cell-matrix adhesion and which have important roles in both health and disease.
The expanding spectrum of pathogenic mutations in skin adhesion genes and the protean nature of inherited blistering skin diseases have led to the re-classification of this group of diseases, a major revision to the established paradigms for genotype-phenotype correlation, and the discovery of several new clinicopathological entities.
New molecular discoveries have generated substantial clinical benefits for patients in terms of more accurate diagnoses, improved genetic counselling, the development of prenatal testing, and considerable translational research activity, with clinical trials of gene and cell-based therapies, including whole bone marrow transplantation for certain severe life-threatening inherited blistering skin diseases.
Introduction
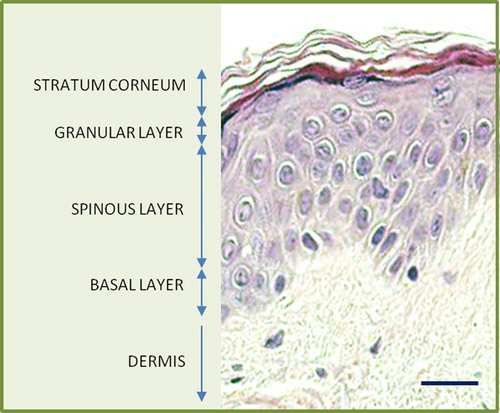
Human skin is the body's largest organ, covering a surface area of up to 2 m2 and providing a mechanical and immunological barrier against the external environment. Structurally, the outer layer of the skin, the epidermis, consists of a stratified squamous epithelium that, in healthy skin, is constantly renewed every 50–70 days () (Citation1). Epidermal keratinocytes differentiate to form corneocytes with a robust cell envelope, which, in combination with extracellular lipids, amino acids, and water, form an impervious cutaneous barrier (Citation2). Keratinocytes are structurally linked to epidermal basement membrane and neighbouring cells via cell-cell junctions, predominantly hemidesmosomes and desmosomes, respectively (Citation3,Citation4). Secure keratinocyte adhesion and intricate signalling pathways are required both to withstand external trauma and to ensure normal skin homeostasis. In some individuals, however, the resilience of the skin as a protective barrier is lost. Defective skin can arise because of trauma or infections or autoantibodies targeting adhesion proteins in the skin, but another possible aetiology is inherited mutations in the genes encoding proteins involved in maintaining skin integrity. Such patients experience epithelial fragility, blisters and erosions following relatively minor skin trauma; this group of diseases is known as epidermolysis bullosa (EB) (Citation5). Over the last 20 years, mutations in at least 18 distinct genes have been identified in EB encoding key adhesive, signalling, or transport proteins in the skin (Citation6). Knowledge of these mutations in humans, in combination with new in vitro and animal models, has improved our understanding of disease pathogenesis and led to new opportunities for translational research and clinical trials of novel therapies.
Figure 1. Histology of normal human skin (haematoxylin and eosin; scale bar = 25 μm).
This review will explore two main topics: recent discoveries in our understanding of blistering genodermatoses with emphasis on the molecular mechanisms underlying disease, as well as current and future therapies aimed at correcting the skin abnormalities and improving patient quality of life.
Epidermolysis bullosa
EB comprises a group of phenotypically diverse blistering genodermatoses which affect the skin and, in some subtypes, mucous membranes and other organ systems (Citation5). In most forms of EB, light microscopy shows blistering at or close to the junction between the epidermis and the dermis (known as the dermal-epidermal junction) (). Traditionally, EB is classified into three main subtypes depending on the level of blister formation within the cutaneous basement membrane zone or epidermis, as determined by transmission electron microscopy (Citation7). Tissue separation occurs in the basal keratinocyte layer in EB simplex (EBS), within the lamina lucida of the basement membrane in junctional EB (JEB), and in the superficial dermis in dystrophic EB (DEB). The clinical spectrum of EB, however, which was last updated in 2008, extends to 30 possible clinical subtypes with inherent genetic defects in at least 13 different genes (Citation1). Such is the progress of gene discovery, however, that more recent literature has extended the basis of inherited skin blistering to 18 candidate genes—some of which fall into the classical clinicopathological subtyping of EB, while others raise new issues about what precisely should be included in the classification of EB (; and ) (Citation6).
Figure 2. Light microscopic appearances of inherited skin fragility at either the dermal-epidermal junction (A) or within the lower epidermis (B). Asterisk indicates the blister formation (Richardson's stain; scale bar = 50 μm).
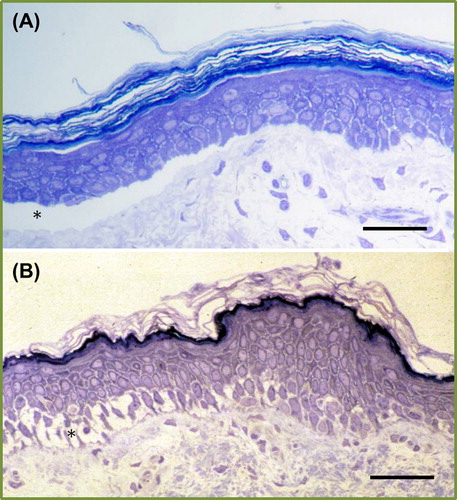
Figure 3. Stylized diagram depicting the important components in the skin that provide the keratinocyte, cell-cell, and cell-extracellular matrix integrity along with the protein components that are mutated in inherited skin fragility diseases.
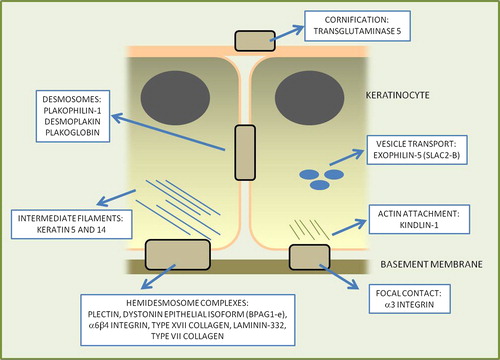
Figure 4. Clinical illustrations of different genetic disorders showing varying degrees of skin fragility. In each case the mutated skin protein is shown.

Table I. Summary of the gene and protein targets and disease phenotypes in the inherited skin fragility disorders.
Established EB disorders
Keratins 5 and 14: KRT5, KRT14
Keratins are the most abundant structural proteins in the cytoplasm of epithelial cells, forming a network of 10-nm intermediate filaments (Citation8). The keratin filament network helps maintain the shape of keratinocytes by providing both structural stability and flexibility (Citation9). Many keratin isoforms exist, with keratin 5 and 14 representing the major keratins in basal keratinocytes (Citation10). Autosomal dominant mutations in KRT5 or KRT14 underlie the most common EB subtype, EBS localized to hands and feet (OMIM 131800), a condition affecting ˜8000 people in the UK (Citation11). EBS results in minor blistering that is usually worse in the summer months and which does not result in scarring. There are several other clinical variants of EBS that also result from KRT5 or KRT14 mutations; most of these are dominant, but autosomal recessive mutations in KRT14 have also been reported (Citation12).
Plectin: PLEC
Plectin is an epidermal plakin protein, also found within the z-lines of striated muscle (Citation13). Although present throughout much of the epidermis, in basal keratinocytes it plays a key role in linking the keratin filament network to hemidesmosomes at the plasma cell membrane (Citation14). Autosomal recessive mutations in PLEC cause EBS associated with muscular dystrophy (OMIM 226670), which manifests as relatively minor skin blistering and progressive muscle weakness (Citation15,Citation16). Autosomal recessive mutations in PLEC can also cause skin blistering with pyloric atresia (OMIM 612138), or, occasionally, all three manifestations (Citation17). Autosomal dominant mutations in plectin may also occur in other forms of EBS, including the Ogna subtype (OMIM 131950); these cases do not usually have extra-cutaneous features (Citation18).
α6β4 Integrin: ITGA6, ITGB4
Integrins represent a family of cell adhesion receptors that have important roles in ligand binding and signalling; the α6β4 integrin is involved in hemidesmosome assembly and in epithelial-mesenchymal signalling (Citation19,Citation20). Mutations in ITGA6 or ITGB4 have been shown to result in autosomal recessive JEB associated with pyloric atresia (OMIM 226730) (Citation21). The clinical severity of both the skin fragility and degree of gastric outflow obstruction in this condition can vary, but surgical correction of the pylorus is usually required. More severe forms of the disease usually result from loss-of-function mutations on both alleles of ITGA6 or ITGB4, although missense mutations in certain critical cysteine residues may also have devastating clinical consequences (Citation22). Other missense mutations can result in different forms of JEB, known as non-Herlitz disease (OMIM 226650) (Citation23).
