Abstract
Rifampicin is a widely used anti-tuberculosis agent. Apart from hepatotoxicity, rifampicin can rarely lead to adverse reactions of immunologic nature such as acute renal failure (ARF). We report the case of 57-year-old previously healthy man under treatment for pulmonary tuberculosis who presented with hemolysis and severe ARF. Rifampicin was discontinued and the patient was treated with fluid repletion, iv furosemide and dialysis therapy. Kidney biopsy revealed acute tubulointerstitial nephritis with no evidence of granulomas. The patient significantly improved and was discharged after 51 days of hospitalization. Clinicians using rifampicin should be aware of this rather uncommon but severe complication.
Introduction
Rifampicin is widely used for the treatment of tuberculosis and other mycobacterial infections and is also considered an effective antistaphylococcal agent. Hepatotoxicity is the most frequently observed side effect, however adverse reactions of immunologic nature such as acute renal failure (ARF), hemolysis, thrombocytopenia and disseminated intravascular coagulation have also been reported.Citation1–4 According to the ATS recommendations for the treatment of tuberculosis, it is not necessary to routinely monitor renal function in the course of treatmentCitation5 and most chest physicians are probably not aware of rifampicin-associated renal failure. In the present report, we describe the case of hemolysis and severe ARF due to rifampicin in a patient suffering from pulmonary tuberculosis.
Case report
A 57-year-old previously healthy man was admitted to our department for severe fatigue, lack of appetite, weight loss and vomiting during the past 15 days. The patient had been diagnosed with pulmonary tuberculosis affecting both his lungs 2 months before and was receiving rifampicin, isoniazid, ethambutol and pyrazinamide on a daily basis. The patient reported regular intake of his medications and also daily consumption of alcohol.
The patient presented with severe malaise, hypotension (BP 90/50 mmHg, 100 bpm) and hypoxemia (sat 94%) and a BMI of 17.5 kg/m2. Extensive bilateral infiltrates were observed on chest x-ray () and the patient was initially suspected of having resistant tuberculosis. However, his laboratory data revealed anemia (hemoglobin 8.1 g/dL) with evidence of hemolysis (lactate dehydrogenase 429 IU/L, total bilirubin 2.5 mg/dL with an indirect component of 2.15 mg/dL), renal failure (urea 446 mg/dL, creatinine 15.72 mg/dL, potassium 6.93 mEq/L) and elevated erythrocyte sedimentation rate (ESR; 75 mm/h). Metabolic acidosis was observed in his blood gases (ph; 7.06, pCO2: 24.4 mmHg, pO2: 67.3 mmHg, HCO3: 7.1 mmol/Lt). Oliguria, proteinuria and microscopic hematuria were also present. Direct Coombs test was positive. Based on reports of rifampicin-associated renal failure and hemolysis, rifampicin was discontinued and the patient was treated with fluid repletion, iv furosemide and dialysis therapy for four consecutive days and then 3 times weekly. Significant clinical and biochemical improvement was observed and oliguria was recessed. Ziehl–Neelsen stain was positive in sputum but negative in urine and drug susceptibility testing from his initial sputum culture revealed a sensitive strain. Based on the discontinuation of rifampicin and the patient’s glomerular filtration rate (GFR) (13.6 mL/min) the antituberculosis regimen was modified to isoniazid and moxifloxacin once daily and ethambutol and pyrazinamide 3 times per week, after dialysis. The kidney echo showed normal sized kidneys without signs of urinary tract obstruction. Since the possibility of kidney tuberculosis could not be excluded and the patient’s renal function was still impaired a kidney biopsy was performed and acute tubulointerstitial nephritis was observed (). Granulomas were not detected and Ziehl–Neelsen stain was negative. The patient was discharged 51 days after admission, clinically stable with negative sputum Ziehl–Neelsen stains and having gained 3 kg. His anemia and renal function significantly improved (hemoglobin 12.5 g/d, urea 120 mg/dL, creatinine 2.2 mg/dL) along with his ESR (22 mm/h). Based on the increase in GFR (46.3 mL/min), all anti-tuberculosis medications were given daily. The patient is followed up on a weekly basis and 2 weeks after his discharge his renal function and chest X-ray have significantly improved (urea 71 mg/dL, creatinine 1.67 mg/dL).
