Abstract
Chlorine dioxide is a commonly used water disinfectant. Toxicity of chlorine dioxide and its metabolites is rare. In experimental studies, it was shown that acute and chronic toxicity were associated with insignificant hematological changes. Acute kidney injury due to chlorine dioxide was not reported. Two cases of renal toxicity due to its metabolites, chlorate and chlorite were reported. Herein, we report a case of chlorine dioxide poisoning presenting with acute kidney injury.
Introduction
Chlorine dioxide (ClO2) is a commonly used water disinfectant. Chlorine dioxide metabolizes into chlorite and chlorate which are strong oxidizing agents. Several studies done before the introduction of ClO2 for routine usage did not show detrimental effects either in animal studies or in human volunteers. Nevertheless, few reports suggest toxicity involves respiratory, gastrointestinal and hematological systems. Two cases were reported regarding the toxicity due to direct ingestion of sodium chlorite and sodium chlorate poisoning. Herein we report a case of acute kidney injury due to chlorine dioxide poisoning.
Case details
A 20 years aged man presented with anuria of one day duration following history of consumption of 250 mL of stable ClO2 (). There was no history of breathlessness, cyanosis, pedal edema. On examination, he was comfortable, respiratory rate was 18/min, pulse rate was 88/min and BP was 120/80 mm of Hg. General examination and systemic examination were unremarkable. Evaluation showed hemoglobin of 10.5 gm/dL, total leucocyte count – 11,000/mm3, platelet count – 1.5 lakhs/mm3, peripheral smear was normal. His blood urea was 188 mg/dL, serum creatinine was 7.2 mg/dL. Serum electrolytes were normal. Urine analysis showed bland sediment. Color Doppler ultrasound of kidneys was normal. The pelvicaliceal system and the renal vessels were normal. The levels of methemoglobin were not detectable. In view of severe renal failure, he was initiated on hemodialysis. Renal biopsy showed features suggestive of acute tubular necrosis (). By day 15 his urine output improved. At discharge, his serum creatinine was 2.5 mg/dL.
Figure 1. Image of the chlorinedioxide consumed.

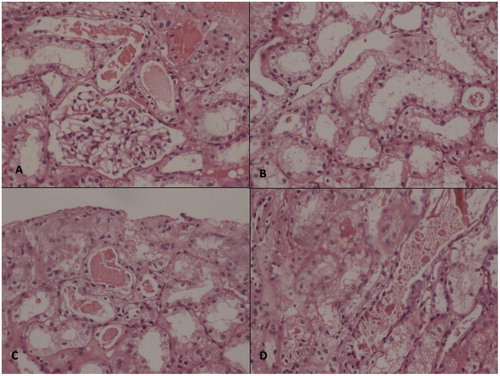
Figure 2. (A) Glomerulus showing normal size and cellularity with normal thickness of the basement membrane. (B) The tubular epithelial cells showing vacuolation of the lining epithelial cells (C & D) Intratubular RBC casts.
Discussion
Chlorine dioxide (ClO2; CASRN 10049-04-4) is a strong oxidizing agent that is reduced to chlorite (ClO2−; CASRN 7758-19-2) under oxidant stress. The strong oxidizing property makes it a very useful agent in water disinfection, bleaching textiles, antimicrobial applications, reducing loads of adsorbable organic halogenated compounds in industrial effluents. Chlorine dioxide rapidly dissociates into chlorite and chloride, and to a lesser extent into chlorate. The interconversion amongst these occurs in water and also in gut.
