Abstract
Congenital megacalycosis is a rare renal disease characterized by calyceal dilatation without pelvic or ureteral obstruction. If not accompanied by nephrolithiasis and urinary tract infection, this disease is completely benign and does not cause renal dysfunction. We present a case of congenital megacalycosis that was diagnosed at the age of 41 (oldest case in the literature) after admitting with hematuria and acute renal dysfunction. IgA nephropathy was also diagnosed in this patient. Since renal dysfunction is not likely in these patients, if encountered; renal biopsy should be performed although technically difficult to diagnose the cause of this dysfunction.
INTRODUCTION
Congenital megacalycosis is a rare renal disease characterized by calyceal dilatation without renal pelvic or ureteral obstruction. It was first described in 1963.Citation1 The presentation is mostly unilateral and shows male predominance. It is usually diagnosed in childhood or adolescence.Citation2 If not accompanied by nephrolithiasis and urinary tract infection, this disease is completely benign and does not cause renal dysfunction.Citation3 We present a case of congenital megacalycosis that was diagnosed at the age of 41 (oldest case reported in the literature) after admitting with hematuria and acute renal dysfunction.
CASE REPORT
A 41-year-old male patient had been referred to our clinic for acute impairment in kidney function tests. He had a history of bilateral hydronephrosis that was incidentally diagnosed by abdominal ultrasonography 3 years ago. At that time, his renal function and intravenous pyelographic examinations were normal. There was no obstruction or urolitithiasis. He never had a urinary tract infection.
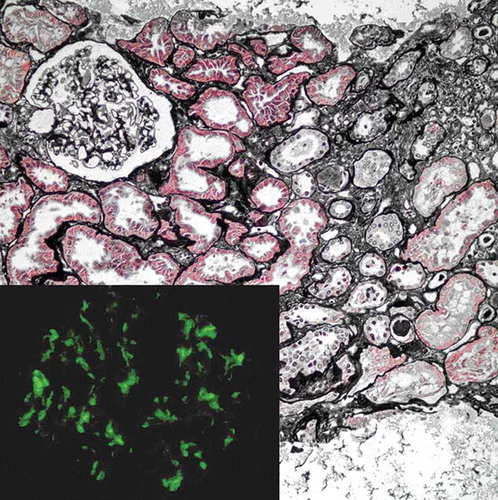
He had experienced a severe upper respiratory tract infection 2 months before and received azithromycin and oseltamivir. Four days later, he complained of dark-colored urine and oliguria. His creatinine level was 2.7 mg/dL. Urinalysis showed hematuria with no protein. Renal ultrasonography revealed bilateral hydronephrosis. The patient was recommended to increase oral intake and was followed for 2 weeks. Although his creatinine level decreased to 1.5 mg/dL, the patient was referred to our center after his hematuria recurred. On admission, the patient’s creatinine level was 1.58 mg/dL and estimated glomerular filtration rate (GFR) was 49 mL/min/1.73 m2. Blood pressure was 130/80 mm Hg and the physical examination was unremarkable. He had dysmorphic erythrocytes on urine sediment without marked proteinuria or eosinophiluria. Sizes and parenchymal thicknesses of both kidneys were normal on ultrasonography. There was mild to intermediate bilateral hydronephrosis in collecting systems with no dilatation in ureters. Magnetic resonance urography revealed increased number of calyces and renal pelvic dilatation. Ureters and bladder were normal and obstruction was excluded (). He was diagnosed with megacalycosis. Renal biopsy was performed to reveal the cause of hematuria and acute kidney dysfunction. Biopsy represented a sample from a small area in renal cortex and included 15 glomeruli, four of which were globally sclerotic. Glomeruli looked normal light microscopically (). No mesangial, endocapillary or extracapillary proliferations were present. Necrosis, karyorrhexis, or segmental glomerular sclerosis was not identified. Mesangial regions were not expanded significantly. There were a few narrow foci of mild tubular atrophy and interstitial fibrosis (). Interstitial inflammatory infiltrate was not observed except a small amount of lymphocytes in the subcapsular scar region. Arteries revealed mild to moderate intimal fibrosis. Immunofluorescence microscopy showed diffuse and global IgA deposition in the mesangial regions (, inset). C3 accompanied IgA in glomeruli. Staining for IgG, IgM, C4 and C1q was negative. The histopathological diagnosis was IgA nephropathy. Prednisolone (1 mg/kg/day) was started for the patient to treat IgA nephropathy. However, he could not tolerate prednisolone due to side effects, and conservative treatment was recommended with an angiotensin receptor blocker to control blood pressure. Under this treatment, serum creatinine level of the patient was 1.3–1.4 mg/dL.