Laminin-332: LAMA3, LAMB3, LAMC2
Laminin-332, previously known as laminin-5, is a heterotrimeric protein consisting of α3, β3, and γ2 laminin polypeptide chains located within the lamina lucida/lamina densa of the epidermal basement membrane (Citation24). Autosomal recessive mutations affecting both alleles of any of the three genes can give rise to Herlitz or non-Herlitz JEB (Citation25). Herlitz disease (OMIM 226700) is the most severe form of EB, often resulting in widespread muco-cutaneous fragility and a poor prognosis, with most affected individuals not surviving beyond infancy (Citation26). Non-Herlitz JEB is usually associated with mutations that allow for some residual functional laminin-332 protein and is clinically milder (Citation27). Mutations in the LAMA3A isoform of the LAMA3 gene are associated with a form of JEB known as laryngo-onycho-cutaneous syndrome (OMIM 245660), in which excessive granulation tissue can develop, leading to laryngeal obstruction and blindness (Citation28).
Type XVII collagen: COL17A1
Type XVII collagen, also known as the 180-kDa bullous pemphigoid antigen, is a transmembranous protein located within the hemidesmosome and lamina lucida (Citation29). It is the antigenic target in the autoimmune blistering disease, bullous pemphigoid (Citation30), but loss-of-function mutations on both alleles result in non-Herlitz JEB (Citation31). The finding that a complete loss of type XVII collagen results in a less severe blistering disease than complete loss of laminin-332 provides some physiological insight into the respective contributions of these two proteins in normal epidermal-dermal cohesion (Citation27). Some dominant missense mutations in type XVII collagen may result in defective dental enamel and occasionally skin fragility (Citation32,Citation33), but most pathogenic mutations in COL17A1 are autosomal recessive.
Type VII collagen: COL7A1
Type VII collagen is the major component of anchoring fibrils (Citation34). These adhesion complexes insert into the dermal side of the lamina densa and are traversed by dermal collagen fibres to provide adhesion between the epidermis and dermis (Citation35). Mutations in COL7A1 underlie both autosomal dominant and autosomal recessive forms of DEB. Typically, loss-of-function mutations on both alleles of COL7A1 underlie the severe generalized forms of recessive DEB (OMIM 226600), where affected individuals develop widespread trauma-induced blistering (Citation36). Poor wound healing results in chronic wounds, mutilating scar formation, and an increased incidence of early, aggressive cutaneous malignancy (Citation37). However, there is a spectrum of clinical severity in recessive DEB with some less disruptive mutations giving rise to less severe phenotypes (Citation38). Dominant DEB (OMIM 131750) is usually clinically milder than recessive disease, and most cases result from heterozygous missense mutations within the type VII collagen triple helix (Citation39).
Kindlin-1: KIND1
Kindlin-1 is a component of different cell-matrix complexes at the dermal-epidermal junction, focal contacts, which are important in cell migration (Citation40). Kindlin-1, which is also known as fermitin family homologue-1, and the KIND1 gene as FERMT1, is associated with anchorage of the actin cytoskeleton to focal contacts and formation of a signalling platform via β1 integrin (Citation41). Autosomal recessive mutations in KIND1 result in Kindler syndrome (OMIM 173650), a blistering genodermatosis that may resemble DEB in early life (Citation42,Citation43). With increasing age, the blistering often diminishes, and affected individuals exhibit photosensitivity and poikiloderma (a combination of hyperpigmentation, hypopigmentation, telangiectases, and skin atrophy) (Citation44). Individuals with Kindler syndrome may also have an increased risk of cutaneous malignancy (squamous cell carcinoma) (Citation44).
Plakophilin-1: PKP1
Inherited skin fragility has also been shown to result from mutations in desmosome cell-cell junctions (Citation45). Desmosomes form structural and signalling links between adjacent keratinocytes but are also found in cardiac myocytes, the meninges, and the cortex of lymph nodes (Citation46). Plakophilin-1 has a restricted localization to keratinocyte desmosomes, and autosomal recessive loss-of-function mutations in PKP1 result in ectodermal dysplasia-skin fragility syndrome (OMIM 604536) (Citation47). The skin fragility results from a loss of keratinocyte adhesion within the desmosomal inner plaque; the ectodermal dysplasia partly results from altered differentiation and proliferation in the epidermis but also from the fact that plakophilin-1 is also present in the nuclei of cells that lack desmosomes (Citation48,Citation49). In those cells, the interactions of plakophilin-1 with other signalling molecules involved in epithelial development may be disrupted (Citation50).
Desmoplakin: DSP
Desmoplakin is the major intracellular structural component of the desmosomal plaque (Citation51). Autosomal dominant mutations in DSP can give rise to striate palmoplantar keratoderma (OMIM 612908), a disorder characterized by linear thickening (but no blisters) on trauma-prone sites on the palms or weight-bearing areas on the soles (Citation52). Other dominant mutations underlie cases of arrhythmogenic cardiomyopathy (OMIM 607450), often in the absence of any cutaneous abnormalities (Citation53). Furthermore, autosomal recessive mutations in DSP can result in woolly hair and keratoderma with or without cardiomyopathy (OMIM 605676) (Citation54). However, some recessive mutations can result in devastating muco-cutaneous skin fragility, notably in a clinicopathological entity referred to as lethal acantholytic EB (OMIM 609638) (Citation55). Loss of desmoplakin expression in these cases leads to early death because of the profound skin loss and potential involvement of other organs, notably the heart (Citation56).
New EB disorders
Collectively, the above clinical and molecular entities represent the forms of EB recognized and classified as such in the last official classification of EB (Citation5). However, a number of new discoveries have been made in subsequent years.
Dystonin-epithelial isoform: DST1-e
Autosomal recessive mutations in the epithelial isoform of dystonin, also known as the 230-kDa bullous pemphigoid antigen, have been shown to result in a relatively mild form of inherited skin blistering (Citation57). Loss-of-function mutations on both alleles of DST1-e lead to a complete absence of the hemidesmosomal inner plaques—the sites at which keratin intermediate filaments anchor to the hemidesmosomes (Citation58). It is therefore perhaps somewhat surprising that the clinical blistering is relatively trivial. In part, this can be accounted for by a compensatory up-regulation in keratin 14 and plectin (Citation59). Thus far, only two pedigrees with DST1-e mutations have been reported (Citation57,Citation58). Although dystonin isoforms have a wide tissue distribution, neurological or cardiac involvement does not appear to be a clinical feature—skin blistering is the main abnormality. Whether heterozygous mutations in DST1-e can also cause skin fragility, akin to the findings for plectin (Citation18), has not yet been determined.
α3 Integrin: ITGA3
The α3 integrin subunit is a component of focal contacts at the dermal-epidermal junction, where it may dimerize with β1 integrin and contribute to epithelial-mesenchymal signalling (Citation60). Autosomal recessive loss-of-function mutations have been reported in three subjects with trauma-induced skin fragility (Citation61). Affected individuals also displayed pulmonary inflammation and congenital nephrotic syndrome, reflecting the important role of α3 integrin in lung and kidney biology (Citation60). In comparison to the pulmonary and renal manifestations, the cutaneous changes were relatively trivial, and yet they provided the clue to the inherent genetic abnormality. Affected individuals died early in life because of lung/kidney disease (Citation10).
Plakoglobin: JUP
Plakoglobin is an intracellular armadillo protein component of the desmosome (Citation62). Autosomal recessive mutations have been reported in individuals with Naxos disease (OMIM 601214)—a combination of woolly hair, palmoplantar keratoderma, and cardiomyopathy (Citation63); heterozygous carriers may also be prone to cardiac arrhythmias or heart failure (Citation64). Other autosomal dominant mutations may cause cardiomyopathy (Citation65). None of these cases, however, have demonstrated skin fragility. In contrast, patients with hair abnormalities, keratoderma, skin fragility, but no cardiac abnormalities have been described in whom autosomal recessive mutations in JUP were observed (Citation66). In some cases, the seemingly truncating mutations were rescued by use of alternative splicing (Citation67), but a case of overwhelming skin fragility associated with complete loss of plakoglobin expression in the skin has been documented (Citation11). That child died in early life, and the disorder, which so far represents a solitary case, was described as lethal congenital EB (Citation68).
Exophilin-5: EXPH5
A consanguineous pedigree has been reported with minor trauma-induced skin scaling/crusting and intermittent skin blistering associated with mottled dyspigmentation (Citation69). Whole exome sequencing was used to identify a homozygous loss-of-function mutation in EXPH5 which encodes exophilin-5, also known as Slac2-b. EXPH5 is an effector protein of Rab GTPase Rab27B, which is thought to have an important role in intracellular vesicle trafficking along actin and tubulin networks, as well as membrane fusion (Citation70). Patients with this condition demonstrated a loss of exophilin-5 immunostaining, disrupted keratinocyte adhesion within the lower epidermis, and increased numbers of perinuclear vesicles. This form of inherited skin fragility has been classified as an autosomal recessive form of EBS, although only two other affected individuals have been reported to date (Citation71,Citation72).
Transglutaminase-5: TGM5
Autosomal recessive mutations in TGM5 have been shown to underlie acral peeling skin syndrome (OMIM 609796) (Citation73). Transglutaminase 5 is one of eight different transglutaminase enzymes expressed in skin and has a distinct role in formation of the cornified cell envelope (Citation74). In acral peeling skin syndrome, the level of blister formation occurs just above the granular layer, just below the stratum corneum (Citation75). However, given the increased thickness of the stratum corneum in palms and soles relative to other body sites, the clinical appearances often resemble the most common form of EBS localized to hands and feet and indeed may cause some clinical confusion (Citation76). Acral skin peeling associated with TGM5 mutations may be more common than is currently appreciated since up to 3% of individuals in some populations, particularly in northern Europe, may be carriers of a common mutant ancestral allele (Citation77).
