Abstract
Background: Our study aimed to investigate the factors associated with elevated plasma FGF23 (cFGF23) levels in maintenance hemodialysis (MHD) patients and to determine whether plasma FGF23 level is related to aortic artery calcification (AAC). Methods: This study included 120 MHD patients and 20 controls. The FGF23 level was measured using a C-terminal assay and AAC was detected by a lateral lumbar X-ray plain. Results: Plasma FGF23 levels were significantly higher among dialysis patients compared to controls: FGF23 level of 27691.42 ± 55646.41 RU/mL in MHD patients versus 49.89 ± 23.94 RU/mL in health people. Significant correlations were observed between FGF23 levels and vintage, intact parathyroid hormone (iPTH), serum phosphate, total calcium, 25(OH)D, urea nitrogen (BUN), and serum creatinine (SCR). Stepwise multiple regression analysis showed that the independent parameters associated with FGF23 level were serum phosphate, total calcium, parathyroid hormone (PTH), SCR, and prealbumin. There were 73 patients (60.83%) with visible calcification in the abdominal aorta. Bivariate analysis showed that AAC score correlated with FGF23, phosphate, total calcium, vintage, age, and diastolic blood pressure. Forward logistic analysis showed that the independent parameters associated with AAC were age, total protein, and Lg FGF23. Conclusion: Plasma FGF23 level is significant increased in hemodialysis patients and is independently associated with AAC.
INTRODUCTION
Cardiovascular disease (CVD) is the main cause of death in maintenance hemodialysis (MHD) patients. Vascular calcification is an important predictor of mortality in end-stage renal disease. Recently, several novel regulators of arterial calcification, including fibroblast growth factor 23 (FGF23), have been identified. Several studies reported that increased FGF23 was associated with higher rate of CVD.
Different vascular calcification scores have now been evaluated in the dialysis patient. The diagnosis of vascular calcification is usually based on very expensive and highly technical devices like electron beam computed tomography (EBCT) or multislice spiral computed tomography (MSCT). However, lateral lumbar X-ray is a useful approach to detect aortic artery calcification (AAC) with cheap price and low radiation. Additionally, the use of plain radiographic films of bone has already been suggested in kidney disease: improving global outcomes (KDIGO) chronic kidney disease mineral and bone disorder (CKD-MBD) clinic practice guideline.Citation1
Our study aimed to survey the prevalence of AAC and investigate the factors associated with elevated plasma C-terminal FGF23 (cFGF23) levels and to determine whether plasma FGF23 level is related with AAC in Chinese MHD patients.
METHOD
The study included 120 MHD patients as well as 20 controls. All MHD patients were treated in Shanghai’s Ruijin Hospital in July 2011. All MHD patients met the following inclusion criteria: (1) age over 18 years old; (2) receiving hemodialysis three times a week, on a 4-hour schedule, using a dialysate calcium concentration of 1.5 mmol/L; (3) no rapidly progressive kidney disease; and (4) no malignancy. The plasma samples of 20 controls were from the Medical Examination Center of Ruijin Hospital. This study was approved by the Institutional Review Board of the Ruijin Hospital, Shanghai Jiaotong University School of Medicine, and was in accordance with the principle of the Helsinki Declaration.
All clinic data of MHD patients were collected, including blood pressure, which were recorded using the mean of the precious 1 month, height and weight, medical history, and pre-dialysis blood tests, which included prealbumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), total protein (TP), albumin, urea nitrogen (BUN), serum creatinine (SCR), uric acid (UA), parathyroid hormone (PTH), 25(OH)D, triglyceride, cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), serum phosphate, and calcium. PTH was measured using an intact assay by a chemiluminescent method (Abbott i2000); serum 25(OH)D was measured by electrochemiluminescence immunoassay (Roche Cobas e601). The samples for measuring FGF23 were ethylene diamine tetraacetic acid (EDTA) plasma. We collected all the samples with other blood test samples on the same day in July 2011 before dialysis. After centrifugation for 10 min at 2000 rpm, all plasma was stored at –80° as soon as possible. The plasma FGF23 level was measured using a C-terminal assay [FGF23 (C-Term) enzyme-linked immunosorbent assay (ELISA), Immutopics Inc.]. Serum total calcium levels were corrected for serum albumin, calculated by measured Ca level in mg/mL + (4.0–albumin level in mg/mL). Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared.