Figure 1. Magnetic resonance urography revealed calyceal dilatation, increased number of calyces, and normal ureters and bladder.
Figure 2. Glomeruli had no significant alterations light microscopically [(A) hematoxylin and eosin stain, ×200 magnification and (B) Masson’s trichrome stain, ×400 magnification].
![Figure 2. Glomeruli had no significant alterations light microscopically [(A) hematoxylin and eosin stain, ×200 magnification and (B) Masson’s trichrome stain, ×400 magnification].](/cms/asset/5e57354d-ed17-49e7-aa8b-ddb5c315cdf0/irnf_a_731996_f0002_b.jpg)
Figure 3. Mild tubular atrophy with interstitial fibrosis is noted at right side of the picture (Jone’s methanamine silver stain, × 200 magnification). Inset shows deposition of IgA in the mesangial regions (imunofluorescence, fluorescein isothiocyanate-conjugated anti-IgA antibody ×400).
DISCUSSION
Congenital megacalycosis is a rare congenital abnormality. The renal calyces in affected kidneys are enlarged without any evidence of obstruction in infundibula, pelvis, or ureter.Citation2,3 In addition to dilatation, the calyces may be increased in number. Renal parenchymal thickness and structure are often normal. This anomaly is encountered predominantly in male Caucasian patients, and usually presents unilaterally.Citation2
Congenital megacalycosis is thought to occur due to abnormal development of the renal medulla, which leads to hypoplastic renal pyramids and blunted, dilated calyces.Citation4 Renal papillae are hypoplastic and, instead of protruding into the calyceal cavity, they surround hypotonic calyces. Urinary stasis in those dilated calyces may predispose to infection and stone formation.Citation5 Abnormalities such as megaureter or Schinzel–Giedion syndrome may accompany this condition.Citation3,5–7
This disorder is generally diagnosed during evaluation of nephrolithiasis and/or urinary tract infection.Citation7–12 Obstructive nephropathy and vesicoureteral reflux should be excluded before diagnosing congenital megacalycosis. Ultrasonography, intravenous pyelography, scintigraphy, and computed tomography play important roles in the exclusion of obstructive causes.Citation13,14 We preferred magnetic resonance urography as the diagnostic imaging modality, because of the risk of contrast nephropathy.
Patients described in the literature were mostly children, and the oldest patients were 22 years of age.Citation7,8 Probably because of asymptomatic course of our patient, he was diagnosed at the fifth decade, and he is the oldest patient in the literature at the time of diagnosis. Clinical characteristics of all the reported patients with congenital megacalycosis were shown in .Citation7–12,Citation15–18
Table 1. Clinical and demographic characteristics of the cases with congenital megacalycosis described in the literature.
Renal function of patients with congenital megacalycosis is usually normal both at the time of diagnosis and during follow-up.Citation12 Slight defects in concentration capacity can be seen due to relative loss of juxtamedullary nephrons.Citation2 There were case reports of patients who had normal renal GFRs, but had parenchymal injury due to recurrent urinary tract infections.Citation8 If there is renal dysfunction in patients with congenital megacalycosis that cannot be explained by simple blood, urine, and radiological tests, a renal biopsy should be performed to diagnose the other causes such as glomerulonephritis. Management of congenital megacalycosis includes prompt treatment of urinary tract infections and nephrolithiasis. Patients should be followed annually by kidney function tests and urinalysis.Citation12 To minimize the risk of stone formation, liberal fluid intake is advised. Prognosis is very good in these patients. The patient in this report had hematuria and impaired renal functions without an obvious cause such as urinary tract infection or nephrolithiasis. He also had a history of a severe upper respiratory infection requiring use of antibacterial and antiviral medications.