Other possible EB-like disorders
Inclusion of the above clinicopathological entities increases the number of individual gene abnormalities in ‘EB’ to 18. In addition to these conditions, a number of other inherited disorders associated with skin fragility have also been described. Whether these should be included in the next classification of EB is much debated and currently unresolved.
Desmocollin 3: DSC3
Desmocollin-3 is one of the transmembranous desmosomal cadherins that is expressed throughout the epidermis, particularly in the basal keratinocyte layer (Citation78). Autosomal recessive mutations in DSC3 were reported in a single consanguineous pedigree from Afghanistan that presented with hereditary hypotrichosis (scalp hair thinning) and recurrent small blisters (OMIM 613102) on the affected individuals’ scalps and at several other body sites (Citation79). A scalp skin biopsy from an affected individual was reported to show mild hair follicle plugging. Although a homozygous nonsense mutation in DSC3 was documented, there was no skin biopsy evidence of the protein changes or the presence of vesicles, and, from a dermatology perspective, the cutaneous changes more closely resembled keratosis pilaris, a common disorder often seen on the extensor aspects of the upper arms in association with dry skin or atopy. For now, there appears to be insufficient data to designate DSC3 as a further EB gene.
Desmoglein-1: DSG1
Desmoglein-1 is a transmembranous desmosomal cadherin predominantly expressed in the superficial epidermis (Citation80). It is the autoantigen responsible for the autoimmune blistering skin disease pemphigus foliaceous, and the target for bacterial toxins in staphylococcal scalded skin syndrome (Citation81). Autosomal dominant mutations in DSG1 have been reported in striate palmoplantar keratoderma (OMIM 148700) (Citation82). This condition is not normally associated with skin blistering, although skin fragility has on rare occasions been reported (Citation83). Autosomal recessive mutations in DSG1 have also been described in individuals with disruption of the skin barrier (Citation84). Notably, loss of cell adhesion within the epidermis led to severe dermatitis, multiple allergies, and metabolic wasting. An up-regulation of allergy-related cytokines secondary to the loss of cell adhesion was also observed (Citation84). Although defective keratinocyte cell-cell attachment was a primary abnormality, the clinical features did not manifest as blisters or erosions, and therefore classification as a form of EB is probably not justified.
Corneodesmosin: CDSN
Corneodesmosin is an essential component of corneodesmosomes and must undergo degradation in order for desquamation to occur (Citation85,Citation86). Surprisingly, autosomal dominant mutations in CDSN have been shown to underlie hereditary hypotrichosis (OMIM 146520) simplex rather than a skin barrier abnormality (Citation87). However, autosomal recessive mutations in CDSN have been described in patients with a form of generalized skin peeling disease (OMIM 270300) (Citation88). Clinically, loss of corneodesmosin expression results in profound skin barrier disruption with marked inflammation and a predisposition to atopy as well as symptoms of pruritus. The barrier disruption associated with CDSN loss does not resemble trauma-induced fragility, and the clinical syndrome does not show much overlap with other desmosomal blistering genodermatoses that feature as EB or EB-like entities.
CD151 antigen/tetraspanin: CD151
CD151 is a cell surface protein which in skin is expressed on the basolateral surface of basal keratinocytes concentrated within hemidesmosomes (Citation89). It contributes to cell adhesion, motility, and intracellular vesicular transport of integrins. CD151 is also thought to be important for signal transduction and cytoskeleton formation due to its association with phosphatidylinositol-4-kinase (Citation21,Citation22). A previous report described two teenage siblings with hereditary nephritis, EB, and beta-thalassaemia minor (OMIM 609057). Both showed multiple recurrent infected skin blisters of the lower limbs followed by atrophy, nail dystrophy, bilateral lacrimal duct stenosis, sensorineural deafness, proteinuria, and anaemia (Citation90). These siblings, and one other individual, were subsequently shown to be homozygous for a 1-bp insertion in CD151 (Citation91). Thus far, no consensus has been reached as to whether the CD151 changes were causative or coincidental and whether the cases warrant inclusion in the classification of EB.
Keratins 1 and 10: KRT1, KRT10
The major epidermal keratins in the spinous layer of the epidermis (i.e. superficial to the basal keratinocytes) are keratins 1 and 10, mutations in which result in epidermolytic ichthyosis (OMIM 113800) (Citation92). Although these conditions cause microscopic evidence of keratinocyte cytolysis (hence the term epidermolytic), and there may be clinical overlap with some EB subtypes, the major pathological consequences are altered epidermal differentiation and proliferation leading to scaling (ichthyosis). For that reason, genodermatoses involving mutations in KRT1 and KRT10 are classified as forms of ichthyosis rather than blistering genodermatoses (Citation93).
Treatment of blistering genodermatoses
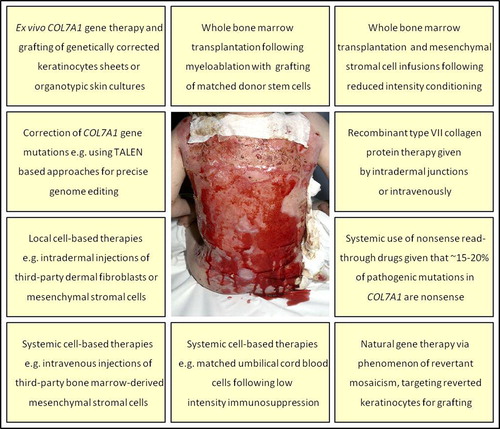
An improved understanding of the molecular basis of the blistering genodermatoses has had several direct translational benefits for patients in terms of improved genetic counselling and the development of prenatal testing. For example, in sporadic cases of DEB, it had often been difficult to determine autosomal recessive from de novo inheritance: now, COL7A1 mutation analysis can differentiate the two scenarios and guide counselling (Citation94). With regard to prenatal testing, the fetal skin biopsy analyses developed in the 1980s for severe forms of EB have now, for the most part, been superseded by DNA assessment at much earlier stages in the pregnancy, usually using chorionic villus sampling (Citation95). In addition, preimplantation genetic diagnosis and haplotyping methods have been designed, approved, and applied to families at risk for recurrent EB (Citation96). However, the key challenge in translational research has been to try to engineer new therapies for patients living with blistering genodermatoses. To that end, there have been several recent advances in developing gene, protein, cell, drug, and small molecule therapies, several of which, particularly cell therapies, have entered clinical trials ().
Figure 5. Clinical illustration of the therapeutic challenge presented by a patient with recessive dystrophic EB and very extensive skin fragility. The various endeavours to develop new therapies that are currently at preclinical or clinical trial stages are listed.
Gene therapy
For autosomal dominant blistering genodermatoses the principal strategy being assessed is silencing of the mutant allele using small interfering RNA (siRNA) approaches. A clinical trial of siRNA against a mutant keratin (K6a in a patient with pachyonychia congenita (OMIM 167200), a disorder that causes thickening of the nails and skin on the palms and soles) showed effective gene silencing and a clinical response with decreased skin thickening compared to vehicle alone (Citation97). Delivery was a problem, however, since injecting siRNA into the dermis was painful and impractical; alternative topical delivery methods are now being assessed. With regard to blistering genodermatoses, siRNA technology has also been successfully used in vitro with silencing of mutant K5 and minimal effect on wild-type K5 expression, findings that have potential clinical translation for patients with EBS (Citation98). Another approach for dominant and recessive diseases, still at the in vitro stage, is spliceosome-mediated RNA trans-splicing (SMaRT). SMaRT works on the same principle as siRNA, with gene correction generated through silencing of mutant genes. This technique utilizes endogenous spliceosome machinery to excise mutant exons, thus knocking out the mutant protein in affected cells. SMaRT has been successfully used to replace a mutation in PLEC in EBS (Citation99), as well as COL7A1 mutations in DEB (Citation100). This approach has also been used specifically to replace the first seven exons of KRT14 in an EB simplex cell line (Citation101). SMaRT effectively excises the mutation within a gene while increasing normal allele expression, making this approach a potential therapy for genodermatoses. Most recessive blistering genodermatoses are associated with loss-of-function mutations on both alleles, and therefore gene replacement strategies, which have been in development for more than a decade, are being pursued. In theory, replacing a non-functioning gene with a synthetic copy of a functional gene makes mechanistic sense, but advancing to clinical trials has been beset with difficulties—efficiency, delivery, and safety concerns continue to require preclinical optimization (Citation102). To date there has only been one report of a clinical trial of gene therapy in EB which involved grafting of LAMB3 gene-corrected keratinocytes in a patient with non-Herlitz JEB (Citation103). This led to correction of the laminin-332 protein at the dermal-epidermal junction and functional improvement with stronger skin. However, this approach used a retroviral vector that evoked some potential safety concerns, and therefore more extensive treatment in this patient, or other affected individuals, has not been reported. For recessive DEB, ex vivo COL7A1 gene correction and grafting of keratinocyte sheets onto affected individuals is in the early stage of a phase 1 trial in Stanford, USA, (http://clinicaltrials.gov/ct2/show/NCT01263379?term = NCT01263379&rank = 1), although international efforts to launch similar clinical trials are ongoing in many other countries.