Aortic artery calcification (AAC) was detected by a lateral lumbar X-ray plain at a voltage of 70 kV in 120 MHD patients and read by two radiologists using a semiquantitative score (). This semiquantitative score was also used by othersCitation2–Citation5 and summarized as follows: calcified deposits along the anterior and posterior longitudinal walls of the abdominal aorta adjacent to each lumbar vertebra from L1 to L4 were assessed using the midpoint of the intervertebral space above and below the vertebrae as the boundaries. Calcifications were graded as follows: 0, no aortic calcific deposits; 1, less than one-third of the corresponding vertebral length; 2, one-third or more, but less than two-thirds of the corresponding length; 3, more than two-thirds of the corresponding length. Each patient’s radiological semiquantitative score ranged from 0 to 4 for the segment affected, from 0 to 6 for each vertebral level, and from 0 to 24 for the total score. The blood tests and X-ray plain were be done within one month.
Figure 1. Aortic artery calcification score.
STATISTICAL ANALYSIS
Statistical Package for Social Analysis (SPSS) version 19.0 was used for data analysis. Results are expressed as mean ± SD, median (and range), or frequency (as percentage). Comparison between groups was performed by an unpaired t-test or the nonparametric Wilcoxon rank-sum test in case of non-normally distributed variables. Spearman’s correlation was used for bivariate analysis. Stepwise multiple regression was done to demonstrate relationships between FGF23 and the other studied factors (criteria: enter p ≤ 0.05, remove ≥0.10). One-way analysis of variance (ANOVA) and independent sample t-test were used to compare the variables according to quartiles of serum FGF23 level. Forward logistic regression was performed to determine significant associations between AAC and other variables, adjusted for potential confounders (criteria: enter p ≤ 0.05, remove ≥0.10). Non-normally distributed variable FGF23, dialysis vintage, PTH, and triglyceride were Lg-transformed to achieve a normal distribution and used in statistical analysis. All statistical tests were performed at the two-sided 0.05 level of significance.
RESULTS
The demographic and clinical characteristics of MHD patients are presented in . Fifteen of 120 MHD patients (12.5%) with diabetes mellitus (DM).
Table 1. Clinical characteristics of MHD patients.
Plasma FGF23 Levels
The plasma samples of 120 MHD patients and 20 health people were tested in our study. Plasma FGF23 levels were significantly higher among the dialysis patients compared to controls, with the FGF23 level of 27691.42 ± 55646.41 RU/mL in MHD patients versus 49.89 ± 23.94 RU/mL in healthy people (p < 0.0001). In MHD patients, the median plasma FGF23 level was 5601.27 RU/mL (interquartile range 1310.47–25783.44 RU/mL) and Lg FGF23 was 3.82 ± 0.79.
Significant correlations were observed between plasma FGF23 levels and Lg vintage (r = 0.413, p < 0.001; A), Lg PTH (r = 0.283, p = 0.002; B), serum phosphate (r = 0.587, p < 0.001; C), total calcium (r = 0.419, p < 0.001; D), 25(OH)D (r = 0.195, p = 0.033; E), BUN (r = 0.263, p = 0.004), and SCR (r = 0.415, p < 0.001; F).
Figure 2. (A) Correlations between Lg FGF23 and Lg Vintage (r = 0.413, p < 0.001). (B) Lg PTH (r = 0.283, p = 0.002). (C) serum phosphate (r = 0.587, p < 0.001). (D) total calcium (r = 0.419, p < 0.001). (E) 25(OH)D (r = 0.195, p = 0.033). (F) SCR (r = 0.415, p < 0.001).