Of various antioxidant mechanisms in the body, glutathione redox cycle is important. In the presence of oxidant stress, reduced glutathione (GSH) antagonizes the oxidants. But if the severity of oxidant stress is high, the injury to the cells, proteins, lipids, basement membranes, amino acids would be high. The first target hemoglobin undergoes oxidant stress, it gets reduced and forms methemoglobin. Similarly, the injury to cell membranes due to oxidative cross linking of spectrin and lipid peroxidation leads to intravascular hemolysis. In addition, it was observed that ClO2− and ClO3− alter the incorporation of 3H-thymidine into the nuclei of various organs of the rat, thus inhibiting DNA synthesis in several organs.Citation1
The renal manifestations include acute severe interstitial nephritis, acute tubular necrosis and severe vasoconstriction of renal vasculature. The oxidant injury is implicated in the pathogenesis of reversible acute kidney injury. The strong oxidizers would deplete the glutathione in renal tubular and interstitial cells thus causing tubulointerstitial pattern of disease. The imbalance between oxidant stress and the antioxidizing system (Reactive oxygen species (ROS)) leads to injury, usually in the form of acute tubular necrosis. The ROS in renal injury includes superoxide anion, hydrogen peroxide and the hydroxyl radical. Sometimes severe renal vasoconstriction leads to acute tubular necrosis.
Lin and LimCitation2 reported acute kidney injury due to methemoglobinemia in a 25-year-old Chinese patient with sodium chlorite poisoning. The renal biopsy showed features of acute tubulointestinal nephritis and there was complete renal recovery. The second case was reported by Ranghino et al. in a 45 years aged man who had acute sodium chlorate poisoning with acute kidney injury due to methemoglobinemia.Citation3
Other clinical features of toxicity include gastrointestinal symptoms and cyanosis. The irritation of gastric mucosa causes nausea, vomiting, abdominal discomfort. Cyanosis due to methemoglobinemia occurs if the level exceeds 10%. Chlorinedioxide is known to cause intravascular hemolysis.Citation4 A case of myocardial damage due to chlorine dioxide toxicity was reported in the literature.Citation5
Musil et al., Hefferman et al., Abdel-Rehman et al., Courier et al., reported methemoglobinemia, hemolytic anemia, suppressed glutathione levels in experimental animals. Hefferman et al. observed renal toxicity in the form of increase in the kidney/body weight ratio. Bercz et al. reported thyroid toxicity in addition to the hematological changes in African monkeys.Citation6
The effects were usually dose related and marked changes were observed only at the higher dosages (up to 1000 mg/L). Experimentally, rats given a high dose of ClO2 of 1000 mg/L showed alterations in erythrocyte morphology and osmotic fragility, mild hemolytic anemia, dose-related diminution of glutathione content and the enzymes.
Unlike the two other cases reported in the literature, our patient, did not have evidence of methemoglobinemia or hemolysis. The renal biopsy showed features suggestive of acute tubular necrosis.
Though the anuria could not be explained based on histopathology, acute tubular necrosis remains one of the important causes of reversible acute kidney injury in chlorine dioxide poisoning.
The point of interest are three fold:
Direct consumption of Chlorine dioxide can cause acute kidney injury.
Acute kidney injury due to Chlorine dioxide can occur in the absence of methemoglobinemia, hemolysis and disseminated intravascular coagulation.
Acute kidney injury is reversible if it is due to acute tubular necrosis.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Couri D, Abdel-Rahman MS, Bull RJ. Toxicological effects of chlorine dioxide, chlorite and chlorate. Environ Health Perspect. 1982;46:13–17
- Lin JL, Lim PS. Acute sodium chlorite poisoning associated with renal failure. Ren Fail. 1993;15(5):645–648
- Ranghino A, Costantini L, Deprado A, et al. A case of acute sodium chlorate self-poisoning successfully treated without conventional therapy. Nephrol Dial Transplant. 2006;21(10):2971–2974
- Kishan H. Chlorine dioxide-induced acute hemolysis. J Med Toxicol. 2009;5(3):177
- Zhao M, Wang Y. Zhonghua Lao Dong Wei Sheng Zhi Ye One case of myocardial damage due to chlorine dioxide poisoning. Bing Za Zhi. 2005;23(6):470. Chinese
- Lubbers JR, Chauan S, Bianchine JR. Controlled clinical evaluations of chlorine dioxide, chlorite and chlorate in man. Envir Health Perspect. 1982;46:57–62