After excluding urinary tract infections and nephrolithiasis, IgA nephropathy is one of the most common causes of hematuria in general population. Approach to renal dysfunction in patients with congenital megacalycosis is not well described. In this case, a renal biopsy was performed to elucidate the cause of hematuria and renal dysfunction. Although renal biopsies performed by experienced physicians have low probability of causing severe complications, dilated calyceal system and relatively thin renal parenchyme make renal biopsy technically challenging in patients with congenital megacalycosis.Citation19 The result of biopsy in this case was IgA nephropathy, consistent with the clinical picture including hematuria and renal dysfunction. This is the first case of IgA nephropathy accompanying congenital megacalycosis in the literature.
In conclusion, congenital megacalycosis does not cause symptoms if not associated with nephrolithiasis or urinary tract infection and has a benign prognosis. Since renal dysfunction is not likely in these patients, if encountered; renal biopsy should be performed although technically difficult to diagnose the cause of this dysfunction.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- Puıgvert A. Megacalyosis: differential diagnosis from hydrocalyectasia. Med Clin (Barc). 1963;41:294–302.
- Gittes RF, Talner LB. Congenital megacalices versus obstructive hydronephrosis. J Urol. 1972;108(6):833–836.
- Kimche D, Lask D. Megacalycosis. Urology. 1982;19(5): 478–481.
- Herman TE, Sweetser DA, McAlister WH, Dowton SB. Schinzel-Giedion syndrome and congenital megacalyces. Pediatr Radiol. 1993;23(2):111–112.
- Mandell GA, Snyder HM III, Heyman S, Keller M, Kaplan JM, Norman ME. Association of congenital megacalycosis and ipsilateral segmental megaureter. Pediatr Radiol. 1987;17(1):28–33.
- Perera Soler R, Ruiz González AP, Molini Menchón N, García Nieto VM. Unilateral multicystic dysplastic kidney and contralateral megacalycosis. An unusual association. An Pediatr (Barc). 2004;60(5):473–476.
- Vargas B, Lebowitz RL. The coexistence of congenital megacalyces and primary megaureter. AJR Am J Roentgenol. 1986;147(2):313–316.
- Kasap B, Kavukcu S, Soylu A, Turkmen M, Secil M. Megacalycosis: report of two cases. Pediatr Nephrol. 2005;20(6):828–830.
- Alivanis P, Giannikouris I, Arvanitis A, Volanaki M, Zervos A, Paliuras C. Bilateral congenital megacalycosis in a young male patient. Nephrol Dial Transplant. 2006;21(5):1446–1447.
- Parlaktas BS, Erdemir F, Uluocak N. Congenital megacalycosis: a rare renal developmental anomaly. Turk J Med Sci. 2004;34(6):401–403.
- Pieretti-Vanmarcke R, Pieretti A, Pieretti RV. Megacalycosis: a rare condition. Pediatr Nephrol. 2009;24(5):1077–1079.
- Redman JF, Neeb AD. Congenital megacalycosis: a forgotten diagnosis? Urology. 2005;65(2):384–385.
- Gabutti L, Alerci M, Marone C. Spiral CT angiography for discriminating between megacalyces and intermittent hydronephrosis. Nephrol Dial Transplant. 1997;12(7):1487–1489.
- Cacciaguerra S, Bagnara V, Arena C, Megacalycosis on duplex system upper moiety. Eur J Pediatr Surg. 1996;6(1):42–44.
- Reyes Lara F, Trejo Castillo W. Congenital megacalycosis. Bol Med Hosp Infant Mex. 1982;39(1):29–31.
- Shieh CP, Lin KY, Li YW. Congenital megacalyces. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1990;31(4):237–241.
- Kleszczyński J, Musiał K, Naleśniak M, Fornalczyk K, Czapiga E. Megacalycosis as a diagnostic problem in children. Przegl Lek. 2006;63(3):137–139.
- Bekele W, Sanchez TR. Congenital megacalyces presenting as neonatal hydronephrosis. Pediatr Radiol. 2010;40(9):1579.
- Lefaucheur C, Nochy D, Bariety J. Renal biopsy: procedures, contraindications, complications. Nephrol Ther. 2009;5(4):331–339.