Abstract
A 62-year-old man was admitted to our hospital with complaints of abdominal pain and rectal bleeding. Although the colonoscopic examination was highly suggestive of a carcinoma, the histopathological examinations were consistent with chronic inflammation. CT examination revealed a solid lesion from cecum to the ascending colon with right urethral invasion. Percutaneous right nephrostomy was performed for grade 2–3 hydronephrosis. Three days after hospitalization, ileus developed and right hemicolectomy was performed. During surgery we observed that the lesion had invaded the middle part of ureter. So the middle part of ureter was removed with side-to-side urethral anastomosis and 6F double-J catheter was placed. The histopathological findings of resected specimen were consistent with ameboma. Reviewing the literature unilateral hydronephrosis due to colonic amebiasis has not been reported.
INTRODUCTION
Amebiasis is an infectious disease caused by the protozoan Entamoeba histolytica. Transmission is mostly by ingestion of contaminated food and water; however, venereal transmission via the fecal–oral route can also occur. It may rarely evolve into invasive colitis and formation of ameboma, which can closely resemble colorectal carcinoma. The clinical spectrum of colorectal amebiasis ranges from asymptomatic carrier to severe fulminant necrotizing colitis with bleeding and perforation.Citation1 Generally a quick way to diagnose is by examining the stool for trophozoites and cyst.Citation2 During the course of colonic amebiasis, misdiagnosis and delay in treatment have often caused significant morbidity and mortality. Localized colonic infection resulting in a mass of granulation tissue forming an ameboma is another uncommon presentation, which can mimic colon cancer. Herein we report a case of right urethral hydronephrosis due to invasive colonic amebiasis, which was mimicking a carcinoma on colonoscopy.
CASE REPORT
A 62-year-old man was admitted to our hospital with complaints of abdominal pain, rectal bleeding, and severe loss of weight. He denied symptoms of nausea, vomiting, diarrhea, or fever. His past medical history was unremarkable and he had no family history of colorectal carcinoma. Initial physical examination revealed mild abdominal tenderness and palpable mass on the right upper quadrant. Rectal examination was also normal. Initial laboratory test results were hemoglobin 11.9 g/dL, white cell count 11,800/mm3, platelet count 285,000/mm3, and ESR 38 mm/h; the liver and renal functional tests were normal. Colonoscopy showed a huge mass lesion charging the cecum and nearly caused obstruction. The histopathological examination of tissue specimens revealed chronic inflammation. CT scan of the abdomen and pelvis revealed a solid lesion of dimension 7.5 × 7.5 cm from cecum to the ascending colon, and several lymph nodes were detected in the right parailiac region (A). In addition the lesion infiltrated the right urethral wall and right-sided hydronephrosis was developed (B). Percutaneous right nephrostomy was performed for grade 2–3 hydronephrosis. On the fifth day of hospitalization, nausea, vomiting, and abdominal pain developed. Physical examination revealed abdominal distention and rebound tenderness in all quadrants. Signs of ileus were present and his general condition deteriorated rapidly so that emergency surgery including right hemicolectomy was performed. During surgery we observed that the lesion had invaded the middle part of the ureter. Thereafter the middle part of the ureter was removed with side-to-side urethral anastomosis and 6F double-J catheter was placed. The pathological examination of the specimen revealed ameboma () and metronidazole was started and he was discharged from hospital on the seventh day of hospitalization. The double-J stent was easily removed 3 months after surgery.
Figure 1. (A) CT scan of the abdomen and pelvis revealed a solid lesion of dimension 7.5 × 7.5 cm from cecum to the ascending colon (white arrow). (B) CT scan showed grade 2–3 right-sided hydronephrosis (white arrow).
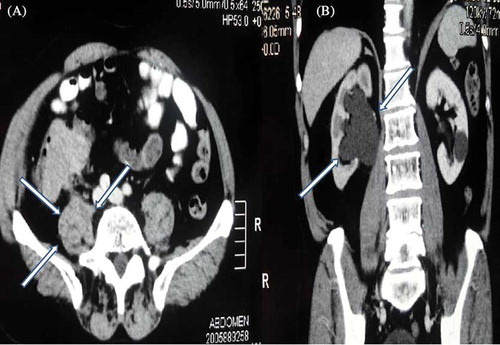
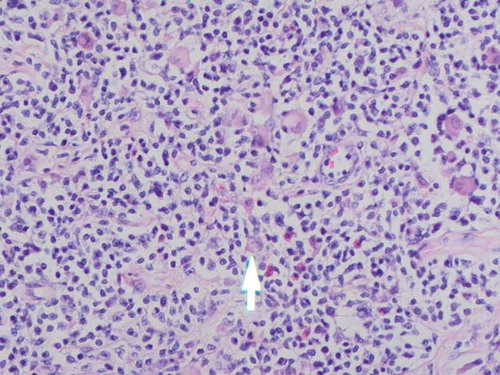
Figure 2. The histopathological examination showed trophozoites of Entamoeba histolytica.