Genomic editing and engineering
New technologies that edit or correct mutant genomic sequences also represent promising innovative therapies for EB and other genetic disorders. Genomic editing utilizes the properties of engineered nucleases, which are molecules composed of two main components; a sequence-specific DNA-binding domain and a non-specific DNA cleavage module (Citation104,Citation105). Once bound, these nucleases produce targeted DNA double-strand breaks, which activate cellular DNA repair mechanisms. The delivery of nucleases to target DNA binding domains can be achieved via zinc-finger and transcription activator-like effector proteins, termed zinc-finger nucleases (ZFNs) and transcription activator-like effector nucleases (TALENs), respectively. More recently has been the emergence of clustered regulatory interspaced short palindromic repeats (CRISPR)-based RNA-guided DNA endonucleases. CRISPR systems provide acquired immunity to bacteria and archaea through the silencing of invading foreign DNA. This system can be modified to deliver Cas, an RNA-guided DNA endonuclease, to target DNA which is subsequently cleaved. Genome-editing technology has been explored in recessive DEB. Notably TALENs have been used to correct COL7A1 gene mutations in primary fibroblasts (Citation106).
Recombinant protein therapy
Another potentially attractive approach is recombinant protein therapy—if conditions such as recessive DEB lack type VII collagen (C7) protein in the skin, then why not simply make artificial C7 and restore this to the defective skin? This approach has been tested in murine models: intradermal injections of human recombinant C7 localized to the basement membrane zone and organized into human anchoring fibril structures, thus reversing the pathological features of the disease (Citation107). Other mouse models have also been used to test intravenously injected human recombinant C7 (Citation108). These studies have shown C7 homing to recessive DEB skin grafts, restoration of dermal-epidermal adhesion, C7 expression, and anchoring fibril formation. Recombinant C7 protein therapy in recessive DEB is now being assessed in a dog model (Citation109). Extension of these studies to clinical trials of C7 protein therapy in humans (intradermal or intravenous) is expected within the next 2–3 years. One concern has been whether patients might develop autoantibodies to the new C7. However, a recent study showed that as a baseline finding, although many subjects with recessive DEB do have circulating anti-C7 antibodies (detected by ELISA), these antibodies do not tend to bind to the dermal-epidermal junction (negative indirect immunofluorescence) and therefore may not be clinically relevant—although clearly this will need to be monitored closely in human trials of recombinant C7 (Citation110).
Cell therapy with intradermal allogeneic fibroblasts
The C7 protein is normally synthesized by keratinocytes and fibroblasts. Therefore, one therapeutic consideration in recessive DEB, a blistering genodermatosis in which functional C7 is lacking or absent, has been to assess whether injection of wild-type fibroblasts might help restore some C7 expression in the skin. First-in-man studies showed that intradermal injection of allogeneic fibroblasts in patients with recessive DEB could increase C7 expression at the dermal-epidermal junction for at least 3 months following a single injection (Citation111). The donor cells were not tissue-matched and were undetectable 2 weeks after injection, but no adverse effects (inflammation or allergy) were noted. Mechanism of action studies have investigated whether the allogeneic fibroblasts have an indirect benefit, increasing the recipient's own COL7A1 mRNA levels (through up-regulation of local cytokines and growth factors), leading to greater deposition of mutant, but partially functional, C7 at the basement membrane zone (Citation112), or whether the fibroblasts directly release wild-type C7 (Citation113,Citation114). Both mechanisms seem plausible. Two clinical trials comparing allogeneic fibroblasts versus vehicle in wound healing in recessive DEB have been reported. One study found no difference between fibroblasts or vehicle in wound healing responses (Citation115), but a different study showed that a single injection of allogeneic fibroblasts can accelerate wound healing in recessive DEB for 28 days after injection compared to vehicle alone (Citation116). Injecting fibroblasts into patient skin can be painful, and therefore further studies on the mode of cell delivery, as well as additional optimization of the frequency of fibroblast injections and the amount of cells per injection, will be necessary in order to define the clinical utility of allogeneic fibroblast cell therapy in the overall management of recessive DEB or other forms of EB.
Cell therapy with intradermal mesenchymal stromal cells
Intradermal injections of bone marrow-derived mesenchymal stromal cells (MSCs) have been assessed in two individuals with recessive DEB (Citation117). This study showed improved wound healing following injection of 0.5 × 106 allogeneic MSCs compared to saline. In contrast to allogeneic fibroblasts, allogeneic MSCs appeared to be able to induce de novo synthesis of basement membrane C7. Clinicopathological improvements were sustained for 4 months, after which the original skin fragility and pathology returned. Recent mechanism of action studies in mice have shown that the MSC pool in bone marrow contains a subpopulation of cells that include epithelial progenitors (Citation118). These MSCs, which are platelet-derived growth factor receptor-alpha (PDGFRα)-positive and Lineage-negative, are recruited to damaged skin along a concentration gradient of the tissue distress factor high mobility group box-1 (HMGB1) that is rapidly released from hypoxic keratinocytes in recessive DEB blister roofs. Future clinical trials in recessive DEB are likely to target and exploit this population of MSCs and the HMGB1 recruitment factor. These studies are likely to have much broader implications and relevance in regenerative medicine, with regard to the management of other chronic wounds. Intravenous clinical trials of bone marrow-derived MSCs and adipose-derived MSCs are also entering early clinical trials for recessive DEB in Egypt, the United Kingdom, and Brazil. Although these cells are not tissue-matched, it is hoped that the MSCs will trigger a systemic anti-inflammatory effect (modifying T cells and B cells and up-regulating cytokines such as interleukin-10) that may lead to clinical benefits that last for several months (Citation119).
Bone marrow stem cell therapy
Bone marrow transplantation (BMT) is primarily indicated for haematological diseases, such as aplastic anaemia and leukaemia. However, because the pluripotent stem cells can differentiate not only into blood cells but also other functional cells, the scope of BMT has been expanded to encompass tissue regeneration and thereby treat genetic disorders (Citation120). In 2010, a phase 1 clinical trial of whole bone marrow transplantation in six children with recessive DEB was reported (Citation121). Those transplants mostly involved myeloablation of the EB subjects’ bone marrow followed by sibling-matched donor grafting. Reduced cutaneous blistering (by up to 50% in half; more than 50% in the remainder) was noted, and there was increased C7 in the skin of 5/6 subjects. Clinical improvement was also noted in the one individual who did not show an increase in C7; some children are now more than 5 years post-BMT, and their skin remains much improved. One of the children reported in the trial died from graft failure and sepsis, and a further child died from complications of the recessive DEB before grafting took place. Subsequently, new protocols for the use of BMT in EB patients have started to be developed—usually involving revisions to the immune conditioning regimens and transplantation protocols (Citation122). Reduced intensity conditioning has significantly reduced the mortality from BMT in EB, although substantial clinical improvement still occurs. Several patients have reported a reduction in blister severity from ˜70% of their skin surface to ˜5%, although none has been totally cured. The mechanism of action leading to the clinical and skin pathology improvement remains unclear as some patients continue to benefit long-term despite showing no increase in skin C7, especially in those who have undergone reduced intensity conditioning BMT. The optimal use and application of BMT in recessive DEB (and potentially other EB subtypes), therefore, remains in clinical development (Citation123).
Natural gene therapy: revertant mosaicism
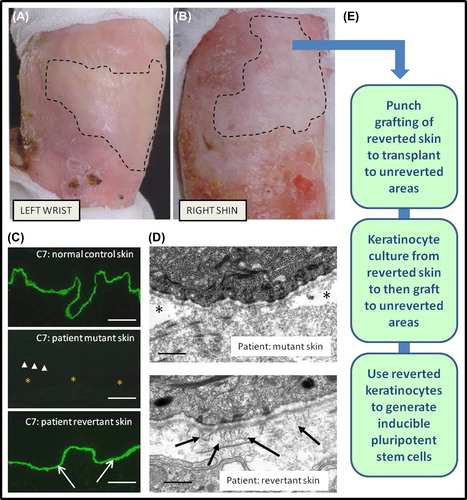
A remarkable recent clinical observation has been that some individuals with blistering genodermatoses, particularly non-Herlitz JEB, possess patches of skin which are more resistant to trauma and tend not to blister, and which show partial or total correction of the inherent basement membrane defect (Citation124,Citation125). This phenomenon, termed revertant mosaicism, or natural gene therapy, results from several possible corrective genetic events and has been observed in numerous other inherited skin diseases, as well as genetic diseases affecting bone marrow (Citation126). Revertant mosaicism is likely to be more common than is currently appreciated, and, indeed, perhaps all patients with non-Herlitz JEB display clinical evidence of this (Citation127). A key question has been how best to exploit this natural phenomenon to help patients (). Initial attempts to expand revertant keratinocytes from a patient with non-Herlitz JEB in culture and then skin grafting were not successful, mostly because the degree of reversion was not maintained in culture over mutant cells (Citation128). However, punch grafting of revertant skin in another patient to unreverted areas has led to clinical and functional improvement with maintenance of reversion in the both the donor and recipient sites (Citation129).