Figure 1. Chest X-ray at presentation showing bilateral infiltrates.
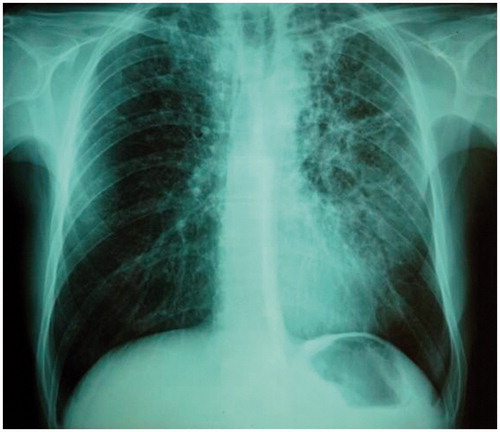
Figure 2. (A) Expansion of the interstitium because of inflammatory infiltrates that separate the tubules. The glomeruli appear unremarkable (hematoxylin and eosin [H + E] stain). (B) Large numbers of small lymphocytes expand the renal interstitium (H + E). (C) Leukocyte infiltration of the tubular epithelium (tubulitis) and variable amounts of tubular injury (tubular necrosis, desquamation, degeneration). (D) In addition to the interstitial lymphocytes, plasma cell and sparse eosinophils are observed (H + E).
![Figure 2. (A) Expansion of the interstitium because of inflammatory infiltrates that separate the tubules. The glomeruli appear unremarkable (hematoxylin and eosin [H + E] stain). (B) Large numbers of small lymphocytes expand the renal interstitium (H + E). (C) Leukocyte infiltration of the tubular epithelium (tubulitis) and variable amounts of tubular injury (tubular necrosis, desquamation, degeneration). (D) In addition to the interstitial lymphocytes, plasma cell and sparse eosinophils are observed (H + E).](/cms/asset/9f46835a-6dd1-4da1-bb6e-fa6f3d92e12b/irnf_a_815567_f0002_b.jpg)
Discussion
Rifampicin-associated ARF is a complication of anti-tuberculosis treatment occurring in less than 0.1% of patients with tuberculosis.Citation5,Citation6 It has also been reported in the setting of leprosy,Citation7 staphylococcal endocarditisCitation8 and infection with non-tuberculous mycobacteria.Citation9 ARF is postulated to be the result of immunologically mediated tubulointerstitial injury.Citation1 Anti-rifampicin antibodies are produced massively, usually after re-exposure to the antigen and cause target-cell damage after complement activation.Citation1 According to the few case series published in the literature several histopathologic patterns have been described: acute tubular necrosis (ATN), acute interstitial nephritis (AIN) and less often rapidly progressing glomerulonephritis and light chain proteinuria.Citation1,Citation2,Citation6,Citation10 De Vriese et al.Citation2 have classified patients with tubulointerstitial nephritis into two groups; one with ATN after intermittent rifampicin treatment and another with AIN after continuous rifampicin intake. This classification has been questioned by othersCitation1,Citation11 as it appears that AIN is often present after intermittent administration of rifampicin.
In any case, it is widely accepted that the vast majority of rifampicin-induced ARF comprise patients receiving rifampicin intermittently, patients with previous drug exposure or poor compliers.Citation1,Citation2,Citation6,Citation12--Citation14 However, cases of ARF after continuous use of rifampicin have been also reported.Citation2,Citation15 In the case presented here the fulminant introduction of symptoms, the oliguric course that required dialysis and the presence of anemia due to intravascular hemolysis would have been more consistent with pre-exposure to rifampicin.Citation2 The mechanism that underlies this observation is thought to involve the continuous formation and clearance of rifampicin-antibody complexes that prevents the increase of antibody titers above a critical level when rifampicin is administered daily.Citation2 To our surprise, the patient denied previous use of rifampicin. Compliance to antituberculosis medication was investigated but he insisted on regular intake of his drugs.