DISCUSSION
E. histolytica is the causative organism responsible for human amebiasis and amebic dysentery.Citation3 The gastrointestinal tract and liver are the two main organ systems affected by the parasite. Rarely, patients with long-standing or partially treated infections develop tumors, exophytic, cicatricial, and inflammatory masses known as “amebomas.” Amebomas occur in only 1.5% of patients with amebiasisCitation4 and result from the formation of annular colonic granulation tissue at single or multiple sites, usually within the cecum or ascending colon. They can also cause obstructive symptoms. In areas in which infection is prevalent, crampy abdominal pain plus a palpable mass usually suggests the diagnosis.Citation3 In contrast, in western countries, a similar presentation alternatively raises suspicion of malignancy.
The standard method for diagnosis of intestinal amebiasis is examination of stools by microscopy. However, the reported sensitivity of this method for identifying amebic organisms ranges from 25% to 60%.Citation5 Currently, more sensitive and specific methods, including antigen detection in stools and serum, and polymerase chain reaction techniques are utilized. Radiological findings prompted the surgeons to investigate for amebic etiology and ameboma was considered a more probable diagnosis. Although plain radiograph of abdomen and ultrasound cannot differentiate between colon cancer and ameboma, CT scan plays a crucial role in clinching the diagnosis.Citation6
Urinary tract obstruction (UTO) may be acute or chronic, partial or complete, unilateral or bilateral, and may occur at any site in the urinary tract.Citation7 The causes of UTO are anatomic abnormalities, calculi, prostatic hypertrophy or carcinoma, and retroperitoneal or pelvic neoplasms. Reviewing the literature unilateral hydronephrosis due to colonic amebiasis with urethral invasion has never been reported.
Renal hydatidosis is a rare site of presentation of hydatid disease and the diagnosis of this condition is usually difficult. Up to 80% of cases with renal hydatidosis were diagnosed through radiological and serologic examinations. The remaining 20% of cases cannot confirm the diagnosis, so urine cytology should be done.Citation8 Scolices of Echinococcus granulosus may be revealed by urine cytology if there is urethral invasion due to colonic amebiasis.
In conclusion, clinicians should keep in mind ameboma in the differential diagnosis of colonic mass lesion with UTO, which can be due to urethral invasion.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- Haque R, Huston CD, Hughes M, Amebiasis. N Engl J AU: Please check whether the short title running head is OK.Med. 2003;348:1565.
- Haque R, Kress K, Wood S, . Diagnosis of pathogenic Entamoeba histolytica infection using a stool ELISA based on monoclonal antibodies to the galactose-specific adhesin. J Infect Dis. 1993;167:247–249.
- Simsek H, Elsurer R, Sokmensuer C, Balaban HY, Tatar G. Ameboma mimicking carcinoma of the cecum: Case report. Gastrointest Endosc. 2004;59:453–454.
- Misra SP, Misra V, Dwivedi M. Ileocecal masses in patients with amebic liver abscess: Etiology and management. World J Gastroenterol. 2006;12:1933–1936.
- Ng DC, Kwok SY, Cheng Y, Chung CC, Li MK. Colonic amoebic abscess mimicking carcinoma of the colon. Hong Kong Med J. 2006;12:71–73.
- Powell SJ, MacLeod I, Wilmot AL, Elsdon-Dew R. Metronidazole in amoebic dysentery and amoebic liver abscess. Lancet. 1966;2:1329–1331.
- Rose BD, Black RM. Manual of Clinical Problems in Nephrology. Boston, MA: Little Brown; 1988:337–343.
- Noi I, Cohen I, Loberant N. Renal hydatid cyst: Urinary cytological diagnosis. Diagn Cytopathol. 1995;12:152–154.