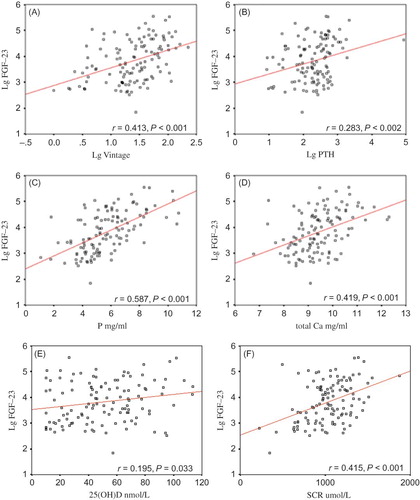
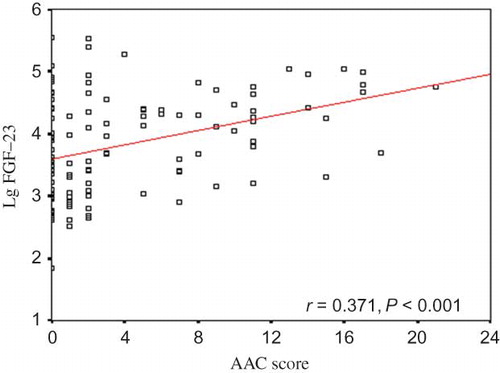
Figure 3. Bivariate correlation between Lg FGF23 level and AAC score (r = 0.371, P < 0.001).
Because Lg FGF23 was normal distribution, stepwise multiple regression analyses showed that the independent parameters associated with FGF23 level were serum phosphate, total calcium, Lg PTH, SCR, and prealbumin (R2 = 0.638, p < 0.001; ).
Table 2. Stepwise multiple regression for factors associated with FGF23 P, Phosphate; Total Ca, total calcium; PTH, parathyroid hormone; SCR, serum creatinine.
Aortic Artery Calcification (AAC)
There were 73 patients (60.83%) with visible calcification in the abdominal aorta, whereas 56 patients (46.67%) with calcification in more than two segments, suggesting severe calcification. The median AAC score was 2.0 (0–21) and median AAC segments affected were 1.0 (0–4).
Aortic Artery Calcification (AAC) and FGF23
According to the FGF23 quartiles, the AAC score in the first quartile was 0.97 ± 1.59, which increased to 3.30 ± 4.81 in the second quartile, 4.93 ± 4.53 in the third quartile, and 6.50 ± 6.92 in the fourth quartile. The third and fourth FGF23 quartiles were associated with more severe AAC ().
Table 3. Baseline characteristics and AAC Score of MHD patients by quartiles of FGF23 level.
Bivariate analysis showed that AAC score correlated in MHD patients with Lg FGF23 (r = 0.371, p < 0.001; ), phosphate (r = 0.201, p = 0.028), total calcium (r = 0.216, p = 0.018), Lg vintage (r = 0.404, p < 0.001), age (r = 0.395, p < 0.001), and diastolic blood pressure (r = 0.395, p = 0.026). Forward logistic analysis showed that the independent parameters associated with AAC were age, TP, and Lg FGF23 (Nagelkerke R2 = 0.395, p < 0.001) ().
Table 4. Forward logistic regression for factors associated AAC Score.
DISCUSSION
Vascular calcification is very common in CKD patients, especially in MHD patients. In 2004, Russo et al. reported that 40% of all CKD patients had vascular calcification as compared to 13% in a matched control population.Citation6 Our study showed that 60.8% of MHD patients had visible calcification in the abdominal aorta. A lower prevalence of AAC (60.83%) detected by later lumbar X-rays that we found in MHD patients compared to other studies reporting a prevalence of 81–94% is probably attributable to a younger population (mean age 55.1 years in our study vs. 61.4 years in calcification outcome in renal disease (CORD) study vs. 66.9 years in Australia study)Citation3,Citation4 or geographical location differences.Citation7
Aortic artery calcification was shown to be associated with coronary artery calcification5 and mortality.Citation2,Citation8,Citation9 Aortic artery calcification can be evaluated by different methods, mainly X-ray plain and computed tomography (CT). Non-contrast abdominal CT, considered as gold standard method, is highly reliable and sensitive for diagnosis of AAC, but it is expensive and delivers a substantial dose of radiation. Because of these limitations, it cannot be widely used in the clinic. Lateral lumbar X-ray is a simple method for detecting AAC with cheap price, available devices, and low radiation. Besides, we also used the AAC score to evaluate the severity of calcification. An AAC score has been reported to be highly correlated with coronary artery calcification.5 In a previous study, FGF\23 has been reported to associate with peripheral calcificationCitation10,Citation11 in dialysis patients, but not with aortic calcification.11 In our study, the main finding was that a single factor of FGF23 was independently correlated to aortic calcification on X-ray plain in MHD patients.