Figure 6. Clinicopathological features of revertant mosaicism in a patient with recessive dystrophic EB and potential clinical translation for therapy. There are demarcated areas in which trauma-induced blistering does not occur on the left wrist (A) and right shin (B). Immunolabelling of the dermal-epidermal junction (C) with an antibody to type VII collagen (C7) shows bright linear staining in normal skin but a complete absence in patient skin (arrow-heads indicate dermal-epidermal junction, and asterisk denotes subepidermal blistering). In contrast, in the revertant areas there is bright linear labelling for type VII collagen (arrows) which resembles normal skin (scale bar = 50 μm). Ultrastructurally (D), the patient's blister-prone skin shows focal blistering beneath the lamina densa (asterisk), whereas in the area of revertant mosaicism there is no blistering and also evidence of new anchoring fibrils (arrows) that are completely lacking in the blistered skin (scale bar = 0.2 μm). The phenomenon of revertant mosaicism presents several opportunities for translational research and therapy (E), including culturing the reverted keratinocytes, skin grafting, and creation of inducible pluripotent stem cells.
Inducible pluripotent stem cells
One of the most significant recent advances in stem cell biology has been the discovery that cells resembling pluripotent embryonic stem cells can be derived from somatic cells such as fibroblasts or keratinocytes by transfection with three or four embryonic transcription factors (Citation130). Similar reprogramming can also be achieved chemically using a combination of seven small molecule compounds (Citation131). How best to make use of these inducible pluripotent stem cells (iPSCs) for clinical gain is a key question in translational research. Thus far, recessive DEB fibroblasts and keratinocytes have been used to make iPSCs (Citation132,Citation133), which can be differentiated into various other cell/tissues, including MSCs containing epithelial progenitors (Citation118). The iPSCs derived from blistering genodermatoses can be used for disease modelling and for testing of disease-modifying compounds but inherently still possess the same genetic defects underlying the skin fragility as the original patient skin. Nevertheless, recent data have shown successful gene-editing of these mutant cells, which provides encouragement for iPSC gene therapy clinical translation (Citation106). Aside from gene editing, it may also be plausible to harness the natural gene therapy observed in recessive DEB keratinocytes: use of such cells in the manufacture and differentiation of iPSCs would avoid the need for additional gene correction and thereby facilitate clinical utility (Citation134). Use of iPSCs in clinical practice still requires optimization in terms of using non-viral methods of transfection (e.g. using mRNAs) and other safety data to be established, but the field is changing rapidly and new therapeutic opportunities are expected shortly.
Nonsense read-through drugs and small molecule therapies
Nonsense mutations are responsible for an estimated 10% of all human genetic diseases. These mutations act as stop codons during transcription, creating truncated mRNA molecules that subsequently get degraded. Nonsense read-through drugs act by promoting ribosomes to ‘read through’ premature stop codons allowing the production of a viable protein product (Citation135). Unfortunately, problems with false positive luciferase assays, used to determine successful drug read-through, have slowed effective drug development (Citation136). With regard to genetic skin diseases, one study looked at the nonsense read-through drug, PTC124 (PTC Therapeutics, New Jersey, South Plainfield, USA), in pseudoxanthoma elasticum (OMIM 264800), a condition characterized by the fragmentation and ectopic mineralization of elastic fibres in tissues such as the skin, eyes, and blood vessels, and which results from mutations in the ABCC6 gene. Studies in zebrafish models have indicated that PTC124 is safe up to 20 μg mL−1 concentrations, that read-through ability was variable, and that amino acids substituted in place of the original mutated sequence still produced abcc6a protein (Citation137). This study provided support for the feasibility of this class of drugs as an effective treatment for inherited skin disorders, although caveats about the robustness of the assays used for biological read-outs are of concern to some investigators. Interest in other small molecules for the treatment of EB includes an assessment of topical diacerin in EBS associated with keratin gene mutations (Citation138). A pilot study demonstrated reduction in blisters, possibly through alterations in interleukin-1β signalling (Citation138); further clinical trials are awaited.
Conclusion
This review highlights the huge strides that research into genodermatoses has taken over the last decade, enhancing our understanding of skin structure, physiology, molecular biology, and affiliated disease processes. The progress in translational research is also evident with the development of novel therapies including gene, protein, drug, and small molecule therapies, several of which have entered clinical trials. In future, we are likely to see even more comprehensive molecular diagnostic work that utilizes next-generation sequencing approaches to identify causative mutations, as well as the emergence of new therapies that will offer significant and sustainable benefits to patients living with these debilitating conditions.
Declaration of interest: The authors report no conflicts of interest.
This review has been supported by the UK National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas’ NHS Foundation Trust and King's College London, as well as DebRA UK, the Rosetrees Trust, and the Sohana Research Fund in conjunction with Goldman Sachs Gives. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the UK Department of Health.
References
- Simpson CL, Patel DM, Green KJ. Deconstructing the skin: cytoarchitectural determinants of epidermal morphogenesis. Nat Rev Mol Cell Biol. 2011;12:565–80.
- Elias PM. Skin barrier function. Curr Allergy Asthma Rep. 2008;8: 299–305.
- Tsuruta D, Hashimoto T, Hamill KJ, Jones JC. Hemidesmosomes and focal contact proteins: functions and cross-talk in keratinocytes, bullous diseases and wound healing. J Dermatol Sci. 2011; 62:1–7.
- Green KJ, Getsios S, Troyanovsky S, Godsel LM. Intercellular junction assembly, dynamics, and homeostasis. Cold Spring Harb Perspect Biol. 2010;2:a000125.
- Fine JD, Eady RA, Bauer EA, Bauer JW, Bruckner-Tuderman L, Heagerty A, et al. The classification of inherited epidermolysis bullosa (EB): report of the Third International Consensus Meeting on Diagnosis and Classification of EB. J Am Acad Dermatol. 2008;58: 931–50.
- Bruckner-Tuderman L, McGrath JA, Robinson EC, Uitto J. Progress in epidermolysis bullosa research: Summary of DEBRA International Research Conference 2012. J Invest Dermatol. 2013;133:2121–6.
- Pearson RW. Studies on the pathogenesis of epidermolysis bullosa. J Invest Dermatol. 1962;39:551–75.
- Kim S, Coulombe PA. Intermediate filament scaffolds fulfill mechanical, organizational, and signaling functions in the cytoplasm. Genes Dev. 2007;21:1581–97.
- Celli A, Sanchez S, Behne M, Hazlett T, Gratton E, Mauro T. The epidermal Ca(2+) gradient: measurement using the phasor representation of fluorescent lifetime imaging. Biophys J. 2010;98:911–21.
- Coulombe PA, Lee CH. Defining keratin protein function in skin epithelia: epidermolysis bullosa simplex and its aftermath. J Invest Dermatol. 2012;132:763–75.
- McLean WH, Moore CB. Keratin disorders: from gene to therapy. Hum Mol Genet. 2011;20:R189–97.
- Sprecher E. Epidermolysis bullosa simplex. Dermatol Clin. 2010;28: 23–32.
- Rezniczek GA, Walko G, Wiche G. Plectin gene defects lead to various forms of epidermolysis bullosa simplex. Dermatol Clin. 2010;28: 33–41.
- Winter L, Wiche G. The many faces of plectin and plectinopathies: pathology and mechanisms. Acta Neuropathol. 2013;125:77–93.
- McLean WH, Pulkkinen L, Smith FJ, Rugg EL, Lane EB, Bullrich F, et al. Loss of plectin causes epidermolysis bullosa with muscular dystrophy: cDNA cloning and genomic organization. Genes Dev. 1996; 10:1724–35.
- Smith FJ, Eady RA, Leigh IM, McMillan JR, Rugg EL, Kelsell DP, et al. Plectin deficiency results in muscular dystrophy with epidermolysis bullosa. Nat Genet. 1996;13:450–7.
- Charlesworth A, Chiaverini C, Chevrant-Breton J, DelRio M, Diociaiuti A, Dupuis RP, et al. Epidermolysis bullosa simplex with PLEC mutations: new phenotypes and new mutations. Br J Dermatol. 2013;168:808–14.
- Bolling MC, Jongbloed JD, Boven LG, Diercks GF, Smith FJ, McLean WH, et al. Plectin mutations underlie epidermolysis bullosa simplex in 8% of patients. J Invest Dermatol. 2014;134:273–6.
- Kligys KR, Wu Y, Hopkinson SB, Kaur S, Platanias LC, Jones JC.α6β4 Integrin, a master regulator of expression of integrins in human keratinocytes. J Biol Chem. 2012;287:17975–84.
- Margadant C, Charafeddine RA, Sonnenberg A. Unique and redundant functions of integrins in the epidermis. FASEB J. 2010;24:4133–52.
- Chung HJ, Uitto J. Type VII collagen: the anchoring fibril protein at fault in dystrophic epidermolysis bullosa. Dermatol Clin. 2010;28: 93–105.