The differential diagnosis of ARF in a patient with tuberculosis includes kidney involvement. In that, setting testing of anti-rifampicin antibodies would have been helpful in order to clarify the immunologic nature of ARF. Unfortunately, this test was not available and a kidney biopsy was performed. The biopsy revealed features suggestive of drug-induced ARF with no evidence of tuberculosis.Citation11 The administration of steroid treatment in patients with drug-induced AIN is a matter of debate.Citation11,Citation16,Citation17 Previous reports did not support the routine administration of steroids in the management of AIN since they were not found to decrease the risk of chronic renal failure.Citation11,Citation16 However more recently, early steroid treatment was shown to improve the recovery of renal function.Citation17 Despite the severity of ARF in our patient, we decided against the use of steroids based on the extent of pulmonary damage and the fact that he was still stain positive 2 months after initiation of treatment. In addition, post-rifampicin ARF has a favorable course with 96% of patients reaching full recovery of renal function 3 months from onset although deaths have been reported.Citation1,Citation6 Based on the patients’ renal function at discharge, it is probable that he will experience a full recovery.
In conclusion, we reported the case of rifampicin-induced AIN in a patient with pulmonary tuberculosis. As tuberculosis is reemerging as one of the most prevalent infectious diseases worldwide, clinicians should be aware of this rather uncommon but severe complication and be prompt to investigate renal function in patients presenting with constitutional and gastrointestinal symptoms.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Muthukumar T, Jayakumar M, Fernando EM, Muthusethupathi MA. Acute renal failure due to rifampicin: a study of 25 patients. Am J Kidney Dis. 2002;40:690–696
- De Vriese AS, Robbrecht DL, Vanholder RC, Vogelaers DP, Lameire NH. Rifampicin-associated acute renal failure: pathophysiologic, immunologic, and clinical features. Am J Kidney Dis. 1998;31:108–115
- Costiniuk CT, McCarthy AE, Talreja H, et al. Acute renal failure and disseminated intravascular coagulation associated with rifampin in tuberculosis treatment. Int J Tuberc Lung Dis. 2011;15:421
- American Thoracic Society/Centers for Disease Control and prevention/Infectious Diseases Society of America. Treatment of tuberculosis. Am J Resp Crit Care Med. 2003;167:603–662
- Rosati S, Cherubini C, Iacomi F, et al. Acute rifampicin-associated interstitial tubulopathy in a patient with pulmonary tuberculosis: a case report. J Med Case Rep. 2013;7:106. doi 10.1186/1752-1947-7-106
- Covic A, Goldsmith DJ, Segall L, et al. Rifampicin-induced acute renal failure: a series of 60 patients. Nephrol Dial Transplant. 1998;13:924–929
- Havey TC, Cserti-Gazdewich C, Sholzberg M, Keystone JS, Gold WL. Recurrent disseminated intravascular coagulation caused by intermittent dosing of rifampin. Am J Trop Med Hyg. 2012;86:264–267
- Wiggins KJ, Galanos JW, Hill PA, Scott KV, Langham RG. Rifampicin-associated segmental necrotizing glomerulonephritis in staphylococcal endocarditis. J Nephrol. 2007;20:489–494
- Ogata H, Kubo M, Tamaki K, Hirakata H, Okuda S, Fujishima M. Crescentic glomerulonephritis due to rifampin treatment in a patient with pulmonary atypical mycobacteriosis. Nephron. 1998;78:319–322
- Prakash J, Kumar NS, Saxena RK, Verma U. Acute renal failure complicating rifampicin therapy. J Assoc Physicians India. 2001;49:877–880
- Rossert J. Drug-induced acute interstitial nephritis. Kidney Int. 2001;60:804–817
- Munteanu L, Golea O, Nicolicioiu M, Tudorache V. Specific features of acute renal failure in patients treated with rifampicin. Pneumologia. 2002;51:15–20
- Covic A, Gusbeth-Tatomir P, Tarevici Z, Mihăescu T, Covic M. Post-rifampicin acute renal failure–serious, but seldom recognized complication of the anti-tuberculosis treatment. Pneumologia. 2001;50:225–231
- Burnette PK, Ameer B, Hoang V, Phifer W. Rifampin-associated thrombocytopenia secondary to poor compliance. DICP. 1989;23:382–384
- Power DA, Russell G, Smith FW, et al. Acute renal failure due to continuous rifampicin. Clin Nephrol. 1983;20:155–159
- Clarkson MR, Giblin L, O'Connell FP, et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004;19:2778–2783
- González E, Gutiérrez E, Galeano C, et al. Early steroid treatment improves the recovery of renal function in patients with drug-induced acute interstitial nephritis. Kidney Int. 2008;73:940–946