Why FGF23 relates to vascular calcification is still unknown. FGF23 is a novel bone-derived phosphaturic factor involved in mineral metabolism disorder. In our study, we also found that higher FGF23 levels were related to more severe secondary hyperparathyroidism, hypherphosphatemia, and hypercalcinemia. Increased FGF23 levels are observed in early CKDCitation12 and have been linked to increased mortalityCitation13–Citation16 and CVD, such as left ventricle hypertrophyCitation17–Citation19 and vascular calcificationCitation20 in CKD. Although the effects of FGF23 on cells of vascular wall have not been understood, it may play an important role in vascular calcification. FGF23 level increases with decreased kidney function and phosphate accumulates.Citation21 Recent studies have established a relationship between higher phosphate intake and FGF23 levelCitation22 and have found that phosphate binder could reduce the FGF23 level.Citation23,Citation24 FGF23 can promote renal phosphorus wasting and inhibit the conversion of 25(OH)D to the active 1,25-dihydroxyvitamin D form.Citation25–Citation28 Because 25(OH)D did not correlate with FGF23 or AAC score in multivariable models, AAC may not be the result of altered vitamin D levels. However, this point should be interpreted cautiously, because we did not measure the 1,25-dihydroxyvitamin D level in our study.
Another important protein for FGF23 effects is Klotho, a transmembrane protein expressed predominantly in the kidney. High levels of FGF23 as well as deficient renal Klotho expression are observed in CKD patients.Citation29 Some studies showed that, in the absence of Klotho, the increased FGF23 would bind to nonspecific low-affinity receptorsCitation30 and may lead to a procalcification situation. However, serum Klotho levels were not tested in our study.
In multiple logistic regression analysis, the result also showed that TP is a protection factor of aortic calcification in MHD patients. Total protein is not only a nutrition factor, but also reflects the inflammation state of patients. The decreased TP level is associated with an inflammation situation in patients. So, in our study, patients with low TP may have a severe inflammation reaction and may have a link to aortic calcification.
There were a few limitations in our study. First, this study is cross-sectional and therefore does not show FGF23 level predicting the progression of vascular calcification or the detection of AAC by lateral lumbar radiographs predicting incident cardiovascular events and mortality in dialysis population. There is no longitudinal evaluation of the FGF23 level for cardiovascular events. Second, this is one single-center study and requires replication in other independent populations.
CONCLUSION
There is a high prevalence of AAC in Chinese hemodialysis patients. Lateral lumbar X-ray is a simple method for detecting AAC with cheap price, available devices, and low radiation. The plasma FGF23 level is significantly increased in hemodialysis patients, and our study is the first to find that FGF23 is independently associated with AAC detected by X-ray plain. Future studies might investigate the AAC and FGF23 level and mortality or cardiovascular events in Chinese hemodialysis patients, and whether FGF23 is a simple biomarker related to vascular calcification.
Acknowledgments
This work was supported by grant from the Chinese National Key Technology R&D Program (No. 2011BAI10B06).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int. 2009;76(Suppl.113):S1–S130.
- Kauppila LI, New indices to classify location, severity and progression of calcific lesions in the abdominal aorta: a 25-year follow-up study. Atherosclerosis. 1997;132(2):245–250.
- Honkanen E, Abdominal aortic calcification in dialysis patients: results of the CORD study. Nephrol Dial Transplant. 2008;23(12):4009–4015.
- Toussaint ND, Lateral lumbar X-ray assessment of abdominal aortic calcification in Australian haemodialysis patients. Nephrology (Carlton). 2011;16(4):389–395.