- Ashton GH, Sorelli P, Mellerio JE, Keane FM, Eady RA, McGrath JA. Alpha 6 beta 4 integrin abnormalities in junctional epidermolysis bullosa with pyloric atresia. Br J Dermatol. 2001;144:408–14.
- Inoue M, Tamai K, Shimizu H, Owaribe K, Nakama T, Hashimoto T, et al. A homozygous missense mutation in the cytoplasmic tail of beta4 integrin, G931D, that disrupts hemidesmosome assembly and underlies non-Herlitz junctional epidermolysis bullosa without pyloric atresia?J Invest Dermatol. 2000;114:1061–4.
- Sugawara K, Tsuruta D, Ishii M, Jones JC, Kobayashi H. Laminin-332 and -511 in skin. Exp Dermatol. 2008;17:473–80.
- Kiritsi D, Has C, Bruckner-Tuderman L. Laminin 332 in junctional epidermolysis bullosa. Cell Adh Migr. 2013;7:135–41.
- Laimer M, Lanschuetzer CM, Diem A, Bauer JW. Herlitz junctional epidermolysis bullosa. Dermatol Clin. 2010;28:55–60.
- Yancey KB, Hintner H. Non-Herlitz junctional epidermolysis bullosa. Dermatol Clin. 2010;28:67–77.
- McLean WH, Irvine AD, Hamill KJ, Whittock NV, Coleman-Campbell CM, Mellerio JE, et al. An unusual N-terminal deletion of the laminin alpha3a isoform leads to the chronic granulation tissue disorder laryngo-onycho-cutaneous syndrome. Hum Mol Genet. 2003;12: 2395–409.
- Powell AM, Sakuma-Oyama Y, Oyama N, Black MM. Collagen XVII/BP180: a collagenous transmembrane protein and component of the dermoepidermal anchoring complex. Clin Exp Dermatol. 2005;30: 682–7.
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381: 320–32.
- McGrath JA, Gatalica B, Christiano AM, Li K, Owaribe K, McMillan JR, et al. Mutations in the 180-kD bullous pemphigoid antigen (BPAG2), a hemidesmosomal transmembrane collagen (COL17A1), in generalized atrophic benign epidermolysis bullosa. Nat Genet. 1995;11:83–6.
- McGrath JA, Gatalica B, Li K, Dunnill MG, McMillan JR, Christiano AM, et al. Compound heterozygosity for a dominant glycine substitution and a recessive internal duplication mutation in the type XVII collagen gene results in junctional epidermolysis bullosa and abnormal dentition. Am J Pathol. 1996;148:1787–96.
- Almaani N, Liu L, Dopping-Hepenstal PJ, Lovell PA, Lai-Cheong JE, Graham RM, et al. Autosomal dominant junctional epidermolysis bullosa. Br J Dermatol. 2009;160:1094–7.
- Burgeson RE, Lunstrum GP, Rokosova B, Rimberg CS, Rosenbaum LM, Keene DR. The structure and function of type VII collagen. Ann N Y Acad Sci. 1990;580:32–43.
- Tidman MJ, Eady RA. Ultrastructural morphometry of normal human dermal-epidermal junction. The influence of age, sex, and body region on laminar and nonlaminar components. J Invest Dermatol. 1984;83: 448–53.
- Christiano AM, Suga Y, Greenspan DS, Ogawa H, Uitto J. Premature termination codons on both alleles of the type VII collagen gene (COL7A1) in three brothers with recessive dystrophic epidermolysis bullosa. J Clin Invest. 1995;95:1328–34.
- Fine JD, Mellerio JE. Extracutaneous manifestations and complications of inherited epidermolysis bullosa: part I. Epithelial associated tissues. J Am Acad Dermatol. 2009;61:367–84.
- Christiano AM, McGrath JA, Tan KC, Uitto J. Glycine substitutions in the triple-helical region of type VII collagen result in a spectrum of dystrophic epidermolysis bullosa phenotypes and patterns of inheritance. Am J Hum Genet. 1996;58:671–81.
- Christiano AM, Ryynanen M, Uitto J. Dominant dystrophic epidermolysis bullosa: identification of a Gly--> Ser substitution in the triple-helical domain of type VII collagen. Proc Natl Acad Sci U S A. 1994;91:3549–53.
- Meves A, Stremmel C, Gottschalk K, Fassler R. The Kindlin protein family: new members to the club of focal adhesion proteins. Trends Cell Biol. 2009;19:504–13.
- Lai-Cheong JE, Parsons M, McGrath JA. The role of kindlins in cell biology and relevance to human disease. Int J Biochem Cell Biol. 2010;42:595–603.
- Jobard F, Bouadjar B, Caux F, Hadj-Rabia S, Has C, Matsuda F, et al. Identification of mutations in a new gene encoding a FERM family protein with a pleckstrin homology domain in Kindler syndrome. Hum Mol Genet. 2003;12:925–35.
- Siegel DH, Ashton GH, Penagos HG, Lee JV, Feiler HS, Wilhelmsen KC, et al. Loss of kindlin-1, a human homolog of the Caenorhabditis elegans actin-extracellular-matrix linker protein UNC-112, causes Kindler syndrome. Am J Hum Genet. 2003;73: 174–87.
- Lai-Cheong JE, Tanaka A, Hawche G, Emanuel P, Maari C, Taskesen M, et al. Kindler syndrome: a focal adhesion genodermatosis. Br J Dermatol. 2009;160:233–42.
- Kowalczyk AP, Green KJ. Structure, function, and regulation of desmosomes. Prog Mol Biol Transl Sci. 2013;116:95–118.
- Nekrasova O, Green KJ. Desmosome assembly and dynamics. Trends Cell Biol. 2013;23:537–46.
- McGrath JA, McMillan JR, Shemanko CS, Runswick SK, Leigh IM, Lane EB, et al. Mutations in the plakophilin 1 gene result in ectodermal dysplasia/skin fragility syndrome. Nat Genet. 1997;17:240–4.
- South AP, Wan H, Stone MG, Dopping-Hepenstal PJ, Purkis PE, Marshall JF, et al. Lack of plakophilin 1 increases keratinocyte migration and reduces desmosome stability. J Cell Sci. 2003;116:3303–14.
- Hatzfeld M. Plakophilins: multifunctional proteins or just regulators of desmosomal adhesion?Biochim Biophys Acta. 2007;1773:69–77.
- Wolf A, Hatzfeld M. A role of plakophilins in the regulation of translation. Cell Cycle. 2010;9:2973–8.
- Garrod D, Chidgey M. Desmosome structure, composition and function. Biochim Biophys Acta. 2008;1778:572–87.
- Armstrong DK, McKenna KE, Purkis PE, Green KJ, Eady RA, Leigh IM, et al. Haploinsufficiency of desmoplakin causes a striate subtype of palmoplantar keratoderma. Hum Mol Genet. 1999;8: 143–8.
- Rizzo S, Pilichou K, Thiene G, Basso C. The changing spectrum of arrhythmogenic (right ventricular) cardiomyopathy. Cell Tissue Res. 2012;348:319–23.
- Petrof G, Mellerio JE, McGrath JA. Desmosomal genodermatoses. Br J Dermatol. 2012;166:36–45.
- Jonkman MF, Pasmooij AM, Pasmans SG, van den Berg MP, Ter Horst HJ, Timmer A, et al. Loss of desmoplakin tail causes lethal acantholytic epidermolysis bullosa. Am J Hum Genet. 2005;77:653–60.
- Hobbs RP, Han SY, van der Zwaag PA, Bolling MC, Jongbloed JD, Jonkman MF, et al. Insights from a desmoplakin mutation identified in lethal acantholytic epidermolysis bullosa. J Invest Dermatol. 2010;130:2680–3.
- Groves RW, Liu L, Dopping-Hepenstal PJ, Markus HS, Lovell PA, Ozoemena L, et al. A homozygous nonsense mutation within the dystonin gene coding for the coiled-coil domain of the epithelial isoform of BPAG1 underlies a new subtype of autosomal recessive epidermolysis bullosa simplex. J Invest Dermatol. 2010;130:1551–7.
- Liu L, Dopping-Hepenstal PJ, Lovell PA, Michael M, Horn H, Fong K, et al. Autosomal recessive epidermolysis bullosa simplex due to loss of BPAG1-e expression. J Invest Dermatol. 2012;132:742–4.
- Michael M, Begum R, Fong K, Pourreyrone C, South AP, McGrath JA, et al. BPAG1-e restricts keratinocyte migration through control of adhesion stability. J Invest Dermatol.2013 Sep 11 [Epub ahead of print].
- Hodivala-Dilke KM, DiPersio CM, Kreidberg JA, Hynes RO. Novel roles for alpha3beta1 integrin as a regulator of cytoskeletal assembly and as a trans-dominant inhibitor of integrin receptor function in mouse keratinocytes. J Cell Biol. 1998;142:1357–69.
- Has C, Sparta G, Kiritsi D, Weibel L, Moeller A, Vega-Warner V, et al. Integrin alpha3 mutations with kidney, lung, and skin disease. N Engl J Med. 2012;366:1508–14.