- Bellasi A, Correlation of simple imaging tests and coronary artery calcium measured by computed tomography in hemodialysis patients. Kidney Int. 2006;70(9):1623–1628.
- Russo D, Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis. 2004;44(6): 1024–1030.
- El-Saed A, The prevalence of aortic calcification in Japanese compared to white and Japanese-American middle-aged men is confounded by the amount of cigarette smoking. Int J Cardiol. January 10, 2012 [Epub ahead of print].
- London GM, Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18(9):1731–1740.
- Okuno S, Presence of abdominal aortic calcification is significantly associated with all-cause and cardiovascular mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2007;49(3):417–425.
- Jean G, Peripheral vascular calcification in long-haemodialysis patients: associated factors and survival consequences. Nephrol Dial Transplant. 2009;24(3):948–955.
- Inaba M, Role of fibroblast growth factor-23 in peripheral vascular calcification in non-diabetic and diabetic hemodialysis patients. Osteoporos Int. 2006;17(10):1506–1513.
- Ix JH, Fibroblast growth factor-23 and early decrements in kidney function: The Heart and Soul Study. Nephrol Dial Transplant. 2010;25(3):993–997.
- Isakova T, Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. J Am Med Assoc. 2011;305(23):2432–2439.
- Jean G, High levels of serum fibroblast growth factor (FGF)-23 are associated with increased mortality in long haemodialysis patients. Nephrol Dial Transplant. 2009;24(9): 2792–2796.
- Gutierrez OM, Fibroblast growth factor 23 and mortality among patients undergoing hemodialysis. N Engl J Med. 2008;359(6):584–592.
- Holden RM, FGF-23 is associated with cardiac troponin T and mortality in hemodialysis patients. Hemodial Int. 2012;16(1):53–58.
- Canziani ME, Fibroblast growth factor 23 in chronic kidney disease: bridging the gap between bone mineral metabolism and left ventricular hypertrophy. Blood Purif. 2011;31(1–3):26–32.
- Faul C, FGF23 induces left ventricular hypertrophy. J Clin Invest. 2011;121(11):4393–4408.
- Seiler S, The phosphatonin fibroblast growth factor 23 links calcium-phosphate metabolism with left-ventricular dysfunction and atrial fibrillation. Eur Heart J. 2011;32(21):2688–2696.
- Nasrallah MM, Fibroblast growth factor-23 (FGF-23) is independently correlated to aortic calcification in haemodialysis patients. Nephrol Dial Transplant. 2010;25(8):2679–2685.
- Isakova T, Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int. 2011;79(12):1370–1378.
- Gutierrez OM, Wolf M, Taylor EN. Fibroblast growth factor 23, cardiovascular disease risk factors, and phosphorus intake in the health professionals follow-up study. Clin J Am Soc Nephrol. 2011;6(12):2871–2878.
- Koiwa F, Sevelamer hydrochloride and calcium bicarbonate reduce serum fibroblast growth factor 23 levels in dialysis patients. Ther Apher Dial. 2005;9(4):336–339.
- Gonzalez-Parra E, Lanthanum carbonate reduces FGF23 in chronic kidney disease stage 3 patients. Nephrol Dial Transplant. 2011;26(8):2567–2571.
- Antoniucci DM, Yamashita T, Portale AA. Dietary phosphorus regulates serum fibroblast growth factor-23 concentrations in healthy men. J Clin Endocrinol Metab. 2006;91(8):3144–3149.
- Burnett SM, Regulation of C-terminal and intact FGF-23 by dietary phosphate in men and women. J Bone Miner Res. 2006;21(8):1187–1196.
- Shimada T, Cloning and characterization of FGF23 as a causative factor of tumor-induced osteomalacia. Proc Natl Acad Sci USA. 2001;98(11):6500–6505.
- Gutierrez O, Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J Am Soc Nephrol. 2005;16(7):2205–2215.
- Torres PU, Klotho: an antiaging protein involved in mineral and vitamin D metabolism. Kidney Int. 2007;71(8):730–737.
- Urakawa I, Klotho converts canonical FGF receptor into a specific receptor for FGF23. Nature. 2006;444(7120):770–774.