- Yin T, Green KJ. Regulation of desmosome assembly and adhesion. Semin Cell Dev Biol. 2004;15:665–77.
- McKoy G, Protonotarios N, Crosby A, Tsatsopoulou A, Anastasakis A, Coonar A, et al. Identification of a deletion in plakoglobin in arrhythmogenic right ventricular cardiomyopathy with palmoplantar keratoderma and woolly hair (Naxos disease). Lancet. 2000;355:2119–24.
- Azaouagh A, Churzidse S, Konorza T, Erbel R. Arrhythmogenic right ventricular cardiomyopathy/dysplasia: a review and update. Clin Res Cardiol. 2011;100:383–94.
- Li D, Liu Y, Maruyama M, Zhu W, Chen H, Zhang W, et al. Restrictive loss of plakoglobin in cardiomyocytes leads to arrhythmogenic cardiomyopathy. Hum Mol Genet. 2011;20:4582–96.
- Winik BC, Asial RA, McGrath JA, South AP, Boente MC. Acantholytic ectodermal dysplasia: clinicopathological study of a new desmosomal disorder. Br J Dermatol. 2009;160:868–74.
- Cabral RM, Liu L, Hogan C, Dopping-Hepenstal PJ, Winik BC, Asial RA, et al. Homozygous mutations in the 5’ region of the JUP gene result in cutaneous disease but normal heart development in children. J Invest Dermatol. 2010;130:1543–50.
- Pigors M, Kiritsi D, Krumpelmann S, Wagner N, He Y, Podda M, et al. Lack of plakoglobin leads to lethal congenital epidermolysis bullosa: a novel clinico-genetic entity. Hum Mol Genet. 2011;20:1811–19.
- McGrath JA, Stone KL, Begum R, Simpson MA, Dopping-Hepenstal PJ, Liu L, et al. Germline mutation in EXPH5 implicates the Rab27B effector protein Slac2-b in inherited skin fragility. Am J Hum Genet. 2012;91:1115–21.
- Stenmark H. Rab GTPases as coordinators of vesicle traffic. Nat Rev Mol Cell Biol. 2009;10:513–25.
- Pigors M, Schwieger-Briel A, Leppert J, Kiritsi D, Kohlhase J, Bruckner-Tuderman L, et al. Molecular heterogeneity of epidermolysis bullosa simplex: contribution of EXPH5 mutations. J Invest Dermatol.2013 Sep 4 [Epub ahead of print].
- Liu L, Mellerio JE, Martinez AE, McMillan JR, Aristodemou S, Parsons M, et al. Mutations in EXPH5 result in autosomal recessive skin fragility. Br J Dermatol. 2014;170:204–7.
- Cassidy AJ, van Steensel MA, Steijlen PM, van Geel M, van der Velden J, Morley SM, et al. A homozygous missense mutation in TGM5 abolishes epidermal transglutaminase 5 activity and causes acral peeling skin syndrome. Am J Hum Genet. 2005;77:909–17.
- Pietroni V, Di Giorgi S, Paradisi A, Ahvazi B, Candi E, Melino G. Inactive and highly active, proteolytically processed transglutaminase-5 in epithelial cells. J Invest Dermatol. 2008;128:2760–6.
- Kharfi M, El Fekih N, Ammar D, Jaafoura H, Schwonbeck S, van Steensel MA, et al. A missense mutation in TGM5 causes acral peeling skin syndrome in a Tunisian family. J Invest Dermatol. 2009;129:2512–15.
- Kiritsi D, Cosgarea I, Franzke CW, Schumann H, Oji V, Kohlhase J, et al. Acral peeling skin syndrome with TGM5 gene mutations may resemble epidermolysis bullosa simplex in young individuals. J Invest Dermatol. 2010;130:1741–6.
- van der Velden JJ, Jonkman MF, McLean WH, Hamm H, Steijlen PM, van Steensel MA, et al. A recurrent mutation in the TGM5 gene in European patients with acral peeling skin syndrome. J Dermatol Sci. 2012;65:74–6.
- Chen J, Den Z, Koch PJ. Loss of desmocollin 3 in mice leads to epidermal blistering. J Cell Sci. 2008;121:2844–9.
- Ayub M, Basit S, Jelani M, Ur Rehman F, Iqbal M, Yasinzai, et al. A homozygous nonsense mutation in the human desmocollin-3 (DSC3) gene underlies hereditary hypotrichosis and recurrent skin vesicles. Am J Hum genet. 2009;85:515–20.
- Hammers CM, Stanley JR. Desmoglein-1, differentiation, and disease. J Clin Invest. 2013;123:1419–22.
- Amagai M, Stanley JR. Desmoglein as a target in skin disease and beyond. J Invest Dermatol. 2012;132:776–84.
- Rickman L, Simrak D, Stevens HP, Hunt DM, King IA, Bryant SP, et al. N-terminal deletion in a desmosomal cadherin causes the autosomal dominant skin disease striate palmoplantar keratoderma. Hum Mol Genet. 1999;8:971–6.
- Zamiri M, Smith FJ, Campbell LE, Tetley L, Eady RA, Hodgins MB, et al. Mutation in DSG1 causing autosomal dominant striate palmoplantar keratoderma. Br J Dermatol. 2009;161:692–4.
- Samuelov L, Sarig O, Harmon RM, Rapaport D, Ishida-Yamamoto A, Isakov O, et al. Desmoglein 1 deficiency results in severe dermatitis, multiple allergies and metabolic wasting. Nat Genet. 2013;45:1244–8.
- Jonca N, Guerrin M, Hadjiolova K, Caubet C, Gallinaro H, Simon M, et al. Corneodesmosin, a component of epidermal corneocyte desmosomes, displays homophilic adhesive properties. J Biol Chem. 2002; 277:5024–9.
- Simon M, Jonca N, Guerrin M, Haftek M, Bernard D, Caubet C, et al. Refined characterization of corneodesmosin proteolysis during terminal differentiation of human epidermis and its relationship to desquamation. J Biol Chem. 2001;276:20292–9.
- Levy-Nissenbaum E, Betz RC, Frydman M, Simon M, Lahat H, Bakhan T, et al. Hypotrichosis simplex of the scalp is associated with nonsense mutations in CDSN encoding corneodesmosin. Nat Genet. 2003;34:151–3.
- Oji V, Eckl KM, Aufenvenne K, Natebus M, Tarinski T, Ackermann K, et al. Loss of corneodesmosin leads to severe skin barrier defect, pruritus, and atopy: unraveling the peeling skin disease. Am J Hum Genet. 2010;87:274–81.
- Sterk LM, Geuijen CA, Oomen LC, Calafat J, Janssen H, Sonnenberg A. The tetraspan molecule CD151, a novel constituent of hemidesmosomes, associates with the integrin alpha6beta4 and may regulate the spatial organization of hemidesmosomes. J Cell Biol. 2000;149:969–82.
- Kagan A, Feld S, Chemke J, Bar-Khayim Y. Occurrence of hereditary nephritis, pretibial epidermolysis bullosa and beta-thalassemia minor in two siblings with end-stage renal disease. Nephron. 1988;49:331–2.
- Karamatic Crew V, Burton N, Kagan A, Green CA, Levene C, Flinter F, et al. CD151, the first member of the tetraspanin (TM4) superfamily detected on erythrocytes, is essential for the correct assembly of human basement membranes in kidney and skin. Blood. 2004;104: 2217–23.
- Arin MJ, Oji V, Emmert S, Hausser I, Traupe H, Krieg T, et al. Expanding the keratin mutation database: novel and recurrent mutations and genotype-phenotype correlations in 28 patients with epidermolytic ichthyosis. Br J Dermatol. 2011;164:442–7.
- Oji V, Tadini G, Akiyama M, Blanchet Bardon C, Bodemer C, Bourrat E, et al. Revised nomenclature and classification of Soreze 2009. inherited ichthyoses: results of the First Ichthyosis Consensus Conference in J Am Acad Dermatol. 2010;63:607–41.
- Varki R, Sadowski S, Uitto J, Pfendner E. Epidermolysis bullosa. II. Type VII collagen mutations and phenotype-genotype correlations in the dystrophic subtypes. J Med Genet. 2007;44:181–92.
- Fassihi H, Eady RA, Mellerio JE, Ashton GH, Dopping-Hepenstal PJ, Denyer JE, et al. Prenatal diagnosis for severe inherited skin disorders: 25 years’ experience. Br J Dermatol. 2006;154:106–13.
- Fassihi H, Liu L, Renwick PJ, Braude PR, McGrath JA. Development and successful clinical application of preimplantation genetic haplotyping for Herlitz junctional epidermolysis bullosa. Br J Dermatol. 2010;162:1330–6.
- Leachman SA, Hickerson RP, Schwartz ME, Bullough EE, Hutcherson SL, Boucher KM, et al. First-in-human mutation-targeted siRNA phase Ib trial of an inherited skin disorder. Mol Ther. 2010; 18:442–6.
- Atkinson SD, McGilligan VE, Liao H, Szeverenyi I, Smith FJ, Moore CB, et al. Development of allele-specific therapeutic siRNA for keratin 5 mutations in epidermolysis bullosa simplex. J Invest Dermatol. 2011;131:2079–86.
- Wally V, Klausegger A, Koller U, Lochmuller H, Krause S, Wiche G, et al. 5’ Trans-splicing repair of the PLEC1 gene. J Invest Dermatol. 2008;128:568–74.
- Dallinger G, Puttaraju M, Mitchell LG, Yancey KB, Yee C, Klausegger A, et al. Development of spliceosome-mediated RNA trans-splicing (SMaRT) for the correction of inherited skin diseases. Exp Dermatol. 2003;12:37–46.
- Wally V, Brunner M, Lettner T, Wagner M, Koller U, Trost A, et al. K14 mRNA reprogramming for dominant epidermolysis bullosa simplex. Hum Mol Genet. 2010;19:4715–25.
- Carulli S, Contin R, De Rosa L, Pellegrini G, De Luca M. The long and winding road that leads to a cure for epidermolysis bullosa. Regen Med. 2013;8:467–81.
- Mavilio F, Pellegrini G, Ferrari S, Di Nunzio F, Di Iorio E, Recchia A, et al. Correction of junctional epidermolysis bullosa by transplantation of genetically modified epidermal stem cells. Nat Med. 2006;12: 1397–402.
- Urnov FD, Rebar EJ, Holmes MC, Zhang HS, Gregory PD. Genome editing with engineered zinc finger nucleases. Nat Rev Genet. 2010; 11:636–46.
- Carroll D. Genome engineering with zinc-finger nucleases. Genetics. 2011;188:773–82.
- Osborn MJ, Starker CG, McElroy AN, Webber BR, Riddle MJ, Xia L, et al. TALEN-based gene correction for epidermolysis bullosa. Mol Ther. 2013;21:1151–9.
- Remington J, Wang X, Hou Y, Zhou H, Burnett J, Muirhead T, et al. Injection of recombinant human type VII collagen corrects the disease phenotype in a murine model of dystrophic epidermolysis bullosa. Mol Ther. 2009;17:26–33.
- Woodley DT, Wang X, Amir M, Hwang B, Remington J, Hou Y, et al. Intravenously injected recombinant human type VII collagen homes to skin wounds and restores skin integrity of dystrophic epidermolysis bullosa. J Invest Dermatol. 2013;133:1910–13.
- Palazzi X, Marchal T, Chabanne L, Spadafora A, Magnol JP, Meneguzzi G. Inherited dystrophic epidermolysis bullosa in inbred dogs: a spontaneous animal model for somatic gene therapy. J Invest Dermatol. 2000;115:135–7.
- Cogan J, Wang XY, Hou YP, Khilili M, Woodley DT, Chen M. Epitope mapping of anti-type VII collagen antibodies in the patients with recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2013;133:S45.
- Wong T, Gammon L, Liu L, Mellerio JE, Dopping-Hepenstal PJ, Pacy J, et al. Potential of fibroblast cell therapy for recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2008;128:2179–89.
- Nagy N, Almaani N, Tanaka A, Lai-Cheong JE, Techanukul T, Mellerio JE, et al. HB-EGF induces COL7A1 expression in keratinocytes and fibroblasts: possible mechanism underlying allogeneic fibroblast therapy in recessive dystrophic epidermolysis Bullosa. J Invest Dermatol. 2011;131:1771–4.
- Fritsch A, Loeckermann S, Kern JS, Braun A, Bosl MR, Bley TA, et al. A hypomorphic mouse model of dystrophic epidermolysis bullosa reveals mechanisms of disease and response to fibroblast therapy. J Clin Invest. 2008;118:1669–79.
- Kern JS, Loeckermann S, Fritsch A, Hausser I, Roth W, Magin TM, et al. Mechanisms of fibroblast cell therapy for dystrophic epidermolysis bullosa: high stability of collagen VII favors long-term skin integrity. Mol Ther. 2009;17:1605–15.
- Venugopal SS, Yan W, Frew JW, Cohn HI, Rhodes LM, Tran K, et al. A phase II randomized vehicle-controlled trial of intradermal allogeneic fibroblasts for recessive dystrophic epidermolysis bullosa. J Am Acad Dermatol. 2013;69:898–908.e7.
- Petrof G, Martinez-Queipo M, Mellerio JE, Kemp P, McGrath JA. Fibroblast cell therapy enhances initial healing in recessive dystrophic epidermolysis bullosa wounds: results of a randomised, vehicle- controlled trial. Br J Dermatol. 2013;169:1025–33.
- Conget P, Rodriguez F, Kramer S, Allers C, Simon V, Palisson F, et al. Replenishment of type VII collagen and re-epithelialization of chronically ulcerated skin after intradermal administration of allogeneic mesenchymal stromal cells in two patients with recessive dystrophic epidermolysis bullosa. Cytotherapy. 2010;12:429–31.
- Tamai K, Yamazaki T, Chino T, Ishii M, Otsuru S, Kikuchi Y, et al. PDGFRalpha-positive cells in bone marrow are mobilized by high mobility group box 1 (HMGB1) to regenerate injured epithelia. Proc Natl Acad Sci U S A. 2011;108:6609–14.
- Dimarino AM, Caplan AI, Bonfield TL. Mesenchymal stem cells in tissue repair. Front Immunol. 2013;4:201.
- Tolar J, Mehta PA, Walters MC. Hematopoietic cell transplantation for nonmalignant disorders. Biol Blood Marrow Transplant. 2012;18: S166–71.
- Wagner JE, Ishida-Yamamoto A, McGrath JA, Hordinsky M, Keene DR, Woodley DT, et al. Bone marrow transplantation for recessive dystrophic epidermolysis bullosa. N Engl J Med. 2010;363:629–39.
- Tolar J, Blazar BR, Wagner JE. Concise review: transplantation of human hematopoietic cells for extracellular matrix protein deficiency in epidermolysis bullosa. Stem Cells. 2011;29:900–6.
- Tolar J, Wagner JE. Allogeneic blood and bone marrow cells for the treatment of severe epidermolysis bullosa: repair of the extracellular matrix. Lancet. 2013;382:1214–23.
- Jonkman MF, Scheffer H, Stulp R, Pas HH, Nijenhuis M, Heeres K, et al. Revertant mosaicism in epidermolysis bullosa caused by mitotic gene conversion. Cell. 1997;88:543–51.
- Almaani N, Nagy N, Liu L, Dopping-Hepenstal PJ, Lai-Cheong JE, Clements SE, et al. Revertant mosaicism in recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2010;130:1937–40.
- Lai-Cheong JE, McGrath JA. Revertant mosaicism in the skin. G Ital Dermatol Venereol. 2013;148:73–82.
- Pasmooij AM, Nijenhuis M, Brander R, Jonkman MF. Natural gene therapy may occur in all patients with generalized non-Herlitz junctional epidermolysis bullosa with COL17A1 mutations. J Invest Dermatol. 2012;132:1374–83.
- Gostynski A, Deviaene FC, Pasmooij AM, Pas HH, Jonkman MF. Adhesive stripping to remove epidermis in junctional epidermolysis bullosa for revertant cell therapy. Br J Dermatol. 2009;161:444–7.
- Gostynski A, Pasmooij AM, Bremer J, Huizinga J, Duipmans J, Jonkman MF. Successful therapeutic transplantation of revertant skin in a patient with epidermolysis bullosa. J Invest Dermatol. 2013; 133:S132.
- Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, Tomoda K, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell. 2007;131:861–72.
- Hou P, Li Y, Liu C, Guan J, Li H, Zhao T, et al. Pluripotent stem cells induced from mouse somatic cells by small-molecule compounds. Science.2013;341:651–4.
- Tolar J, Xia L, Riddle MJ, Lees CJ, Eide CR, McElmurry RT, et al. Induced pluripotent stem cells from individuals with recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2011;131: 848–56.
- Itoh M, Kiuru M, Cairo MS, Christiano AM. Generation of keratinocytes from normal and recessive dystrophic epidermolysis bullosa-induced pluripotent stem cells. Proc Natl Acad Sci U S A. 2011;108:8797–802.
- Tolar J, McGrath JA, Xia L, Riddle M, Lees CJ, Eide C, et al. Patient-specific naturally gene-reverted induced pluripotent stem cells in recessive dystrophic epidermolysis bullosa. J Invest Dermatol. 2014; in press.
- Bidou L, Allamand V, Rousset JP, Namy O. Sense from nonsense: therapies for premature stop codon diseases. Trends Mol Med. 2012;18:679–88.
- Roberts RG. A read-through drug put through its paces. PLoS Biol. 2013;11:e1001458.
- Zhou Y, Jiang Q, Takahagi S, Shao C, Uitto J. Premature termination codon read-through in the abcc6 gene: potential treatment for pseudoxanthoma elasticum. J Invest Dermatol. 2013;133:2672–7.
- Wally V, Kitzmueller S, Lagler F, Moder A, Hitzl W, Wolkersdorfer M, et al. Topical diacerin for epidermolysis bullosa. Orphanet J Rare Dis. 2013;8:69.